

Abstract
Background:
Hepatitis B is the world's most common blood-borne viral infection, accounting for 2 billion infections, 350 million carriers, and 6 lakh deaths annually. Country like India still harbors approximately 30–60 million hepatitis B virus (HBV) carriers. A modest estimate would put the number of deaths occurring due to HBV infection per year in India to around 100,000. To prevent transmission and progression of the disease, proper community awareness including prevention is necessary. Therefore, this study aims to study the knowledge awareness among the healthy population about hepatitis B including knowledge regarding vaccine.
Methodology:
A community-based cross-sectional study was undertaken in two districts of Gujarat. Cluster sampling (30 clusters) was used, and pretested questionnaire was administered to 600 (with a prevalence rate of 5% in Gujarat having design effect of 2 within 95% confidence interval and 10% nonrespondent) healthy individuals, who heard about hepatitis B. Data handled and analyzed in EpiData Analysis V2.2.2.183.
Results:
Majority of the participants knew about symptoms whereas only 41% knew about prevention methods and few 34% knew about the mode of transmission. Although 40% sample has knowledge about the availability of vaccination, only 20% were self-vaccinated. The common reason for nonvaccination was lack of awareness.
Conclusions:
Only one-third of the populations in study districts are aware about hepatitis B and its vaccine. Less than one-fifth of the populations are vaccinated for hepatitis B. Important knowledge deficits about the routes of hepatitis B transmission/prevention were identified. Continued efforts should be made to develop and implement hepatitis B educational campaigns/health promotion for these communities.
Keywords: Awareness, hepatitis B, hepatitis B vaccine, hepatitis B virus, knowledge
Introduction
About 240 million persons worldwide are chronically infected with hepatitis B virus (HBV);[1] with heterogeneous prevalence throughout the world. There is an intermediate to high prevalence in the Asia-Pacific region, representing three-quarters of chronic HBV-positive subjects worldwide.[2] In South-East Asia region, the estimated burden of chronic HBV infection is around 100 million.[3] During HBV infection, an estimated 15%–40% of chronic hepatitis B patients would develop complications such as acute exacerbation, liver cirrhosis, and hepatocellular carcinoma.[4,5] The HBV is 50–100 times more infectious than HIV.[6,7,8]
Hepatitis B is a vaccine-preventable infection. Universal HBV vaccination in newborns has dramatically changed the epidemiology of chronic HBV infection.[1,9] A decision-analytical model estimates that in India, vaccination would save 25 lives per 100,000 population per year.[10] By knowing facts, having proper awareness, and attitudes the menace of this disease can be prevented to a great extent.[11] The awareness of HBV infection and its vaccine in our country is believed to be very poor; however, there are no published study/data on the community awareness about HBV infection and its vaccine from India.[12]
HBV is the second most common cause of acute viral hepatitis after HEV in India.[13] With 3.7% point prevalence with over 40 million HBV carriers, India is considered in an intermediate level of HBV endemicity. Every year, one million Indians are at risk for HBV and about 100,000 die from HBV infection.[14,15] In the Middle-East and Indian subcontinent, an estimated number of 2-5% of the general population is chronically infected;[16] however, the exact prevalence of hepatitis B surface antigen is not known in Gujarat state. In Gujarat in February 2009, Modasa town of Sabarkantha district witnessed a major outbreak of hepatitis B. A total of 593 cases were reported to the district authorities of these, 94 had died (case fatality ~17.6%).[17,18] The recommendations from the outbreak investigation reveal that education and awareness programs directed at such populations may make them more aware of the risks they pose to society.
In the present study, we have made an attempt to document the knowledge and awareness of hepatitis B and HBV vaccine status among the general healthy population in two districts of Gujarat, India.
Methodology
Study setting
Gujarat state is composed of 33 districts, the average population of a district being 2 million. Districts are further divided into 10–20 blocks of approximately 100–200,000 populations. For this study, two diverse districts have been chosen named as Mehsana and Sabarkantha [Figure 1]. Sabarkantha distrcit (considered as “District-II” for this study) have population of 2,428,589 with an outbreak of HBV in the year 2009, whereas Mehsana (considered as “District-I” for this study) having population of 184,133 without such kind of incidence. This study has been conducted during October–November 2015.
Figure 1.

Map of Gujarat (India) indicating the study districts (Mehsana, Sabarkantha)
Study sample and sampling
Cluster sampling method was used to select the villages from the two study districts. An estimated sample size of 600 participants from 30 clusters was sampled with a prevalence rate of 5% at Gujarat having design effect of 2 within 95% confidence interval and expected 10% nonrespondent. Therefore, 300 samples have been recruited from each district. To get 300 sample sizes from each district, snow-ball sampling of households has done to identify either any of them at least heard the term hepatitis B. Thus, about 1935 healthy population approached to recruit 600 samples who have heard at least the term hepatitis B.
Study data collection
A community-based cross-sectional study was conducted among healthy population of two above selected study districts, Gujarat, India. Prior permission was taken from the Government of Gujarat. A pretested structured questionnaire consisting of close-ended questionnaire was administered by the trained research assistants. Confidentiality of identity was ensured to all the participated people, and written consent was obtained before filling up of the questionnaire. Ethical permission and clearance were taken from the Indian Institute of Public Health Gandhinagar-Institutional Ethics Committee (IIPHG-IEC).
Study analysis
Data obtained were entered and analyzed through EpiData analysis software v2.2.2.183 (EpiData Association, Odense, Denmark). Descriptive statistics was done to document the knowledge level, and Chi-square or Student's t-test also performed to understand the significant difference (P < 0.05) across the geographic location.
Results
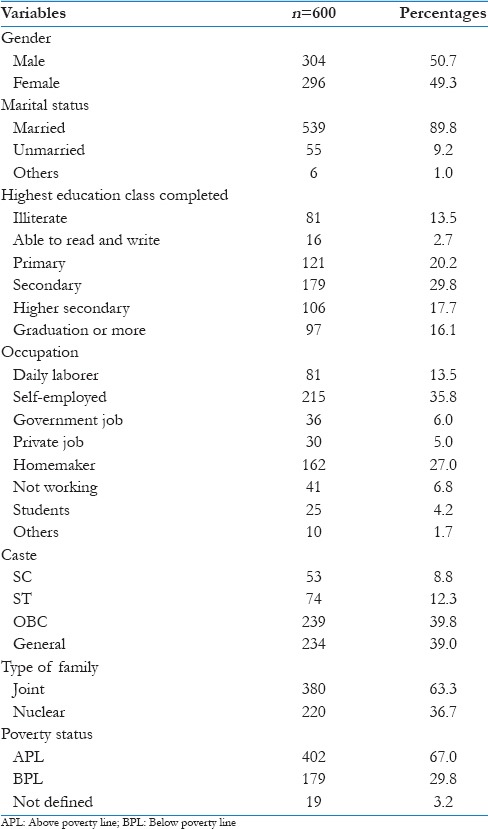
A total of 600 subjects were involved in the study 300 from each district. To recruit 600 participants who have heard the term hepatitis B, investigators have to approach 1953 healthy population. In district-I, 961 general populations approached to recruit 300 (31.2%) participants, whereas, in the district-II, 974 have been approached to recruit 300 (30.8%) healthy population. All the participants were in the age group of 18–92 years with a mean age of 44.8 ± 16.2 years. There were 304 (50.7%) male, and 296 (49.3%) were female participants. Most of the sampled populations were married Hindu with formal education either self-employed or homemakers lives in joint family. The details of descriptive statistics are shown in Table 1.
Table 1.
Sociodemographic characteristics of surveyed health population
Knowledge about symptoms of hepatitis B
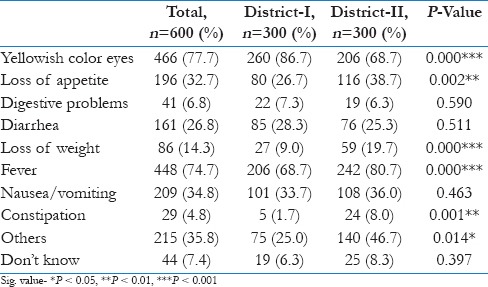
Among all participants, about 92.7% were aware of at least one symptom of hepatitis B. In both the district; there was no significant (P = 0.410) difference in knowledge of symptoms found in this study, even though one of the district has an outbreak earlier. About two-third of sample identified that yellowish color of eyes, fever as one of the primary symptoms of hepatitis B. About one-third of the sample said that loss of appetite, diarrhea, nausea/vomiting also associated with hepatitis B. Among others, digestive problems (6.8%), loss of weight (14.3%), and constipation (4.8%) also have been reported as symptoms of the same. The difference in knowledge about symptoms in two study districts is shown in Table 2.
Table 2.
Knowledge about symptoms of Hepatitis-B
Knowledge about mode of transmission of hepatitis B
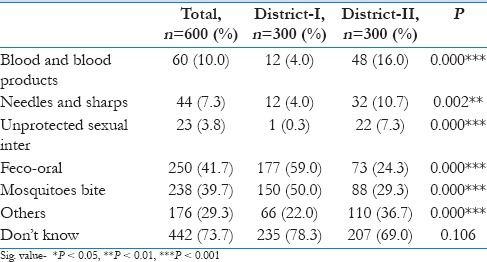
Results revealed that most of the respondents were unaware of the hepatitis B infection. The awareness regarding the modes of transmission of hepatitis B was dissatisfactory as many of participants’ believed that hepatitis B is transmitted by mosquito bite or by feco-oral modes. The transmission by blood and blood products (10%), needles and sharps (7.3%), unprotected sex (3.8%) knowledge level found to be very low, and dissatisfactory. It has been identified that there is statistical significant difference (P < 0.05) in knowledge level about mode of transmission in between two study districts among those have knowledge about transmission. About two-third of sample in both the districts have no knowledge about mode of transmission and found to have no statistical significant (P = 0.106) difference among these study districts. The district-level differences in knowledge of mode of transmission are indicated in Table 3.
Table 3.
Knowledge about mode of transmission of hepatitis B
Knowledge of mode of prevention of hepatitis B
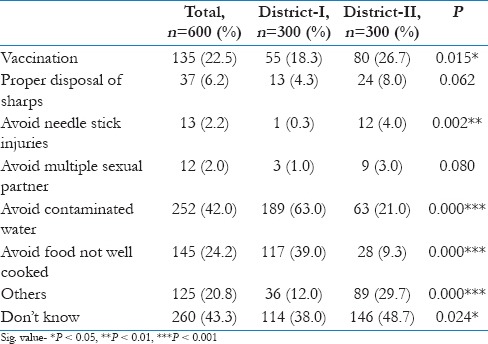
It was found that only 135 (22.5%) people have knowledge that vaccination can prevent hepatitis B transmission. Many of people still have the wrong belief that avoiding contaminated water (24.2%), avoiding uncooked food (20.8%) also prevents the transmission of HBV. Only a few people were aware of preventing hepatitis B infection by proper disposal of sharps (6.2%), needles (2.2%), and avoiding multiple sexual partners (2%) but the other ways of prevention of infection revealed statistically significant difference in results among different districts as indicated in Table 4.
Table 4.
Knowledge about mode of prevention of hepatitis B
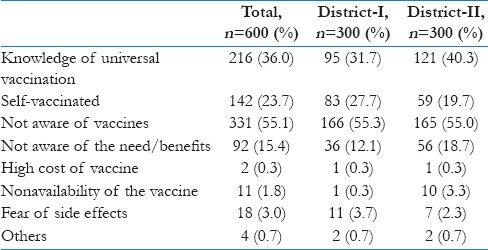
Vaccine status among general population
Only 36% people were aware of the presence of vaccine against HBV. The knowledge regarding the existence of hepatitis B vaccine is mainly acquired by these people due to their recent childbirth and immunization to the newborn which has mentioned in the immunization schedule card. Nearly, 24% of people were vaccinated against HBV as majority of population were unaware of availability of such vaccines and its importance. The reason of nonvaccination among these populations found to be lack of awareness (55.1%), lack of awareness of its benefit (15.4%), due to high cost (0.3%), nonavailability (1.8%), and fear of side-effects (3%). The regional difference between the two districts is shown in Table 5.
Table 5.
Vaccination status and reasons to fail to get vaccinated
This analysis indicates that about two-third of population were never heard about hepatitis B. About 10% of population indicated that either him/her-self or any of family members were affected by any kind of hepatitis during lifetime. TV/radio message found to be the preferred mode of knowledge sharing about any kind of health message in these communities, followed by newspaper (37%), street play (11.3%), and advertisement/hooding (25.5%) for message sharing to improve the health of people.
Discussion
The current study sought to document the knowledge toward hepatitis B among healthy individuals, one of the unique study from Western India. Results of the study revealed poor knowledge toward hepatitis B, majority of people still unaware about the disease and its vaccine even after a recent outbreak in one of the study area. HBV is probably the most important chronic viral infection affecting Indians. However, despite the development of an effective vaccine against HBV, this infection remains a serious threat to public health in India. Awareness about the vaccine and self-vaccination among the subjects was 36% and 24%, respectively, which is quite low and at par with other studies conducted in different parts of the world.[19,20,21,22,23] A study was conducted to know the knowledge, attitude, and practices of married women in the reproductive age group in Jammu regarding HBV infection. Only 20% of the women were found aware of the mode of transmission of HBV. However, 50% of the women were having the misconceptions regarding mode of transmission of HBV.[24] Similarly, another study in Eastern India reveals that awareness about the disease and the vaccine among the subjects was 38% and 32%, respectively. 50% of those who were aware had no knowledge about route of transmission, infectivity, or importance of vaccination.[13] This study had clearly demonstrated that the much lower level of awareness regarding HBV and its vaccination as compared to above two studies.
HBV control now focuses both on pregnancy screening and on vaccinating risk groups, such as newborns from HBV-infected mothers, children with parent(s) from an HBV-endemic area, and people with high-risk behavior. These programs, however, have not contributed to the health of the general adult population, leaving a substantial part of this population both undetected and unprotected regarding HBV. The level of ignorance and the low awareness about immunization should draw attention of policy makers at the earliest.
Limitations
The study was conducted in two districts and therefore results of the research are not representative of the entire population of Gujarat, India.
Conclusion
About two-third of the populations in Gujarat are unaware about hepatitis B and its vaccine, even after recent HBV epidemic. Less than a fifth of the populations are vaccinated for hepatitis B. Important knowledge deficits about routes of hepatitis B transmission/prevention were identified, though these health populations are aware of at least a symptom of HBV. Continued efforts should be made to develop and implement hepatitis B educational campaigns/health promotion for these communities. Emphasis should especially be laid on awareness campaigns to educate the public that hepatitis B is vaccine-preventable disease and do not spread by polluted water or by sharing utensils and that it could be easily prevented by three simple, easily available, inexpensive shots of hepatitis B vaccine. There is an urgent need for community-based interventional study for improving the knowledge and awareness level of these healthy population regarding hepatitis B and its vaccine.
Financial support and sponsorship
The Conquer Hepatitis Project leading to these results been funded by Bristol-Myers Squibb (BMS) Foundation. The funders did not have role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We acknowledge project field staff and participants of this survey. We also acknowledge the Department of Health, Government of Gujarat for support.
References
- 1.Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012;30:2212–9. doi: 10.1016/j.vaccine.2011.12.116. [DOI] [PubMed] [Google Scholar]
- 2.Liaw YF. Antiviral therapy of chronic hepatitis B: Opportunities and challenges in Asia. J Hepatol. 2009;51:403–10. doi: 10.1016/j.jhep.2009.04.003. [DOI] [PubMed] [Google Scholar]
- 3.London WT, McGlynn KA. Liver cancer. In: Scottenfeld D, Fraumeni JF, editors. Cancer Epidemiology and Prevention. United Kingdom: Oxford University Press; 2006. [Google Scholar]
- 4.Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. 2007;45:507–39. doi: 10.1002/hep.21513. [DOI] [PubMed] [Google Scholar]
- 5.de Franchis R, Hadengue A, Lau G, Lavanchy D, Lok A, McIntyre N, et al. EASL International Consensus Conference on hepatitis B 13-14 September, 2002 Geneva, Switzerland. Consensus statement (long version) J Hepatol. 2003;39(Suppl 1):S3–25. [PubMed] [Google Scholar]
- 6.National Foundation for Infectious Diseases. Facts about Hepatitis-B. January. 2012. [Last accessed on 2015 Nov 02]. Available from: http://www.adultvaccination.org/vpd/hepb/facts.html .
- 7.Liaw YF, Leung N, Guan R, Lau GK, Merican I, McCaughan G, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2005 update. Liver Int. 2005;25:472–89. doi: 10.1111/j.1478-3231.2005.01134.x. [DOI] [PubMed] [Google Scholar]
- 8.Ray SK. Vaccine preventable diseases. In: Chaturvedi S, Jena TK, editors. Epidemiology in Maternal and Child Health, Preventive Medicine. MME-101. New Delhi: IGNOU; 2003. pp. 40–66. [Google Scholar]
- 9.Van Damme P, Kane M, Meheus A. Integration of hepatitis B vaccination into national immunisation programmes. Viral Hepatitis Prevention Board. BMJ. 1997;314:1033–6. doi: 10.1136/bmj.314.7086.1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Singh SP. Hepatitis B Eradication Day: It's never too late!! Hepat B Annu. 2006;3:11–3. [Google Scholar]
- 11.Razi A, Rehman R, Naz S, Ghafoor F, Ullah MA. Knowledge attitude and practices of university students regarding hepatitis B and C. ARPN J Agric Biol Sci. 2010;5:38–43. [Google Scholar]
- 12.Misra B, Panda C, Das HS, Nayak KC, Singh SP. Study on awareness about hepatitis B viral infection in coastal Eastern India. Hepat B Annu. 2009;6:19–28. [Google Scholar]
- 13.Rao MB. The Prevalence of Hepatitis B in India and its Prevention. 2012. [Last accessed on 2015 Dec 23]. p. 19. Available from: http://www.namahjournal.com/doc/Actual/Hepatitis-B-vol-19-iss-4.html .
- 14.National Centre for Disease Control (NCDC). Hepatitis in India: Burden, Startergies and Plans. NCDC Newsl. 2014;3:1–3. [Google Scholar]
- 15.Batham A, Narula D, Toteja T, Sreenivas V, Puliyel JM. Sytematic review and meta-analysis of prevalence of hepatitis B in India. Indian Pediatr. 2007;44:663–74. [PubMed] [Google Scholar]
- 16.Gandhi SJ. Hepatitis B outbreak investigation report in Sabarkantha District, Gujarat State, February 2009. Int J Med Med Sci. 2011;3:109–21. [Google Scholar]
- 17.Seetharam S. Hepatitis B outbreak in Gujarat: A wake-up call. Indian J Med Ethics. 2009;6:120–1. doi: 10.20529/IJME.2009.042. [DOI] [PubMed] [Google Scholar]
- 18.Patel DA, Gupta PA, Kinariwala DM, Shah HS, Trivedi GR, Vegad MM. An investigation of an outbreak of viral hepatitis B in Modasa town, Gujarat, India. J Glob Infect Dis. 2012;4:55–9. doi: 10.4103/0974-777X.93762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cheung J, Lee TK, Teh CZ, Wang CY, Kwan WC, Yoshida EM. Cross-sectional study of hepatitis B awareness among Chinese and Southeast Asian Canadians in the Vancouver-Richmond community. Can J Gastroenterol. 2005;19:245–9. doi: 10.1155/2005/583406. [DOI] [PubMed] [Google Scholar]
- 20.Taylor VM, Jackson JC, Chan N, Kuniyuki A, Yasui Y. Hepatitis B knowledge and practices among Cambodian American women in Seattle, Washington. J Community Health. 2002;27:151–63. doi: 10.1023/a:1015229405765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Taylor VM, Yasui Y, Burke N, Choe JH, Acorda E, Jackson JC. Hepatitis B knowledge and testing among Vietnamese-American women. Ethn Dis. 2005;15:761–7. [PubMed] [Google Scholar]
- 22.Schenkel K, Radun D, Bremer V, Bocter N, Hamouda O. Viral hepatitis in Germany: Poor vaccination coverage and little knowledge about transmission in target groups. BMC Public Health. 2008;8:132. doi: 10.1186/1471-2458-8-132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Saif SA, Iqbal R, Hussain H, Khan MH. Awareness of viral hepatitis B in ten villages of district Nowshera. Gomal J Med Sci. 2009;7:10–3. [Google Scholar]
- 24.Sharma R, Sharma CL, Khajuria R. The knowledge, attitude and practices regarding HBV infection of married women in the reproductive age group living in cantonment area, Sunjawan, Jammu. JK Sci. 2004;6:127–30. [Google Scholar]