

Abstract
Strychnine poisoning is a rare method of deliberate self-harm in adults. Poisoning with strychnine leaves is a rare form of strychnine poisoning, as the usual plant parts used are nuts, bark, and seeds. Although the common cardiac manifestations of strychnine positioning include tachycardia and hypertension, we report a patient with mild strychnine poisoning with bradycardia.
Keywords: Strychnine, strychnine leaves, strychnine cardiovascular effects
Introduction
Strychnos nux-vomica is a thorny tree native to the Indian subcontinent. The poisonous derivatives of the tree are seeds and bark. However, toxic alkaloids may be found in the entire plant.[1] The poisonous compounds are strychnine, strychnine, brucine, and loganin. Lethal dose for adults is 30–120 mg. Strychnine poisoning occurs accidentally after the consumption of herbal and native medicinal preparations and as adulterants in illicit drugs or as deliberate self-harm in consumption of rodenticides or direct consumption of the nuts and bark of nux-vomica tree.[2] In the context of deliberate self-harm, there are few reports of consumption of leaves of nux-vomica tree.
Case Report
A 39-year-old man with no previous known comorbidities presented with acute onset myalgias and generalized body ache. He gave a history of consuming six leaves of the local “etti” plant after making it into a decoction with 100 ml of boiling water, with suicidal intent. Later, the plant was confirmed to be Strychnine nux-vomica by visualization [Figure 1].
Figure 1.

Parts of the etti plant as brought by the patients family
Following consumption, he had induced a few episodes of small volume nonbilous vomiting. On presentation to the Emergency Department, he was apprehensive and restless. His pulse rate was 60/min. His respiratory rate was 16 and blood pressure was 100/80 mmHg. The rest of the systemic examination was within normal limits except for moderate muscle tenderness over the calf and thighs. Within hours of consumption, he began to develop twitching movements of the arm and forearm muscles that were more pronounced in his sleep. His basic blood investigations revealed normal blood counts and metabolic panel including electrolytes (serum sodium of 140 mEq/L, serum potassium of 3.8 mEq/L, serum magnesium of 1.86 mg/dl, and corrected serum calcium of 8.46 mg/dl). While under observation, his heart rate dropped to 48 beats/min without any associated hypotension. Urgent electrocardiogram (ECG) showed PR interval prolongation (210 ms) with left anterior fascicular heart block and heart rate of 46 bpm, corrected QT interval of 407 ms, and QRS interval of 96 ms. The patient was put on cardiac monitor, and the vitals were closely monitored. He was kept on maintenance intravenous fluids, and urine output was closely monitored. The levels of serum potassium, magnesium and creatinine kinase were periodically monitored. He was started on tablet lorazepam 2 mg thrice daily for the muscle twitches and injection atropine 1.2 mg was administered as and when required for bradycardia <50 beats/min. He required 2 doses of injection atropine on day 1 of poisoning. The muscle twitches and hypervigilance reduced in severity and he was discharged on day 4.
Discussion
Strychnine poisoning can be secondary to accidental exposure to rodenticide or following consumption with the intention of deliberate self-harm. Strychnine poisoning is known to occur after transdermal, oral, inhalational, or injectable exposure to the toxin.[3] Following exposure, strychnine is absorbed rapidly and clinical features appear within minutes to hours based on the route of exposure. Strychnine primarily acts on the central nervous system as a competitive antagonist on the postsynaptic glycine receptors. The inhibitory effect of the spinal interneurons on the muscles is lost and this in turn leads to twitching, muscle spasms, and these muscles spasms in a conscious patient resemble a “awake” seizure known as spinal seizure. Like tetanus, these spasms can also be provoked with minimal stimulation.[4] Respiratory paralysis can occur following the involvement of thoracic and abdominal musculature and is the most common cause of death. Other complications in severe poisoning include lactic acidosis, hyperthermia, and rhabdomyolysis.[3] In adults, 1–2 mg/kg is considered the lethal dose,[5] however, poisoning with doses as low as 20 mg were lethal and as high as 3750 mg have been salvaged.[6] The cardiovascular effects due to strychnine are usually tachycardia, hypertension, and feeble pulse. As studied in experimental animals, there is an increase in blood pressure and increase in heart rate as a result of inhibition of the pathways that inhibit the central vasomotor outflow.[7] Although strychnine inhibits the spinal sympathetic outflow to the heart,[8] this peripheral action of strychnine is less predominant than the central action on the vasomotor outflow.[7] However, rarely bradycardia and hypotension have also been reported.[5] Other causes of bradycardia in strychnine poisoning that manifest with ECG changes are nonspecific ST-segment and T-wave changes and QRS and QTc prolongation secondary to hypocalcemia.[5] Hypokalemia has also been reported with strychnine poisoning[5] which may contribute to bradycardia.
In our patient, hypocalcemia and hypokalemia were ruled out. Our patient neither had any previous known cardiovascular comorbidity nor was he on any cardiac drugs. Copoisoning with other plant cardiac glycosides was ruled out by direct visualization of the plant parts brought by the relatives. A bedside echocardiogram ruled out any evidence of structural heart disease. Other causes considered were concomitant electrolyte disturbances and preexisting heart block. Eleven days after having consumed the poisonous leaves, at a follow-up visit, an ECG was repeated which showed persistence of bradycardia. Whether the bradycardia was secondary to the poisoning or a confounder probably due to a preexisting heart block is unclear. The elimination of strychnine is mainly by the liver although 1%–30% is excreted by urine.[6] The elimination is by first-order kinetics with a half-life of 12 h.[6]
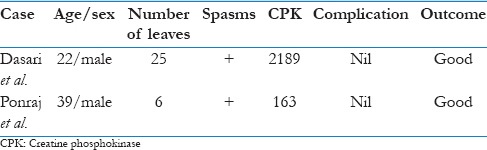
This is the second patient after Dasari and Naha[9] to be described to have clinical features of strychnine poisoning after consumption of leaves of S. nux-vomica as to the knowledge of the authors [Table 1]. Moreover, in both these patients, the clinical manifestations were milder, and neither of them had any of the above-mentioned complications of strychnine poisoning. Both had a good outcome following symptomatic management with diazepam and analgesics.
Table 1.
Comparison of cases of Strychinine nux-vomica leaves poisoning
Conclusion
Deliberate self-harm with S. nux-vomica leaves is very rare. Toxicity profile after the ingestion of leaves is milder. The predominant cardiovascular symptoms are usually tachycardia and hypertension. However, we report the second case of mild poisoning with S. nux-vomica leaves that had a rarer presentation with bradycardia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Dr. Samuel George Hansdak, Professor, Internal Medicine -Unit IV, Christian Medical College and Hospital, Vellore, for his guidance and support.
References
- 1.European Food Safety Authority; 2009. Compendium of botanicals that have been reported to contain toxic, addictive, psychotropic or other substances of concern on request of EFSA. EFSA J. 2009;7:36. [Google Scholar]
- 2.Makarovsky I, Markel G, Hoffman A, Schein O, Brosh-Nissimov T, Tashma Z, et al. Strychnine – A killer from the past. Isr Med Assoc J. 2008;10:142–5. [PubMed] [Google Scholar]
- 3.Boyd RE, Brennan PT, Deng JF, Rochester DF, Spyker DA. Strychnine poisoning. Recovery from profound lactic acidosis, hyperthermia, and rhabdomyolysis. Am J Med. 1983;74:507–12. doi: 10.1016/0002-9343(83)90999-3. [DOI] [PubMed] [Google Scholar]
- 4.Dickson E, Hawkins RC, Reynolds R. Strychnine poisoning: An uncommon cause of convulsions. Aust N Z J Med. 1992;22:500–1. [PubMed] [Google Scholar]
- 5.Bateman DN, Jefferson RD, Thomas SH, Thompson JP, Vale A. Oxford Desk Reference: Toxicology. USA: Oxford University Press; 2014. pp. 261–433. [Google Scholar]
- 6.Wood D, Webster E, Martinez D, Dargan P, Jones A. Case report: Survival after deliberate strychnine self-poisoning, with toxicokinetic data. Crit Care. 2002;6:456–9. doi: 10.1186/cc1549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sofola OA, Odusote KA. Sympathetic cardiovascular effects of experimental strychnine poisoning in dogs. J Pharmacol Exp Ther. 1976;196:29–34. [PubMed] [Google Scholar]
- 8.Hong YG, Yashpal K, Henry JL. Cardiovascular responses to intrathecal administration of strychnine in the rat. Brain Res. 1989;499:169–73. doi: 10.1016/0006-8993(89)91148-7. [DOI] [PubMed] [Google Scholar]
- 9.Dasari S, Naha K. A rare case of strychnine poisoning by consumption of Strychnos nux-vomica leaves. Asian Pac J Trop Biomed. 2011;1:S303–4. [Google Scholar]