

Abstract
Background
Few data is available on the association between body mass index (BMI), serum uric acid (SUA) levels and blood pressure (BP) categories in the disease continuum, when efforts for its prevention may be applicable.
Methods
We performed a cross-sectional study to examine the association between BMI, SUA and BP in a community-dwelling sample of Japanese men. Individuals not on antihypertensive and uric acid lowering medications, and aged 50 to 90 years [817men aged 66 ± 9 (mean ± standard deviation) years] were recruited for the survey during a community based annual medical check-up. The main outcome was the presence of prehypertension [systolic BP (SBP) 120-139 mmHg and/or diastolic BP (DBP) 80-89 mmHg] and hypertension [SBP ≥ 140 and /or DBP ≥ 90].
Results
In participants with a BMI of < 21.0 kg/m2, increased SUA levels were positively associated with SBP and DBP, but in those with a BMI of ≥ 21.0 kg/m2, increased SUA levels were negatively associated with SBP and DBP. The interaction between BMI and SUA as well as BMI and SUA was a significant and independent determinant for both SBP (β = − 1.125, p = 0.001) and DBP (β = − 0.995, p = 0.005). Among participants, the respective prevalence of normotension, prehypertension, and hypertension was 19.5% and 53.7%, and 19.8%. The prevalence of normotension and prehypertension decreased with increasing BMI and the prevalence of hypertension increased with increasing BMI. In participants with a BMI ≥ 21.0 kg/m2, the adjusted-odds ratio of SUA for hypertension was 0.75 (95% CI, 0.59-0.95) compared with normotension and 0.82 (0.70-0.96) compared with prehypertension. In those with a BMI of < 21.0 kg/m2, these associations were not shown.
Conclusion
BMI may modify the association between SUA and blood pressure status among community-dwelling men.
Keywords: Blood pressure, Uric acid, Body mass index, Interaction, Risk factor, Community-dwelling men
Background
Hypertension is likely the most common disease in Japan and is strongly associated with an increased risk of cardiovascular disease (CVD). The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7) defined a systolic blood pressure (SBP) of 120 to 139 mmHg and/or diastolic blood pressure (DBP) 80 to 89 mmHg as prehypertension [1] based on the evidence of a modestly increasing risk of CVD among individuals with such levels [2]. Many studies demonstrated that the prehypertensive group had a higher body mass index (BMI), central obesity, a family history of hypertension, a sedentary lifestyle, eating high sodium foods, smoking, excessive alcohol intake, impaired glucose tolerance/diabetes, higher levels of blood glucose, low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG), and lower levels of high-density lipoprotein cholesterol (HDL-C) than the normotensive group [3–6]. The Jichi Medical School Cohort Study which enrolled 4706 males and 7342 females from among the general Japanese population suggested that BMI > 23.0 kg/m2 was the strongest determinant of prehypertension [7]. Thus lifestyle modification or even medical treatment is recommended for individuals with prehypertension [8].
Serum uric acid (SUA) is the end product of endogenous and dietary purine metabolism in humans, and is catalyzed by the enzyme xanthine oxidase, which is involved in producing reactive-oxygen species (ROS). Its excess accumulation can lead to various diseases [9]. SUA is closely associated with an increased risk of prehypertension [10, 11], hypertension [12], metabolic syndrome [13], and cardiovascular disease (CVD) [14, 15]. However, despite an association between serum SUA level and these conditions, SUA may not be considered a risk in these conditions [16], but rather as biologically inert or possibly anti-inflammatory because it can function as an antioxidant [17]. Increased SUA was significantly elevated in a linear manner. Moreover, increased BMI and weight loss may represent an effective nonmedical strategy for reducing SUA levels, especially in postmenopausal women and men [18]. Thus, the relationships between SUA and BP of participants categorized by BMI level may be different, and an interactive effect between BMI and SUA on blood pressure may be considered.
The aim of this study was to evaluate the prevalence of prehypertension and hypertension, and its association with BMI, SUA and other confounding factors {e.g., age, habits, lipid, fasting plasma glucose (FPG), renal function, and liver function} using cross-sectional data from community-dwelling Japanese men aged of ≥50 years.
Methods
Study population
The present study was designed as a part of the Nomura study [19]. Participants were selected through a community-based annual check-up process in a rural town located in Ehime prefecture, Japan. Baseline clinical characteristics including anthropometric parameters were obtained from the subject’s personal health records of the evaluated medical check-up. Other characteristics such as smoking and alcohol habit, medication, and history of CVD were investigated by individual interviews using a structured questionnaire. After excluding individuals with antihypertensive and UA lowering medications, the final study sample included only eligible persons (Fig. 1). This study was approved by the ethics committee of Ehime University School of Medicine, and written informed consent was obtained from each subject.
Fig. 1.
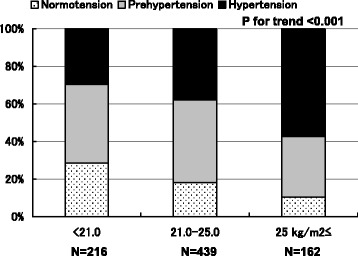
Prevalence of blood pressure status of participants categorized by body mass index. The prevalence of normotension and prehypertension decreased with increasing BMI and the prevalence of hypertension increased with increasing BMI (p < 0.001). P-value;χ2 test
Evaluation of risk factors
Information on demographic characteristics and risk factors was collected using clinical files. BMI was calculated by dividing weight (in kilograms) by the square of height (in meters). Smoking status was defined as the number of cigarette packs per day multiplied by the number of years smoked (pack year), and the participants were classified into never smokers, past smokers, light smokers (< 30 pack・year) and heavy smokers (≥30 pack・year). Daily alcohol consumption was measured using the Japanese liquor unit in which a unit corresponds to 22.9 g of ethanol, and the participants were classified into never drinkers, occasional drinkers (< 1 unit/day), light drinkers (< 2 unit/day), and heavy drinkers (≥2 unit/day). We measured SBP and DBP in the right upper arm of participants in the sedentary position using an automatic oscillometric blood pressure recorder while the participants were seated after having rested for at least 5 min. Appropriate cuff bladder size was determined at each visit based on arm circumference. Normotension was defined as not being on antihypertensive medication and having a SBP < 120 mmHg and DBP < 80 mmHg. Prehypertension was defined as not being on antihypertensive medication and having a SBP of 120 to 139 mmHg and/or DBP of 80 to 89 mmHg. Hypertension was defined as SBP ≥140 mmHg and/or DBP ≥90 mmHg (9). Total cholesterol (T-C), TG, HDL-C, FPG, creatinine (enzymatic method), SUA, aspartate transaminase (ALT), and γ-glutamyl transpeptidase (GGT) were measured during fasting. LDL-C levels were calculated by the Friedewald formula (14). Participants with TG levels ≥400 mg/dL were excluded. The presence of diabetes and CVD was defined as a history of treatment for diabetes and CVD. Estimated glomerular filtration ratio (eGFR) was calculated using CKD-EPI equations modified by a Japanese coefficient: Male, Cr ≤0.9 mg/dl, 141 × (Cr/0.9) –0.411 × 0.993 age × 0.813; Cr > 0.9 mg/dl, 141 × (Cr/0.9) –1.209 × 0.993 age × 0.813 [20].
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics Version 20 (Statistical Package for Social Science Japan, Inc., Tokyo, Japan). All values are expressed as mean ± standard deviation (SD), unless otherwise specified. Data for TG, FPG, ALT, and GGT were skewed, and are presented as median (interquartile range) values, and were log-transformed for analysis. Differences in means and prevalence among the groups were analyzed by Student’s t-test for continuous data and χ2 test for categorical data. Correlations between various characteristics and BP were determined using age-adjusted partial Pearson’s correlation test and multiple linear regression analysis. Logistic regression analyses were used to test significant factors of prehypertension and hypertension (versus normotension), with prehypertension and hypertension serving as the dichotomous outcome variables, and age, BMI, alcohol consumption, smoking status, history of CVD, lipids, antilipidemic medication, FPG, antidiabetic medication, SUA, eGFR, ALT, and GGT as the confounding factors. The synergistic effect of BMI and SUA levels on blood pressure was evaluated using a general linear model. A value of p < 0.05 was considered significant.
Results
The participants comprised 817 men aged 66 ± 9 years (range, 50-90) who do not take antihypertensive and UA lowering medications. Mean BMI in the study sample was 22.9 kg/m2 (SD, 2.8), with 26.4% being underweight (BMI < 21.0 kg/m2), 53.7% normal weight (BMI, 21.0 to 24.9 kg/m2), 19.8% overweight or obese (BMI ≥25 kg/m2). Table 1 shows the background characteristics of participants categorized by BMI. BMI, SBP, DBP, TG, LDL-C, prevalence of antilipidemic medication, FPG, SUA, ALT, and GGT were significantly high in the high BMI group, but HDL-C was low in the low BMI group. There were no inter-group differences regarding prevalence of alcohol consumption, smoking status, history of CVD, prevalence of antidiabetic medication, and eGFR.
Table 1.
Characteristics of participants categorized by body mass index
| Body mass index category (kg/m2) | ||||
|---|---|---|---|---|
| Characteristics N = 817 | < 21.0 | 21.0-24.9 | ≥25.0 | P-value |
| N = 216 | N = 439 | N = 162 | ||
| Age (years) | 67 ± 9 | 67 ± 9 | 63 ± 9 | < 0.001 |
| Body mass index (kg/m2) | 19.5 ± 1.1 | 23.0 ± 1.1 | 27.0 ± 2.0 | < 0.001 |
| Alcohol consumptiona (%) | 37.0/20.8/9.3/32.9 | 42.6/21.9/9.1/26.4 | 34.6/30.2/7.4/27.8 | 0.157 |
| Smoking statusb (%) | 25.5/30.6/25.9/18.1 | 25.1/27.6/26.4/21.0 | 23.5/28.4/24.7/23.5 | 0.910 |
| History of CVD, N (%) | 16 (7.4) | 41 (9.3) | 11 (6.8) | 0.514 |
| Systolic blood pressure (mmHg) | 132 ± 21 | 136 ± 19 | 142 ± 18 | < 0.001 |
| Diastolic blood pressure (mmHg) | 79 ± 11 | 82 ± 10 | 85 ± 11 | < 0.001 |
| Triglycerides (mg/dL) | 79 (59-101) | 95 (72-141) | 119 (81-161) | < 0.001 |
| HDL cholesterol (mg/dL) | 67 ± 17 | 58 ± 15 | 53 ± 13 | < 0.001 |
| LDL cholesterol (mg/dL) | 103 ± 28 | 114 ± 30 | 115 ± 33 | < 0.001 |
| Antilipidemic medication, N (%) | 3 (1.4) | 25 (5.7) | 9 (5.6) | 0.035 |
| Fasting plasma glucose (mg/dL) | 98 (91-114) | 102 (93-117) | 103 (94-120) | 0.042 |
| Antiidiabetic medication, N (%) | 6 (2.8) | 28 (6.4) | 8 (4.9) | 0.145 |
| Serum uric acid (mg/dL) | 5.3 ± 1.2 | 5.7 ± 1.3 | 5.9 ± 1.2 | < 0.001 |
| eGFR (ml/min./1.73m2) | 79.8 ± 13.9 | 77.0 ± 14.3 | 78.6 ± 15.3 | 0.051 |
| Aspartate transaminase (IU/L) | 17 (14-23) | 19 (15-25) | 23 (17-32) | < 0.001 |
| γ-glutamyl transpeptidase (IU/L) | 29 (20-43) | 30 (22-49) | 44 (28-69) | < 0.001 |
Data for triglycerides, fasting plasma glucose, aspartate transaminase, and γ-glutamyl transpeptidase were skewed and are presented as median (interquartile range) values, and were log-transformed for analysis. P-value: Student’s t-test for continuous variables or the χ2 -test for categorical variables. Bolded numbers indicate significance
CVD cardiovascular disease, HDL high-density lipoprotein, LDL low-density lipoprotein, eGFR estimated glomerular filtration rate. Data presented are mean ± standard deviation
aDaily alcohol consumption was measured using the Japanese liquor unit in which a unit corresponds to 22.9 g of ethanol, and the participants were classified into never, occasional, light daily (< 2 unit/day), and heavy daily drinkers (≥ 2 unit/day)
bSmoking status [never-smoker, past-smoker, light smoker (< 30 pack · year), and heavy smoker (≥ 30 pack · year)]
Among them, the respective prevalence of normotension, prehypertension, and hypertension was 19.5% and 53.7%, and 19.8%. The prevalence of normotension and prehypertension decreased with increasing BMI and the prevalence of hypertension increased with increasing BMI (Fig. 1).
In addition to their direct associations, we observed a synergistic effect between BMI category and SUA levels on BP status in Fig. 2. In BMI < 21.0 kg/m2, SUA correlated positively with both SBP and DBP (r = 0.112, p = 0.100 and r = 0.163, p = 0.016, respectively), but in BMI ≥25.0 kg/m2, SUA correlated negatively with both SBP and DBP (r = − 0.178, p = 0.023 and r = − 0.064, p = 0.421, respectively). Analysis of covariance showed that three regression lines in each graph were significantly different (SBP, F = 8.139, p = 0.004 and DBP, F = 5.199, p = 0.023, respectively).
Fig. 2.
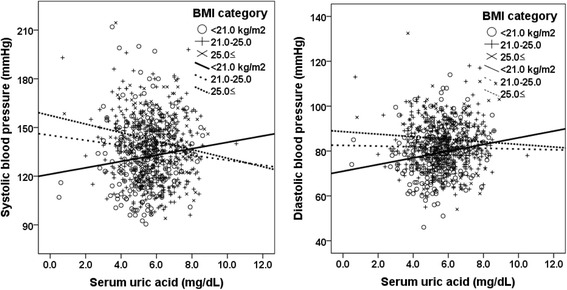
Correlation between serum uric acid and blood pressure status of participants categorized by body mass index. In body mass index (BMI) < 21.0 kg/m2, serum uric acid correlated positively with both systolic blood pressure (SBP) and diastolic blood pressure (DBP) (r = 0.112, p = 0.100 and r = 0.163, p = 0.016, respectively), but in BMI ≥21.0 kg/m2 serum uric acid correlated negatively with both SBP and DBP (BMI 21-25 kg/m2, r = − 0.108, p = 0.024 and r = − 0.022, p = 0.651; BMI ≥25.0 kg/m2, r = − 0.178, p = 0.023 and r = − 0.064, p = 0.421, respectively). Analysis of covariance showed that three regression lines in each graph were significantly different (SBP, F = 8.139, P = 0.004 and DBP, F = 5.199, P = 0.023, respectively)
Table 2 shows the background characteristics of participants categorized by BMI (i.e., < 21.0 kg/m2 and ≥21.0 kg/m2) and blood pressure status. In hypertensive group with a BMI < 21.0 kg/m2, prevalence of smoking status and GGT were significantly higher than normotensive group. In hypertensive group with a BMI ≥21.0 kg/m2, age and BMI as well as smoking status and GGT were also significantly higher, but SUA was significantly lower than normotensive group.
Table 2.
Characteristics of participants categorized by body mass index and blood pressure status
| Body mass index < 21.0 kg/m2 N = 216 | Body mass index ≥21.0 kg/m2 N = 601 | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Normotension | Prehypertension | Hypertension | P-value | Normotension | Prehypertension | Hypertension | P-value |
| N = 817 | N = 62 | N = 90 | N = 64 | N = 97 | N = 245 | N = 259 | ||
| Age (years) | 65 ± 10 | 69 ± 9 | 68 ± 8 | 0.083 | 63 ± 8 | 67 ± 9 | 66 ± 9 | 0.002 |
| Body mass index (kg/m2) | 19.4 ± 1.0 | 19.6 ± 1.1 | 19.6 ± 1.1 | 0.341 | 23.6 ± 2.1 | 23.7 ± 2.1 | 24.5 ± 2.4 | < 0.001 |
| Alcohol consumption (%) | 40.3/21.0/11.2/27.4 | 34.4/27.8/10.0/27.8 | 37.5/10.9/6.3/45.3 | 0.099 | 43.3/19.6/10.3/26.8 | 37.1/27.3/8.6/26.9 | 42.5/22.8/8.1/26.6 | 0.731 |
| Smoking status (%) | 30.6/37.1/21.0/11.3 | 26.7/28.9/32.2/12.2 | 18.8/26.6/21.9/32.8 | 0.011 | 22.7/30.9/25.8/20.6 | 30.6/30.2/22.4/16.7 | 19.7/24.3/29.3/26.6 | 0.012 |
| History of CVD, N (%) | 3 (4.8) | 10 (11.1) | 3 (4.7) | 0.214 | 6 (6.2) | 28 (11.4) | 18 (6.9) | 0.130 |
| Triglycerides (mg/dL) | 79 (57-97) | 79 (63-100) | 80 (62-108) | 0.266 | 110 (74-151) | 99 (74-144) | 100 (72-146) | 0.997 |
| HDL cholesterol (mg/dL) | 68 ± 17 | 64 ± 16 | 70 ± 18 | 0.110 | 55 ± 16 | 57 ± 15 | 58 ± 14 | 0.278 |
| LDL cholesterol (mg/dL) | 101 ± 27 | 102 ± 28 | 108 ± 31 | 0.327 | 118 ± 29 | 114 ± 30 | 114 ± 33 | 0.396 |
| Antilipidemic medication, N (%) | 0 | 2 (2.2) | 1 (1.6) | 0.511 | 6 (6.2) | 17 (6.9) | 11 (4.2) | 0.413 |
| Fasting plasma glucose (mg/dL) | 95 (89-111) | 97 (89-112) | 102 (94-120) | 0.213 | 102 (92-116) | 103 (91-117) | 102 (94-120) | 0.141 |
| Antiidiabetic medication, N (%) | 4 (6.5) | 0 | 2 (3.1) | 0.058 | 3 (3.1) | 18 (7.3) | 15 (5.8) | 0.322 |
| Serum uric acid (mg/dL) | 5.1 ± 1.1 | 5.4 ± 1.3 | 5.6 ± 1.2 | 0.059 | 6.0 ± 1.1 | 5.8 ± 1.3 | 5.6 ± 1.3 | 0.044 |
| eGFR (ml/min./1.73m2) | 81.0 ± 14.8 | 78.3 ± 12.9 | 80.9 ± 14.4 | 0.372 | 76.8 ± 13.4 | 76.4 ± 14.5 | 78.5 ± 15.1 | 0.252 |
| Aspartate transaminase (IU/L) | 19 (15-24) | 17 (13-22) | 18 (14-24) | 0.102 | 18 (15-24) | 20 (15-26) | 20 (16-27) | 0.084 |
| γ-glutamyl transpeptidase (IU/L) | 27 (20-37) | 27 (19-38) | 35 (21-64) | 0.004 | 29 (21-43) | 34 (22-50) | 36 (25-65) | < 0.001 |
Data for triglycerides, fasting plasma glucose, aspartate transaminase, and γ-glutamyl transpeptidase were skewed and were log-transformed for analysis. P-value: Student’s t-test for continuous variables or the χ2 -test for categorical variables. Bolded numbers indicate significance
Table 3 shows the relationship between various characteristics and blood pressure status of participants categorized by BMI. Age-adjusted partial Pearson’s correlation coefficient showed that SUA correlated positively with both SBP and DBP in participants with a BMI < 21.0 kg/m2 but correlated negatively with SBP in participants with a BMI ≥21.0 kg/m2.
Table 3.
Age-adjusted relationship between various characteristics and blood pressure status of participants categorized by body mass index
| Body mass index < 21.0 kg/m2 N = 216 | Body mass index ≥21.0 kg/m2 N = 601 | |||
|---|---|---|---|---|
| Systolic blood pressure | Diastolic blood pressure | Systolic blood pressure | Diastolic blood presure | |
| Characteristics N = 817 | Partial r (P-value) | Partial r (P-value) | Partial r (P-value) | Partial r (P-value) |
| Body mass index | 0.105 (0.127) | 0.093 (0.174) | 0.190 (< 0.001) | 0.153 (< 0.001) |
| Alcohol consumption | 0.137 (0.044) | 0.107 (0.119) | −0.008 (0.844) | −0.030 (0.469) |
| Smoking status | 0.205 (0.003) | 0.245 (< 0.001) | 0.142 (< 0.001) | 0.156 (< 0.001) |
| History of CVD (Yes = 1, No = 0) | −0.061 (0.371) | −0.020 (0.766) | − 0.051 (0.216) | − 0.051 (0.209) |
| Triglycerides | 0.047 (0.489) | 0.112 (0.100) | 0.031 (0.446) | 0.064 (0.116) |
| HDL cholesterol | 0.078 (0.255) | 0.081 (0.240) | 0.054 (0.186) | 0.061 (0.138) |
| LDL cholesterol | −0.027 (0.689) | 0.057 (0.404) | −0.019 (0.643) | 0.000 (0.994) |
| Antilipidemic medication (Yes = 1, No = 0) | 0.068 (0.318) | 0.018 (0.791) | −0.098 (0.017) | −0.040 (0.334) |
| Fasting plasma glucose | 0.138 (0.043) | 0.059 (0.392) | 0.113 (0.005) | 0.029 (0.476) |
| Antiidiabetic medication (Yes = 1, No = 0) | −0.056 (0.410) | −0.064 (0.349) | 0.007 (0.871) | −0.051 (0.214) |
| Serum uric acid | 0.134 (0.049) | 0.153 (0.025) | −0.095 (0.020) | −0.034 (0.401) |
| Estimated GFR | 0.184 (0.007) | 0.083 (0.223) | 0.083 (0.041) | 0.015 (0.719) |
| Aspartate transaminase | 0.001 (0.983) | 0.007 (0.917) | 0.084 (0.040) | 0.080 (0.051) |
| γ-glutamyl transpeptidase | 0.184 (0.007) | 0.240 (< 0.001) | 0.171 (< 0.001) | 0.202 (< 0.001) |
r, Pearson’s partial correlation coefficients adjusted for age. Data for triglycerides, fasting plasma glucose, aspartate transaminase, and γ-glutamyl transpeptidase were skewed and were log-transformed for analysis. Bolded numbers indicate significance
Table 4 shows multivariate-adjusted relationship between various characteristics and blood pressure status of participants categorized by BMI. Multiple linear regression analysis showed that SUA was significantly and positively associated with both SBP and DBP in participants with a BMI < 21.0 kg/m2, but negatively associated with both SBP and DBP in participants with a BMI ≥21.0 kg/m2, independently of other confounding factors.
Table 4.
Multivariate-adjusted relationship between various characteristics and blood pressure status of participants categorized by body mass index
| Body mass index category < 21.0 kg/m2 N = 216 | Body mass index category ≥ 21.0 kg/m2 N = 601 | |||
|---|---|---|---|---|
| Systolic blood pressure | Diastolic blood pressure | Systolic blood pressure | Diastolic blood pressure | |
| Characteristics N = 817 | β(P-value)§ | β(P-value)§ | β(P-value)§ | β(P-value)§ |
| Age | 0.375 (< 0.001) | 0.065 (0.396) | 0.275 (< 0.001) | −0.045 (0.332) |
| Body mass index | – | – | 0.175 (< 0.001) | 0.141 (0.001) |
| Alcohol consumption | 0.124 (0.064) | – | – | −0.046 (0.247) |
| Smoking status | 0.175 (0.010) | 0.182 (0.014) | 0.114 (0.006) | 0.102 (0.020) |
| History of CVD (Yes = 1, No = 0) | – | – | – | −0.042 (0.307) |
| Triglycerides | – | – | – | 0.064 (0.167) |
| HDL cholesterol | – | – | – | 0.083 (0.067) |
| LDL cholesterol | – | 0.162 (0.018) | – | – |
| Antilipidemic medication (Yes = 1, No = 0) | – | – | − 0.090 (0.020) | – |
| Fasting plasma glucose | 0.151 (0.020) | 0.087 (0.197) | 0.088 (0.024) | – |
| Antiidiabetic medication (Yes = 1, No = 0) | – | − 0.060 (0.370) | – | −0.041 (0.302) |
| Serum uric acid | 0.178 (0.011) | 0.155 (0.028) | −0.127 (0.001) | −0.102 (0.019) |
| Estimated GFR | 0.272 (< 0.001) | 0.170 (0.030) | – | − 0.036 (0.429) |
| Aspartate transaminase | – | − 0.086 (0.243) | – | – |
| γ-glutamyl transpeptidase | – | 0.243 (0.002) | 0.124 (0.007) | 0.157 (0.001) |
| R2 | 0.167 (< 0.001) | 0.163 (< 0.001) | 0.127 (< 0.001) | 0.084 (< 0.001) |
Only factors remained in the final model were shown. Data for triglycerides, fasting plasma glucose, aspartate transaminase, and γ-glutamyl transpeptidase were skewed and were log-transformed for analysis. Bolded numbers indicate significance
β standard coefficient, R2 coefficient of determination
§Multivariate adjusted for all confounding factors in Table 1 by multiple linear regression analysis using backward elimination method
We assessed the statistical significance of the synergistic relationship using a general linear model with the following confounding factors: age, BMI, alcohol consumption, smoking status, history of CVD, TG, HDL-C, LDL-C, prevalence of antilipidemic medication, FPG, prevalence of antidiabetic medication, SUA, eGFR, ALT, GGT, and the interaction between BMI and SUA (Table 5). The interaction between increased BMI and SUA as well as BMI and SUA were significant and independent determinants for SBP (β = − 1.125, p = 0.001) and DBP (β = − 0.995, P = 0.005), independently of other confounding factors.
Table 5.
Interaction between body mass index and uric acid on blood pressure status
| Systolic blood pressure | Diastolic blood pressure | |
|---|---|---|
| Characteristics N = 817 | β(P-value)§ | β(P-value)§ |
| Age | 0.294 (< 0.001) | – |
| Body mass index | 0.715 (< 0.001) | 0.620 (< 0.001) |
| Smoking status | 0.117 ((0.001) | 0.137 (< 0.001) |
| LDL cholesterol | – | 0.057 (0.096) |
| Fasting plasma glucose | 0.092 (0.006) | – |
| Serum uric acid | 0.881 (0.002) | 0.776 (0.008) |
| Estimated GFR | 0.092 (0.016) | – |
| γ-glutamyl transpeptidase | 0.119 (0.002) | 0.178 (< 0.001) |
| Body mass indexa serum uric acid | −1.125 (0.001) | −0.995 (0.005) |
| R2 | 0.148 (< 0.001) | 0.118 (0 < 0.001) |
Data for fasting plasma glucose, triglycerides, aspartate transaminase, and γ-glutamyl transpeptidase were skewed and were log-transformed for analysis. Bolded numbers indicate significance
β standard coefficient, R2 coefficient of determination
§Multivariate adjusted for all confounding factors in Table 1 by multiple linear regression analysis using backward elimination method. Only factors remained in the final model were shown
aInteraction between body mass index and serum uric acid
Table 6 shows the odds ratios (ORs) {95% confidence interval (CI)} of SUA for blood pressure status of participants categorized by BMI. In participants with a BMI ≥21.0 kg/m2, the odds ratio of SUA for hypertension was 0.75 (95% CI, 0.59-0.95) compared with normotension, and 0.82 (0.70-0.96) for hypertension compared with prehypertension. In subjects with a BMI < 21.0 kg/m2, these associations were not shown.
Table 6.
Association between serum uric acid levels and blood pressure status of participants categorized by body mass index
| Characteristic N = 817 | Body mass index < 21.0 kg/m2 | Body mass index ≥21.0 kg/m2 | P-interaction | ||||
|---|---|---|---|---|---|---|---|
| N = 216 | OR (95% CI) | P-value § | N = 601 | OR (95% CI) | P-value § | ||
| Prehypertension VS Normotension | |||||||
| Serum uric acid | 90/62 | 1.25 (0.91-1.72) | 0.168 | 245/97 | 0.95 (0.77-1.18) | 0.650 | 0.073 |
| Hypertension VS Normotension | |||||||
| Serum uric acid | 64/62 | 1.53 (0.99-2.38) | 0.058 | 259/97 | 0.75 (0.59-0.95) | 0.018 | 0.004 |
| Hypertension VS Prehypertension | |||||||
| Serum uric acid | 64/90 | 1.26 (0.92-1.74) | 0.149 | 259/245 | 0.82 (0.70-0.96) | 0.012 | 0.077 |
Data for fasting plasma glucose and γ-glutamyl transpeptidase were skewed and log-transformed for analysis. Bolded numbers indicate significance
OR odds ratio, CI confidence interval, VS versus
§Multivariate adjusted for age, body mass index, smoking status, LDL cholesterol, prevalence of antilipidemic medication, fasting plasma glucose, Estimated GFR, and γ-glutamyl transpeptidase, which were significant in Table 4
Discussion
In this cross-sectional, population-based study of 817 middle-aged and elderly men, we set out to determine the prevalence of prehypertension and hypertension, as defined by the JNC-7 criteria [1], and its association with BMI and SUA. This study showed that increased SUA levels were positively associated with SBP and DBP in participants with a BMI < 21.0 kg/m2, but negatively in those with a BMI ≥21.0 kg/m2. The effect of significant interaction between BMI and SUA on blood pressure indicated that increased SUA was a risk factor for elevated blood pressure in underweight participants, but was not a predictor among normal- or overweight participants. To our knowledge, few studies have indicated that BMI may modify the association between SUA and blood pressure status.
In men aged < 40 years, SUA was significantly associated with SBP (β = 0.25, p = 0.002) and DBP (β = 0.41, p < 0.001) after adjustment for age, diabetes, dyslipidemia, BMI, and eGFR, but the association was not significant in those ≥60 years [21]. From a meta-analysis of 25 studies with 97,824 participants assessing the association between UA and incident hypertension, it was suggested that hyperuricemia may modestly increase the risk of hypertension incidence [22]. From a meta-analysis of 18 prospective cohort studies representing data from 55,607 participants, it was shown that hyperuricemia is associated with an increased risk for incident hypertension, independent of traditional hypertension risk factors. This risk appears to be more pronounced in younger individuals and women [12]. Thus, one can suggest that hyperuricemia-related pathogenetic mechanisms may be more dominant in earlier stages of hypertension than later stages when salt-sensitivity becomes apparent [12]. Our study findings indicate that we should consider the effect of BMI as well as age on the relationship between SUA and blood pressure.
The mechanism whereby BMI may modify the association between SUA and blood pressure status are not completely understood. SUA induces endothelial cell dysfunction via nitric oxide (NO) synthetase [23] and directly involves stimulation of the renin-angiotensin system [24]. SUA alters the proliferation/migration of endothelial and vascular smooth muscle cells [25]. These findings may provide insight into a pathogenic mechanism by which UA may induce hypertension and vascular disease [26]. A recent rodent model with induced hyperuricemia demonstrated that UA might have a pathogenic role in the development of renal afferent arteriolopathy and tubulointerstitial disease, leading to hypertension [27]. The renal lesions and the development of hypertension were prevented by lowering UA levels with allopurinol or benziodarone, which inhibits xanthine oxidase and hence blocks both UA and oxidant formation, which are reversed by angiotensin-converting enzyme inhibition [28].
Moreover, SUA also reflects systemic inflammation [29], oxidative stress [30] and is more strongly associated with insulin resistance [31, 32] and other cardiovascular risk factors such as BMI, BP, T-C, HDL-C, TG, and FPG [31, 33]. Increased BMI is also significantly associated with various CVD risk factors. These risk factors cause endothelial dysfunction [34], the loss of vasomotor reactivity [35] and arterial stiffness [36]. Such pathophysiology induced by increased BMI may be greater than that of SUA. Thus, SUA could not be an independent risk factor for increased SBP in participants with a BMI ≥21.0 kg/m2. We suggest that SUA may be more important in participants with a BMI < 21.0 kg. It has been demonstrated that increased SUA induces increased BP that is initially reversible but leads to an irreversible salt-sensitive hypertension over time [37]. Thus, SUA identification is important for risk assessment and treatment of such patients with a BMI < 21.0 kg.
An important observation was that UA may function as an antioxidant, and possibly one of the most important antioxidants in plasma. Increased SUA in subjects with CVD might therefore reflect a compensatory mechanism to counter the oxidative stress that occurs in these conditions [38]. In our study, SUA was negatively associated with hypertension in participants with a BMI ≥21.0 kg/m2. The beneficial antioxidant actions of SUA may partially counter its potential detrimental effects. It is interesting that almost all studies examining the relation of SUA levels with CVD events show a J-shaped curve with the nadir of risk in the second quartile [39, 40].
Some limitations of this study must be considered. First, our cross-sectional study design does not eliminate potential causal relationships between BMI, SUA, and blood pressure status. Second, the prevalence of blood pressure categories is based on single blood pressure measurement. Third, confounding factors are based on a single assessment of blood, which may introduce a misclassification bias. Fourth, we could not eliminate the possible effects of underlying diseases and medications for diabetes and dyslipidemia on the present findings. We could not rule out one-time prehypertension and white-coat prehypertension. Finally, in this study, the demographics and referral source may limit the generalization of the results.
Conclusion
The present study showed that BMI may modify the association between SUA, SBP, and DBP. The underlying mechanism seems to be independent from traditional cardiovascular risk factors such as age, BMI, alcohol consumption, smoking status, history of CVD, lipids, diabetes, renal function, and liver function. For community-dwelling healthy persons, prospective population-based studies are needed to investigate the mechanisms underlying this association to determine whether intervention, such as effective lifestyle modifications that decrease BMI and SUA, in adult populations will decrease risks.
Acknowledgements
This work was supported in part by a grant-in-aid for Scientific Research from the Foundation for Development of Community (2017)
Funding
This work was supported in part by a grant-in-aid from the Foundation for Development of Community (2017).
Availability of data and materials
Not applicable.
Authors’ contributions
RK participated in the design of the study, performed the statistical analysis and drafted the manuscript. RK DN, SK, and TeK contributed to the acquisition and interpretation of data. RK, DN, and TeK contributed to the conception and design of the statistical analysis. All authors read and approved the manuscript.
Ethics approval and consent to participate
This study was approved by the ethics committee of Ehime University School of Medicine, and written informed consent was obtained from each subject.
Consent for publication
The author has given all rights for this manuscript to the publisher.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Ryuichi Kawamoto, Phone: +81-894-72-0180, Email: rykawamo@m.ehime-u.ac.jp.
Daisuke Ninomiya, Email: 98065dn@jichi.ac.jp.
Kensuke Senzaki, Email: p401057b@icloud.com.
Teru Kumagi, Email: terukuma@m.ehime-u.ac.jp.
References
- 1.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee: the seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206–1252. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 2.Gu D, Chen J, Wu X, Duan X, Jones DW, Huang JF, et al. Prehypertension and risk of cardiovascular disease in Chinese adults. J Hypertens. 2009;27(4):721–729. doi: 10.1097/HJH.0b013e328323ad89. [DOI] [PubMed] [Google Scholar]
- 3.Kawamoto R, Kohara K, Tabara Y, Miki T. High prevalence of prehypertension is associated with the increased body mass index in community-dwelling Japanese. Tohoku J Exp Med. 2008;216(4):353–361. doi: 10.1620/tjem.216.353. [DOI] [PubMed] [Google Scholar]
- 4.Isezuo SA, Sabir AA, Ohwovorilole AE, Fasanmade OA. Prevalence, associated factors and relationship between prehypertension and hypertension: a study of two ethnic African populations in northern Nigeria. J Hum Hypertens. 2011;25(4):224–230. doi: 10.1038/jhh.2010.56. [DOI] [PubMed] [Google Scholar]
- 5.Zhang W, Li N. Prevalence, risk factors, and management of prehypertension. Int J Hypertens. 2011;2011:605359. doi: 10.4061/2011/605359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kawamoto R, Tabara Y, Kohara K, Miki T, Abe M, Kusunoki T. Increased high-density lipoprotein cholesterol is associated with a high prevalence of pre-hypertension and hypertension in community-dwelling persons. Endocrine. 2012;42(2):321–328. doi: 10.1007/s12020-012-9625-z. [DOI] [PubMed] [Google Scholar]
- 7.Ishikawa Y, Ishikawa J, Ishikawa S, Kayaba K, Nakamura Y, Shimada K, et al. Jichi medical school cohort investigators group. Hypertens Res. 2008;31(7):1323–1330. doi: 10.1291/hypres.31.1323. [DOI] [PubMed] [Google Scholar]
- 8.Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi: 10.1016/S0140-6736(02)11911-8. [DOI] [PubMed] [Google Scholar]
- 9.Jin M, Yang F, Yang I, Yin Y, Luo JJ, Wang H, et al. Uric acid, hyperuricemia and vascular diseases. Front Biosci (Landmark Ed) 2012;17:656–669. doi: 10.2741/3950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bao X, Wang Q, Chen G, Wang Q, Liang R, Zhang S. Serum concentration of uric acid associated with prehypertension among Chinese population. Angiology. 2014;65(9):800–805. doi: 10.1177/0003319713507628. [DOI] [PubMed] [Google Scholar]
- 11.Jiang M, Gong D, Fan Y. Serum uric acid levels and risk of prehypertension: a meta-analysis. Clin Chem Lab Med. 2017;55(3):314–321. doi: 10.1515/cclm-2016-0339. [DOI] [PubMed] [Google Scholar]
- 12.Grayson PC, Kim SY, LaValley M, Choi HK. Hyperuricemia and incident hypertension: a systematic review and meta-analysis. Arthritis Care Res (Hoboken) 2011;63(1):102–110. doi: 10.1002/acr.20344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yuan H, Yu C, Li X, Sun L, Zhu X, Zhao C, et al. Serum uric acid levels and risk of metabolic syndrome: a dose-response meta-analysis of prospective studies. J Clin Endocrinol Metab. 2015;100(11):4198–4207. doi: 10.1210/jc.2015-2527. [DOI] [PubMed] [Google Scholar]
- 14.Zhao G, Huang L, Song M, Song Y. Baseline serum uric acid level as a predictor of cardiovascular disease related mortality and all-cause mortality: a meta-analysis of prospective studies. Atherosclerosis. 2013;231(1):61–68. doi: 10.1016/j.atherosclerosis.2013.08.023. [DOI] [PubMed] [Google Scholar]
- 15.Puddu PE, Bilancio G, Terradura Vagnarelli O, Lombardi C, Mancini M, Zanchetti A, et al. Serum uric acid and eGFR_CKDEPI differently predict long-term cardiovascular events and all causes of deaths in a residential cohort. Int J Cardiol. 2014;171(3):361–367. doi: 10.1016/j.ijcard.2013.12.029. [DOI] [PubMed] [Google Scholar]
- 16.Lu Z, Dong B, Wu H, Chen T, Zhang Y, Wu J, et al. Serum uric acid level in primary hypertension among Chinese nonagenarians/centenarians. J Hum Hypertens. 2009;23(2):113–121. doi: 10.1038/jhh.2008.104. [DOI] [PubMed] [Google Scholar]
- 17.Glantzounis GK, Tsimoyiannis EC, Kappas AM, Galaris DA. Uric acid and oxidative stress. Curr Pharm Des. 2005;11(32):4145–4151. doi: 10.2174/138161205774913255. [DOI] [PubMed] [Google Scholar]
- 18.Ishizaka N, Ishizaka Y, Toda A, Tani M, Koike K, Yamakado M, et al. Changes in waist circumference and body mass index in relation to changes in serum uric acid in Japanese individuals. J Rheumatol. 2010;37(2):410–416. doi: 10.3899/jrheum.090736. [DOI] [PubMed] [Google Scholar]
- 19.Kawamoto R, Ninomiya D, Kasai Y, Kusunoki T, Ohtsuka N, Kumagi T, et al. Handgrip strength is associated with metabolic syndrome among middle-aged and elderly community-dwelling persons. Clin Exp Hypertens. 2016;38(2):245–251. doi: 10.3109/10641963.2015.1081232. [DOI] [PubMed] [Google Scholar]
- 20.Horio M, Imai E, Yasuda Y, Watanabe T, Matsuo S. Modification of the CKD epidemiology collaboration (CKD-EPI) equation for Japanese: accuracy and use for population estimates. Am J Kidney Dis. 2010;56(1):32–38. doi: 10.1053/j.ajkd.2010.02.344. [DOI] [PubMed] [Google Scholar]
- 21.Lee JJ, Ahn J, Hwang J, Han SW, Lee KN, Kim JB, et al. Relationship between uric acid and blood pressure in different age groups. Clin Hypertens. 2015;21:14. doi: 10.1186/s40885-015-0022-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wang J, Qin T, Chen J, Li Y, Wang L, Huang H, et al. Hyperuricemia and risk of incident hypertension: a systematic review and meta-analysis of observational studies. PLoS One. 2014;9(12):e114259. doi: 10.1371/journal.pone.0114259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Maxwell AJ, Bruinsma KA. Uric acid is closely linked to vascular nitric oxide activity. Evidence for mechanism of association with cardiovascular disease. J Am Coll Cardiol. 2001;38(7):1850–1858. doi: 10.1016/S0735-1097(01)01643-6. [DOI] [PubMed] [Google Scholar]
- 24.Yu MA, Sánchez-Lozada LG, Johnson RJ, Kang DH. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J Hypertens. 2010;28(6):1234–1242. [PubMed] [Google Scholar]
- 25.Kang DH, Park SK, Lee IK, Johnson RJ. Uric acid-induced C-reactive protein expression: implication on cell proliferation and nitric oxide production of human vascular cells. J Am Soc Nephrol. 2005;16(12):3553–3562. doi: 10.1681/ASN.2005050572. [DOI] [PubMed] [Google Scholar]
- 26.Khosla UM, Zharikov S, Finch JL, Nakagawa T, Roncal C, Mu W, et al. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005;67(5):1739–1742. doi: 10.1111/j.1523-1755.2005.00273.x. [DOI] [PubMed] [Google Scholar]
- 27.Johnson RJ, Kang DH, Feig D, Kivlighn S, Kanellis J, Watanabe S, et al. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension. 2003;41(6):1183–1190. doi: 10.1161/01.HYP.0000069700.62727.C5. [DOI] [PubMed] [Google Scholar]
- 28.Mazzali M, Hughes J, Kim YG, Jefferson JA, Kang DH, Gordon KL, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. 2001;38(5):1101–1106. doi: 10.1161/hy1101.092839. [DOI] [PubMed] [Google Scholar]
- 29.Lyngdoh T, Marques-Vidal P, Paccaud F, Preisig M, Waeber G, Bochud M, et al. Elevated serum uric acid is associated with high circulating inflammatory cytokines in the population-based Colaus study. PLoS One. 2011;6(5):e19901. doi: 10.1371/journal.pone.0019901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Park JH, Jin YM, Hwang S, Cho DH, Kang DH, Jo I. Uric acid attenuates nitric oxide production by decreasing the interaction between endothelial nitric oxide synthase and calmodulin in human umbilical vein endothelial cells: a mechanism for uric acid-induced cardiovascular disease development. Nitric Oxide. 2013;32:36–42. [DOI] [PubMed]
- 31.Vuorinen-Markkola H, Yki-Järvinen H. Hyperuricemia and insulin resistance. J Clin Endocrinol Metab. 1994;78(1):25–29. doi: 10.1210/jcem.78.1.8288709. [DOI] [PubMed] [Google Scholar]
- 32.Kawamoto R, Tabara Y, Kohara K, Miki T, Kusunoki T, Takayama S, et al. Usefulness of combining serum uric acid and high-sensitivity C-reactive protein for risk stratification of patients with metabolic syndrome in community-dwelling women. Endocrine. 2013;44(1):132–139. doi: 10.1007/s12020-013-9912-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cigolini M, Targher G, Tonoli M, Manara F, Muggeo M, De Sandre G. Hyperuricaemia: relationships to body fat distribution and other components of the insulin resistance syndrome in 38-year-old healthy men and women. Int J Obes Relat Metab Disord. 1995;19(2):92–96. [PubMed] [Google Scholar]
- 34.Jagla A, Schrezenmeir J. Postprandial triglycerides and endothelial function. Exp Clin Endocrinol Diabetes. 2001;109(4):S533–S547. doi: 10.1055/s-2001-15116. [DOI] [PubMed] [Google Scholar]
- 35.Lundman P, Eriksson M, Schenck-Gustafsson K, Karpe F, Tornvall P. Transient triglyceridemia decreases vascular reactivity in young, healthy men without risk factors for coronary heart disease. Circulation. 1997;96(10):3266–3268. doi: 10.1161/01.CIR.96.10.3266. [DOI] [PubMed] [Google Scholar]
- 36.Yao WM, Zhang HF, Zhu ZY, Zhou YL, Liang NX, Xu DJ, et al. Genetically elevated levels of circulating triglycerides and brachial-ankle pulse wave velocity in a Chinese population. J Hum Hypertens. 2013;27(4):265–270. doi: 10.1038/jhh.2012.23. [DOI] [PubMed] [Google Scholar]
- 37.Watanabe S, Kang DH, Feng L, Nakagawa T, Kanellis J, Lan H, et al. Uric acid, hominoid evolution, and the pathogenesis of salt-sensitivity. Hypertension. 2002;40(3):355–360. doi: 10.1161/01.HYP.0000028589.66335.AA. [DOI] [PubMed] [Google Scholar]
- 38.Nieto FJ, Iribarren C, Gross MD, Comstock GW, Cutler RG. Uric acid and serum antioxidant capacity: a reaction to atherosclerosis? Atherosclerosis. 2000;148(1):131–139. doi: 10.1016/S0021-9150(99)00214-2. [DOI] [PubMed] [Google Scholar]
- 39.Iribarren C, Sharp DS, Curb JD, Yano K. High uric acid: a metabolic marker of coronary heart disease among alcohol abstainers? J Clin Epidemiol. 1996;49(6):673–678. doi: 10.1016/0895-4356(96)00034-0. [DOI] [PubMed] [Google Scholar]
- 40.Fang J, Alderman MH. Serum uric acid and cardiovascular mortality: the NHANES I epidemiologic follow-up study, 1971–1992. JAMA. 2000;283(18):2404–2410. doi: 10.1001/jama.283.18.2404. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.