

Abstract
Purpose:
The purpose of this study is to describe the epidemiological profile, histopathological features, and outcomes of patients diagnosed with renal cell carcinoma (RCC) in a tertiary referral center over 10 years.
Methodology:
This is a retrospective cohort of 219 Saudi patients diagnosed with RCC between June 2003 and May 2013. The variables collected included the sociodemographic details and clinical presentation. The histopathological features investigated include the tumors histological subtype, pathologic staging tumor, node, and metastasis descriptors, and lymph-vascular invasion. Patients were followed until May 2013. Bivariable analysis was calculated using Chi-square test, with level of significance set at P < 0.05. Kaplan–Meier estimate was used to calculate the survival rate.
Results:
The mean age of patients was 57.18 (±14.68 standard deviation). The trend of patients diagnosed with RCC over the past 10 years was higher among males than females (60.27% vs. 39.73%). Noticeably, more than half (57.58%) were diagnosed incidentally. The most common histological subtype was clear cell (conventional) RCC (70.44%). Patients were usually diagnosed at the pT1 stage (48.1%).
The histopathological features associated with worse patient outcome were the stage of the primary tumor (P = 0.01) and lymph-vascular invasion (P = 0.003). The overall mean survival rate was 2.03 years.
Conclusion:
In the past 10 years, there are more patients diagnosed incidentally with RCC, which is in line with the global trend. Patients were more likely to be male and middle aged. We recommend further population-based studies in this area to establish a national epidemiological data for this common type of cancer.
Keywords: Epidemiology, outcomes, pathology, renal cell carcinoma, trends
INTRODUCTION
Renal cell carcinoma (RCC) is a malignancy originating from the epithelium of the renal tubules.[1] Worldwide RCC accounts for 2-3% of all adult malignancies and 90% of renal malignancies.[1,2] The most common histological types are clear cell carcinoma (75%), papillary RCC (10%), and chromophobe RCC (5%).[3,4]
RCC affects men and women in the fifth and sixth decade of life.[5] Clinical presentation varies between individuals, but patients in the advanced stages can present with the classical triad of hematuria, flank pain, and abdominal mass.[1,6] However, only 10% of patients present with all of the symptoms of the triad while 40% present with one of the three symptoms. Recently, there has been an increase in the number incidentally diagnosed asymptomatic patients through medical imaging.[7]
Internationally, RCC is increasing at a rate of 2%–3% per year.[8] The rates are higher in North America, Scandinavia, and Western Europe when compared to South America and Asia.[7] Europe has the highest incidence in the world affecting 7.2–33.6/100,000 males and 3.4–15/100,000 females. The age standardized is 8.9–12.9/100,000 for males and 4.1–5.9/100,000 for females. In the Middle East and Africa, the age-standardized incidence is 1.8–4.8/100,000 for males and 1.2–2.2/100,000 for females.[9]
The National Cancer Registry in Saudi Arabia reported in 2013 that renal cancer is the tenth most common cancer contributing to 2.7% of all cancers.[10] The Asir, Najran, and Northern Provinces have the highest renal cancer incidence of 4%.[11] In recent years, there has been an increase in kidney cancer incidence in Saudi Arabia.[12]
With the increase in RCC incidence, there was also an increase in kidney cancer mortality trend.[7] The epidemiological and mortality burden of RCC is high, especially metastatic tumors which have a survival rate of 0%–13% compared to localized tumors with a survival rate of 50%–90%.[8,13]
Despite that RCC is a common malignancy and its incidence is increasing, there is little information concerning the disease in Saudi Arabia. The purpose of this study is to describe the epidemiological profile, clinical characteristics, histopathological features, and outcomes of patients diagnosed with RCC in a tertiary referral center over 10 years.
METHODOLOGY
Study design
This is a retrospective cohort of all Saudi patients registered in the National Guard Hospital Pathology Department database diagnosed with RCC from June 2003 to May 2013. All Saudi patients were included in the study and were followed until the end of the study period or until death. No sample size calculation was needed as all of the patients' records included in the study over 10 years.
Data collection
Data were collected by SM and AA from June 22 to July 4, 2013. The variables were collected from the medical records and pathology reports. The variables included were as follows: (1) sociodemographic features: age, gender, and the city of origin in Saudi Arabia. (2) clinical presentation: hematuria, flank pain, palpable mass in the flank or abdomen, weight loss, fever, night sweats, malaise, varicocele, hypertension, hypercalcemia, and incidental finding. (3) histopathological features: twelve features from the College of American Pathologists (CAP) protocol for the examination of specimens from patients with carcinoma of the ureter and renal pelvis. The variables included were specimen type, laterality, tumor site, tumor size, focality, histologic type, sarcomatoid features, tumor necrosis, histological grade, microscopic tumor extension, tumor margins, lymph-vascular invasion, tumor, node, metastasis (TNM) pathologic staging, primary tumor staging, regional lymph node staging, and distant metastasis. (4) Survival: date of diagnosis, date of the last encounter, outcome of the patient, recurrence of RCC, cause of death, and date of death. Any information that was not explicitly mentioned in the records was considered missing data.
Data analysis
Raw data were processed in accordance with the best practices for raw data management to identify any inaccuracies or incompleteness in advance to the statistical analysis. All variables were summarized and reported across the study cohorts using descriptive statistics. Categorical variables were summarized and reported in terms of frequency distribution and compared statistically using Chi-square test with a level of significance set at P < 0.05. Kaplan–Meier estimate was used to calculate the survival rate. The data were analyzed using SAS, version 9.2 (SAS Institute Inc., Cary, NC).
Ethical considerations
All ethical issues were taken into consideration, including confidentiality and privacy of patient data. The study was approved by King Abdullah International Medical Research Center (KAIMRC) and institutional review board.
RESULTS
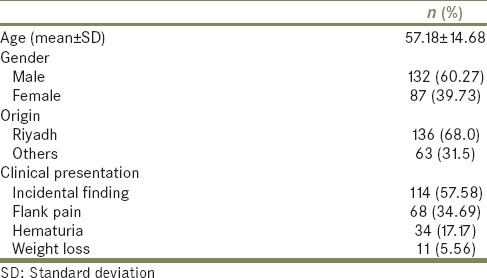
Data were collected from a total of 219 patients. The patients' age ranged from 22 to 95 and the mean age of the sample was 57.18 (±14.68 standard deviation). Overall, patients with RCC were more likely to be male (60.27% vs. 39.73%) and from Riyadh (68% vs. 31.5%). More than half were diagnosed incidentally (57.58%). The most frequent clinical presentation was flank pain (34.69%), followed by hematuria (17.17%), and weight loss (5.56%). Table 1 summarizes the demographic and clinical characteristics of the patients.
Table 1.
Demographic and clinical characteristics of 219 patients
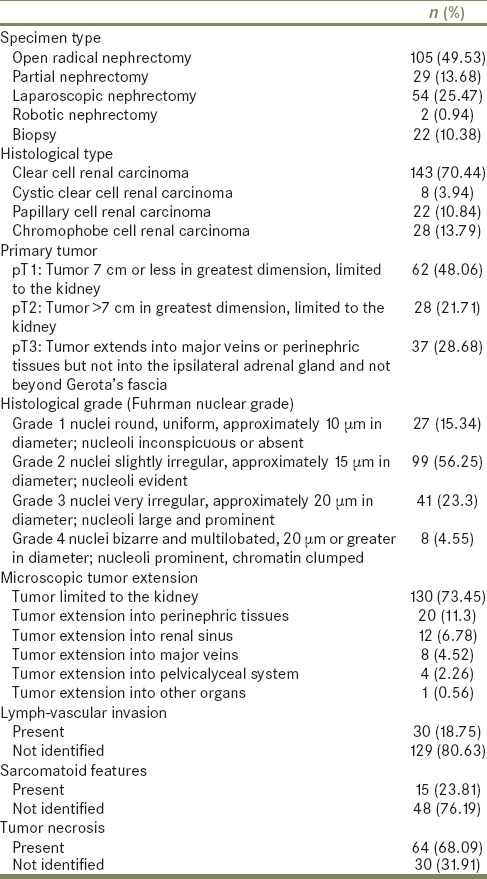
The histopathological characteristics are summarized in Table 2. Nearly half of the patients underwent open radical nephrectomy (49.53%). The most common histological subtype was clear cell (conventional) RCC (70.44%). Patients were most likely to be diagnosed with pT1 stage (48.06%) and Grade 2 Fuhrman nuclear grade (56.25%).
Table 2.
Histological characteristics of renal cell carcinoma
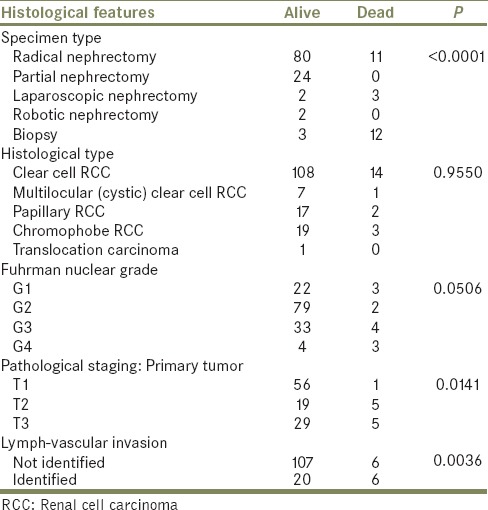
The histopathological features associated with worse patient outcome [Table 3] were the stage of the primary tumor (P = 0.01) and lymph-vascular invasion (P = 0.003). The type of procedure is statistically significant as patients who undergo biopsies are more likely to have worse outcomes (P < 0.0001). There was no association with histological subtype (P = 0.96) or Fuhrman nuclear grade (P = 0.05) with worse outcome.
Table 3.
Histopathological features associated with worse outcome
In 10 years, the overall number of patients diagnosed with RCC has increased over time, especially male patients [Graph 1]. There is a noticeable increase in the number of patients diagnosed incidentally. However, the symptomatic presentation is constant throughout the years [Graph 2]. Open radical nephrectomy was the most common surgery, but there has been a sharp decline after 2012. The number of patients undergoing laparoscopic resection of the tumor is increasing drastically [Graph 3]. The predominant subtype is the clear cell (conventional) RCC [Graph 4]. More patients are presenting and being diagnosed in the early stages of pT1 and Grade G2 [Graphs 5 and 6]. The overall mean survival rate in our sample was 2.03 years from the date of diagnosis with a 95% confidence interval (1.84–2.33) [Graph 7].
Graph 1.
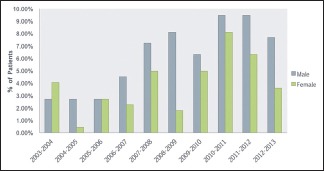
Distribution of renal cell carcinoma by gender over 10 years
Graph 2.
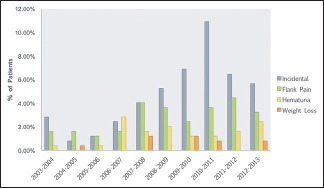
Clinical presentation of renal cell carcinoma over 10 years
Graph 3.
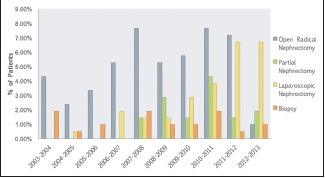
Surgical management of renal cell carcinoma over 10 years
Graph 4.
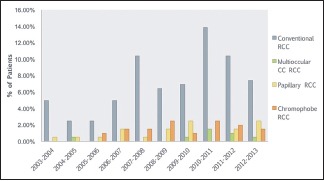
Histopathological subtypes of renal cell carcinoma over 10 years
Graph 5.
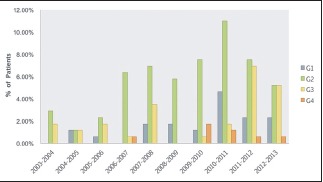
Fuhrman nuclear grade of renal cell carcinoma over 10 years
Graph 6.
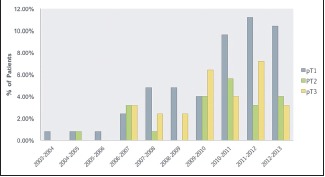
Pathological staging of renal cell carcinoma primary tumor over 10 years
Graph 7.
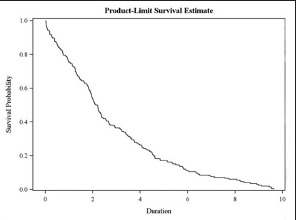
Kaplan–Meier survival curve of 219 patients
DISCUSSION
RCC is a heterogeneous disease, and the incidence varies internationally ranging from 22 per 100,000 in Czech men to <1 per 100,000 in African countries.[14] However, it is increasing in most countries for both genders with Europe and North America having the highest incidence. In the Middle East, renal cancer epidemiology is consistent. Of all the cancers, they represent 1.6% in Iraq, 2% in Jordan, and 1.8% in Syria and Lebanon. Renal cancer is the second most common urological tumor in Iraq while in Jordan, it is the third most common.[15]
In Saudi Arabia, renal cancers contribute to 3.6% of all cancers in men and 2.2% in women. In 2003, 139 cases of renal cancers were registered, 55.3% were men, and 44.6% were women. The age-standardized rate was 1.6 per 100,000 in males and 1.3 per 100,000 in females.[16] The Saudi cancer registry in 2013 reported a total of 313 renal cancer cases in which 61.7% were men and 38.3% were women. The age-standardized rate was 2.9 per 10,000 in males and 1.7 per 10,000 in females.[10] Our findings are consistent with international and local epidemiology as there is an increase in the number of cases in King Abdulaziz Medical City, National Guard Health Affairs over 10 years.
Medical images detect small renal masses and have contributed to nearly 50% to the overall incidence in western countries.[17] In our study, more than half of the patients presented incidentally, and it can be attributed to the patients' access to healthcare services. However, other studies in the Middle East show that patients are more likely to present with symptoms. A study in Jordan and Iraq showed that the most common presentation was hematuria (38.6%) and loin pain (27.2%). Only 16% were diagnosed incidentally.[15] Most of the patients in King Abdulaziz University Hospital in Jeddah, Saudi Arabia presented with gross hematuria (35.5%) compared to the 25.8% presented who incidentally.[18] In a tertiary center in Riyadh, 40.5% presented incidentally which is the closest to our result.[12]
The majority of patients in our cohort underwent a surgical intervention for the management of RCC. Most underwent partial nephrectomy (nephron-sparing surgery); however, there was a surge in the number of laparoscopic procedures done starting from 2010. According to the latest clinical management guidelines from the Saudi oncology society and Saudi urology association, localized RCC in the early stage should be treated surgically. Partial nephrectomy is the standard of care in the T1a stage. Radical nephrectomy is preferred in the more advanced stages and if possible to be done laparoscopically.[19] Urological laparoscopic procedures are becoming common practice in Saudi Arabia as Rabah et al. found that 54.3% of urologists in Saudi devote 5% or more of their practice time to laparoscopic procedures. The majority of those surgeons are affiliated with a university hospital or an academic institution.[20] The procedures the patients have had could reflect the clinical practices and the urologists' adherence to guidelines.
In our cohort, tumors were detected early such as the pT1 stage or Fuhrman Grade 1 or 2. There is an evidence of RCC stage migration over the years. The number of cases detected is increasing, and they are found in the earlier stages. A study that analyzed the United States national cancer data based showed the number of new Stage I cases increased from 43% to 57% over 20 years.[21] A proposed hypothesis is with the increased use of cross-sectional images, detected tumors are caught more frequently in the earlier stages and more likely to be small and benign.[21,22]
Mortality is associated with advanced tumor stage and lymph-vascular invasion in our sample. Prognosis of RCC relies on several factors such as anatomical, histological, clinical, and molecular factor. In general, the tumors with higher T-stages, metastasis to the lymph nodes, or distant metastasis have a worse prognosis. However, the Fuhrman nuclear grade and TNM staging are the strongest independent factors for localized RCC.[23]
One of the limitations of our study is the results reflect the characteristics and outcomes of patients in one center and not the Saudi population as a whole. Furthermore, we only included patients who underwent a surgical procedure or a biopsy to confirm diagnosis. This excludes patients who have small renal masses which were managed conservatively. Another limitation is during the data collection phase; we used the CAP protocol to collect histopathological information. The information that was not mentioned in the medical reports or pathology reports were reported as missing data. This could have affected our analysis as the quality of the reports was variable.
In conclusion, there is an increase in the number of patients diagnosed with RCC. Within the past few years, there is an increasing trend of incidental presentation most likely due to the utilization of medical imaging and access to healthcare. These findings are consistent with the global trends. The patients are more likely to be middle-aged males and undergo open radical nephrectomy. Since 2010, there has been an increase in the number of laparoscopic surgeries performed. The tumors are detected in earlier stages (Stage pT1, Fuhrman Grade 1 and 2) and limited to the kidney. The worse outcome is associated with the type of procedure that the patient underwent, advanced tumor stage, and presence of lymph-vascular invasion. We recommend further population-based studies to establish a national epidemiological data for RCC in Saudi Arabia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank Dr. Naila Ashraf for statistical analysis, Dr. Abrar Alahmadi for data collection and entry, the pathology department and the medical record department of King Abdulaziz Medical City – Riyadh, for assisting in data retrieval. We also thank KAIMRC and the National Guard Research Summer School organizers and faculty members for their support and feedback.
REFERENCES
- 1.Eble JE, Sauter G, Epstein IJ, Sesterhenn IA. Lyon, France: IARC Press; 2004. Tumours of the Urinary System and Male Genital Organs, WHO Classification of Tumours; pp. 221–49. [Google Scholar]
- 2.Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): A literature review. Cancer Treat Rev. 2008;34:193–205. doi: 10.1016/j.ctrv.2007.12.001. [DOI] [PubMed] [Google Scholar]
- 3.Cheville JC, Lohse CM, Zincke H, Weaver AL, Blute ML. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am J Surg Pathol. 2003;27:612–24. doi: 10.1097/00000478-200305000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Grignon DJ, Che M. Clear cell renal cell carcinoma. Clin Lab Med. 2005;25:305–16. doi: 10.1016/j.cll.2005.01.012. [DOI] [PubMed] [Google Scholar]
- 5.Murai M, Oya M. Renal cell carcinoma: Etiology, incidence and epidemiology. Curr Opin Urol. 2004;14:229–33. doi: 10.1097/01.mou.0000135078.04721.f5. [DOI] [PubMed] [Google Scholar]
- 6.Gibbons RP, Monte JE, Correa RJ, Jr, Mason JT. Manifestations of renal cell carcinoma. Urology. 1976;8:201–6. doi: 10.1016/0090-4295(76)90366-6. [DOI] [PubMed] [Google Scholar]
- 7.Mathew A, Devesa SS, Fraumeni JF, Jr, Chow WH. Global increases in kidney cancer incidence, 1973-1992. Eur J Cancer Prev. 2002;11:171–8. doi: 10.1097/00008469-200204000-00010. [DOI] [PubMed] [Google Scholar]
- 8.Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–30. doi: 10.3322/canjclin.56.2.106. [DOI] [PubMed] [Google Scholar]
- 9.Levi F, Ferlay J, Galeone C, Lucchini F, Negri E, Boyle P, et al. The changing pattern of kidney cancer incidence and mortality in Europe. BJU Int. 2008;101:949–58. doi: 10.1111/j.1464-410X.2008.07451.x. [DOI] [PubMed] [Google Scholar]
- 10.Cancer Incidence Report, Saudi Arabia; 2013. [Last accessed on 2017 Feb 02]. Available from: http://www.shc.gov.sa/Ar/HealthCenters/NCC/CancerRegistry/CancerRegistryReports/2013.pdf .
- 11.Abomelha MS. Genito-urinary cancer in Saudi Arabia. Saudi Med J. 2004;25:552–6. [PubMed] [Google Scholar]
- 12.Alkhateeb SS, Alkhateeb JM, Alrashidi EA. Increasing trends in kidney cancer over the last 2 decades in Saudi Arabia. Saudi Med J. 2015;36:698–703. doi: 10.15537/smj.2015.6.10841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353:2477–90. doi: 10.1056/NEJMra043172. [DOI] [PubMed] [Google Scholar]
- 14.Znaor A, Lortet-Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur Urol. 2015;67:519–30. doi: 10.1016/j.eururo.2014.10.002. [DOI] [PubMed] [Google Scholar]
- 15.Ibrahim AK. Trends of adult primary malignant renal tumors over 6 years. Pak J Med Sci. 2013;29:1385. doi: 10.12669/pjms.296.3736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cancer Incidence Report, Saudi Arabia. 2003. [Last accessed on 2017 Feb 02]. Available from: http://www.chs.gov.sa/ar/healthrecords/cancerregistry/cancerregistryreports/incidence%20report%202003.pdf .
- 17.Sun M, Thuret R, Abdollah F, Lughezzani G, Schmitges J, Tian Z, et al. Age-adjusted incidence, mortality, and survival rates of stage-specific renal cell carcinoma in North America: A trend analysis. Eur Urol. 2011;59:135–41. doi: 10.1016/j.eururo.2010.10.029. [DOI] [PubMed] [Google Scholar]
- 18.Ebu AM. Renal tumors in adults: The clinical experience of 124 patients. J King Abdulaziz Univ. 2011;18:15. [Google Scholar]
- 19.Alghamdi A, Alkhateeb S, Alghamdi K, Bazarbashi S, Murshid E, Alotaibi M, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for renal cell carcinoma. Urol Ann. 2016;8:136–40. doi: 10.4103/0974-7796.179239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rabah D, Abumostafa N, Sulaihim A, Arafa M. Survey of urologic laparoscopic practice patterns in Saudi Arabia. J Endourol. 2010;24:1293–5. doi: 10.1089/end.2010.0007. [DOI] [PubMed] [Google Scholar]
- 21.Kane CJ, Mallin K, Ritchey J, Cooperberg MR, Carroll PR. Renal cell cancer stage migration: Analysis of the national cancer data base. Cancer. 2008;113:78–83. doi: 10.1002/cncr.23518. [DOI] [PubMed] [Google Scholar]
- 22.Chow WH, Devesa SS, Warren JL, Fraumeni JF., Jr Rising incidence of renal cell cancer in the United States. JAMA. 1999;281:1628–31. doi: 10.1001/jama.281.17.1628. [DOI] [PubMed] [Google Scholar]
- 23.Volpe A, Patard JJ. Prognostic factors in renal cell carcinoma. World J Urol. 2010;28:319–27. doi: 10.1007/s00345-010-0540-8. [DOI] [PubMed] [Google Scholar]