

Abstract
The Fukushima Medical University conducted a mental health care program for evacuees after the Fukushima Daiichi nuclear power plant accident. However, the mental health status of non-respondents has not been considered for surveys using questionnaires. Therefore, the aim of this study was to clarify the characteristics of non-respondents and respondents. The target population of the survey (FY2011-2013) is people living in the nationally designated evacuation zone of Fukushima prefecture. Among these, the participants were 967 people (20 years or older). We examined factors that affected the difference between the groups of participants (i.e., non-respondents and respondents) using multivariate logistic regression analysis. Employment was higher in non-respondents (p=0.022) and they were also more socially isolated (p=0.047) when compared to respondents; non-respondents had a higher proportional risk of psychological distress compared to respondents (p<0.033). The results of the multivariate logistic regression analysis showed that, within the participants there was a significant association between employment status (OR=1.99, 95% confidence interval [CI]:1.12-3.51) and psychological distress (OR=2.17, 95% CI: 1.01-4.66). We found that non-respondents had a significantly higher proportion of psychological distress compared to the respondents. Although the non-respondents were the high-risk group, it is not possible to grasp the complexity of the situation by simply using questionnaire surveys. Therefore, in the future it is necessary to direct our efforts towards the mental health of non-respondents and respondents alike.
Keywords: non-respondent, evacuee, disaster, mental health survey, psychological distress
Introduction
The accident of the Fukushima Daiichi Nuclear Power Plant occurred after the Great East Japan Earthquake, which took place on March 11, 2011. Fukushima Medical University has, commissioned by Fukushima Prefecture, conducted “the Fukushima Health Management Survey”1) based on the health effects of radiation due to the accident. The Mental Health and Lifestyle Survey2) (MHLS) is one of the detailed surveys included in the project. Participants are about 2.1 million people in 13 municipalities within the evacuation area. Based on the questionnaire survey respondents, we have been conducting telephone support for evacuees who need mental health support and lifestyle-related diseases support since FY2011. However, the response rate of the survey participants is low and the characteristics of the non-respondents are unclear. Previous studies have found that many evacuees face the problem of psychological distress after disaster3,4). The same result was also obtained after this disaster5). In addition, previous studies reported that non-respondents who did not return the questionnaire were worse off with regard to their subjective health, had more negative health behaviors, and had higher age-adjusted mortality rates than respondents6-8). Therefore, the aim of this study was to clarify the characteristics of non-respondents of MHLS (FY2011-FY2013).
Materials and Methods
Participants
The target population of the MHLS (20 years or older) for each year was 173,537 (FY2011), 174,337 (FY2012), and 177,146 (FY2013) in the nationally designated evacuation zone including the 13 municipalities of Fukushima prefecture. In addition, the survey response rate was 41.0%, 30.3%, and 25.4%, respectively. Among these, 967 participants who had lived in two municipalities in Fukushima prefecture and evacuated inside or outside Fukushima prefecture, were randomly selected. We performed 30 to 60-minute face-to-face interviews with questionnaires on basic attributes, socioeconomic status, and mental health of 387 people (40.0% participation) from October 2014 to January 2015. Consequently, excluding the 74 participants whose response history of MHLS was unknown in this study, a total of 313 people (32.4%) were included in the study analyses.
In this study, we examined the characteristics of non-respondents in the MHLS conducted in FY2013. Regarding the representativeness, we found that the K6, PCL-S, and LSNS-6 scores among the participants of this study were similar to those of the survey population in FY2013 (K6: 5.8 vs. 5.2, PCL-S: 30.7 vs. 30.4, LSNS-6: 12.3 vs. 13.1)9). However, some results were not similar; the participants in this study were older (58.0 vs. 54.7 years old, p=0.002), had a higher proportion of women (women: 58.1% vs. 51.2%, p=0.014).
Data collection
We divided the remaining 313 people into two groups: non-respondents and respondents. Respondents refer to the people who answered the survey one or more times over three years. We collected the following participant characteristics data for the analysis of both groups: age, gender, living place, family structure, educational attainment, employment status, financial circumstances, and the Lubben Social Network Scale-6 (LSNS-6)10,11). If a participant scored <12 on the LSNS-6, he/she was defined as socially isolated10,11).
The psychological distress of evacuees was measured using the Japanese version12) of the 6-item Kessler Psychological Distress Scale (K6)13). The K6 is a self-administered questionnaire consisting of six questions that evaluate depressive mood and anxiety over the preceding 4 weeks on a 5-point response scale from 0=None of the time to 4=All of the time (range of the scale score: 0-24). In this study, we used a cut-off score of 13 to identify cases with psychological distress, as was used in previous studies of community populations in Japan14,15).
Posttraumatic stress disorder (PTSD) of evacuees was measured using the PTSD Checklist Stressor-Specific Version (PCL-S)16-18). The PCL-S is a self-administered questionnaire consisting of 17 questions that evaluate PTSD based on the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV)19). Participants indicated whether they were bothered by symptoms due to a traumatic event in the past month on a 1-5 Likert scale (1=Not at all to 5=Extremely), with the sum of all responses generating a total score ranging from 17-85. The score providing the optimal screening cut-off point has been shown to be ≥4417,20,21), including in this study.
Statistical analysis
Statistical comparisons between groups (non-respondents and respondents) were conducted using a chi-square test, t-test, and Mann-Whitney U test. Moreover, a multivariate logistic regression analysis was performed to determine differences between groups. The multivariate logistic regression analysis was used only for K6 scores, because a strong correlation was found between the K6 and PCL-S scores18) in a previous study.
The scores were expressed as means and standard deviations (SD), and p<0.05 was regarded to indicate statistical significance. All statistical procedures were performed using SPSS for Windows (version 21; Armonk, NY:IBM).
Ethical considerations
This study was approved by the ethics review committee of Fukushima Medical University (No. 2086). The study objective was explained to all participants and all were advised that 1) participation in the study was completely voluntary, 2) they could withdraw from the study at any time, and 3) if they chose to withdraw, they would not be disadvantaged in any way.
Results
The characteristics of the participants in the two groups (non-respondents and respondents) are shown in Table 1. Non-respondents were more likely to be employed (p=0.022) and socially isolated (p=0.047) compared to respondents.
Fig. 1.
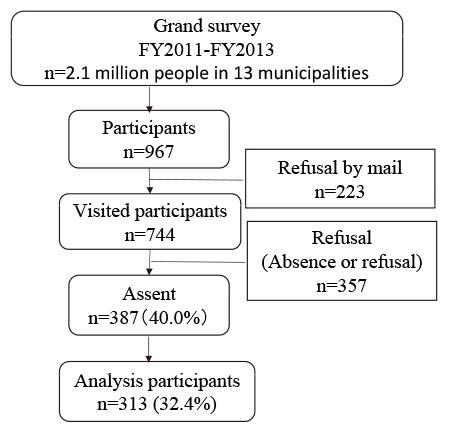
Selection of participants
Table 1.
Characteristics of participants
| total
n=313 |
non-respondents
n=144 |
respondents
n=169 |
p | ||||
| Age | |||||||
| Mean (SD) | 58.0±18.7 | 57.7±20.5 | 58.9±16.9 | 0.588 | |||
| Gender | |||||||
| Men | 131 | (41.9) | 66 | (45.8) | 65 | (38.5) | 0.207 |
| Women | 182 | (58.1) | 78 | (54.2) | 104 | (61.5) | |
| Living place | |||||||
| Inside Fukushima prefecture | 145 | (46.3) | 61 | (42.4) | 84 | (49.7) | 0.212 |
| Outside Fukushima prefecture | 168 | (53.7) | 83 | (57.6) | 85 | (50.3) | |
| Family structure | |||||||
| Single and Spouses | 117 | (40.1) | 47 | (35.9) | 70 | (43.5) | 0.230 |
| Other | 175 | (59.9) | 84 | (64.1) | 91 | (56.5) | |
| Educational attainment | |||||||
| Elementary or junior high school | 60 | (20.5) | 32 | (24.2) | 28 | (17.5) | 0.190 |
| High school or more | 232 | (79.5) | 100 | (75.8) | 132 | (82.5) | |
| Employment status | |||||||
| Unemployed | 179 | (61.1) | 71 | (53.8) | 108 | (67.1) | 0.022 |
| Employed | 114 | (38.9) | 61 | (46.2) | 53 | (32.9) | |
| Financial circumstances | |||||||
| Good | 200 | (67.8) | 90 | (67.2) | 110 | (68.3) | 0.901 |
| Bad | 95 | (32.2) | 44 | (32.8) | 51 | (31.7) | |
| LSNS-6 | |||||||
| Median (25%-75%) | 12.0 | (7.0-17.8) | 10.0 | (6.0-17.3) | 13.0 | (8.0-18.0) | 0.125 |
| <12 | 144 | (48.6) | 74 | (55.2) | 70 | (43.2) | 0.047 |
| ≥12 | 152 | (51.4) | 60 | (44.8) | 92 | (56.8) | |
n (%) Chi-square test, t-test, and Mann-Whitney U test were used.
Note: Socially isolated was measured using LSNS-6 scale; a participant with a LSNS-6 score of <12 was defined as socially isolated.
Table 2 shows the results of the chi-square tests and Mann-Whitney U test for associations between non-response and mental health (psychological distress and PTSD). The K6 and PCL-S scores of non-respondents had a lower median compared to those of respondents. On the other hand, non-respondents had a higher proportional risk of psychological distress and PTSD compared to respondents.
Table 2.
The number (rate) of non-respondents corresponding to psychological distress and posttraumatic stress disorder
| total
n=313 |
non-respondents
n=144 |
respondents
n=169 |
p | ||||
| K6 | |||||||
| Median (25%-75%) | 4.0 | (1.0-9.0) | 4.0 | (0-10.0) | 5.0 | (1.0-10.0) | 0.941 |
| <13 | 254 | (87.3) | 107 | (82.3) | 147 | (91.3) | 0.033 |
| ≥13 | 37 | (12.7) | 23 | (17.7) | 14 | (8.7) | |
| PCL | |||||||
| Median (25%-75%) | 27.0 | (20.0-36.5) | 25.0 | (19.0-36.8) | 29.0 | (20.0-37.0) | 0.256 |
| <44 | 243 | (84.1) | 101 | (78.9) | 142 | (88.2) | 0.036 |
| ≥44 | 46 | (15.9) | 27 | (21.1) | 19 | (11.8) | |
n (%) Chi-square test and Mann-Whitney U test were used.
Note: Psychological distress was measured using K6 scale, a participant with a K6 score of ≥13 was defined as having psychological distress. Posttraumatic stress disorder was measured using PCL scale; a participant with a PCL score of ≥44 was defined as having posttraumatic stress disorder.
Table 3 shows the results of the multivariate logistic regression analysis of factors that affected the difference of the participants of the self-administered questionnaire. Non-respondents in the survey had a significant association with employment (OR=1.99, 95% confidence interval [CI]:1.12-3.51) and psychological distress (OR=2.17, 95% CI: 1.01-4.66).
Table 3.
Factors associated with non-response to the self-administered questionnaire in the multivariate analysis
| Variable | Total | |||
| OR | 95% CI | |||
| Age | 1.00 | 0.99-1.02 | ||
| Gender | (Ref. Men) | 0.68 | 0.40-1.14 | |
| Living place | (Ref. Inside Fukushima prefecture) | 1.69 | 0.99-2.86 | |
| Family structure | (Ref. Single and Spouses) | 1.63 | 0.97-2.73 | |
| Educational attainment | (Ref. Elementary or junior high school) | 0.58 | 0.30-1.10 | |
| Employment status | (Ref. Unemployed) | 1.99 | 1.12-3.51 | * |
| Financial circumstances | (Ref. Good) | 1.26 | 0.72-2.23 | |
| LSNS-6 <12 | (Ref. ≥12) | 0.80 | 0.47-1.35 | |
| K6 ≥13 | (Ref. <13) | 2.17 | 1.01-4.66 | * |
Multivariate logistic regression was used to calculate ORs and 95% confidence intervals (95% CI) after controlling simultaneously for independent variables. N=418
*p<0.05
Note: K6 score ≥13 was defined as psychological distress.
Table 4 shows the results of why respondents took part in the study and the suggested improvement plan regarding the submission of the questionnaire. “For contribution (48.5%)” was the most popular reason as to why respondents took part in the study, followed by “to tell my thoughts (45.6%)” and “to take part in a study at the Fukushima Medical University (40.2%).” On the other hand, “having no time to spare (46.7%)” was the highest-ranking reason for non-respondents, followed by “no need to do this for myself (26.8%),” “asking too many questions (16.0%),” and “stress brought about by the answers (16.0%).” Furthermore, “to reduce the number of questions (45.9%)” was highest in the suggestions for improving the response rate. Followed by “the study should be repeated every few years (18.7%)” and “to be able to participate in the study at the same time as the health checkup (16.0%)” were also of high importance to the participants.
Table 4.
Reasons for answering the questionnaire and proposal for improvement in the Mental Health and Lifestyle Survey
| total | non-respondents | respondents | ||||
| n=169 | ||||||
| The reason for response | ||||||
| For contribution | - | - | 82 | (48.5) | ||
| To tell my thoughts. | - | - | 77 | (45.6) | ||
| To take part in a study at the Fukushima Medical University | - | - | 68 | (40.2) | ||
| To always participate | - | - | 33 | (19.5) | ||
| To have time to spare. | - | - | 23 | (13.6) | ||
| Because a result report arrived | - | - | 7 | (4.1) | ||
| Because it was recommended to be submitted to the family | - | - | 4 | (2.4) | ||
| Other | - | - | 13 | (7.7) | ||
| n=257 | n=144 | n=113* | ||||
| The reason for non-response | ||||||
| To have no time to spare | 120 | (46.7) | 59 | (41.0) | 61 | (54.0) |
| No need for myself | 69 | (26.8) | 38 | (26.4) | 31 | (27.4) |
| For asking too many questions. | 41 | (16.0) | 20 | (13.9) | 21 | (18.6) |
| Stress of answers | 41 | (16.0) | 31 | (21.5) | 10 | (8.8) |
| Do not remember | 25 | (9.7) | 19 | (13.2) | 6 | (5.3) |
| Do not understand the purpose of the study. | 23 | (8.9) | 17 | (11.8) | 6 | (5.3) |
| Because it was a study at the Fukushima Medical University | 9 | (3.5) | 9 | (6.3) | 0 | (0.0) |
| Because a result report did not arrive | 3 | (1.2) | 1 | (0.7) | 2 | (1.8) |
| Other | 59 | (23.0) | 25 | (17.4) | 9 | (8.0) |
| n=257 | n=144 | n=113* | ||||
| Suggestions for improving the response rate | ||||||
| To reduce the number of questions. | 118 | (45.9) | 44 | (30.6) | 74 | (65.5) |
| The study should be repeated every few years | 48 | (18.7) | 22 | (15.3) | 26 | (23.0) |
| To be able to participate in the study at the same time as the health checkup | 41 | (16.0) | 29 | (20.1) | 12 | (10.6) |
| To make a result report arrive | 27 | (10.5) | 17 | (11.8) | 10 | (8.8) |
| Do not submit so troublesome | 9 | (3.5) | 8 | (5.6) | 1 | (0.9) |
| Interview study | 7 | (2.7) | 7 | (4.9) | 0 | (0.0) |
| Improvement of the question items | 5 | (1.9) | 4 | (2.8) | 1 | (0.9) |
| To receive benefits. | 3 | (1.2) | 3 | (2.1) | 0 | (0.0) |
| Other | 36 | (14.0) | 31 | (21.5) | 5 | (4.4) |
n (%)
*We excluded those who participated all three times.
Discussion
In this study, we examined the characteristics of non-respondents in a mental health survey after a disaster. We found that participants (non-respondents and respondents) were significantly associated with employment and the prevalence of high-risk psychological distress. Furthermore, non-respondents were significantly more employed and socially isolated than respondents. Further, non-respondents were more often male, younger, and with a lower educational history. Although these findings were not statistically significant, similar trends have been observed in other studies7,22). In addition, regarding representativeness of the MHLS in this research, we believe that the target of this survey is a representative group.
Non-respondents had a significantly higher proportion of psychological distress compared to respondents. As there was no difference in the median between these groups, we considered that people with psychological distress were more likely to become non-respondents. Une et al.23) found differences in non-respondents and respondents in a population-based mail survey: non-respondents had higher age-adjusted mortality rates, cancer, heart disease, and stroke compared to respondents. In addition, non-respondents have been characterized as having poorer mental health than respondents24). From the above, it is necessary to consider efforts that ensure the mental and physical health of evacuees.
In addition, non-respondents had higher ratios of social isolation. Kawachi et al.25) stated that social support may act on the pathway between the stressful event and mental illness. Recently, Goodwin et al.26) reported psychological distress and social support among refugees in the Great East Japan Earthquake and Tsunami. As people who are socially isolated have poorer mental health27), socially isolated evacuees, in particular, need to be considered and require support.
Furthermore, non-respondents had a higher proportion of employment than respondents. This may have reflected the fact that many employees do not have time to spare when it comes to responding to questionnaires28), because the proportion of non-respondents was high among men and young people7). However, because non-respondents are potentially at higher risk for psychological distress, we need to encourage them to take part in surveys with an aim to improve the situation of non-respondents.
One of the reasons non-respondents did not submit the questionnaire was that they “do not have time to spare.” As the proportion of employment was higher in non-respondents, not enough time is considered to be one of the factors that had an effect on response rate. The proportion of non-respondents was significantly higher than that of previous research29). As there may be people at high risk for mental health problems among non-respondents, it would be useful to employ measures that encourage response. We consider it important to connect to these non-respondents over the telephone to support these evacuees. In addition, Edwards et al.30) stated that response was more likely when short questionnaires were used, when a monetary incentive was used, and when follow-up contact was conducted. Similarly, in terms of suggestions for improving the response rate in our study, “to reduce the number of questions” obtained the highest score. For this reason, we decided to change the study to use a short questionnaire that was easy to answer in FY2014 in the MHLS. Further, to increase the response rate, we took the approach that if participants did not return the results of the questionnaire, we sent a reminder, and called participants to complete the survey through cooperation with municipalities. In a post-disaster survey, researchers recognize that participants want “to contribute” or “to share their thoughts.” However, we also need to consider research methods that do not create stress among evacuees.
There are several limitations to this study. First, the study participants were evacuees after a disaster rather than community residents. In addition, the evacuation area was quite broad. This limits the generalizability of our findings. Second, the use of the K6 scale is inferior to a clinician administered diagnostic tool. However, measures of psychological distress such as the K6 have been used for evacuees who experience continuous living stress. Third, the response rate of 40.0% was not high. In addition, there is also a possibility of a lack of representativeness of the participants in the FY2013 survey; it is possible that selection bias occurred. Despite these limitations, the present study is aimed at clarifying the characteristics of non-respondents in a post-disaster study. We hope that our findings will contribute to the study of post-disaster.
In this study, we examined the characteristics of non-respondents and respondents by age, gender, socioeconomic status, and psychological distress. We found that non-respondents were significantly more likely to suffer from psychological distress compared to respondents. Although the non-respondents were a high-risk group, it is not possible to grasp the full situation simply by using questionnaire surveys. In addition, we found non-respondents felt stress about answering the questionnaire compared to respondents. Therefore, efforts are necessary to provide mental health care after a disaster while considering the characteristics of non-respondents.
Acknowledgements
This study was supported by the Grant-in-Aid for Scientific Research (C) (No. 26510011), and was conducted as part of Fukushima prefecture’s post-disaster recovery plan.
Conflict of interest
The authors declare no conflicts of interest.
References
- 1.Yasumura S, Hosoya M, Yamashita S, et al. Study Protocol for the Fukushima Health Management Survey. Journal of Epidemiology, 22(5): 375-383, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yabe H, Suzuki Y, Mashiko H, et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant Accident: results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima Journal of Medical Science, 60(1): 57-67, 2014. [DOI] [PubMed] [Google Scholar]
- 3.Kuwabara H, Shioiri T, Toyabe S, et al. Factors impacting on psychological distress and recovery after the 2004 Niigata-Chuetsu earthquake, Japan: Community-based study. Psychiatry and Clinical Neurosciences, 62(5): 503-507, 2008. [DOI] [PubMed] [Google Scholar]
- 4.Ohta Y, Araki K, Kawasaki N, Nakane Y, Honda S, Mine M. Psychological distress among evacuees of a volcanic eruption in Japan: A follow-up study. Psychiatry and Clinical Neurosciences, 57(1): 105-111, 2003. [DOI] [PubMed] [Google Scholar]
- 5.Oe M, Fujii S, Maeda M, et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident [The Fukushima Health Management Survey]. Psychiatry and Clinical Neurosciences, 70(6): 245-252, 2016. [DOI] [PubMed] [Google Scholar]
- 6.Macera CA, Jackson KL, Davis DR, Kronenfeld JJ, Blair SN. Patterns of non-response to a mail survey. Journal of Clinical Epidemiology, 43(12): 1427-1430, 1990. [DOI] [PubMed] [Google Scholar]
- 7.Van Loon AJM, Tijhuis M, Picavet HSJ, Surtees PG, Ormel J. Survey non-response in the Netherlands: effects on prevalence estimates and associations. Annals of Epidemiology, 13(2): 105-110, 2003. [DOI] [PubMed] [Google Scholar]
- 8.Iwasaki M, Otani T, Yamamoto S, et al. Background characteristics of basic health examination participants: the JPHC Study Baseline Survey. Journal of Epidemiology, 13(4): 216-225, 2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.The Mental Health and Lifestyle Survey FY2013. Survey results available from http://www.pref.fukushima.lg.jp/uploaded/attachment/115330.pdf/, (Date of access:12/09/2017).
- 10.Lubben J, Blozik E, Gillmann G, et al. Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. The Gerontologist, 46(4): 503-513, 2006. [DOI] [PubMed] [Google Scholar]
- 11.Kurimoto A, Awata S, Ohkubo T, et al. Study of reliability and validity of a Japanese brief version of Lubben Social Network Scale (LSNS-6) (in Japanese). Nihon Ronen Igakkai Zasshi, 48: 149-157, 2011. [DOI] [PubMed] [Google Scholar]
- 12.Furukawa TA, Kawakami N, Saitoh M, et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. International Journal of Methods in Psychiatric Research, 17(3): 152-158, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32(6): 959-976, 2002. [DOI] [PubMed] [Google Scholar]
- 14.Sakurai K, Nishi A, Kondo K, Yanagida K, Kawakami N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry and Clinical Neurosciences, 65(5):434-441, 2011. [DOI] [PubMed] [Google Scholar]
- 15.Inoue A, Kawakami N, Tsuchiya M, Sakurai K, Hashimoto H. Association of occupation, employment contract, and company size with mental health in a national representative sample of employees in Japan. Journal of Occupational Health, 52(4): 227-240, 2010. [DOI] [PubMed] [Google Scholar]
- 16.Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM, editors. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Annual Convention of the International Society for Traumatic Stress Studies. San Antonio, 1993. [Google Scholar]
- 17.Suzuki Y, Yabe H, Horikoshi N, et al. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia-Pacific Psychiatry, 2016. [DOI] [PubMed] [Google Scholar]
- 18.Iwasa H, Suzuki Y, Shiga T, Maeda M, Yabe H, Yasumura S. Psychometric evaluation of the Japanese version of the Posttraumatic Stress Disorder Checklist in community dwellers following the Fukushima Daiichi Nuclear Power Plant incident. SAGE Open, 6(2): 2158244016652444, 2016. [Google Scholar]
- 19.American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-IV). Washington, DC: Author, 1994. [Google Scholar]
- 20.Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD Checklist (PCL). Behaviour Research and Therapy, 34(8): 669-673, 1996. [DOI] [PubMed] [Google Scholar]
- 21.Cukor J, Wyka K, Jayasinghe N, et al. Prevalence and predictors of posttraumatic stress symptoms in utility workers deployed to the World Trade Center following the attacks of September 11, 2001. Depression and Anxiety, 28(3): 210-217, 2011. [DOI] [PubMed] [Google Scholar]
- 22.Picavet HSJ. National health surveys by mail or home interview: effects on response. Journal of Epidemiology and Community Health, 55(6): 408-413, 2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Une H, Miyazaki M, Momose Y. Comparison of mortality between respondents and non-respondents in a mail survey. Journal of Epidemiology, 10(3): 136-139, 2000. [DOI] [PubMed] [Google Scholar]
- 24.Knudsen AK, Hotopf M, Skogen JC, Øverland S, Mykletun A. The health status of nonparticipants in a population-based health study: the Hordaland Health Study. American Journal of Epidemiology, 172(11): 1306-1314, 2010. [DOI] [PubMed] [Google Scholar]
- 25.Kawachi I, Berkman LF. Social ties and mental health. Journal of Urban Health, 78(3): 458-467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Goodwin R, Takahashi M, Sun S, Ben-Ezra M. Psychological distress among tsunami refugees from the Great East Japan Earthquake. British Journal of Psychiatry Open, 1(1): 92-97, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schweitzer R, Melville F, Steel Z, Lacherez P. Trauma, post-migration living difficulties, and social support as predictors of psychological adjustment in resettled Sudanese refugees. Australian and New Zealand Journal of Psychiatry, 40(2): 179-187, 2006. [DOI] [PubMed] [Google Scholar]
- 28.Holmen J, Midthjell K, Krüger Ø, Langhammer A, Holmen TL, Bratberg GH, et al. The Nord-Trøndelag Health Study 1995-97 (HUNT 2): objectives, contents, methods and participation. Norsk Epidemiologi, 13(1): 19-32, 2003. [Google Scholar]
- 29.Locke III GR, Schleck CD, Ziegenfuss JY, Beebe TJ, Zinsmeister AR, Talley NJ. A low response rate does not necessarily indicate non-response bias in gastroenterology survey research: a population-based study. Journal of Public Health, 21(1): 87-95, 2013. [Google Scholar]
- 30.Edwards P, Roberts I, Clarke M, et al. Increasing response rates to postal questionnaires: systematic review. BMJ (Clinical Research Edition), 324(7347): 1183, 2002. [DOI] [PMC free article] [PubMed] [Google Scholar]