

Abstract
Background
Worldwide breast cancer incidence correlates with socioeconomic status and increases in parallel with westernization, however urban–rural disparity and trends have not been adequately investigated in China.
Methods
The age standardized rate (ASR) of female breast cancer by population‐based cancer registration was compared between urban Shijiazhuang city and rural Shexian County in relation to socioeconomic status. The increasing trend of breast cancer in Shexian County from 2000–2015 was examined using Joinpoint analysis and the correlation with gross domestic product (GDP) per capita was analyzed.
Results
In 2012, the ASR of female breast cancer in Shijiazhuang was more than three times higher than in Shexian County (45.5/1 00 000 vs.13.8/1 00 000; P < 0.01) when the GDP per capita was 2.6 times higher (US$6964.80 vs. US$2700). In parallel with rapid socioeconomic development and urbanization, the biennial ASR of female breast cancer in Shexian county has increased significantly from 2.8/1 00 000 in 2000–2001 to 17.3/1 00 000 in 2014–2015, with an average biennial percent change of +10.2% (P < 0.01). The Pearson correlation between ASR and GDP was significantly positive (r = 0.94, P < 0.01).
Conclusion
The incidence of breast cancer in women in China is increasing along with lifestyle westernization and changing reproductive patterns associated with socioeconomic development and urbanization. Urgent prevention measures, including the development of a healthy diet, giving birth at a younger age, an increase in breastfeeding, limiting menopause estrogen therapy, and control of alcohol consumption, are required.
Keywords: Healthy diet, obesity and/or overweight, prevention of female breast cancer, socioeconomic development, urbanization
Introduction
In China, the risk factors for breast cancer are significantly different between urban and rural women, and risk transitions have taken place in parallel with socioeconomic development and urbanization over the past three decades. There has been a steady increase in the prevalence of overweight and obese conditions, reduced physical activity, reduced fertility and breastfeeding, older age at first birth, and earlier age of menarch.1 However, the changing epidemiology of breast cancer has been inadequately documented. For example, although China has the world's largest urban–rural disparity in socioeconomic development,2 the difference in age standardized incidence rate (ASR) of breast cancer in women reported between 77 Chinese cities and 100 counties for 2011 was merely 31.6 vs. 21.0 per 100 000,3 much smaller than that the difference reported between developed and developing countries according to GLOBOCAN 2012 (73.4 vs. 31.3 per 100 000).4 These statistics suggest that urban–rural classification criteria may be flawed. By highlighting a striking urban–rural disparity in female breast cancer between urban Shijiazhuang city and rural Shexian county in Hebei province and a progressively increasing trend from 2000–2015 in Shexian County in parallel with socioeconomic development and urbanization, this paper aims to draw the attention of health policy‐makers to the urgent need for breast cancer prevention in China.
Methods
Shexian
Shexian County is located 200 km southwest of Shijiazhuang city, which is the capital city of Hebei province. Shexian County is an entirely mountainous region that joins the three provinces of Hebei, Henan, and Shanxi (Fig 1). In 2012, its population was 408 998. Shexian County is a northern neighbor of Linxian County of Henan province and a northwestern neighbor of Cixian County of Hebei province. All three counties have been noted for extraordinary high incidence rates of esophagogastric cancers.5 Shexian is a rural agricultural county, consisting of a town and 580 villages. In 2012, 48% of the population lived in the town, and 52% in villages. Town economy relies on employment in the iron/steel, thermal power, agricultural product, food manufacture, and tourist industries; while the rural population is engaged in growing rice, wheat, persimmon, Chinese prickly ash, and walnuts. The diet in Shexian has traditionally been of agrarian style, with a staple food of rice or steamed buns flavored with vegetables, soybean, pork, or eggs, although since the 1990's a transition has occurred toward a more westernized style of diet. Occupational manual exertion is the primary physical activity for villagers, but in town the majority of people aged ≥ 60 walk or jog in the morning or evening.
Figure 1.

Geographic location of urban Shijiazhuang city (upper right) at the foot of Taihang Mountain and Shexian county located 250 km southwest in the Taihang mountain ranges.
Shijiazhuang city
Shijiazhuang is located 200 km northeast of Shexian County (Fig 1). At the beginning of the 20th century, it was not an urban city and consisted of over a dozen villages. The villages were located at the crossing point of the north‐south bound Peking–Wuhan railway and the east‐west bound Shijiazhuang‐Taiyuan railway. Prime urbanization began in 1953 when it was chosen by the Chinese central government as the capital of Hebei Province and one of cities with development priority during the first national five‐year program (1953–1957). During the program, the North China Pharmaceutical Corporation, the largest antibiotic factory in Asia, and five modern textile plants were established in Shijiazhuang city. Upon completion of the five‐year program, the total number of municipal employees had increased from 81 067 to 182 188, and the total municipal population from 182 188 to 376 792.
Population‐based tumor registration
Population‐based cancer registration was established in Shexian County in 1999 and in Shijiazhuang City in 2010, by the National Central Cancer Registry of China (NCCRC) and the International Association of Cancer Registration (IACR). The Chinese Ministry of Health provides a running budget. Cancer diagnoses are reported to local cancer registries from multiple sources, including local hospitals and community health centers, as well as the local Urban Resident Basic Medical Insurance Program and the New Rural Cooperative Medical Scheme, public insurance programs with almost complete coverage of registered urban or rural residents since 2011. Data quality is supervised and assessed annually by NCCRC before publication.
Population data
Population data concerning the gender and age distribution in Shexian County and Shijiazhuang city was obtained from the Population Division of the local Public Security Bureau (Fig 2). The 2012 population in Shexian County was 408 998 (male: female ratio 1.07:1), and in urban Shijiazhuang was 2, 374 827 (male: female ratio 0.95:1).
Figure 2.
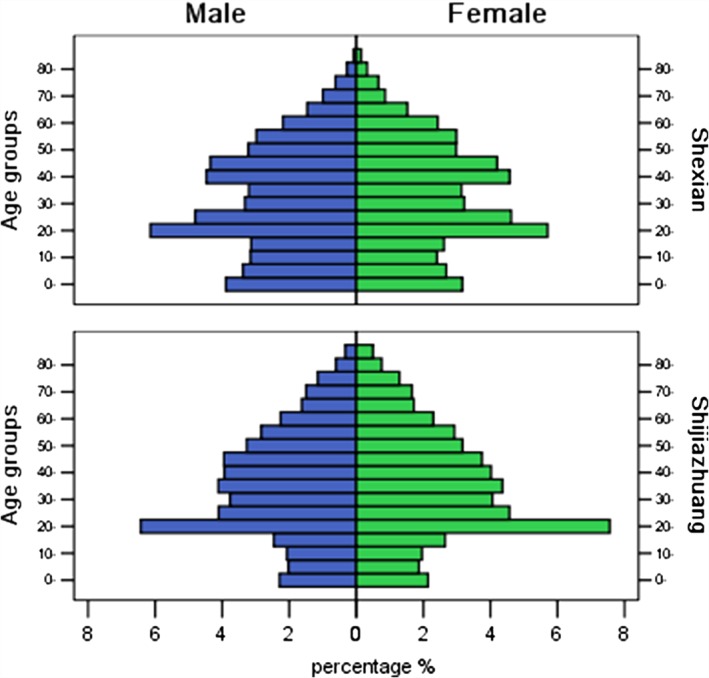
Comparison of the population pyramids between rural ShexianCounty and urban Shijiazhuang city in 2012.
Statistical methods
Age‐specific incidence rates were calculated by dividing the number of new cancer cases by the number of people at age intervals of 0, 1–4, 5–9…80–84, 85+. The rates were then multiplied by the proportion of people in that age interval using Segi's standard world population (a hypothesized 100 000 people),6 and then added to obtain the ASR. The Segi world standard population was first introduced by Segi in 1960, drawn from a pooled population of 46 countries and modified by Doll et al. in 1966. The Segi–Doll world standard population is used thoroughout the world to standardize incidence rates for comparison.
The difference in ASR of female breast cancer between Shexian County and Shijiazhuangcity was tested using approximate methods described by Esteve et al. 7 Briefly, the approximate method uses the formula: Z = (t1 − t2/SQUARE(m1t1 + m2t2)/m1m2), where t1 and t2 are the rates to be compared and m1 and m2 are person–years of observation, to calculate the value of Z, assumes that Z obeys standard normal distribution. If the Z value is > 1.96, the hypothesis of equality of the rates between the two populations is rejected at a level of significance of α = 0.05.
The trends of biennial ASR of female breast cancer in Shexian between 2000 and 2015 were analyzed using JoinPoint Analysis 4.2.0.2 (http://surveillance.gov/joinpoint).Pearson'scorrelation coefficient between biennial ASR of breast cancer incidence and the corresponding gross domestic product (GDP) value in Shexian County from 2000–2015 was analyzed by bivariate correlation using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
The study was approved by the Institutional Ethics Review Board of the Fourth Hospital of Hebei Medical University.
Results
Comparison of 2012 demographic and lifestyle characteristics
Although both regions started from a rural agrarian background 60 years ago, Shexian is considerably underdeveloped in comparison to Shijiazhuang. As shown in Table 1, in which demographic and socioeconomic data obtained from government websites8, 9, 10, 11, 12 or published papers13, 14 are listed, the GDP per capita in 2012 was 2.6 times higher in Shijiazhuang than in Shexian County (US$6964.80 vs. US$2700). The annual disposable income per person was US$1538 for Shijiazhuang but only US$750 for Shexian residents. Shijiazhuang residents spent more of their disposable income on diet than those in Shexian (40% vs. 20%). The proportion of animal food in the diet was higher in Shijiazhuang (> 30%) than in Shexian (< 10%). Regarding physical activity, Shijiazhuang residents led a more sedentary lifestyle because of the greater availability of white‐collar jobs and the fact of living in a relatively more built‐up environment. By contrast, Shexian residents are physically more active as a result of working in agricultural roles or walking. As is true in other non‐metropolitan areas of China, women in both regions seldom smoke cigarettes or drink alcohol. The prevalence of daily smoking in men is higher in Shexian than in Shijiazhuang (40% vs. 35%), whereas the prevalence of habitual alcohol drinking is the opposite (Shijiazhuang 38% vs. Shexian 25%). Although the prevalence of an overweight condition was similar between the two areas, obesity incidence was higher in urban Shijiazhuang than in rural Shexian women (23.2% vs. 17.1%). In addition, the population in Shijiazhuang is older than in Shexan: the percentage of residents aged < 25 in Shexian was 36.29% compared to 31.46% in Shijiazhuang and of residents aged ≥ 65 years was 11.15% and 6.98%, respectively (Fig 2). A four‐year difference in life expectancy was observed between Shijiazhuang and Shexian in 2012 (75 vs. 71 years). The birth rate was higher in Shexian than in Shijiazhuang (1.8 vs. 1.1). Shexian women give birth four years younger than Shijiazhuang women (23 vs. 27 years), and breastfeeding is more common among Shexian than Shijiazhuang women (95% vs. 60%) (Table 1).
Table 1.
Comparison of demographic and lifestyle characteristics between urban Shijiazhuang and rural Shexian in 2012
| Demographic | Urban Shijiazhuang | Rural Shexian |
|---|---|---|
| Population (2012) | 23748278 | 408,9959, 10, 11, 12 |
| % of urban population (2012) | 100%8 | 48%9, 10, 11, 12 |
| Altitude (m above sea level) | 30–100 m | 1000 m |
| Latitude N | 37°27′~38°47′ | 36°17′~36°55′ |
| GDP per capita 2012 (US$) | 6964.8 8 | 27009, 10, 11, 12 |
| Annual net income per person 2012 (US$) | 30008 | 12009, 10, 11, 12 |
| Annual disposable income per person 2012 (US$) | 15388 | 7509, 10, 11, 12 |
| % of annual disposable income spent on diet 2012 | 40%8 | 20%9, 10, 11, 12 |
| % of animal products in diet (as opposed to plant food) 2012 | > 30%8 | < 10%9, 10, 11, 12 |
| % of people that regularly exercise 2010 | 60%8 | 10%9, 10, 11, 12 |
| % of people employed inmanual labour 2010 | 20%8 | 70%9, 10, 11, 12 |
| % daily smoker men 2010 | 35%8 | 40%9, 10, 11, 12 |
| % habitual alcohol drinker men 2010 | 38%8 | 25%9, 10, 11, 12 |
| Fertility rate 2012 | 1.18 | 1.89, 10, 11, 12 |
| Age of menarch 2012 (years) | 12.08 | 13.09, 10, 11, 12 |
| Age at first birth 2012 (years) | 278 | 239, 10, 11, 12 |
| Age at menopause 2012 (years) | 55.88 | 55.59, 10, 11, 12 |
| Breastfeeding 2012 | 60%8 | 95% 9, 10, 11, 12 |
| Household automobile 2015 (%) | 408 | 129, 10, 11, 12 |
| Household mobile phone 2015 (%) | 1008 | 909, 10, 11, 12 |
| Household refrigerator 2015 (%) | 1008 | 609, 10, 11, 12 |
| % overweight male (BMI ≥ 24 kg/m2) 18–69 years, 2004 | 43.713, 14 | 30.213 |
| % overweight female (BMI ≥ 24 kg/m2) 18–69 years, 2004 | 36.713, 14 | 35.413 |
| % obese male (BMI ≥ 28 kg/m2) 18–69 years, 2004 | 19.913, 14 | 14.513 |
| % obese female (BMI ≥ 28 kg/m2) 18–69 years, 2004 | 23.213, 14 | 17.113 |
| % aged < 25 | 31.468 | 36.299, 10, 11, 12 |
| % aged ≥ 65 | 11.158 | 6.989, 10, 11, 12 |
| Life expectancy in 2012 (years) | 758 | 719, 10, 11, 12 |
BMI, body mass index; GDP, gross domestic product.
Comparison of 2012 age standardized incidence rate (ASR) of female breast cancer
Of the 1 217 437 women registered in Shijiazhuang City in 2012, 726 breast cancer cases were diagnosed, for a crude incidence rate of 59.6/1 00 000. Breast cancer accounted for 28.7% of all new cancer cases and was the most commonly diagnosed cancer in women. In contrast, in Shexian in 2012 only 36 breast cancer cases were diagnosed among the 197 416 women, for a crude incidence rate of 18.1/1 00 000. Breast cancer accounted for only 6.6% of all new cancer cases in Shexian women. It was the fifth most common cancer after stomach, esophageal, cervical, and lung cancers.
The ASR of female breast cancer was 3.3 times higher in Shijiazhuang than in Shexian (45.5vs. 13.8/1 00 000; P < 0.01), and the cumulative incidence rate for 0–74 years was 3.5 times higher (5.2% vs. 1.5%; P < 0.01). These differences between Shijiazhuang and Shexian are much larger than the corresponding differences reported between 77 Chinese cities and 100 Chinese counties for 2011 (31.6 vs. 20.1/1 00 000, P < 0.05; 3.5% vs. 2.2%, P < 0.05, respectively) (Table 2).3
Table 2.
Comparison of female breast cancer incidence rates
| Age group | Urban Shijiazhuang 2012 | Rural Shexian 2012 | 77 Chinese cities 2011† | 100 rural counties 2011† |
|---|---|---|---|---|
| 0~ | 0.00 | 0.00 | 0.00 | 0.00 |
| 1~ | 0.00 | 0.00 | 0.00 | 0.00 |
| 5~ | 0.00 | 0.00 | 0.05 | 0.00 |
| 10~ | 0.00 | 0.00 | 0.00 | 0.00 |
| 15~ | 0.00 | 0.00 | 0.00 | 0.16 |
| 20~ | 0.00 | 0.00 | 1.04 | 1.27 |
| 25~ | 7.37 | 5.29 | 4.54 | 5.16 |
| 30~ | 22.84 | 7.59 | 13.81 | 11.37 |
| 35~ | 41.52 | 15.57 | 33.28 | 25.39 |
| 40~ | 77.42 | 21.36 | 61.29 | 48.90 |
| 45~ | 136.96 | 46.52 | 93.09 | 68.33 |
| 50~ | 150.13 | 57.40 | 100.80 | 63.64 |
| 55~ | 153.57 | 49.10 | 106.99 | 72.58 |
| 60~ | 159.09 | 30.17 | 96.21 | 61.63 |
| 65~ | 127.56 | 32.09 | 91.27 | 44.65 |
| 70~ | 165.09 | 28.36 | 87.65 | 38.76 |
| 75~ | 88.37 | 37.00 | 82.30 | 32.56 |
| 80~ | 27.88 | 0.00 | 72.84 | 24.96 |
| 85+ | 8.37 | 0.00 | 48.85 | 15.81 |
| Crude rate (1/105) | 59.63 | 18.24 | 46.74 | 28.43 |
| ASR (China) (1/105) | 48.54 | 11.33 | 33.66 | 22.59 |
| ASR (1/105) | 45.52 | 13.83 | 31.63 | 20.96 |
| Cum rate 0–74 years (%) | 5.18 | 1.47 | 3.45 | 2.21 |
Source Jia et al, 2015.3 ASR, age standardized incidence rate.
In addition to female breast cancer, the ASR of lung cancer in men in Shijiazhuang was also significantly higher than in Shexian (46.5 vs. 30.0/1 00 000; P < 0.01), but not in women (19.0 vs. 20.8/1 00 000). Other significantly higher cancer incidence included colorectal (22.8 vs. 11.9/1 00 000, P < 0.01 in men; 14.9 vs. 9.3/1 00 000, P < 0.01 in women), kidney (6.9 vs. 2.2/1 00 000, P < 0.05 in men; 3.9 vs. 0.5/1 00 000, P < 0.05 in women), pancreatic (3.1 vs. 0.1/1 00 000, P < 0.01 in men; 2.4 vs. 0.8/1 00 000, P < 0.10 in women), thyroid (1.9 vs. 0.1/1 00 000, P < 0.05 in men; 3.9 vs. 0.8/1 00 000, P < 0.05 in women), prostate (5.3 vs. 0.7/1 00 000, P < 0.01), and ovarian cancer (7.0 vs. 2.1/1 00 000, P < 0.05) (Table 3).
Table 3.
Comparison of ASR of major cancer types, 2012
| Tumor site | Cases | Rank | Incidence rate (1/105) | Percentage (%) | ASR World (1/105) | P † | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| USZ | RSX | USZ | RSX | USZ | RSX | USZ | RSX | USZ | RSX | ||
| Male | |||||||||||
| Lung (C33–34) | 786 | 72 | 1 | 3 | 67.9 | 33.4 | 25.2 | 9.3 | 46.5 | 30.0 | < 0.01 |
| Stomach (C16) | 469 | 389 | 2 | 1 | 40.5 | 180.4 | 15.1 | 50.2 | 28.5 | 162.0 | < 0.01 |
| Colorectal (C18–21) | 381 | 29 | 3 | 5 | 32.9 | 13.7 | 12.2 | 3.7 | 22.8 | 11.9 | < 0.01 |
| Liver (C22) | 279 | 46 | 4 | 4 | 24.1 | 21.3 | 9.0 | 5.9 | 17.4 | 18.5 | |
| Esophagus (C15) | 266 | 172 | 5 | 2 | 23.0 | 79.8 | 8.5 | 22.2 | 15.7 | 72.1 | < 0.01 |
| Kidney (C64–66,68) | 114 | 5 | 6 | 8 | 9.9 | 2.3 | 3.7 | 0.6 | 6.9 | 2.2 | < 0.05 |
| Prostate (C61) | 106 | 2 | 7 | 10 | 9.2 | 0.9 | 3.4 | 0.3 | 5.3 | 0.7 | < 0.01 |
| Leukemia (C91–95) | 104 | 9 | 8 | 6 | 9.0 | 4.2 | 3.3 | 1.2 | 6.5 | 4.0 | < 0.20 |
| Bladder (C67) | 101 | 5 | 9 | 8 | 8.7 | 2.3 | 3.2 | 0.6 | 5.8 | 3.0 | < 0.20 |
| Lymphoma (C81–85,88,90,96) | 100 | 8 | 10 | 7 | 8.6 | 3.7 | 3.2 | 1.0 | 6.3 | 3.1 | < 0.10 |
| Pancreas (C25) | 50 | 0 | 11 | 11 | 4.3 | 0.0 | 1.6 | 0.0 | 3.1 | 0.1 | < 0.01 |
| Larynx (C32) | 39 | 4 | 12 | 9 | 3.4 | 1.9 | 1.3 | 0.5 | 2.4 | 1.6 | |
| Gallbladder (C23–24) | 38 | 4 | 13 | 9 | 3.3 | 1.9 | 1.2 | 0.5 | 2.4 | 1.6 | |
| Thyroid (C73) | 29 | 0 | 14 | 11 | 2.5 | 0.0 | 0.9 | 0.0 | 1.9 | 0.1 | < 0.05 |
| Brain (C70–72) | 27 | 9 | 15 | 6 | 2.3 | 4.2 | 0.9 | 1.2 | 2.0 | 4.5 | < 0.05 |
| Nasopharynx (C11) | 21 | 5 | 16 | 8 | 1.8 | 2.3 | 0.7 | 0.6 | 1.3 | 2.1 | |
| Bone (C40–41) | 14 | 9 | 17 | 6 | 1.2 | 4.2 | 0.4 | 1.2 | 0.9 | 4.1 | < 0.01 |
| All Male Cancer | 3114 | 775 | 269.1 | 359.5 | 100.0 | 100.0 | 187.5 | 325.2 | < 0.01 | ||
| Female | |||||||||||
| Breast (C50) | 726 | 36 | 1 | 5 | 59.6 | 18.2 | 28.7 | 6.6 | 45.5 | 13.8 | < 0.01 |
| Lung (C33–34) | 346 | 46 | 2 | 4 | 28.4 | 23.1 | 13.7 | 8.4 | 19.0 | 20.8 | |
| Colorectal (C18–21) | 260 | 22 | 3 | 7 | 21.4 | 11.1 | 10.3 | 4.0 | 14.9 | 9.3 | < 0.05 |
| Stomach (C16) | 137 | 166 | 4 | 1 | 11.3 | 83.2 | 5.4 | 30.3 | 7.7 | 71.5 | < 0.01 |
| Cervix (C53) | 132 | 64 | 5 | 3 | 10.8 | 32.1 | 5.2 | 11.7 | 8.4 | 25.0 | < 0.01 |
| Corpus uteri (C54) | 126 | 18 | 6 | 8 | 10.4 | 9.0 | 5.0 | 3.3 | 7.9 | 7.0 | |
| Ovary (C56) | 112 | 6 | 7 | 11 | 9.2 | 3.0 | 4.4 | 1.1 | 7.0 | 2.1 | < 0.05 |
| Lymphoma (C81–85,88,90,96) | 93 | 6 | 8 | 11 | 7.6 | 3.0 | 3.7 | 1.1 | 5.5 | 2.5 | < 0.10 |
| Esophagus (C15) | 79 | 86 | 9 | 2 | 6.5 | 43.1 | 3.1 | 15.7 | 4.1 | 36.2 | < 0.01 |
| Liver (C22) | 74 | 30 | 10 | 6 | 6.1 | 15.0 | 2.9 | 5.5 | 4.2 | 13.3 | < 0.01 |
| Leukemia (C91–95) | 66 | 8 | 11 | 10 | 5.4 | 4.0 | 2.6 | 1.5 | 4.6 | 5.3 | |
| Thyroid (C73) | 60 | 2 | 12 | 15 | 4.9 | 1.0 | 2.4 | 0.4 | 3.9 | 0.8 | < 0.05 |
| Kidney (C64–66,68) | 60 | 1 | 12 | 16 | 4.9 | 0.5 | 2.4 | 0.2 | 3.9 | 0.5 | < 0.05 |
| Pancreas (C25) | 44 | 2 | 13 | 15 | 3.6 | 1.0 | 1.7 | 0.4 | 2.4 | 0.8 | < 0.10 |
| Bladder (C67) | 21 | 4 | 14 | 13 | 1.7 | 2.0 | 1.7 | 0.2 | 1.4 | 2.0 | |
| Gallbladder (C23–24) | 20 | 5 | 15 | 12 | 1.6 | 2.5 | 0.8 | 0.9 | 1.3 | 2.3 | |
| Brain (C70–72) | 12 | 18 | 16 | 8 | 1.0 | 9.0 | 0.5 | 3.3 | 1.0 | 7.3 | < 0.01 |
| Bone (C40–41) | 11 | 9 | 17 | 9 | 0.9 | 4.5 | 0.4 | 1.6 | 0.8 | 4.0 | < 0.01 |
| Nasopharynx (C11) | 9 | 0 | 18 | 17 | 0.7 | 0.0 | 0.4 | 0.0 | 0.7 | 0.0 | |
| Larynx (C32) | 1 | 3 | 19 | 14 | 0.1 | 1.5 | 0.0 | 0.5 | 0.1 | 1.1 | < 0.01 |
| All Female Cancer | 2527 | 547 | 207.6 | 274.2 | 100.0 | 100.0 | 150.4 | 230.7 | < 0.01 | ||
Calculated using the approximate method for the comparison of incidence of a disease in two groups as described in Esteve et al. 1994.7
ASR, age‐standardized incidence rate; RSX, rural Shexian; USZ, urban Shijiazhuang.
Conversely, the ASR of stomach cancer in men in Shexian is 5.7 times higher than in Shijiazhuang (162.0 vs. 28.5/1 00 000; P < 0.01) and 9.3 times higher in women (71.5 vs. 7.7/1 00 000; P < 0.01); esophageal cancer is 4.6 times higher in men (72.1 vs. 15.7/1 00 000; P < 0.01) and 8.8 times higher in women (36.2 vs. 4.1/1 00 000; P < 0.01); and liver cancer is 3.2 times higher in women (13.3 vs. 4.2/1 00 000; P < 0.01). In addition to upper gastrointestinal cancer, the ASR of cervical cancer is three times higher in Shexian compared to Shijiazhuang women (25.0 vs. 8.4/1 00 000; P < 0.01). All of these cancer types are infection‐related, associated with disadvantaged socioeconomic development (Table 3).
Socioeconomic development and urbanization and risk factors for non‐communicable diseases between 2000–2015 in rural Shexian County
Shexian is traditionally a rural agrarian county, but as is the case in most of eastern and central China, rapid socioeconomic development and urbanization has taken place since 1978, particularly in the last two decades. From 2000 to 2015, a boom in real estate development led to a shift in the economy from agricultural and heavy industry toward service and tourism. Overall, the annual GDP of Shexian County increased from US$860 to US$3000.9, 10, 11, 12 In addition to increasing income and supply of manufactured food, a transition in diet has gradually take place, with the staple starch food or soybean formerly consumed replaced by increasing proportions of high‐energy animal products, such as saturated fat, meat, eggs, and milk. In recent decades, most young or middle‐aged villagers joined the rural–urban migrant population. From 2000 to 2015, the proportion of town residents increased from 22.4% (85 000/3 80 000) to 54.8% (230 000/4 20 000), representing an increase of 170%, with an annual increase of 10.7%.9, 10, 11, 12 As a result of the altered diet, reduced physical activity, and migration from a rural to an urban environment, lifestyles are becoming increasingly westernized.
In addition to rural–urban migration, the construction of cement or bitumen roads linking villages to the town had commenced in 2000 and was completed by the end of 2005, thus reaching all 580 villages.9, 10, 11, 12 Each day, buses run between the town and villages, picking up villagers to and from work and shopping. Thus, the villagers’ diet has also changed. Consumption of sausage, soda, and potato chips has become common in children. In the past, walking was the principle means of transportation in this mountainous area, but now with greatly improved road conditions, more and more villagers are in possession of cars and motorbikes.
In parallel with economic growth and urbanization, the prevalence of an overweight condition (body mass index [BMI] ≥ 24 kg/m2) in women aged 18–69 in Shexian tripled from 1991 (11.0%) to 2010 (33.0%), and the prevalence of obesity (BMI ≥ 28 kg/m2) in women aged 18–69 reached 15% in 2010 (Table 1).13 Meanwhile, the county has also experienced rapid population aging. The proportion of residents aged ≥ 60 increased from 7.9% in 2000 to 13.9% in 2015.9, 10, 11, 12 Women in Shexian rarely smoke or drink alcohol. As a result of the one child policy that was in place from 1978 to 2013, the total fertility rate has remained stable at 1.8 in Shexian County from 2000 through 2015.9, 10, 11, 12 We retrospectively surveyed the average age of menarche using a randomly chosen sample of high school girls, and observed a decrease from age 13.8 years in 2000 to 12.4 years in 2015.
Increasing female breast cancer incidence and positive correlation with GDP growth in rural Shexian County, 2000–2015
In JoinPoint Analysis, the biennial ASR of female breast cancer in Shexian County between 2000 and 2015 increased over 500% from 2.8/1 00 000 to 17.3/1 00 000 (average biennial percent change [ABPC] = +10.2%; P < 0.01) (Table 4, Fig 3). In Pearson correlation analysis, a significant positive correlation was observed between increasing biennial ASR of breast cancer and the biennially averaged GDP (r = 0.94, P < 0.01) (Table 4).
Table 4.
Biennial ASR of female breast cancer 2000–2015 and average biennial GDP in Shexian County
| 2000–2001 | 2002–2003 | 2004–2005 | 2006–2007 | 2008–2009 | 2010–2011 | 2012–2013 | 2014–2015 | ABPC1–8 ^ | P < | |
|---|---|---|---|---|---|---|---|---|---|---|
| Standardized incidence rates (1/100) | ||||||||||
| Breast (C50) | 2.8 | 5.5 | 5.5 | 12.6 | 15.1 | 15.5 | 18.1 | 17.3 | 10.2 | 0.00** |
| GDP US$ | 880 | 1175 | 1480 | 1765 | 2050 | 2180 | 2710 | 2950 | ||
P < 0.01.
ABPC, average biennial percent change; ASR, age standardized incidence rate; GDP, gross domestic product.
Figure 3.
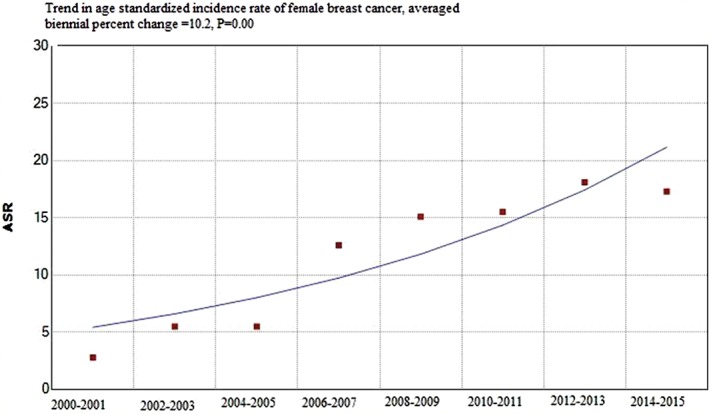
Trends in biennial age standardized incidence rates (ASR) of female breast cancer in rural Shexian County between 2000 and 2015 by JoinPoint Analysis 4.2.0.2. Average biennial percent change 10.2, P = 0.00.
Notably, although breast cancer incidence increased significantly between 2000 and 2015 in Shexian county, parallel with socioeconomic development and urbanization, by 2012, the ASR was still less than a third of the rate in Shijiazhuang City (13.8 vs. 45.5/1 00 000; P < 0.01), while the GDP per capita was US$ 2700 vs. US$6964, respectively. These results suggest that this trend will continue to increase in Shexian.
Discussion
Worldwide breast cancer incidence increases with industrialization and urbanization
Worldwide, the incidence of breast cancer increases in parallel with socioeconomic development. According to GLOBOCAN 2012, the ASR in developed countries (73.4/1 00 000) was 2.4 times higher than in developing countries (31.3/1 00 000).4 In the present study, we found that although Shijiazhuang and Shexian had had a similar agrarian economy before 1953, 60 years of unequal development since then has resulted in significant urban–rural disparity in breast cancer incidence: 45.5 vs. 13.8/1 00 000 in 2012. This difference is much larger than that reported between 77 Chinese tumor registration cities and 100 counties in 2011 (31.6 vs. 21.0/1 00 000).3
Although GLOBOCAN 2012 reported that breast cancer ASR incidence in China was among the lowest of all countries,4 since that time rapid social economic development and changing reproductive patterns have seen the Chinese rate increase twice as fast as the average global rate.1 By 2012, the ASR of female breast cancer in Shijiazhuang city (45.5/1 00 000) reached the level of countries with a high human development index (45.2/1 00 000),4 about half of the rate of Northern American women (91.6/1 00 000).4 Although the rate in Shexian County was still low in 2012 (13.8/1 00 000), it increased over 500% between 2000 and 2015, from 2.8 to 17.3 per 100 000, with an ABPC of +10.2% (P < 0.01).
Breast cancer burden expected to increase in China
Because of significant disparity in socioeconomic development, modernization and urbanizationin, China still has a long way to go. Hong Kong is the most westernized city in China, with the highest breast cancer incidence of all Chinese cities; however, this rate is still lower than Singapore.15 In Hong Kong, the ASR of female breast cancer rose on average 1.7% per annum between 1976 and 2010. On the basis of these trends, Wong et al. predicted that the female breast cancer ASR would increase from 56.7 in 2011–2015 to 62.5/1 00 000 in 2021–2025.16 Between 2010 and 2015, urbanization in China was taking place at a rate of 3.1% annually. By 2015, 55.6% of the Chinese population had moved into cities, leading to a percentage of city dwellers 29.4% higher than in 1990.17 Generations of women affected by the family planning program (implemented from the late 1970s until the early 2010s) have not reached the peak age of incidence (around 50 years old), thus the effect of the family planning program has not yet been fully realized. As a result of these factors, breast cancer incidence is expected to increase in the coming years.
Breast cancer prevention
Marked urban–rural disparity and the rising rate of breast cancer incidence in parallel with socioeconomic development and urbanization suggest breast cancer is preventable.18 The American Cancer Society Guidelines on nutrition and physical activity for cancer prevention recommend maintaining a healthy body weight, increasing physical activity, and minimizing alcohol intake to reduce the risk of developing breast cancer.19 Based on the distribution of major breast cancer risk factors in a representative sample of Mainland Chinese women (n = 17 078) participating in the Chinese National Family Planning and Reproductive Health Survey, Linos et al. predicted modest reductions in menopausal hormone and alcohol use, and that weight maintenance could prevent 270 000 of the 2.5 million cases of breast cancer that would occur by 2021 (among the total population of 130.3 million Chinese women aged 35–49 years in 2001).1, 20
In conjuction with the prevention measures recommended for adults, dietary patterns in childhood have a significant effect on the risk of breast cancer. In a study of Asian emigrants to Hawaii and the United States mainland, mothers recalled their children's diets during different age periods. The results indicated that soy offers protection against breast cancer in those who have a high intake during childhood, but that the effect decreases in adolescence and adulthood.21 A prospective cohort study from China confirmed this finding.22 In recent decades in China, however, western‐style fast food and high‐sugar drinks have become more and more popular among children and fried chicken, hot sausages, or processed meat have replaced the traditional Chinese diet of soybeans or puffed rice. Overweight and obese conditions have increased and the age of menarche among girls has significantly decreased as a result of these high calorie and high fat diets. Ma et al. reported that the age of menarche among urban Chinese girls decreased from 13.5 years in 1979 to 12.27 years between 2003 and 2005.23 A study by Iqbal et al. found that each year decrease in the age of menarche significantly increased the risk of breast cancer (odds ratio 1.67, 95% confidence interval 1.09–2.56; P = 0.02).24 Considering that childhood and adolescent exposure has a significant impact on adult breast cancer risk, limiting the development of an unhealthy food industry aimed at children should be a priority in China.25
The predominance of breast cancer cases in younger women has been observed in Mainland China since the 1980s. In 2008, breast cancer was diagnosed in 78% of women aged < 65 in China, compared to 57% in the United States.26 In China, the increasing ASR of breast cancer is particularly rapid in women aged < 50. The rate peaks at 50 years of age and then subsequently plateaus or declines. This pattern suggests that exposure to breast cancer risk factors differs significantly between women born before and after westernization. However, as the older generation dies out and the birth cohort effect disappears, age distribution will gradually approach that of western countries.26 In the present study, the age distribution in Shexian County was younger than in Shijiazhuang city, and that in 100 Chinese counties was younger than in 77 cities (Fig 4).The predominance of younger breast cancer cases is biologically relvant. The positive rate of hormone receptor in these younger patients is significantly lower than in breast cancer patients aged ≥ 50.26 Because hormone receptor‐negative breast cancer is generally more aggressive than positive, such as basal‐like cancer or triple negative breast cancer, younger breast cancer patients have a poorer prognosis on average than postmenopausal women with breast cancer in China.26 A recent meta‐analysis including 21 941 breast cancer patients and 864 177 controls concluded that breast feeding was associated with a reduced risk of developing triple‐negative breast cancer (odds ratio 0.79, 95% confidence interval 0.66–0.94; P = 0.01).27 Therefore, encouraging breastfeeding as a preventive policy may produce a positive effect in China, especially after the one child policy was discontinued in 2013.
Figure 4.
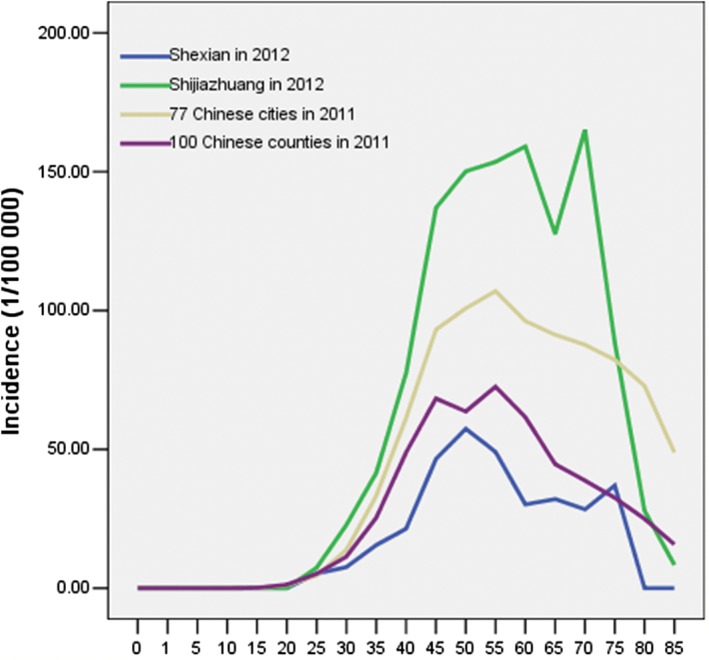
Urban–rural comparison of age‐specific incidence curves of female breast cancer in China.
Another major concern with breast cancer in China is that although the incidence and mortality rates are low at present, the prognosis is very poor, especially in rural women. The five‐year relative survival rate of breast cancer in Chinese women was only 73.0% in 2003–200528 compared to 91% in American women in 2005–2011.29 Along with differences in treatment practices between the two countries,26 another important cause for the substantial difference in survival is the stage at which the cancer is detected. Less than 1% of breast cancer patients in China were detected with carcinoma in situ at diagnosis in 1999–2008,30 whereas in the United States the proportion was 20% in both non‐Hispanic white and African American women in 2013.31 This difference is determined to a large extent by different screening techniques. Although population‐based breast cancer screening has been practiced for nearly half a century in developed countries and breast cancer has been proven as one of the few cancers for which screening is a successful weapon, the coverage of mammography screening for breast cancer is still very low in China. The overall mammography screening rate in China was only 21.7% in 2010,32 while population‐based mammography screening in America women was 68.5% in 2008.33 Therefore, specific screening schemes tailored for high‐risk groups, such as women with low birth rates, reduced breastfeeding, obesity, or a positive family history of cancer should be incorporated into primary health service programs.
Previous studies of urban–rural disparity in cancer in China have defined urban or rural population according to administration level.34 Prefecture‐level cities (e.g. a province‐governing city) or municipalilies are considered urban, while county or county‐level cities are regarded as rural. However, in addition to the urban and suburban population, a typical Chinese prefecture‐level city also includes several rural counties. When the latter are misclassified as urban, the real urban–rural difference is diluted. For example, the difference in ASR of female breast cancer in 77 Chinese cities (31.6/1 00 000) and 100 counties (21.0/1 00 000) reported by Jia et al. 3 was much smaller than that reported between more and less developed countries in GLOBOCAN 2012 (73.4 vs. 31.3 per 100 000).4 This may also explain the inconsistent results for urban–rural disparity in cancer so far reported in China.34, 35 As a result, we limited our comparison to pure urban and rural female populations and found a much larger disparity (45.5/1 00 000 vs. 13.8/1 00 000).
A limitation of this study may lie in the representativeness of Shexian County for rural China. Because Shexian County has been endemic for esophagogastric cancers, it may be socioeconomically more disadvantaged than other counties in China and may have a somewhat lower incidence rate of breast cancer in women. However, situated in northern central China, Shexian County is socioeconomically more developed than most counties in southwestern and northwestern China. In 2010, it had a total product value of 21.4 billion RMB yuan (US$3.6 billion). Its economy was ranked 19th during 2001–2005 and 13th during 2006–2010 among 136 counties in Hebei province.11
In conclusion, we found a threefold urban–rural disparity in the breast cancer incidence rate between sample rural and urban regions in China.The rate in urban Chinese women has reached the level of countries with a high human development index, according to GLOBOCAN 2012. The rate in both urban and rural settings will continue to increase in parallel with socioconomic development and urbanization. To reduce the increasing burden, interventions targeted at modifiable risk factors, such as improving the quality of food provided to children, weight control to avoid overweight or obese conditions, giving birth at a younger age, and increases in physical activity, breastfeeding, and breast cancer screening, should be incorporated into public health programs.
Disclosure
No authors report any conflict of interest.
Acknowledgments
This work was supported by the Key Medical Research Subjects in Hebei Province (2012, No.2056), and by the Key Subject Development Program in universities of Hebei province, headed by ProfessorBaoen Shan, 4th Hospital of Hebei Medical University.
References
- 1. Linos E, Spanos D, Rosner BA et al Effects of reproductive and demographic changes on breast cancer incidence in China: A modeling analysis. J Natl Cancer Inst 2008; 100: 1352–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ministry of Health . National Health Services Survey 2003. Peking Union Medical University Press, Beijing: 2004. [Google Scholar]
- 3. Jia M, Zheng R, Zhang S, Zeng H, Zou X, Chen W. Female breast cancer incidence and mortality in 2011, China . J Thorac Dis 2015; 7: 1221–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87–108. [DOI] [PubMed] [Google Scholar]
- 5. Wen DG, Zhang N, Shan B, Wang S. Helicobacter pylori infection may be implicated in the topography and geographic variation of upper gastrointestinal cancers in the Taihang Mountain high‐risk region in northern China. Helicobacter 2010; 15: 416–21. [DOI] [PubMed] [Google Scholar]
- 6. Doll R, Payne P, Waterhouse J, eds. Cancer Incidence in Five Continents: A Technical Report. Springer‐Verlag, Berlin: 1966. [Google Scholar]
- 7. Esteve J, Benhamou E, Raymond L, eds. Techniques for the analysis of cancer risk In: Statistical Methods in Cancer Research. Vol. IV. Descriptive Epidemiology IARC Scientific Publications 128, Lyon: 1994; 74–7. [PubMed] [Google Scholar]
- 8. Elivecity Research Group . Gross Domestic Production in Chinese Cities in 2012. Development History of Shijiazhuang City 2013. [Cited 21 Oct 2017.] Available from URL: http://tieba.baidu.com/p/2417841476.
- 9. Shexian Bureau of Reform and Development . [Socioeconomic Development in Shexian(2011–2015)] 2011. (In Chinese.) [Cited 15 May 2017.] Available from URL: http://www.docin.com/p-511099233.html.
- 10. Hebei News Network . Website of Shexian County. 2017. [Cited 21 Oct 2017.] Available from URL: http://shexian.hebnews.cn/node_26370.html.
- 11. Government of Shexian County . China Shexian. 2017. (In Chinese.) [Cited 15 May 2017.] Available from URL: http://www.sx.hd.gov.cn/sxxq/sxgk.htm.
- 12. Department of Propaganda . Shexian County. 2017. (In Chinese.) [Cited 15 May 2017.] Available from URL: http://www.sxsxw.cn/
- 13. Li H, Wang LN, Zhu JQ, Zhang JY, Zhang ZC. [A analysis of body mass parameters of urban and rural adults residents in Hebei province in 2004.]. Chin J Prev Contr Chron Non‐Commun Dis 2006; 14: 250–3 (In Chinese.) [Google Scholar]
- 14. Ma XM, Ma WH. [Prevalence of risk factors of non‐communicable chronic disease in a community in Shijiazhuang City.]. Hebei Med J 2010; 32: 3556–7 (In Chinese.) [Google Scholar]
- 15. Ferlay J, Shin HR, Bray F et al GLOBOCAN 2008 Version1.2, Cancer Incidence and Mortality Worldwide. International Agency for Research on Cancer, Cancer BaseNo. 10. IARC, Lyon: 2010. [Cited 2 May 2017.] Available from URL: http://globocan.iarc.fr. [Google Scholar]
- 16. Wong IO, Schooling CM, Cowling BJ, Leung GM. Breast cancer incidence and mortality in a transitioning Chinese population: Current and future trends. Br J Cancer 2015; 112: 167–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Central Intelligence Agency . The World Factbook 2014. [Cited 27 Feb 2014.] Available from URL: https://www.cia.gov/library/publications/the-world-factbook/geos/ch.html.
- 18. Colditz GA, Sellers TA, Trapido E. Epidemiology ‐ identifying the causes and preventability of cancer? Nat Rev Cancer 2006; 6: 75–83. [DOI] [PubMed] [Google Scholar]
- 19. Kushi LH, Doyle C, McCullough M et al American Cancer Society guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 2012; 62: 30–67. [DOI] [PubMed] [Google Scholar]
- 20. Ding QJ, Hesketh T. Family size, fertility preferences, and sex ratio in China in the era of the one child family policy: Results from national family planning and reproductive health survey. BMJ 2006; 333: 371–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Korde LA, Wu AH, Fears T et al Childhood soy intake and breast cancer risk in Asian American women. Cancer Epidemiol Biomarkers Prev 2009; 18: 1050–9. [DOI] [PubMed] [Google Scholar]
- 22. Lee SA, Shu XO, Li H et al Adolescent and adult soy food intake and breast cancer risk: Results from the Shanghai Women's Health Study. Am J Clin Nutr 2009; 89: 1920–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ma HM, Du ML, Luo XP et al Onset of breast and pubic hair development and menses in urban Chinese girls. Pediatrics 2009; 124: e269–77. [DOI] [PubMed] [Google Scholar]
- 24. Iqbal J, Ferdousy T, Dipi R et al Risk factors for premenopausal breast cancer in Bangladesh. Int J Breast Cancer 2015; 2015: 612042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Colditz GA, Frazier AL. Models of breast cancer show that risk is set by events of early life: Prevention efforts must shift focus. Cancer Epidemiol Biomarkers Prev 1995; 4: 567–71. [PubMed] [Google Scholar]
- 26. Fan L, Strasser‐Weippl K, Li JJ et al Breast cancer in China. Lancet Oncol 2014; 15: e279–89. [DOI] [PubMed] [Google Scholar]
- 27. Lambertini M, Santoro L, Del Mastro L et al Reproductive behaviors and risk of developing breast cancer according to tumor subtype: A systematic review and meta‐analysis of epidemiological studies. Cancer Treat Rev 2016; 49: 65–76. [DOI] [PubMed] [Google Scholar]
- 28. Zeng HM, Zheng RS, Guo Y et al Cancer survival in China, 2003–2005: A population‐based study. Int J Cancer 2015; 136: 1921–30. [DOI] [PubMed] [Google Scholar]
- 29. Siegel RL, Miller KD, Jemal A et al Cancer statistics, 2016. CA Cancer J Clin 2016; 66: 7–30. [DOI] [PubMed] [Google Scholar]
- 30. Wang Q, Li J, Zheng S et al Breast cancer stage at diagnosis and area‐based socioeconomic status: A multicenter 10‐year retrospective clinical epidemiological study in China. BMC Cancer 2012; 12: 122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. DeSantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin 2014; 64: 52–62. [DOI] [PubMed] [Google Scholar]
- 32. Wang B, He M, Wang L, Engelgau MM, Zhao W, Wang L. Breast cancer screening among adult women in China, 2010. Prev Chronic Dis 2013; 10: E183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Breen N, Gentleman JF, Schiller JS. Update on mammography trends: Comparisons of rates in 2000, 2005, and 2008. Cancer 2011; 117: 2209–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Wang N, Yuan YN, Zheng RS et al [An analysis on difference of cancer incidence between urban and rural areas in China, 2009.]. China Cancer 2013; 22: 168–73 (In Chinese.) [Google Scholar]
- 35. Chen WQ, Zheng RS, Baade P et al Cancer statistics in China 2015. CA Cancer J Clin 2016; 66: 115–32. [DOI] [PubMed] [Google Scholar]