

Abstract
The separate and combined efficacy of a social norms and a self-affirmation intervention to motivate decreased sugar-sweetened beverage (SSB) consumption was examined in two experiments. College students were randomly assigned to receive information about SSB consumption risks, norms, both, or neither. In addition, participants performed either a self-affirmation or control task. Self-affirmation only weakly affected SSB consumption intentions and behaviors. However, participants in Experiment 2 who received risks information, norms information, or both reported greater SSB reduction intentions than did those who received no information. Two-weeks later, those who received both types of information reported more frequent behavior change preparations, and it appears this effect may have been partially mediated by the changes in intentions to reduce SSB consumption.
Keywords: social norms, self-affirmation, sugar-sweetened beverage consumption, intentions
There is increasing concern about the health risks of added dietary sugar, particularly when consumed in sugar-sweetened beverages (SSBs) that contain no essential nutrients (e.g., sodas, sports drinks, energy drinks). SSBs are the largest contributor of added sugar intake and a significant source of calories in the United States (US; Huth, Fulgoni, Keast, Park, & Auestad, 2013) and around the world (Popkin & Nielson, 2003). In the US, the consumption of SSBs doubled across all age groups between 1977 and 2002 (Brownell et al, 2009), and there was a concomitant dramatic increase in the prevalence of obesity (from 22.9% among adults and 10.5% among adolescents in 1988 to 37.7% and 20.6%, respectively, in 2014; Flegal, Kruszon-Moran, Carroll, Fryar, & Ogden, 2016; Ogden et al., 2016). In addition to being implicated in weight gain and obesity (Harrington, 2008; Malik, Schulze, & Hu, 2006), SSB intake has been linked to a variety of other health risks, including Type 2 diabetes (Imamura et al., 2016), hypertension, coronary heart disease, stroke (Anand et al., 2015), and even poor cognitive function (Crichton, Elias, & Torres, 2016; Ye, Gao, Scott, et al., 2011).
One group that tends to have particularly high SSB consumption rates is young adults—especially college students (Huffman & West, 2007; West et al., 2006). Indeed, one study found that 65% of undergraduates reported drinking at least one SSB daily (West et al., 2006). Moreover, this group also may be at an increased risk of consuming particularly unhealthy SSBs, such as energy drinks, given their college-related demands (Han & Powell, 2013; Kit, Fakhouri, Park, Nielsen, & Odgen, 2013). Further, the social engineering-based approaches that have often been employed with children, such as installing more water fountains (Ebbeling et al., 2012; Ritenbaugh et al., 2003; Sichieri, Paula Trotte, de Souza, & Veiga, 2009) and banning SSBs in school vending machines (Fletcher, Frisvold, & Tefft, 2010; Taber, Chriqui, Powell, & Chaloupka, 2012) may not be as successful among college students because they have greater freedom and independence (e.g., can buy SSBs off campus; parents are not in control of their diet). Even price increases may not necessarily reduce the consumption of SSBs among college students as one study found that SSB taste was more important than price for this group (Block, Gillman, Linakis, & Goldman, 2013). Therefore, information-based interventions have been the preferred method to reduce SSB consumption among college students. For instance, Bergen and Yeh (2006) found that vending machines with clear labels for beverages that contain no energy (i.e., “0 calories, 0 carbs”) and motivational posters encouraging the consumption of non-energy beverages had a lower growth rate of SSB sales compared to control machines with no labels or posters. In another intervention, Ha, Caine-Bish, Holloman, and Lowry-Gordon (2009) found a reduction in SSB consumption among college students who took a basic nutrition class. Finally, in a behavioral-economics approach, Yang and Chiou (2010) found that when college students were provided money to buy a beverage of their choice they often bought the lower-priced beverage unless they had been exposed to health-concerns information; in that case, they bought the healthy alternative—even when its price was higher. These studies show promising results regarding the effectiveness of information-based interventions for reducing SSB consumption among college students. However, there is certainly room for improvement. One way that the efficacy of a basic information intervention might be enhanced is via social norms information.
Social Norms
Social norms-based interventions have been effective at influencing beliefs and behaviors in a variety of contexts. Cialdini, Reno, and Kalgren (1990) distinguished between two types of social norms: injunctive and descriptive. While injunctive norms refer to an individual’s belief about what should be done based on what others approve or disapprove of, descriptive norms refer to what others actually do. An example of an injunctive norm might be the belief that one should minimize consumption of soda to prevent diabetes, whereas a descriptive norm might be the belief that most people drink soda every day. In the context of health behaviors, it is not uncommon for people to overestimate the acceptance (injunctive norms) and prevalence (descriptive norms) of risk behaviors and consequently to increase their own unhealthy behaviors to match the perceived norm (Miller & McFarland, 1991; Perkins & Berkowitz, 1986; Schroeder & Prentice, 1998). There is now considerable literature that suggests the efficacy of correcting misperceived norms (or establishing conservative norms) for reducing a variety of health risk behaviors including alcohol use (Mattern & Neighbors, 2004; Neighbors, Larimer, & Lewis, 2004), smoking (Balvig & Holmberg, 2011), excessive sun exposure (Mahler, Kulik, Butler, Gerrard, & Gibbons, 2008; Reid & Aiken, 2013), and poor diet/nutrition (Robinson, Thomas, Aveyard, & Higgs, 2014). Although, to our knowledge, no study to date has used a social norms intervention to reduce SSB consumption, at least two studies have shown that individuals tend to overestimate the SSB intake of their peers (Lally, Bartle, & Wardle, 2011; Perkins, Perkins, & Craig, 2010), and one study demonstrated that the perceived norm showed a greater association with participants’ own SSB intake than did the actual SSB consumption of their peers (Perkins, Perkins, & Craig, 2010). These findings provide some support for the notion that the addition of a social norms-based intervention might prove more efficacious than simply informing people of the health risks of SSB consumption. It may also be beneficial to attempt to reduce the defensive reaction that may be produced by receiving health risk information.
Self-Affirmation
Although knowledge about the potential detrimental health effects of a behavior is clearly necessary for behavior change to occur, receiving such information may elicit a defensive reaction. That is, learning that there is scientific evidence that a behavior one has engaged in may have negative health consequences can threaten one’s self-conception as an intelligent, rational, healthful person and thereby may weaken overall self-integrity (Steele, 1988). In an effort to repair self-integrity the individual may react defensively to the health risk information (e.g., dismissing, denying, and/or minimizing the risk; finding flaws in the evidence; Sherman & Cohen, 2006) decreasing the likelihood that behavior change will be undertaken. However, research in a variety of health domains (e.g. sun protection, safe sex, tobacco use, caffeine consumption) indicates that defensive reactions can be reduced via the process of self-affirmation (Armitage, Harris, & Arden, 2011; Harris, Mayle, Mabbott, & Napper, 2007; Sherman, Nelson, & Steele, 2000; see Sherman & Cohen, 2006 for a review). The self-affirmation process highlights an individual’s important values and personal strengths, thereby making salient that overall self-worth is not dependent on any particular behavior and bolstering self-integrity. The individual then becomes more receptive to health risk information instead of feeling a need to marshal defenses. Although apparently not previously examined in the context of SSB consumption, self-affirmation has been demonstrated to increase receptiveness to risk messages concerning consumption of other beverages, specifically alcohol and caffeine (Harris & Napper, 2005; Reed & Aspinwall, 1998; Sherman, Nelson, & Steele, 2000). Thus, there is reason to expect that self-affirmation might also enhance receptiveness to information regarding the risks of SSB consumption.
Overview of Present Experiments
It appears that no previous work has examined the efficacy of either correcting misperceived social norms or affirming the self for decreasing SSB consumption. Further, to our knowledge, no work in any health risk or other domain has investigated the efficacy of the combination of a social norms-based intervention and self-affirmation. In order to examine these issues, two experiments were conducted in which college students were randomly assigned to receive information about the health risks of SSB consumption, social norms information, or both risks and norms information (in the second experiment a no information control condition was included), and also to one of two self-affirmation conditions (control task; self-affirmation task). Given the extensive literature in other health domains regarding the efficacy of the correction of misperceived norms and, separately, the self-affirmation process, we expected that each of these interventions would result in beneficial outcomes with regard to SSB intentions and behaviors. However, given that no previous work has examined the combined effects of social norms and self-affirmation, our predictions regarding the combination of these interventions were necessarily more tentative. On the one hand, one might assume that the combination of two independently efficacious interventions would result in a more powerful, positive effect than each separately. Indeed, if one conceptualizes the correction of misperceived norms as another piece of information that could pose a threat to self-integrity (i.e., even one’s peers are aware of, and taking action against, a health risk that one is engaging in), then self-affirmation would be expected to lower defensiveness and increase receptiveness to both the risks information and the social norms information. If so, one would expect that participants who undergo the self-affirmation process and receive both SSB risks and social norms information would exhibit the highest SSB reduction intentions and behaviors. Alternatively, we also considered the possibility that the self-affirmation process could weaken any effects of the social norms intervention. That is, fortification of self-integrity may result in less concern about (and less impact of) the behavior or approval of others. If this is the case, SSB reduction intentions and behaviors should be highest among participants who receive both the SSB risks and social norms information but who do not undergo the self-affirmation process.
Experiment 1
Method
Participants
143 California State University San Marcos (CSUSM) undergraduates (83% female), aged 18 to 35 years (M = 20.23, SD = 2.52), participated for course credit. The ethnic background of the sample was 9.1% Asian, 32.9% Caucasian, 46.9% Latino/a, 4.2% Multiracial, 0.7% Pacific Islander, 4.9% African-American, and 1.4% Other. First year students comprised 29.4% of the sample, 35.7% were Sophomores, 25.2% were Juniors, and 9.8% were Seniors.
Design and Conditions
Participants were randomly assigned to one of 6 conditions in a 3 (Information Condition: SSB risks information only vs Social norms information only vs SSB risks information + Social norms information) × 2 (Self-affirmation Condition: Control task vs Self-affirmation task) design.
SSB Risks Information
The SSB risks information was presented via a double-sided 8.5” × 11” laminated card. The card contained information and images regarding the potential health risks associated with the consumption of beverages containing added sugar (e.g., obesity and Type 2 diabetes). In addition, the card provided information about the number of teaspoons of sugar contained in typical SSBs, the duration of exercise required to burn the calories in a typical SSB, and tips for reducing SSB consumption.
Correction of Misperceived Social Norms Intervention
Personalized normative feedback (PNF) was employed to correct misperceived descriptive and injunctive social norms. Specifically, participants were provided with a direct comparison of their own perceptions (assessed at baseline; described below) of typical college students’ approval of limiting SSB consumption (injunctive norm) and efforts to minimize SSB consumption (descriptive norm) against the actual normative values. Following the procedures used by Reid and Aiken (2013) in the context of sun protection, the PNF was delivered to each participant via a personally customized feedback sheet. Each participant’s customized PNF sheet contained feedback for two injunctive and two descriptive norm items. The participant’s own baseline perceptions of each norm was handwritten and contrasted with the true norm (measured in a survey of 213 undergraduates several months prior to the present study). For example, one of the descriptive norms feedback items stated, “You thought that _____ % of college students try to avoid consuming sugar sweetened drinks. On average actually 91% of college students try to avoid consuming sugar-sweetened drinks.” (see Reid & Aiken, 2013, pg. 555 for an example of an injunctive norm feedback item). Participants were asked to carefully review the feedback sheet and compare their perceptions with the actual normative values.
Self-Affirmation Task
The self-affirmation technique required participants to list their personal strengths during a two-minute period (Harris, Mayle, Mabbot, & Napper, 2007). The control task required participants to list all of the buildings they pass on their way home (Napper, Harris, & Epton, 2009).
Procedure
Participants were recruited via the Psychology Department Human Participant Pool and were run individually. After signing a consent form, each participant first completed the demographic and baseline measures (described below). Then, depending on his/her randomly assigned condition, completed the self-affirmation or control process, received the SSB risks information, and/or received the social norms information (PNF sheet). Next all participants completed the outcome measures and manipulation checks (described below). Participants were then probed for suspicion (none was detected), debriefed, and thanked for their participation.
Measures
Baseline SSB Consumption and Perceived Norms
At baseline participants completed measures of demographics (e.g., age, gender), their baseline SSB consumption, and their perceptions of the injunctive and descriptive norms for SSB consumption. Participants’ SSB consumption was assessed utilizing a beverage checklist developed for this study. The beverage checklist assessed current beverage consumption practices and was comprised of eight beverage categories including water, sports drinks, energy drinks, tea drinks, coffee drinks, fruit juices, soft drinks, and milk/dairy drinks. Specific common beverages were listed under each category (e.g., the soft drink category listed Coca-Cola, diet Coke, Pepsi, diet Pepsi, Sprite, etc.). The instructions asked participants to check the specific beverages they had consumed on the previous day and to indicate the number of servings consumed (12 oz = 1 serving). An “Other” section was also provided for participants to list beverages not included on the checklist (e.g., alcoholic beverages).
Perceived injunctive norms were assessed with two items. For example, one item stated, “The typical college student believes that avoiding sugar-sweetened drinks is:”. Response options ranged from 1 (extremely bad) to 7 (extremely good). Two items were also used to assess perceived descriptive norms. For example, participants were asked to estimate the percentage of college students who try to avoid consuming sugar-sweetened drinks.
Subjective Norms
We expected that the correction of misperceived injunctive and descriptive norms might influence participants’ perceived subjective norms (an important component of the Theory of Planned Behavior; Azjen & Madden, 1986). To assess subjective norms, a 4-item measure based closely on similar measures utilized in other contexts (e.g., Fishbein & Azjen, 2010) was developed. Specifically, participants rated their degree of agreement with the statements: “Most people who are important to me think that I should minimize my sugar sweetened drink consumption” and “Most of my friends think that I should minimize my sugar sweetened drink consumption” (1=Completely Disagree; 5= Completely Agree). In addition, participants indicated the extent to which most people who are important to them and, separately, their friends would approve if they were to minimize their SSB consumption (1=Strongly Disapprove; 5= Strongly Approve). The four items demonstrated good internal consistency (α = .83) and were thus combined to create an overall subjective norms index.
Intentions
A 9-item scale (based closely on similar measures utilized in other health contexts, e.g., Mahler, Kulik, Gibbons, Gerrard, & Harrell, 2003) was developed to assess intentions to minimize sugar sweetened beverage consumption (α = .88; e.g., “I plan to avoid consuming sugar sweetened drinks entirely”; “I plan to limit my sugar sweetened drink consumption to special occasions only,”). Participants rated their level of agreement with each item on a 5-point scale (1=Strongly Disagree; 5=Strongly Agree).
Manipulation Checks
The manipulation checks for the risks information consisted of four items assessing recall of information provided on the risks card. Specifically, participants were asked to recall the number of teaspoons of sugar contained in a typical can of soda. They then checked the appropriate answers to the following questions: “Sugar sweetened drink consumption is a ___ (minor; moderate; major) contributor to weigh gain and obesity.”; “How long would the average person have to jog to burn the calories in one soda?” (5 min; 10 min; 30 min; 1 hour; 3 hours). Lastly, they answered “yes” or “no” as to whether or not regular soda consumption has been linked to aging.
Four additional items served as manipulation checks for the social norms information. Specifically, participants were asked to report the information they had received regarding the percentage of college students who report that they try to avoid sugar sweetened drink consumption and, separately, the percentage of college students who try to limit themselves to 1–2 sugar sweetened drinks per day. Participants also rated the following statements, “The typical college student believes that avoiding sugar-sweetened drinks is:” (1=extremely bad; 7= extremely good); “The typical college student believes that avoiding sugar-sweetened drinks is:” (1=extremely unimportant; 7=extremely important).
The State Self-Esteem Scale (Heatherton & Polivy, 1991) was used as a manipulation check for the self-affirmation task. This scale consists of 20 items (e.g., “I feel confident about my abilities”; “I am worried about whether I am regarded as a success or failure.”) rated on a 5-point Likert-type scale (1 = not at all; 5 = extremely; α = .91).
Results and Discussion
Preliminary Analyses
Group Equivalence
Means of the demographic and baseline SSB consumption variables were examined to determine the initial equivalence of the conditions. The results indicated only small differences in age ( for main effects and interaction ranged from .00 –.01), gender ( = .00 –.00), ethnicity ( s = .00 –.03), year in college ( = .00 –.03), or reported baseline SSB consumption ( = .00 – .03) across condition. Thus, it appears that participants were effectively randomized to condition.
Risks Information Manipulation Checks
Participants in either of the conditions who reviewed the risks information card were nearly three quarters of a standard deviation more likely to correctly report that SSB consumption is a major contributor to weight gain and obesity (d = .74), and more than a full standard deviation more likely to correctly report that soda consumption had recently been linked to aging (d = 1.14) than were those who did not receive the risks information. Those who received the risks information also provided somewhat higher estimates of the number of teaspoons of sugar in a typical soda (d = .22) and their reports of the number of minutes of jogging required to burn the calories in one soda (30 minutes) were much closer to correct (Ms = 33.06 and 38.48) than the surprisingly higher estimates provided by those who had not received the risks information (M = 83.40). The d of 1.08 for this latter difference indicates that those who had not received the risks information provided jogging minutes estimates that were more than a full standard deviation higher than the generally correct answers provided by those who had received the SSB risks information. Thus, in general it appears that participants paid attention and processed the information provided, and that the information provided on the risks card is not common knowledge.
Social Norms Manipulation Checks
As one would expect, participants in either of the conditions who had received social norms information provided much higher estimates of the percentage of their peers who report that they try to avoid SSB consumption and the percentage of peers who try to limit themselves to 1–2 SSBs per day (Ms ranged from 89.66% to 90.78%) than did those in the SSB risks information-only condition (Ms = 35.85% and 41.48%, respectively). The respective ds of 4.70 and 3.44 indicate that the estimates of those in either of the social norms information conditions were at least three full standard deviations higher than the estimates of those who did not receive the social norms information, which are considered large effect sizes. In addition, those participants who had received the social norms information perceived their peers’ beliefs about avoiding SSBs to be nearly three quarters of a standard deviation more positive (M = 6.06, SD = .25 and M = 6.02, SD = .15 for social norms only and SSB risks + social norms, respectively) than did those who had only received the SSB risks information (M = 5.46, SD = 1.27), d = .73. Finally, participants in either of the social norms conditions reported that their peers believed avoiding SSBs to be more important (M = 5.85, SD = .86 and M = 6.02, SD = .26 for social norms only and SSB risks + social norms, respectively) than did those who had not received social norms information (M = 5.29, SD = 1.29). The difference was over two thirds of a standard deviation (d = .67), which is considered a medium to large effect size.
State Self-esteem
Although participants who had performed the self-affirmation task, as expected, subsequently reported higher state self-esteem (M = 73.17, SD = 12.40) than did those who performed the control task (M = 71.18, SD = 13.39), the difference was small (d = .16).
Primary Analyses
Table 1 provides descriptive information as a function of condition for perceived subjective norms and future SSB reduction intentions. Analysis of the subjective norms index revealed that those participants who received the social norms information reported higher perceived subjective norms (i.e., that their friends and others who are important in their lives would want them to minimize their SSB consumption) than did those who only received the SSB risks information. The d of .67 indicates that those who had received the PNF had scores on the subjective norms index that were on average approximately two thirds of a standard deviation higher than the scores of those who did not receive the PNF. In contrast, the differences in perceived subjective norms as a function of affirmation condition were negligible (d = .01). Also, the pattern of perceived subjective norms across the information conditions varied only weakly as a function of self-affirmation condition ( < .01).
Table 1.
Experiment 1 descriptives for perceived subjective norms and intentions to reduce SSB consumption as a function of conditions.
| Measure | Risks Info Only
|
Norms Info Only
|
Risks + Norms Info
|
Total
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | Self-Aff | Total | Control | Self-Aff | Total | Control | Self-Aff | Total | Control | Self-Aff | Total | |
| Subjective Norms | ||||||||||||
| Sample size | 28 | 21 | 49 | 25 | 23 | 48 | 21 | 25 | 46 | 74 | 69 | 143 |
| Range | 7–20 | 4–18 | 4–20 | 8–20 | 8–20 | 8–20 | 8–20 | 8–20 | 8–20 | 7–20 | 4–20 | 4–20 |
| Mean | 11.25 | 10.81 | 11.06 | 13.84 | 14.26 | 14.04 | 12.90 | 13.08 | 13.00 | 12.59 | 12.78 | 12.69 |
| Median | 11.00 | 10.00 | 11.00 | 14.00 | 14.00 | 14.00 | 13.00 | 13.00 | 13.00 | 12.00 | 13.00 | 12.00 |
| SD | 3.36 | 3.94 | 3.59 | 3.57 | 2.83 | 3.21 | 3.53 | 3.76 | 3.62 | 3.61 | 3.76 | 3.67 |
| Intentions | ||||||||||||
| Sample size | 28 | 21 | 49 | 25 | 23 | 48 | 21 | 25 | 46 | 74 | 69 | 143 |
| Range | 14–45 | 15–44 | 14–45 | 13–44 | 13–45 | 13–45 | 13–43 | 13–44 | 13–44 | 13–45 | 13–45 | 13–45 |
| Mean | 30.04 | 34.81 | 32.08 | 32.52 | 30.83 | 31.71 | 32.19 | 34.24 | 33.30 | 31.49 | 33.28 | 32.35 |
| Median | 29.00 | 38.00 | 33.00 | 35.00 | 32.00 | 32.50 | 32.00 | 35.00 | 34.00 | 32.00 | 35.00 | 33.00 |
| SD | 8.11 | 8.73 | 8.63 | 9.07 | 8.50 | 8.75 | 7.68 | 7.89 | 7.77 | 8.30 | 8.42 | 8.38 |
Analyses of participants’ intentions to reduce future SSB consumption demonstrated only small differences as a function of information ( = .01), self-affirmation ( =.01), or their interaction ( = .03). However, among participants who had performed the self-affirmation task, those who had received the SSB risks information, relative to those who had not, expressed intentions to reduce their SSB consumption that averaged .42 standard deviation units higher (Ms = 34.81, 34.24 and 30.83, for SSB risks only, SSB risks + social norms, and social norms only conditions, respectively), which is considered a small to medium effect size.
Overall, the results of Experiment 1 demonstrated some promise of the efficacy of both the social norms information and the SSB risks information. The correction of misperceived norms seemed to convince participants that important people in their lives would want them to reduce their SSB consumption, which according to the TPB should be an important step in the process of reducing SSB consumption intentions and behavior (Azjen & Madden, 1986). However, the differences in intentions across information conditions were weaker than might be expected, given previous work in other domains (e.g., Balvig & Holmberg, 2011; Mattern & Neighbors, 2004; Neighbors et al., 2004; Reid & Aiken, 2013). Further, there was only weak evidence that self-affirmation may have resulted in greater receptiveness to the SSB risks information.
Experiment 2
Although weak or null effects can be informative (Trafimow, 2014), we conducted a second experiment to correct some of the methodological limitations that may have contributed to the weak effects obtained in Experiment 1. First, in Experiment 2 we sought to enhance the impact of the SSB risks information by adding a task designed to increase the salience of the sugar content of a typical SSB. Second, we included a no information (control) condition to help determine whether the minimal intention differences across information conditions in the first experiment were due to the equal efficacy, versus inefficacy, of the information conditions. Finally, Experiment 2 also included a behavioral measure as well as a surprise two-week follow-up to assess intervention effects on SSB consumption and behaviors that would indicate preparations to alter SSB consumption (e.g., reading beverage labels for sugar content).
We expected that receiving either or both SSB risks and social norms information would result in greater perceived subjective norms, greater SSB reduction intentions, greater SSB reduction preparation behaviors, and greater reductions in SSB consumption relative to participants who did not receive either type of information. We also expected the combination of SSB risks and social norms information to result in greater SSB reduction intentions and behaviors than either type of information alone. Separately, we also expected that participants who performed the self-affirmation process, relative to those who did not, would report greater SSB reduction intentions and behaviors.
Method
Participants
149 University of California San Diego (UCSD) undergraduates (75% female), aged 18 to 45 years (M = 21.00, SD = 2.99) received course credit for participation. Participants’ ethnic makeup consisted of 45.6% Asian, 18.8% Caucasian, 14.8% Latino/a, 12.1% Multiracial, 2% Pacific Islander, 1.3% African-American, and 5.4% Other. Class standing of the sample included 4.7 % First year students, 9.4% Sophomores, 38.9% Juniors, 41.6% Seniors, and 5.4% other.
Design and Conditions
Participants were randomly assigned to one of 8 conditions in a 4 (Information Condition: No information vs. SSB risks information only vs Social norms information only vs SSB risks information + Social norms information) × 2 (Self-affirmation Condition: Control task vs Self-affirmation task) design. The social norms intervention and the self-affirmation task were identical to Experiment 1. The SSB risks information was also presented using the same laminated card used in Experiment 1. However, in Experiment 2 we sought to strengthen the information by providing an impactful, salient demonstration of the proportion of a typical SSB that is comprised of sugar. Specifically, after reading the risks card, participants were presented with a tray containing sugar cubes and a 12-oz glass resembling a can of soda. They were then asked to place 11 sugar cubes (one at a time) into the glass.
Procedure
Participants were recruited via the Psychology Department Human Participant Pool and were run individually. During recruitment the study was identified only by a number to minimize self-selection and the development of preconceptions about the study.
Intervention session
As each participant arrived to the lab, s/he was escorted through a conference room area that was bedecked as though a graduation party had recently taken place (including “congratulations” signage, empty pizza boxes, paper plates, napkins, etc.). The experimenter apologized “for the mess” and then asked the participant to read and sign the consent form. Thereafter, the participant was escorted to a small adjacent room to complete the same demographic and baseline measures described in Experiment 1. Next, depending on the condition, participants completed the self-affirmation or control process, and then received the SSB risks information, and/or the social norms information (PNF sheet), or no information (control condition). Thereafter, all participants completed the same outcome measures and manipulation checks described in Experiment 1. Participants were then probed for suspicion (none was detected), partially debriefed, and thanked for their participation. Finally, a behavioral measure of intervention efficacy was obtained. Specifically, as each participant was exiting the lab, the experimenter off-handedly invited him/her to “take a drink if you want, we have a lot left over.” Several bottles of water, coke, diet coke, and iced tea were on a counter adjacent to the exit. Immediately after casually inviting the participant to take a drink, the experimenter left the room to avoid the possibility that participants would feel pressure to select a particular type of beverage (i.e., one that did not contain sugar).
Follow-up
Approximately two weeks later (M = 16.86, SD = 3.91, range = 13–29 days) experimenters, who were blind to condition, contacted 90.6% of the original participants by telephone (only 1 declined and 13 participants were not reached [after a minimum of 30 attempts]). Participants were not informed in advance that a follow-up would occur and provided oral informed consent at the time of telephone contact.
At follow-up, participants were asked to list all of the beverages they had consumed the previous day, including the number of servings of each. The interviewer then recorded this information on the beverage checklist (described in Experiment 1). To increase accuracy, participants were given pressure-free time to recall what they drank and were encouraged to think chronologically (e.g., “Take a moment to think about yesterday…”; “What was the first thing you had to drink after you woke up?”; etc.). Participants also responded to eight questions designed to assess the frequency with which they had engaged in various behaviors that might indicate contemplation of/preparation to alter SSB consumption (e.g., “During the past two weeks, how often did you read the labels on the drinks you were considering purchasing to see whether they contained added sugar?”; “During the past two weeks, how often did you browse the water section at a grocery store or vending machine?”). All items were rated on a 5-point scale (0=Not at all; 4=Very Frequently). The eight items displayed acceptable internal consistency (α = .74) and thus were combined into an overall index of preparatory behaviors. At the conclusion of the follow-up, participants were fully debriefed. All study procedures, for both experiments, were reviewed and approved by one of the university’s institutional review boards.
Results and Discussion
Preliminary Analyses
Group Equivalence
Consistent with Experiment 1, there were only small differences across conditions in age, gender, ethnicity, and year in college ( ranged from .00 to .03). Similarly, condition differences in reported SSB consumption at baseline were also small ( ranged from .00 to .04), suggesting effective randomization to condition.
Risks Information Manipulation Checks
Just as in Experiment 1, analyses of the manipulation checks demonstrated that participants processed the risks information when it was provided. Specifically, participants who received the risks information, relative to those who did not, were more likely to correctly report the link between SSB consumption and both weight gain and aging (both ds = .66, indicating medium to large effect sizes), and provided higher estimates of the sugar content in a typical soda (d = .38, indicating a small to medium effect size) and more correct estimates of the jogging minutes required to burn the calories in one soda (d = .93, indicating a large effect size).
Social Norms Manipulation Checks
Similarly, analyses of the social norms manipulation checks suggest that participants processed the information provided and that the information is not common knowledge. Specifically, participants’ estimates of the percentage of their peers who report that they try to avoid SSB consumption and the percentage of peers who try to limit themselves to 1–2 SSBs per day were on average at least three standard deviations higher if they were in one of the conditions that received PNF (Ms ranged from 88.32% to 90.79%) than if they were in either the SSB risks information-only or the no information conditions (Ms ranged from 31.18% to 40.86%), ds = 4.13 and 3.08, respectively. In addition, those participants who had received the social norms information perceived their peers’ beliefs about avoiding SSBs to be on average .81 standard deviation units more positive (M = 5.97, SD = .16 and M = 6.01, SD = .08 for social norms only and SSB risks + social norms, respectively) than did those who had not received such information (M = 5.42, SD = .86 and M = 5.57, SD = .88 for SSB risks only and no information participants, respectively). Finally, participants’ ratings of the importance that their peers place on avoiding SSBs were on average over one and a half standard deviations greater for those in either of the social norms conditions (M = 5.97, SD = .16 and M = 6.00, SD = .23 for social norms only and SSB risks + social norms, respectively) relative to those who had not received social norms information (M = 4.87, SD = .78 and M = 4.60, SD = 1.42 for SSB risks only and no information participants, respectively), d = 1.57.
State Self-esteem
As expected, participants who had performed the self-affirmation task subsequently reported higher state self-esteem (M = 73.35, SD = 11.96) than did participants who performed the control task (M = 69.33, SD = 12.84). A d of .33 indicates that the state self-esteem scores of those who performed the self-affirmation task were one third of a standard deviation higher than those in the control group.
Primary Analyses
To test the prediction that all information conditions would display greater future SSB reduction intentions, greater preparatory behaviors, and reduced SSB consumption relative to those in the no information condition, the three intervention conditions were combined and compared to the no information condition. Additional comparisons tested the hypothesis that the combination of SSB risks and social norms information would result in greater future SSB reduction intentions, greater preparatory behaviors, and reduced SSB consumption relative to either type of information alone. We also examined whether self-affirmation would enhance any effects of the information interventions. Analyses of SSB reduction intentions and of follow-up SSB consumption controlled for baseline SSB consumption. Descriptive information for each outcome as a function of condition can be found in Table 2.
Table 2.
Experiment 2 descriptives for outcome measures as a function of conditions.
| Measure | No Info
|
Risks Info Only
|
Norms Info Only
|
Risks + Norms Info
|
Total
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | Self-Aff | Total | Control | Self-Aff | Total | Control | Self-Aff | Total | Control | Self-Aff | Total | Control | Self-Aff | Total | |
| Subjective Norms | |||||||||||||||
| Sample size | 18 | 17 | 35 | 18 | 20 | 38 | 19 | 19 | 38 | 19 | 19 | 38 | 74 | 75 | 149 |
| Range | 8–17 | 8–16 | 8–17 | 8–19 | 8–20 | 8–20 | 8–19 | 8–20 | 8–20 | 8–20 | 4–20 | 4–20 | 8–20 | 4–20 | 4–20 |
| Mean | 11.72 | 11.12 | 11.43 | 12.83 | 13.10 | 12.97 | 12.58 | 13.47 | 13.03 | 14.74 | 13.37 | 14.05 | 12.99 | 12.81 | 12.90 |
| Median | 12.00 | 11.00 | 11.00 | 14.00 | 12.50 | 13.00 | 12.00 | 13.00 | 12.50 | 16.00 | 13.00 | 14.00 | 13.00 | 12.00 | 12.00 |
| SD | 2.85 | 2.00 | 2.45 | 3.09 | 3.87 | 3.48 | 3.32 | 3.10 | 3.20 | 3.98 | 4.55 | 4.27 | 3.46 | 3.60 | 3.52 |
| Intentions | |||||||||||||||
| Sample size | 18 | 17 | 35 | 18 | 20 | 38 | 19 | 19 | 38 | 19 | 19 | 38 | 74 | 75 | 149 |
| Range | 12–41 | 9–45 | 9–45 | 25–43 | 21–43 | 21–43 | 22–44 | 25–45 | 22–45 | 24–45 | 17–44 | 17–45 | 12–45 | 9–45 | 9–45 |
| Mean | 31.49 | 30.08 | 30.91 | 36.09 | 30.00 | 33.13 | 33.69 | 34.80 | 34.16 | 35.92 | 35.85 | 35.58 | 34.30 | 32.71 | 33.50 |
| Median | 31.50 | 32.00 | 32.00 | 38.00 | 29.50 | 34.50 | 33.00 | 35.00 | 33.50 | 36.00 | 36.00 | 36.00 | 35.00 | 33.00 | 34.00 |
| SD | 7.50 | 10.34 | 8.87 | 5.09 | 5.54 | 6.29 | 6.35 | 6.41 | 6.33 | 6.12 | 6.17 | 6.06 | 6.54 | 7.52 | 7.07 |
| %Took SSB | |||||||||||||||
| Sample size | 10 | 9 | 19 | 10 | 10 | 20 | 15 | 10 | 25 | 11 | 15 | 26 | 46 | 44 | 90 |
| Range | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 |
| Mean | .20 | .44 | .32 | .20 | .30 | .25 | .33 | .10 | .24 | .18 | .27 | .23 | .24 | .27 | .26 |
| Median | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 |
| SD | .42 | .53 | .48 | .42 | .48 | .44 | .49 | .32 | .44 | .41 | .46 | .43 | .43 | .45 | .44 |
| %Took Soda | |||||||||||||||
| Sample size | 10 | 9 | 19 | 10 | 10 | 20 | 15 | 10 | 25 | 11 | 15 | 26 | 46 | 44 | 90 |
| Range | 0–1 | 0–1 | 0–1 | 0–0 | 0–0 | 0–0 | 0–1 | 0–0 | 0–1 | 0–0 | 0–1 | 0–1 | 0–1 | 0–1 | 0–1 |
| Mean | .10 | .33 | .21 | .00 | .00 | .00 | .27 | .00 | .16 | .00 | .07 | .04 | .11 | .09 | .10 |
| Median | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 | .00 |
| SD | .32 | .50 | .42 | .00 | .00 | .00 | .46 | .00 | .37 | .00 | .26 | .20 | .31 | .29 | .30 |
| Preparatory Behaviors | |||||||||||||||
| Sample size | 15 | 16 | 31 | 15 | 19 | 34 | 18 | 17 | 35 | 18 | 17 | 35 | 66 | 69 | 135 |
| Range | 3–29 | 0–23 | 0–29 | 2–19 | 1–17 | 1–19 | 1–18 | 3–20 | 1–20 | 3–26 | 1–24 | 1–26 | 1–29 | 0–24 | 0–29 |
| Mean | 11.53 | 8.78 | 10.11 | 9.87 | 9.99 | 9.93 | 9.00 | 12.53 | 10.71 | 14.61 | 13.56 | 14.10 | 11.30 | 11.21 | 11.26 |
| Median | 11.00 | 6.75 | 7.50 | 10.00 | 10.00 | 10.00 | 9.50 | 13.00 | 12.00 | 14.50 | 13.00 | 14.00 | 10.50 | 12.00 | 11.00 |
| SD | 6.97 | 7.56 | 7.29 | 5.40 | 4.85 | 5.02 | 5.06 | 5.16 | 5.34 | 6.51 | 6.74 | 6.55 | 6.29 | 6.28 | 6.26 |
| Follow-up SSB Consumption | |||||||||||||||
| Sample size | 15 | 16 | 31 | 15 | 19 | 34 | 18 | 17 | 35 | 18 | 17 | 35 | 66 | 69 | 135 |
| Range | 0–5 | 0–6.5 | 0–6.5 | 0–2 | 0–3 | 0–3 | 0–5 | 0–4 | 0–5 | 0–3 | 0–3 | 0–3 | 0–5 | 0–6.5 | 0–6.5 |
| Mean | 1.34 | 0.94 | 1.10 | 0.92 | 1.13 | 0.99 | 1.21 | 0.90 | 1.09 | 1.42 | 1.30 | 1.43 | 1.26 | 1.05 | 1.15 |
| Median | 1.00 | 0.00 | 1.00 | 0.50 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| SD | 1.45 | 1.72 | 1.60 | 0.80 | 1.02 | 0.93 | 1.61 | 1.05 | 1.36 | 0.92 | 0.84 | .88 | 1.25 | 1.19 | 1.22 |
Note. The intentions and the follow-up SSB consumption condition means are adjusted for baseline SSB consumption.
Perceived Subjective Norms
Perceptions that friends and important others would want them to minimize their SSB consumption were on average nearly one half standard deviation higher for those participants who received the SSB risks information (M = 12.97, SD = 3.48), the social norms information (M = 13.03, SD = 3.20), or both (M = 14.05, SD = 4.27) than for those in the no information condition (M = 11.42, SD = 2.45), d = .48. However, differences in perceived subjective norms among the three intervention conditions were small (ds = .02 – .23). Also, there was very little difference in the subjective norms index scores of those who had performed the self-affirmation task and those who had not (d = .06), and the interaction between information and self-affirmation on perceived subjective norms was weak ( =.02).
Intentions
Analysis of participants’ intentions to reduce future SSB consumption demonstrated, perhaps not surprisingly, that people with higher SSB consumption at baseline reported lower future SSB reduction intentions, d = .39. Of more interest, the results also showed that those who received either the SSB risks, the social norms, or both types of information reported future SSB consumption reduction intentions that averaged nearly one half standard deviation higher (M = 33.05, SD = 6.29; M = 34.24, SD = 6.33; and M = 35.88, SD = 6.06 for SSB risks, norms, and both types of information, respectively) relative to those in the no information condition (M = 30.78, SD = 8.87), d = .46. Also, the addition of social norms information to the SSB risks information resulted in SSB reduction intentions that were on average nearly one third of a standard deviation greater than in the risks information alone, d = .30. Participants’ who had performed the self-affirmation task, versus those who had not, reported SSB reduction intentions that averaged approximately one quarter of a standard deviation higher. The d of .24 is considered a small effect size. Further, the interaction between information and self-affirmation was relatively weak ( = .04, see Table 2 for descriptives).
Beverage Sample
Recall that, as a behavioral measure of the impact of the intervention, participants were invited to select a free beverage while exiting the lab. For those participants who did choose to take a beverage (n = 90), there were only small differences in their likelihood of selecting a beverage with, versus one without, sugar as a function of either the type of information they had received (ds ranged from .01 to .17) or whether they had performed the self-affirmation task (d = .11). The interaction effect between the information and self-affirmation conditions was also small ( = .04).
However, given that the SSB risks information and sugar cube task focused heavily on sugar-sweetened sodas, we next examined participants’ likelihood of specifically choosing a sugar-sweetened soda. The results demonstrated that fewer of the participants in any of the information conditions, relative to the no information condition, selected a sugar-sweetened soda (0.0%, 16.0%, 3.9% of participants in the risks only, social norms only, and risks + social norms conditions, respectively vs. 21.1% of no information participants). The d of .46 indicates that participants who had received either or both types of information were on average nearly one half standard deviation less likely to choose a sugar sweetened soda than were those in the control condition (see Figure 1). In addition, as can be seen in Table 2, among those who had completed the self-affirmation task, participants in the no information condition were more likely to take a sugar-sweetened soda than were those who had received any of the information interventions, whereas among those who had not been self-affirmed, it was participants who received only social norms information who were most likely to select a sugar-sweetened soda ( = .09). This interaction pattern was not predicted and is not consistent with the results of the other measures.
Figure 1.
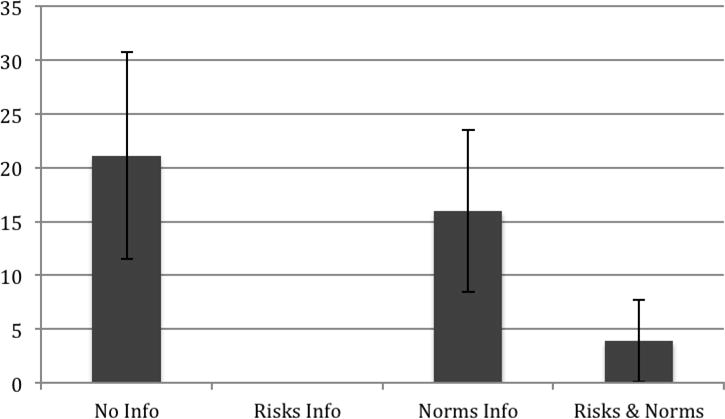
Percentage of participants who selected a sugar-sweetened soda, when offered a free beverage, as a function of information conditions. Note. Standard errors are represented by the error bars attached to each column.
Preparation to Alter SSB Consumption
There were differences in the measure of preparatory behaviors as a function of information condition.1 Specifically, the combination of the SSB risks and the social norms information resulted in greater behaviors that might be considered indicative of contemplation or preparation to alter SSB consumption (e.g., reading labels for sugar content, browsing the water section at the market; M = 14.10, SD = 6.55) than did either the SSB risks (M = 9.93, SD = 5.02) or the social norms (M = 10.71, SD = 5.34) information alone. The ds of .49 and .40, respectively, indicate that the means in each case were separated by slightly less than one half standard deviation. Participants in the combined SSB risks and social norms information condition also reported preparatory behaviors that averaged approximately one half standard deviation greater relative to participants who had not received either type of information (M = 10.11, SD = 7.29; d = .55; see Figure 2). Also, consistent with the other outcome measures, there was little evidence that preparatory behaviors differed as a function of self-affirmation condition (d = .01), and the interaction between information and self-affirmation was small ( = .04).
Figure 2.
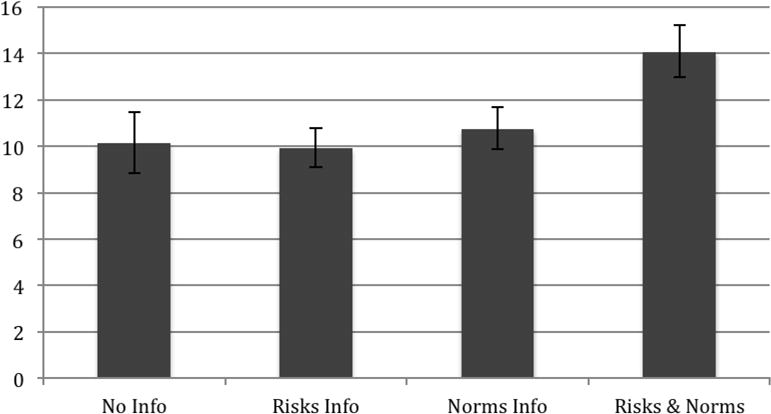
Mean score on preparatory behaviors index as a function of information condition. Note. Standard errors are represented by the error bars attached to each column.
SSB Consumption
Analysis of participants’ reports of their SSB consumption the day prior to the follow-up, which controlled for baseline reported SSB consumption, showed, as one would expect, that people with higher SSB consumption at baseline reported having continued higher consumption levels at follow-up (d = .54). However, there were only small reported consumption differences as a function of information condition (ds ranged from .00 to .20) and, separately, self-affirmation condition (d = .13). Also, the interaction effect between information and self-affirmation was weak ( = .01).
Mediation Analyses
We explored whether the information intervention effects on preparatory behaviors may have been mediated by perceived subjective norms and/or SSB reduction intentions. Given that there were only small effects of self-affirmation on SSB reduction preparatory behaviors, this variable was omitted from these analyses. The results of the mediation analyses demonstrated that perceived subjective norms was only weakly predictive of subsequent SSB reduction preparatory behaviors (d = .23), providing little evidence that it served as a mediator of the information intervention effects on this measure. However, greater SSB reduction intentions assessed shortly after the information intervention did predict on average .63 standard deviation units greater SSB reduction preparatory behaviors reported at the two-week follow-up. Further, when SSB reduction intentions was in the equation, and therefore statistically controlled, the effect of information condition was reduced ( = .07 and = .05 with, and without, intentions in the equation, respectively). This pattern suggests that the effect of the information intervention on subsequent preparatory behaviors may have been, at least in part, due to the extent to which it resulted in intentions to reduce SSB consumption.2
General Discussion
To our knowledge these are the first studies to experimentally examine the effects of either the correction of misperceived social norms or self-affirmation in the context of efforts to reduce SSB consumption. These also appear to be the first experiments to examine the efficacy of combining self-affirmation and the correction of misperceived norms in any context. Our pattern of findings was generally quite consistent across both experiments. There was little evidence that the self-affirmation process either alone or in combination with social norms information affected SSB consumption intentions or behaviors. Of course, null results should always be interpreted cautiously, however there are at least a couple of reasons to suggest that the minimal self-affirmation effects we obtained are unlikely to be the result of “not having done it right” (Trafimow, 2014). First, we utilized a self-affirmation task that has been used extensively previously (Harris et al., 2007; Napper et al., 2009). In addition, the weak effects occurred across two experiments conducted at different universities and across a variety of measures. Also, the higher state self-esteem scores produced by the self-affirmation task, particularly in Experiment 2, make it unlikely that the lack of differential effects on intentions and behaviors is a function of the failure to adequately manipulate self-affirmation. It should be mentioned that previous work suggests that the self-affirmation process may be primarily effective for increasing receptiveness to risks information among those individuals for whom the risky behavior is relevant/important (Sherman et al., 2000). However, we found little evidence that the high SSB users in our samples became more receptive to the SSB risks information after self-affirmation.3 Nevertheless, given that we examined this question posthoc, the possibility that high SSB consumers in particular might benefit from self-affirmation prior to receiving risks information should be more fully addressed in future work.
In contrast to the weak effects involving self-affirmation, the information intervention manipulation more consistently produced stronger effects on several measures of SSB consumption cognitions and behaviors. Specifically, in Experiment 1, participants who received social norms information either alone or in combination with SSB risks information became more convinced that the people in their lives who are important to them want them to reduce their SSB consumption. In Experiment 2, participants who received either or both types of information, reported higher perceived subjective norms, greater intentions to reduce their SSB consumption, and were less likely to select a sugar-sweetened soda when given the opportunity than those who did not receive either type of information. In addition, relative to all other conditions, those who had received both types of information displayed the strongest intentions to reduce their SSB consumption and at follow-up reported having engaged in greater behaviors that suggest contemplation of, or preparation to make, a behavior change. Further, there was some evidence that the effect of the information received on subsequent contemplation/preparation behaviors may, in part, have been mediated by its effect on participants’ intentions to reduce their SSB consumption.
Unfortunately, there was little evidence that either the SSB risks or the social norms information actually resulted in lower SSB consumption at follow-up relative to baseline. It is important to note that the beverage checklist we developed to assess SSB consumption behaviors asked participants to report all beverages (i.e., not just SSBs) that they had consumed on the most recent full day prior to participation (i.e., “yesterday”) at both baseline and follow-up. While such an approach likely resulted in both less social desirability response bias than a general rating of SSB consumption change and fewer memory failures than asking about several days’ worth of beverage consumption, consumption on any particular day may not be representative of overall SSB consumption. For example, for some participants the day prior to participation was a weekend day, holiday, or day on which they were studying for an exam, and people often consume different types of beverages on such days than during the week or when not studying intensively. Thus, it is possible that the lack of effects on reported beverage consumption is due to weaknesses in the measure. Future work could examine methods of obtaining more accurate and reliable information about beverage consumption. Of course, it is also possible that while the interventions were impactful enough to produce changes in intentions and preparation to change they were simply not impactful enough to produce actual behavior change. Both the SSB risks and the correction of misperceived social norms information interventions were very brief (~ 2 – 3 minutes each), one time, mostly textual (although the risk information did include some images) interventions. In fact, one could argue it is actually remarkable that such brief interventions altered even intentions and preparatory behaviors. Future work should examine methods of enhancing the efficacy and impact of the interventions (e.g., booster interventions might include sending participants statements and/or images taken from the interventions as reminders via text message or e-mail several times following participation).
Methodological/Interpretive Issues
This research had several methodological strengths. In addition to the obvious methodological advantages produced by randomization to condition and the statistical control of baseline behavior in both experiments, Experiment 2 went beyond the assessment of only immediate cognitions and intentions by including a behavioral measure and by assessing SSB consumption behaviors at a two-week follow-up. Also, participants were not aware of the follow-up in advance, thus reducing the possibility that they altered their behavior in anticipation.
The research of course also had methodological limitations. First, the fact that both samples were largely female, generally between the ages of 18 and 24, and consisted exclusively of college students raises the question of generalizability. We would note however, that the two experiments were conducted at two different universities and the ethnic background and year in college of the two samples varied considerably. We would also suggest that the college population is an important one to target with SSB reduction interventions for several reasons. First, college students are heavy SSB consumers (Huffman & West, 2007; West et al., 2006), often intentionally infusing sugar and caffeine to cope with long hours of studying. Also, college is a time when many are experiencing day-to-day independence in decision-making for the first time in their lives, and many lifelong health habits are forming (Downes, 2015; Hubert, Eaker, Garrison, & Castelli, 1987). This is also likely a particularly appropriate age and venue for social norms-based interventions because what peers are doing and approve of doing is likely more important to young adults than older adults and more salient to college students, who are constantly in the company of their peers, than to others of the same age who are not attending college. Nevertheless, it would be desirable for future work to examine the efficacy of these interventions in other populations.
Another limitation of this study is the utilization of primarily self-reported outcome measures, which creates concerns about response bias. We made efforts to decrease response bias by strongly emphasizing to participants our interest in accuracy over perceived social desirability, by developing a relatively objective checklist for reporting all beverages consumed, and by having participants complete the checklist with reference to the previous day (to decrease memory failures). We also included a behavioral measure in Experiment 2 by offering participants their choice of free beverage as they exited the lab. Further, we decreased the possibility that participants would feel pressure to select a beverage without sugar by having the experimenter leave the room immediately upon issuing the invitation and by having the beverages haphazardly strewn about (some bottles standing upright, others laying on their side) on a counter near the lab exit in an effort to create the impression that the researchers would be completely unaware of their beverage selection.4
A final concern is that there was only one, short-term follow-up in Experiment 2. Thus, it is not possible to determine whether the effects we observed on preparation for behavior change would eventually progress to actual behavior change or whether additional intervention would be necessary to produce lasting changes in SSB consumption. Multiple follow-ups over longer periods of time would be desirable.
Conclusions
Given the dramatic increases in SSB consumption over the past 30 years (Brownell et al, 2009) and the mounting evidence of the significant health risks posed by SSBs (Anand et al., 2015; Crichton et al., 2016; Harrington, 2008; Imamura et al., 2016; Malik et al., 2006; Ye et al., 2011), interventions that are effective for motivating reduced SSB consumption have the potential for significant impacts on public health and health care costs. SSB consumption is a habitual behavior, likely driven by multiple factors, and it is unlikely that major changes in consumption and health will be realized until a variety of effective interventions have been developed. The experiments reported here represent a preliminary effort to develop an efficacious intervention to motivate SSB reduction. Although the specific findings of these experiments are in need of replication, together with previous work in a variety of other health contexts (Balvig & Holmberg, 2011; Hansen & Graham, 1991; Mahler et al., 2008; Mattern & Neighbors, 2004; Neighbors et al., 2004; Reid & Aiken, 2013), the results of this experiment suggest that correcting misperceived descriptive and injunctive norms regarding SSB consumption holds promise as a risk reduction technique. Particularly when paired with SSB risk information, the social norms information was effective for altering cognitions (i.e., subjective norms and intentions) and behaviors (i.e., reading labels and searching grocery isles for alternative beverages) that are considered important forerunners of behavior change according to the Theory of Planned Behavior (Ajzen & Fishbein, 1980; Ajzen & Madden, 1986) and the Transtheoretical Model of Behavior Change (Prochaska & DiClemente, 1986), respectively. Further, both interventions are brief and easily implemented, increasing their potential utility. It will be important for future work to determine whether the impact of the interventions can be enhanced to produce sustained SSB consumption reductions without decreasing their practical utility. It will also be important for future work to more fully delineate the psychological processes through which the correction of misperceived norms produces behavior changes.
Acknowledgments
The authors thank Lisa Liang and Spencer Michalek, for their help in carrying out this project.
Funding
This research was supported by MARC GM-08807 and RISE GM-64783 grants received from the Office for Training, Research and Education in the Sciences (OTRES).
Footnotes
The number of days between the intervention and the follow-up did not differ as a function of condition ( ranged between .00–.03), and controlling for number of days since the intervention did not alter the pattern of findings reported below for either the preparatory behaviors or SSB consumption measures.
Of course it must be acknowledged that the assumption that mediation analysis actually provides evidence of mechanisms of change has been questioned for a number of reasons, including (but not limited to) the failure of most such analyses to meet the assumption that the predictor variable has been assessed without error (Kline, 2015), the possibility that the mediator and outcome measure are both caused by an unmeasured variable (Kline, 2015), and the tendency to use suboptimal cross-sectional designs that do not clearly establish the temporal order of the variables (Kline, 2015; Tate, 2015). In this particular experiment, we utilized a “measurement of mediation model” which is the minimal design needed to justify conducting a mediation analysis (Kline, 2015). That is, given that our predictor is an experimental variable (i.e., we manipulated the information that Ps received), the proposed mediator was measured after Ps were exposed to the experimental manipulation, and the outcome (preparatory behaviors) was assessed two weeks later, temporal precedence among the predictor, the proposed mediator, and the outcome is established; thus rendering implausible the alternative interpretation that changes in preparatory behaviors actually produced changes in SSB reduction intentions. However, it is nevertheless necessary to interpret the results of our mediation analyses with caution given, among other things, that we did not manipulate the proposed mediator (e.g., SSB reduction intentions) nor can we be certain that SSB reduction intentions and preparatory behaviors do not share an unmeasured cause (i.e., are related because both are caused by a third variable).
To examine this issue we divided our sample in each experiment at the median into low and high SSB users based on their baseline beverage checklist scores. We then conducted analyses that compared high and low SSB users as a function of both information and self-affirmation on all outcome measures in both experiments. We also conducted analyses examining the information and self-affirmation condition effects on the outcome measures for only the high SSB users. In all of these analyses we found only weak effects of self-affirmation alone ( ranged from .00 to .02) or in interaction with information condition ( ranged from .00 to .06). Further, the weak interaction patterns that did exist were inconsistent across outcome measures (i.e., did not consistently show greater receptiveness to risk information in the self-affirmation condition). Of course, these results must be interpreted cautiously given that this experiment was not designed to address this question (i.e., we did not specifically recruit large numbers of high SSB users and then randomly assign them to condition) and the means in some conditions are based on as few as 3 participants.
We believe the fact that several participants actually took more than the one beverage they were invited to take attests to the fact that participants generally were not aware that we would be able to determine what type of beverage they selected.
Contributor Information
Carlos E. Rosas, California State University San Marcos
Petrona Gregorio-Pascual, California State University San Marcos.
Redd Driver, California State University San Marcos.
Alyssa Martinez, California State University San Marcos.
Stephanie L. Price, California State University San Marcos
Cristal Lopez, California State University San Marcos.
Heike I. M. Mahler, California State University San Marcos University of California, San Diego.
References
- Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall; 1980. [Google Scholar]
- Ajzen I, Madden TJ. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology. 1986;22:453–474. doi: 10.1016/0022-1031(86)90045-4. [DOI] [Google Scholar]
- Anand SS, Hawkes C, De Souza RJ, Mente A, Dehghan M, Nugent R, Popkin BM. Food consumption and its impact on cardiovascular disease: importance of solutions focused on the globalized food system: a report from the workshop convened by the World Heart Federation. Journal of the American College of Cardiology. 2015;66(14):1590–1614. doi: 10.1016/j.jacc.2015.07.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armitage CJ, Harris PR, Arden MA. Evidence that self-affirmation reduces alcohol consumption: Randomized exploratory trial with a new, brief means of self-affirming. Health Psychology. 2011;30(5):633–641. doi: 10.1037/a0023738. [DOI] [PubMed] [Google Scholar]
- Balvig F, Holmberg L. The ripple effect: A randomized trial of a social norms intervention in a Danish middle school setting. Journal of Scandinavian Studies in Criminology and Crime Prevention. 2011;12(1):3–19. doi: 10.1080/14043858.2011.561619. [DOI] [Google Scholar]
- Bergen D, Yeh MC. Effects of energy-content labels and motivational posters on sales of sugar-sweetened beverages: stimulating sales of diet drinks among adults study. Journal of the American Dietetic Association. 2006;106(11):1866–1869. doi: 10.1016/j.jada.2006.08.002. [DOI] [PubMed] [Google Scholar]
- Block JP, Gillman MW, Linakis SK, Goldman RE. “If it tastes good, I’m drinking it”: Qualitative study of beverage consumption among college students. Journal of Adolescent Health. 2013;52(6):702–706. doi: 10.1016/j.jadohealth.2012.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brownell KD, Farley T, Willett WC, Popkin BM, Chaloupka FJ, Thompson JW, Ludwig DS. The public health and economic benefits of taxing sugar-sweetened beverages. New England Journal of Medicine. 2009;361(16):1599–1605. doi: 10.1056/NEJMhpr0905723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cialdini RB, Reno RR, Kallgren CA. A focus theory of normative conduct: recycling the concept of norms to reduce littering in public places. Journal of Personality and Social Psychology. 1990;58(6):1015. doi: 10.1037/0022-3514.58.6.1015. [DOI] [Google Scholar]
- Crichton GE, Elias MF, Torres RV. Sugar-sweetened soft drinks are associated with poorer cognitive function in individuals with type 2 diabetes: The Maine–Syracuse Longitudinal Study. British Journal of Nutrition. 2016;115(08):1397–1405. doi: 10.1017/S0007114516000325. [DOI] [PubMed] [Google Scholar]
- Downes L. Physical activity and dietary habits of college students. The Journal for Nurse Practitioners. 2015;11(2):192–198. doi: 10.1016/j.nurpra.2014.11.015. [DOI] [Google Scholar]
- Ebbeling CB, Feldman HA, Chomitz VR, Antonelli TA, Gortmaker SL, Osganian SK, Ludwig DS. A randomized trial of sugar-sweetened beverages and adolescent body weight. New England Journal of Medicine. 2012;367(15):1407–1416. doi: 10.1056/NEJMoa1203388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Predicting and changing behavior: The reasoned action approach. New York: Psychology Press; 2010. [Google Scholar]
- Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. Journal of the American Medical Association. 2016;315(21):2284–2291. doi: 10.1001/jama.2016.6458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher JM, Frisvold D, Tefft N. Taxing soft drinks and restricting access to vending machines to curb child obesity. Health Affairs. 2010;29(5):1059–1066. doi: 10.1377/hlthaff.2009.0725. [DOI] [PubMed] [Google Scholar]
- Ha EJ, Caine-Bish N, Holloman C, Lowry-Gordon K. Evaluation of effectiveness of class-based nutrition intervention on changes in soft drink and milk consumption among young adults. Nutrition Journal. 2009;8(1):50. doi: 10.1186/1475-2891-8-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han E, Powell LM. Consumption patterns of sugar-sweetened beverages in the United States. Journal of the Academy of Nutrition and Dietetics. 2013;113(1):43–53. doi: 10.1016/j.jand.2012.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansen WB, Graham JW. Preventing alcohol, marijuana, and cigarette use among adolescents: Peer pressure resistance training versus establishing conservative norms. Preventive Medicine. 1991;20:414–430. doi: 10.1016/0091-7435(91)90039-7. [DOI] [PubMed] [Google Scholar]
- Harrington S. The role of sugar-sweetened beverage consumption in adolescent obesity: A review of the literature. The Journal of School Nursing. 2008;24(1):3–12. doi: 10.1622/1059-8405(2008)024[0003:TROSBC]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Harris PR, Mayle K, Mabbott L, Napper L. Self-affirmation reduces smokers’ defensiveness to graphic on-pack cigarette warning labels. Health Psychology. 2007;26(4):437–446. doi: 10.1037/0278-6133.26.4.43. [DOI] [PubMed] [Google Scholar]
- Harris PR, Napper L. Self-affirmation and the biased processing of threatening health-risk information. Personality and Social Psychology Bulletin. 2005;31(9):1250–1263. doi: 10.1177/0146167205274694. [DOI] [PubMed] [Google Scholar]
- Heatherton TF, Polivy J. Development and validation of a scale for measuring state self-esteem. Journal of Personality and Social Psychology. 1991;60:895–910. doi: 10.1037/0022-3514.60.6.895. [DOI] [Google Scholar]
- Hubert HB, Eaker ED, Garrison RJ, Castelli WP. Life-style correlates of risk factor change in young adults: An eight-year study of coronary heart disease risk factors in the Framingham offspring. American Journal of Epidemiology. 1987;125(5):812–831. doi: 10.1093/oxfordjournals.aje.a114598. [DOI] [PubMed] [Google Scholar]
- Huffman L, West DS. Readiness to change sugar sweetened beverage intake among college students. Eating Behaviors. 2007;8(1):10–14. doi: 10.1016/j.eatbeh.2006.04.005. [DOI] [PubMed] [Google Scholar]
- Huth PJ, Fulgoni VL, Keast DR, Park K, Auestad N. Major food sources of calories, added sugars, and saturated fat and their contribution to essential nutrient intakes in the US diet: Data from the national health and nutrition examination survey (2003–2006) Nutrition Journal. 2013;12(1):1. doi: 10.1186/1475-2891-12-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Imamura F, O’Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, Forouhi NG. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. British Journal of Sports Medicine. 2016;50(8):496–504. doi: 10.1136/bmj.h3576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kit BK, Fakhouri TH, Park S, Nielsen SJ, Ogden CL. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999-2010. American Journal of Clinical Nutrition. 2013;98(1):180–188. doi: 10.3945/ajcn.112.057943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB. The mediation myth. Basic and Applied Social Psychology. 2015;37:202–213. [Google Scholar]
- Lally P, Bartle N, Wardle J. Social norms and diet in adolescents. Appetite. 2011;57(3):623–627. doi: 10.1016/j.appet.2011.07.015. [DOI] [PubMed] [Google Scholar]
- Mahler HIM, Kulik JA, Butler HA, Gerrard M, Gibbons FX. Social norms information enhances the efficacy of an appearance-based sun protection intervention. Social Science & Medicine. 2008;67(2):321–329. doi: 10.1016/j.socscimed.2008.03.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahler HIM, Kulik JA, Gibbons FX, Gerrard M, Harrell J. Effects of appearance-based intervention on sun protection intentions and self-reported behaviors. Health Psychology. 2003;22(2):199–209. doi: 10.1037/0278-6133.22.2.199. [DOI] [PubMed] [Google Scholar]
- Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: A systematic review. The American Journal of Clinical Nutrition. 2006;84(2):274–288. doi: 10.1093/ajcn/84.1.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattern JL, Neighbors C. Social norms campaigns: Examining the relationship between changes in perceived norms and changes in drinking levels. Journal of Studies in Alcohol. 2004;65:489–493. doi: 10.15288/jsa.2004.65.489. [DOI] [PubMed] [Google Scholar]
- Miller DT, McFarland C. When social comparison goes awry: The case of pluralistic ignorance. In: Suls J, Wills T, editors. Social comparison: Contemporary theory and research. Hillsdale, NJ: Lawrence Erlbaum; 1991. pp. 287–313. [Google Scholar]
- Napper L, Harris PR, Epton T. Developing and testing a self-affirmation manipulation. Self and Identity. 2009;8:45–62. doi: 10.1080/15298860802079786. [DOI] [Google Scholar]
- Neighbors C, Larimer ME, Lewis MA. Targeting misperceptions of descriptive drinking norms: Efficacy of a computer-delivered personalized normative feedback intervention. Journal of Consulting and Clinical Psychology. 2004;72(3):434–447. doi: 10.1037/0022-006X.72.3.434. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, Flegal KM. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. Journal of the American Medical Association. 2016;315(21):2292–2299. doi: 10.1001/jama.2016.6361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins HW, Berkowitz AD. Perceiving the community norms of alcohol use among students: Some research implications for campus alcohol education programming. International Journal of the Addictions. 1986;21:961–976. doi: 10.3109/10826088609077249. [DOI] [PubMed] [Google Scholar]
- Perkins JM, Perkins HW, Craig DW. Misperceptions of peer norms as a risk factor for sugar-sweetened beverage consumption among secondary school students. Journal of the American Dietetic Association. 2010;110(12):1916–1921. doi: 10.1016/j.jada.2010.09.008. [DOI] [PubMed] [Google Scholar]
- Popkin BM, Nielsen SJ. The sweetening of the world’s diet. Obesity Research. 2003;11(11):1325–1332. doi: 10.1038/oby.2003.179. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC. Toward a comprehensive model of change. In: Miller WR, Heather N, editors. Treating addictive behavior. Orlando, Fl: Plenum Press; 1986. [Google Scholar]
- Reed MB, Aspinwall LG. Self-affirmation reduces biased processing of health-risk information. Motivation and Emotion. 1998;22(2):99–132. doi: 10.1023/A:1021463221281. [DOI] [Google Scholar]
- Reid AE, Aiken LS. Correcting injunctive norm misperceptions motivates behavior change: A randomized controlled sun protection intervention. Health Psychology. 2013;32:551–560. doi: 10.1037/a0028140. [DOI] [PubMed] [Google Scholar]
- Ritenbaugh C, Teufel-Shone NI, Aickin MG, Joe JR, Poirier S, Dillingham DC, Cockerham D. A lifestyle intervention improves plasma insulin levels among Native American high school youth. Preventive Medicine. 2003;36(3):309–319. doi: 10.1016/S0091-7435(02)00015-4. [DOI] [PubMed] [Google Scholar]
- Robinson E, Thomas J, Aveyard P, Higgs S. What everyone else is eating: A systematic review and meta-analysis of the effect of informational eating norms on eating behavior. Journal of the Academy of Nutrition and Dietetics. 2014;114(3):414–429. doi: 10.1016/j.jand.2013.11.009. [DOI] [PubMed] [Google Scholar]
- Schroeder CM, Prentice DA. Exploring pluralistic ignorance to reduce alcohol use among college students. Journal of Applied Social Psychology. 1998;28:2150–2180. doi: 10.1111/j.1559-1816.1998.tb01365.x. [DOI] [Google Scholar]
- Sherman DK, Cohen GL. The psychology of self-defense: Self-affirmation theory. In: Zanna MP, Zanna MP, editors. Advances in experimental social psychology. Vol. 38. San Diego, CA, US: Elsevier Academic Press; 2006. pp. 183–242. [DOI] [Google Scholar]
- Sherman DK, Nelson LD, Steele CM. Do messages about health risks threaten the self? Increasing the acceptance of threatening health messages via self-affirmation. Personality and Social Psychology Bulletin. 2000;26(9):1046–1058. doi: 10.1177/01461672002611003. [DOI] [Google Scholar]
- Sichieri R, Paula Trotte A, de Souza RA, Veiga GV. School randomised trial on prevention of excessive weight gain by discouraging students from drinking sodas. Public Health Nutrition. 2009;12(02):197. doi: 10.1017/S1368980008002644. [DOI] [PubMed] [Google Scholar]
- Steele CM. The psychology of self-affirmation: Sustaining the integrity of the self. In: Berkowitz L, editor. Advances in experimental social psychology. Vol. 21. New York: Academic Press; 1988. pp. 261–302. [Google Scholar]
- Taber DR, Chriqui JF, Powell LM, Chaloupka FJ. Banning all sugar-sweetened beverages in middle schools: Reduction of in-school access and purchasing but not overall consumption. Archives of Pediatrics & Adolescent Medicine. 2012;166(3):256. doi: 10.1001/archpediatrics.2011.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tate CU. On the overuse and misuse of mediation analysis: It may be a matter of timing. Basic and Applied Social Psychology. 2015;37:235–246. doi: 10.1080/01973.533.2015.1062380. [DOI] [Google Scholar]
- Trafimow D. Editorial. Basic and Applied Social Psychology. 2014;36:1–2. doi: 10.1080/01973533.2014.865505. [DOI] [Google Scholar]
- West DS, Bursac Z, Quimby D, Prewitt TE, Spatz T, Nash C, Eddings K. Self-reported sugar-sweetened beverage intake among college students. Obesity. 2006;14(10):1825–1831. doi: 10.1038/oby.2006.210. [DOI] [PubMed] [Google Scholar]
- Yang CC, Chiou WB. Substitution of healthy for unhealthy beverages among college students. A health-concerns and behavioral-economics perspective. Appetite. 2010;54(3):512–516. doi: 10.1016/j.appet.2010.02.004. [DOI] [PubMed] [Google Scholar]
- Ye X, Gao X, Scott T, et al. Habitual sugar intake and cognitive function among middle-aged and older Puerto Ricans without diabetes. British Journal of Nutrition. 2011;106:1423–1432. doi: 10.1017/S0007114511001760. [DOI] [PMC free article] [PubMed] [Google Scholar]