

Abstract
Massive rotator cuff tears are particularly challenging to treat and severely limit the function of the shoulder. Compared with a small rotator cuff tear, massive tears are more unpredictable and usually present with low tendon quality. When performing an anatomical repair of the rotator cuff, the surgical treatment is often associated with failure of the construct. An alternative procedure that can be performed in the setting of a massive tear is superior capsular reconstruction (SCR), using an autograft or allograft. This procedure has been shown to be effective and is associated with positive treatment outcomes. Moreover, the combination of an SCR with an anatomic repair of the rotator cuff tendon may provide a stronger fixation for the rotator cuff and ultimately lead to a lower likelihood of retear and failure. The purpose of this Technical Note is to describe our preferred procedure for the treatment of a massive rotator cuff tear through SCR with superimposition of the repair of the native rotator cuff tendons.
Chronic, massive rotator cuff tears involving the posterorsuperior rotator cuff remain particularly difficult to treat, often termed “irreparable.” Possible treatment options for this challenging pathology range from debridement and partial rotator cuff repair1 to more aggressive treatment including patch-augmented rotator cuff repair,2 bridging via graft for rotator cuff reconstruction,3 and, in cases of an irreparable subscapularis tendon or joint space narrowing with arthropathy, reverse total shoulder arthroplasty.4 However, aside from addressing the gap, treatment of this pathology should also aim to restore glenohumeral kinematics. Mihata et al.5 noted that chronic, massive, irreparable rotator cuff tears are often seen in combination with superior capsule defects. Therefore, superior capsular reconstruction (SCR) was proposed for treatment of this pathology.
As one of the primary static stabilizers of the glenohumeral joint, the shoulder capsule helps maintain overall glenohumeral stability.6 In particular, previous biomechanical studies have demonstrated that glenohumeral translation increases in all directions if there is a superior capsular defect, especially superiorly at 5° and 30° of abduction (ABD).5 Reconstruction of the superior capsule through use of a patch graft has been proven effective in a biomechanical cadaveric model, which demonstrated complete restoration of superior translation. However, patch grafting solely of the supraspinatus tendon only partially restored superior translation.5
Outside of the laboratory setting, SCR has also shown clinical promise. Mihata et al. reported on clinical and radiographic outcomes of 23 patients following arthroscopic SCR using a tensor fascia lata autograft. Following an average follow-up of 34.1 months, mean active elevation and external rotation (ER) increased from 84° and 26° to 148° and 40°, respectively.7 Aside from range of motion, American Shoulder and Elbow Surgeons scores also improved dramatically from 23.5 to 92.9 points. No cases of progression of osteoarthritis or rotator cuff muscle atrophy were seen in these patients. Of these 23 patients, 20 (83.3%) showed no tendon retear at follow-up on magnetic resonance imaging.7
Given the positive biomechanical and early clinical results associated with this procedure, SCR is increasingly being performed in cases of chronic, massive, irreparable rotator cuff tears.5, 7 Although previous reports have described incorporation of a posterior rotator cuff repair to the superior graft, none have reported on incorporation of a superior rotator cuff repair. The purpose of this Technical Note is to describe our preferred procedure for the treatment of a massive rotator cuff tear through SCR with superimposition of the repair of the native rotator cuff tendons.
Surgical Technique
Patient Positioning
The patient is placed in a beach chair position. Prior to general anesthesia, a regional block under ultrasound guidance is performed. General anesthesia is induced, and then the patient is prepared and draped in the usual sterile orthopaedic fashion.
Surgical Technique and Approach
The bony landmarks of the acromion and the coracoid are marked with a sterile marking pen (Video 1). A posterior viewing portal is established, and a diagnostic arthroscopy is performed. Under arthroscopic visualization, a midglenoid 5-mm cannula is placed. The defect due to the rotator cuff tear can be visualized (Fig 1). The scope is then moved to the subacromial space. The synovitis in the subacromial space is debrided. Careful debridement is performed anteriorly, superiorly, and posteriorly around the capsule and rotator cuff to do a superior capsular release. It is important to avoid the suprascapular nerve in this region. To perform this release, a combination of a blunt elevator, shaver (Smith and Nephew, Andover, MA), and radiofrequency (Arthrex, Naples, FL) is used. If the patient has reduced internal rotation (IR), an inferior capsular release can be performed at the junction between the capsule and the labrum. A combination of a basket shaver (Arthrex) and radiofrequency wand (Arthrex) can be used for this release.
Fig 1.
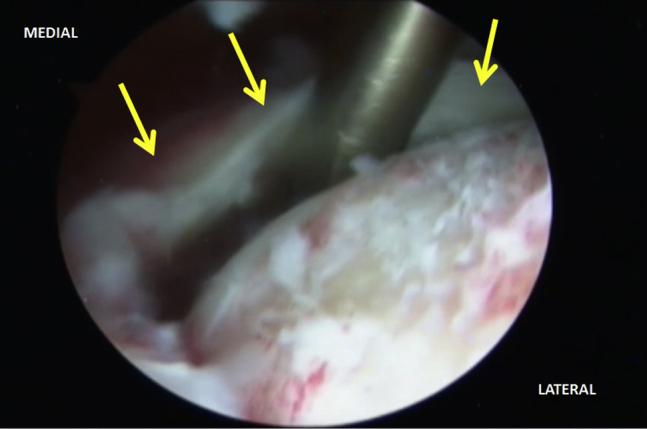
With arthroscopic visualization of this right shoulder joint using a 30° arthroscope through the posterior portal, the rotator cuff tendon (yellow arrows) can be visualized medially to its anatomical insertion on the greater tuberosity. Following the release of the rotator cuff from all adhesions, the mobility of the tendon is evaluated.
SCR
The rotator cuff was freed up anteriorly, superiorly, posteriorly, and underneath the capsule interface. In cases of massive rotator cuff tears with retraction, addition of an SCR can be an advantage. Prior to anchor insertion, the position of the anchors to be placed is prepared with an arthroscopic burr (Smith and Nephew) to get a bleeding surface. A 3.0-mm SutureTak anchor (Arthrex) is placed at the 10 o'clock position using the Neviaser portal (Arthrex), and a similar anchor is placed at the 2 o'clock position in a similar fashion (Fig 2). A dermal patch (Arthrex) for the SCR is then prepared and sized to 25 mm anterior to posterior and 34 mm medial to the lateral patch (Fig 3). The sutures are then brought out laterally with one suture from each anchor passed through the patch. Following this, a central knot from both sutures is tied. Then a tension slide technique is used to bring the graft to the superior glenoid (Fig 4).
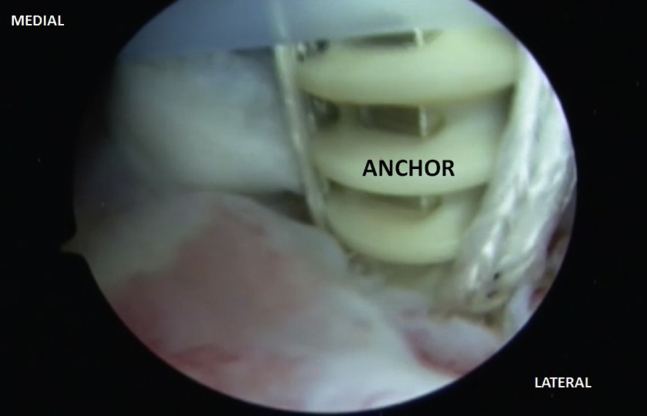
Fig 2.
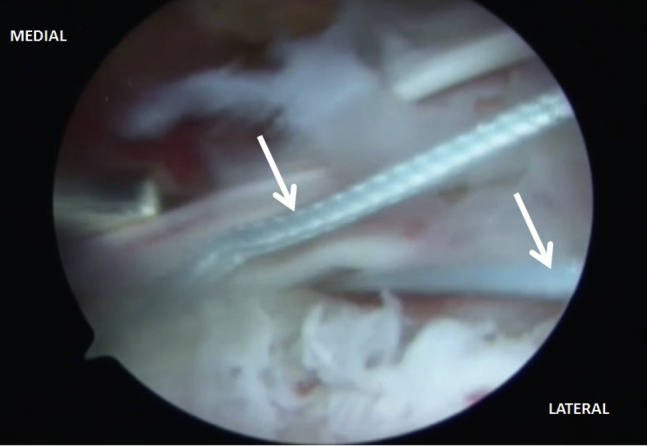
With arthroscopic visualization of this right shoulder through the posterior portal, the superior aspect of the glenoid is prepared using a combination of a radiofrequency wand and high-speed osseous burr. Following this, 2 3.0-mm SutureTak anchors (white arrows) are used, one placed at the 10 o'clock and the other at the 2 o'clock position using the Neviaser portal. Following this, the sutures are retrieved.
Fig 3.
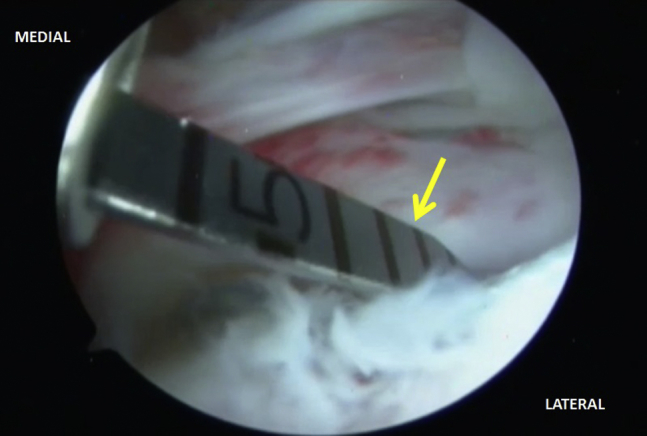
Once the 2 anchors are inserted on the superior aspect of the glenoid and the correct position is confirmed using a 30° arthroscope through the posterior portal, a sizing device (yellow arrow) is used to measure the correct size for the graft to be inserted in the right shoulder through use of anterior to posterior and medial to lateral measurements.
Fig 4.
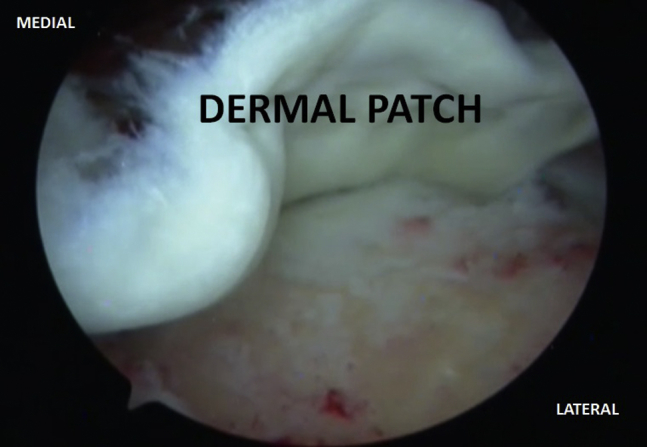
Using the sutures previously retrieved from the right shoulder while visualizing the joint through use of the arthroscope in the posterior portal, the dermal patch that was previously prepared in the back table using the intra-articular measurements is brought to the superior aspect of the glenoid in this right shoulder using a tension slide technique.
In preparation of additional anchors to be inserted, the superior glenoid is then prepared with an arthroscopic burr (Smith and Nephew) to get a bleeding surface. The capsule is repaired to the most medial aspect of the joint using 2 4.75-mm SwiveLock anchors (Arthrex) and FiberTape suture (Arthrex). To place the SwiveLock anchor (Arthrex), a 4.0-mm drill (Arthrex) is used to make a tunnel where the anchors will be placed. If the bone quality is good, it may be necessary to use a tap before inserting the Swivelock (Arthrex). The FiberTape suture (Arthrex) is passed through the dermal patch and then through the SwiveLock, and a horizontal stitch is tied.
Rotator Cuff Repair
The greater tuberosity is then prepared anteriorly, middle, and posteriorly, using a burr and a radiofrequency burr (Fig 5). The rotator cuff is mobilized and pulled laterally. To ensure a complete mobilization of the rotator cuff, anterior and posterior releases of all the tendons must be performed. The FiberTape sutures are placed through the medial row and the capsule. Using a SwiveLock drill, 2 tunnels for the 4.75 mm SwiveLock are prepared. The FiberTape sutures already placed in the medial row are then passed through the SwiveLock, and moderate tension is applied to reduce the supra- and infraspinatus to the footprint on the greater tuberosity. Using horizontal sutures, the repair is completed with a double-row technique (Fig 6).
Fig 5.
With arthroscopic visualization of the shoulder through the use of a 30° arthroscope inserted in the posterior portal, the graft is secured at the superior aspect of the glenoid in the right shoulder. The greater tuberosity is prepared using a combination of a high-speed burr and radiofrequency wand. Following this, 2 4.75-mm SwiveLock anchors are placed on the prepared surface.
Fig 6.
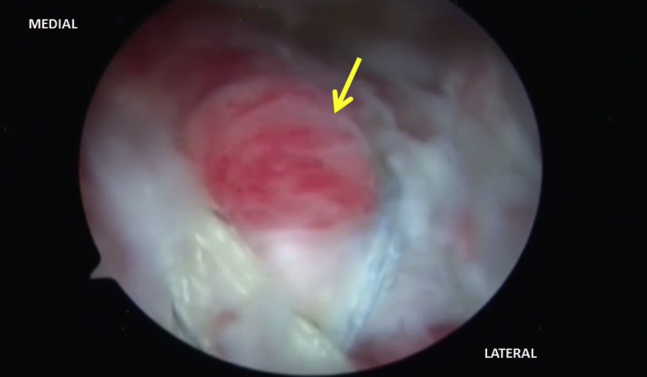
Arthroscopic visualization of the graft used to perform the superior capsule reconstruction and the subsequent superimposition of the rotator cuff atop the graft (yellow arrow) in the right shoulder are shown through a 30° arthroscope inserted in the posterior portal. Ultimately, this reconstruction helps restore the correct position of the humeral head and decrease the acromiohumeral distance.
All instruments are withdrawn from the shoulder. The wounds are closed with 3-0 Monocryl followed by Dermabond, Steri-Strips, plains, ABD, and Medipore dressing. The patient is placed in a padded ABD sling. The advantages and disadvantages associated with the described technique are listed in Tables 1, and pearls and pitfalls are shown in Tables 2.
Table 1.
Advantages and Disadvantages of Superior Capsular Reconstruction With Rotator Cuff Repair
| Advantages | Disadvantages |
|---|---|
| This technique improves biomechanics of the shoulder and treats pain. No complications in the donor site. Allows less hospitalization time and less bleeding than open procedures. |
Technically demanding. Allografts are expensive and may not be available for all surgical centers. |
Table 2.
Pearls and Pitfalls of Superior Capsular Reconstruction With Rotator Cuff Repair
| Pearls | Pitfalls |
|---|---|
| Evaluation of muscular strength and bone defects in the glenoid and humeral head is paramount prior to the surgery. A power rasp is useful to increase bone contact surface. 2 anchors must be placed using the Neviaser portal, at the 10 o'clock and 2 o'clock positions. If the patient lacks internal rotation, an inferior capsule release must be performed. |
Perform this technique in patients with severe glenohumeral osteoarthritis or bone defects in the glenoid or humeral head. Fixation of the graft in the wrong position can jeopardize the procedure. Wrong measurements of the distance between the anchors. Possible damage to suprascapular nerve. |
Rehabilitation Protocol
After the procedure, the patient should use a sling full time for 6 weeks. Aerobic exercises, walking on a level surface, and stationary biking are performed for 30 minutes. Passive range of motion is performed 4 times a week and should reach 90° of forward elevation in the first 2 weeks and ABD to 90°. ER at side is restricted to 45° and IR to 30° during this period. Active wrist and elbow range of motion is incentivized. The second phase initiates when the goals of the first phase are reached, normally after 2 weeks. The limits for this phase are 150° of forward elevation, 60° of ER, and ABD to 120°. The third phase (weeks 4-6) consists of full passive range of motion, as the patient tolerates. Deltoid isometric exercises start at week 4. Active assisted range of motion starts at week 6, when the use of sling is discontinued. Exercises to recover strength also start in this period. After 4 months, throwing is progressed from short to long distances. The return to full activities can be performed after 5 to 6 months and are individualized to each patient.
Discussion
Arthroscopic SCR with incorporation of a superior rotator cuff repair into the superior capsule patch graft is an effective technique that addresses the need for a viable treatment for the particularly difficult pathology of chronic, massive, irreparable superior rotator cuff tears presenting with superior capsule defects. Early efforts to use patch graft surgery to treat irreparable rotator cuff tears, whether implementing allograft,8 porcine dermal collagen implants,9 or porcine small intestinal submucosa,10 yielded a high rate of patch graft retears because the patch graft is abraded and torn by subacromial impingement due to a lack of superior stability. Similarly, in a study using conventional synthetic polyester interposition patch graft surgery where the graft was attached medially to the torn supraspinatus tendon and laterally to the greater tuberosity, no significant difference in acromiohumeral distance and residual superior instability was reported.11 After a study found that the articular capsule of the shoulder joint occupied a substantial area of the greater tuberosity, contrary to previously reported rotator cuff footprint width overestimations,12 Mihata et al.5 conducted a biomechanical cadaveric study comparing superior stability after tensor fascia lata autograft patch grafting medially to the torn supraspinatus tendon to patch grafting medially to the superior glenoid, in order to reconstruct the superior capsule. They found that while the supraspinatus tendon patch graft partially restored superior translation, the superior capsule patch graft fully restored it.5 In the clinical study of the technique following this biomechanical pilot study, Mihata et al.7 reported that the acromiohumeral distance was significantly increased, by 4.1 ± 1.7 mm, after arthroscopic SCR. Additionally, their findings showed that no graft tears or retears of the repaired rotator cuff tendon were seen in 20 of 24 shoulders (83.3%) during the 34.1-month mean follow-up period.7 Their average American Shoulder and Elbow Surgeons shoulder index improved from 23.5 to 92.9 (out of 100), the Japanese Orthopaedic Association score improved from 48.3 to 92.6 (out of 100), and the University of California, Los Angeles score improved from 9.9 to 32.4 (out of 35).7 This is comparable to results seen in the double-row technique13 and arthroscopic complete repair.14 In terms of preoperative active elevation and shoulder ABD strength, the results were improvements from 84° to 157° and from 3 + to 5-,7 similar to the measurements reported after arthroscopic complete repair for massive rotator cuff tears with severe fatty degeneration.15 As opposed to standard arthroscopic rotator cuff repair, Mihata et al.'s7 findings suggest that arthroscopic SCR may reliably restore shoulder function even in cases of >75% fatty degeneration of the infraspinatus as measured by the Goutallier grading system.15, 16
Whereas Mihata et al. used a tensor fascia lata autograft in the clinical application, we prefer, as do other groups,17, 18, 19 to use human acellular dermal patch allograft, which avoids any donor-site morbidity. The original biochemical study by Mihata et al.5 successfully used allograft, and allograft patches were used promisingly in another bridging technique in the clinical setting in the same context of irreparable massive rotator cuff tears.3, 20
We present a technique incorporating an SCR with a superior rotator cuff repair. This may be a reasonable treatment option for irreparable rotator cuff tears in patients wishing to avoid tendon transfer or reverse total shoulder arthroplasty or for whom these treatments are contraindicated. Only retrospective short-term results in small cohorts for other variations of this technique have been reported thus far. Long-term outcomes and clinical trials are needed to establish this new procedure.
Footnotes
The authors report the following potential conflicts of interest or sources of funding: M.T.P. receives support from Arthrex, JRF Ortho, and SLACK and has the following patent numbers issued: 9226743, 20150164498, 20150150594, 20110040339. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
The patient is placed in a beach chair position. The bony landmarks of the right acromion and coracoid are marked with a sterile marking pen. A posterior viewing portal is established, and a diagnostic arthroscopy is performed. Under arthroscopic visualization a midglenoid 5-mm cannula is placed. The defect due to the rotator cuff tear can be visualized. Careful debridement is performed anteriorly, superiorly, and posteriorly around the capsule and rotator cuff. Once the rotator cuff is freed up anteriorly, superiorly, posteriorly, and underneath the capsule interface, a 3.0-mm SutureTak anchor is placed at the 10 o'clock position using the Neviaser portal and then a similar anchor is placed at the 2 o'clock position in a similar fashion. A dermal patch for the superior capsular reconstruction is then prepared and sized to 25 mm anterior to posterior and 34 mm medial to the lateral patch. The sutures are then brought out laterally with one suture from each anchor passed through the patch. A tension slide technique is then used bring the graft to the superior glenoid (Fig 4). The capsule is repaired to the most medial aspect of the joint using 2 4.75-mm SwiveLock anchors and FiberTape suture (Arthrex). Once the graft is fixed onto the superior glenoid, the greater tuberosity is prepared anteriorly, middle, and posteriorly, using a burr and a radiofrequency burr. The rotator cuff is mobilized and pulled laterally. The FiberTape sutures are placed through the medial row and the capsule. Using a SwiveLock drill, 2 tunnels for the 4.75-mm SwiveLock are prepared. The FiberTape sutures already placed in the medial row are then passed through the SwiveLock, and moderate tension is applied to reduce the supra- and infraspinatus to the footprint on the greater tuberosity. This marks the completion of the surgical technique. The wounds are closed with 3-0 Monocryl followed by Dermabond, Steri-Strips, plains, abduction, and Medipore dressing.
References
- 1.Kim S.J., Kim S.H., Lee S.K., Seo J.W., Chun Y.M. Arthroscopic repair of massive contracted rotator cuff tears: aggressive release with anterior and posterior interval slides do not improve cuff healing and integrity. J Bone Joint Surg Am. 2013;95:1482–1488. doi: 10.2106/JBJS.L.01193. [DOI] [PubMed] [Google Scholar]
- 2.Ciampi P., Scotti C., Nonis A. The benefit of synthetic versus biological patch augmentation in the repair of posterosuperior massive rotator cuff tears: a 3-year follow-up study. Am J Sports Med. 2014;42:1169–1175. doi: 10.1177/0363546514525592. [DOI] [PubMed] [Google Scholar]
- 3.Gupta A.K., Hug K., Boggess B., Gavigan M., Toth A.P. Massive or 2-tendon rotator cuff tears in active patients with minimal glenohumeral arthritis: clinical and radiographic outcomes of reconstruction using dermal tissue matrix xenograft. Am J Sports Med. 2013;41:872–879. doi: 10.1177/0363546512475204. [DOI] [PubMed] [Google Scholar]
- 4.Ek E.T.H., Neukom L., Catanzaro S., Gerber C. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: results after five to fifteen years. J Shoulder Elbow Surg. 2013;22:1199–1208. doi: 10.1016/j.jse.2012.11.016. [DOI] [PubMed] [Google Scholar]
- 5.Mihata T., McGarry M.H., Pirolo J.M., Kinoshita M., Lee T.Q. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: a biomechanical cadaveric study. Am J Sports Med. 2012;40:2248–2255. doi: 10.1177/0363546512456195. [DOI] [PubMed] [Google Scholar]
- 6.Ishihara Y., Mihata T., Tomboli M. Role of the superior shoulder capsule in passive stability of the glenohumeral joint. J Shoulder Elbow Surg. 2014;23:642–648. doi: 10.1016/j.jse.2013.09.025. [DOI] [PubMed] [Google Scholar]
- 7.Mihata T., Lee T.Q., Watanabe C. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29:459–470. doi: 10.1016/j.arthro.2012.10.022. [DOI] [PubMed] [Google Scholar]
- 8.Moore D.R., Cain E.L., Schwartz M.L., Clancy W.G. Allograft reconstruction for massive, irreparable rotator cuff tears. Am J Sports Med. 2006;34:392–396. doi: 10.1177/0363546505281237. [DOI] [PubMed] [Google Scholar]
- 9.Soler J.A., Gidwani S., Curtis M.J. Early complications from the use of porcine dermal collagen implants (Permacol) as bridging constructs in the repair of massive rotator cuff tears. A report of 4 cases. Acta Orthop Belg. 2007;73:432–436. [PubMed] [Google Scholar]
- 10.Sclamberg S.G., Tibone J.E., Itamura J.M., Kasraeian S. Six-month magnetic resonance imaging follow-up of large and massive rotator cuff repairs reinforced with porcine small intestinal submucosa. J Shoulder Elbow Surg. 2004;13:538–541. doi: 10.1016/j.jse.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 11.Audenaert E., Van Nuffel J., Schepens A., Verhelst M., Verdonk R. Reconstruction of massive rotator cuff lesions with a synthetic interposition graft: a prospective study of 41 patients. Knee Surg Sports Traumatol Arthrosc. 2006;14:360–364. doi: 10.1007/s00167-005-0689-7. [DOI] [PubMed] [Google Scholar]
- 12.Nimura A., Kato A., Yamaguchi K. The superior capsule of the shoulder joint complements the insertion of the rotator cuff. J Shoulder Elbow Surg. 2012;21:867–872. doi: 10.1016/j.jse.2011.04.034. [DOI] [PubMed] [Google Scholar]
- 13.Sugaya H., Maeda K., Matsuki K., Moriishi J. Repair integrity and functional outcome after arthroscopic double-row rotator cuff repair. A prospective outcome study. J Bone Joint Surg Am. 2007;89:953–960. doi: 10.2106/JBJS.F.00512. [DOI] [PubMed] [Google Scholar]
- 14.Boileau P., Brassart N., Watkinson D.J. Arthroscopic repair of full-thickness tears of the supraspinatus: does the tendon really heal? J Bone Joint Surg Am. 2005;87:1229–1240. doi: 10.2106/JBJS.D.02035. [DOI] [PubMed] [Google Scholar]
- 15.Burkhart S.S., Barth J.R.H., Richards D.P., Zlatkin M.B., Larsen M. Arthroscopic repair of massive rotator cuff tears with stage 3 and 4 fatty degeneration. Arthroscopy. 2007;23:347–354. doi: 10.1016/j.arthro.2006.12.012. [DOI] [PubMed] [Google Scholar]
- 16.Goutallier D., Postel J.M., Bernageau J., Lavau L., Voisin M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res. 1994;304:78–83. [PubMed] [Google Scholar]
- 17.Petri M., Greenspoon J.A., Millett P.J. Arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthrosc Tech. 2015;4:e751–e755. doi: 10.1016/j.eats.2015.07.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hirahara A.M., Adams C.R. Arthroscopic superior capsular reconstruction for treatment of massive irreparable rotator cuff tears. Arthrosc Tech. 2015;4:e637–e641. doi: 10.1016/j.eats.2015.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Katthagen J.C., Tahal D.S., Millett P.J. Arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Healio. http://www.healio.com/orthopedics/arthroscopy/news/print/orthopedics-today/%7B0c782225-11e4-4201-8d9d-265d07558ee4%7D/arthroscopic-superior-capsule-reconstruction-for-irreparable-rotator-cuff-tears [DOI] [PMC free article] [PubMed]
- 20.Gupta A.K., Hug K., Berkoff D.J. Dermal tissue allograft for the repair of massive irreparable rotator cuff tears. Am J Sports Med. 2012;40:141–147. doi: 10.1177/0363546511422795. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient is placed in a beach chair position. The bony landmarks of the right acromion and coracoid are marked with a sterile marking pen. A posterior viewing portal is established, and a diagnostic arthroscopy is performed. Under arthroscopic visualization a midglenoid 5-mm cannula is placed. The defect due to the rotator cuff tear can be visualized. Careful debridement is performed anteriorly, superiorly, and posteriorly around the capsule and rotator cuff. Once the rotator cuff is freed up anteriorly, superiorly, posteriorly, and underneath the capsule interface, a 3.0-mm SutureTak anchor is placed at the 10 o'clock position using the Neviaser portal and then a similar anchor is placed at the 2 o'clock position in a similar fashion. A dermal patch for the superior capsular reconstruction is then prepared and sized to 25 mm anterior to posterior and 34 mm medial to the lateral patch. The sutures are then brought out laterally with one suture from each anchor passed through the patch. A tension slide technique is then used bring the graft to the superior glenoid (Fig 4). The capsule is repaired to the most medial aspect of the joint using 2 4.75-mm SwiveLock anchors and FiberTape suture (Arthrex). Once the graft is fixed onto the superior glenoid, the greater tuberosity is prepared anteriorly, middle, and posteriorly, using a burr and a radiofrequency burr. The rotator cuff is mobilized and pulled laterally. The FiberTape sutures are placed through the medial row and the capsule. Using a SwiveLock drill, 2 tunnels for the 4.75-mm SwiveLock are prepared. The FiberTape sutures already placed in the medial row are then passed through the SwiveLock, and moderate tension is applied to reduce the supra- and infraspinatus to the footprint on the greater tuberosity. This marks the completion of the surgical technique. The wounds are closed with 3-0 Monocryl followed by Dermabond, Steri-Strips, plains, abduction, and Medipore dressing.