

Abstract
Background
Although acute diarrhea often leads to acute dehydration and electrolyte imbalance, children with diarrhea also suffer long term morbidity, including recurrent or prolonged diarrhea, loss of weight, and linear growth faltering. They are also at increased risk of post-acute mortality. The objective of this systematic review was to identify interventions that address these longer term consequences of diarrhea.
Methods
We searched Medline for randomized controlled trials (RCTs) of interventions conducted in low- and middle-income countries, published between 1980 and 2016 that included children under 15 years of age with diarrhea and follow-up of at least 7 days. Effect measures were summarized by intervention. PRISMA guidelines were followed.
Results
Among 314 otherwise eligible RCTs, 65% were excluded because follow-up did not extend beyond 7 days. Forty-six trials were included, the majority of which (59%) were conducted in Southeast Asia (41% in Bangladesh alone). Most studies were small, 76% included less than 200 participants. Interventions included: therapeutic zinc alone (28.3%) or in combination with vitamin A (4.3%), high protein diets (19.6%), probiotics (10.9%), lactose free diets (10.9%), oral rehydration solution (ORS) formulations (8.7%), dietary supplements (6.5%), other dietary interventions (6.5%), and antimicrobials (4.3%). Prolonged or recurrent diarrhea was the most commonly reported outcome, and was assessed in ORS, probiotic, vitamin A, and zinc trials with no consistent benefit observed. Seven trials evaluated mortality, with follow-up times ranging from 8 days to 2 years. Only a single trial found a mortality benefit (therapeutic zinc). There were mixed results for dietary interventions affecting growth and diarrhea outcomes in the post-acute period.
Conclusion
Despite the significant post-acute mortality and morbidity associated with diarrheal episodes, there is sparse evidence evaluating the effects of interventions to decrease these sequelae. Adequately powered trials with extended follow-up are needed to identify effective interventions to prevent post-acute diarrhea outcomes.
Electronic supplementary material
The online version of this article (10.1186/s12889-018-5092-7) contains supplementary material, which is available to authorized users.
Keywords: Pediatric diarrhea management, Child growth, Diarrhea interventions, Child mortality, Long-term sequelae of diarrhea
Background
Close to 600,000 children die each year from diarrheal disease, the majority in low- and middle-income countries (LMICs) [1]. Children with a single episode of moderate-to-severe diarrhea (MSD) experience an 8.5-fold higher risk of dying in the 60-days following the episode compared to age-matched healthy children, despite standard diarrhea case management including rehydration and zinc [2]. A verbal autopsy study conducted in 7 LMICs found that 55.6% of pediatric diarrhea deaths occurred in children who had been rehydrated [3]. Although rehydration and zinc have resulted in millions of lives saved from diarrhea, they may be insufficient to prevent all diarrhea-associated mortality.
The consequences of diarrhea extend beyond acute dehydration and electrolyte imbalance. Over two-thirds of deaths associated with diarrhea occur more than 7 days after presentation [2]. An episode of MSD is also associated with subsequent loss of length/height-for-age z-score (LAZ/HAZ), a measure of chronic malnutrition [2, 4]. Undernutrition is linked to half of all diarrhea-associated mortality and is associated with other long-term outcomes including reduced school attendance and future earning potential [2, 5, 6].
While mortality from diarrheal diseases has declined since the 1990’s, incidence rates have remained stable and there is increasing recognition of the morbidity, disability, and long-term consequences associated with diarrhea. We conducted a systematic review to identify and summarize randomized controlled trials (RCTs) of diarrhea management interventions to determine effects on death, anthropometric status, and prevalence and incidence of diarrhea in the post-acute period.
Methods
The systematic review followed PRISMA guidelines. We searched Medline for English-language RCTs published between January 1, 1980 and October 31, 2016 conducted among children under 15 years of age presenting with diarrhea (all diarrhea definitions accepted) at the time of treatment. Specifically, we searched for trials evaluating 1 of the following interventions: antiemetics, antibiotics, antiprotozoals, antisecretories, dietary supplements, intravenous hydration therapy, oral rehydration therapy, probiotics, prebiotics, lactose replacement, and therapeutic zinc. These interventions were chosen based on consultation with experts in the field. The search terms used were as follows:
((((((((((((antibiotic OR antiinfective OR anti-infective OR antimicrobial OR antiparasitic OR anti-parasitic OR antiprotozoa* OR anti-protozoa* OR ciprofloxacin OR erythromycin OR metronidazole OR antiemetic* OR anti-emetic OR anti-vomit* OR antidiarrheal OR secretoinhibit* OR antipropulsive OR antisecret* OR anti-secret OR breast* OR formula* OR milk OR wean* OR treatment OR management OR “amylose maize starch” OR hams OR lams OR prebiotics OR “resistant starch” OR bifidobacter* OR lactobacill* OR lactococc* OR microbi* OR probiotic* OR fluid OR intravenous OR IV OR ORS OR “oral rehydration salt” OR ORT OR “oral rehydration therapy” OR polymer OR rehydration OR minerals OR zinc)))) AND (“1980/01/01”[Date - Publication]: “2016/10/31”[Date - Publication])) AND (((“bloody stool” OR diarrh* OR dysentery OR gastroenterit*))))) AND ((((clinical trial) OR placebo-controlled trial) OR randomized controlled trial))))) NOT cancer) NOT antibiotic associated diarrhea)
Filters: Clinical Trial; Humans; English; Child: birth-18 years
We excluded studies in 2 steps. The first step aimed to exclude trials that did not address the populations or interventions of interest. Specifically, studies conducted in high-income countries (as defined by the World Bank as of June 2015) [7], those that did not include children with diarrhea at enrollment, utilized a design other than an RCT, or did not present individual-level outcome data were excluded in the first round. The second round excluded trials with insufficient follow up (less than 7 days) and those that lacked outcome data on mortality, length/height, LAZ/HAZ, weight, weight-for-age z-score (WAZ), weight-for-height z-score (WHZ), mid upper arm circumference (MUAC), or diarrhea presence at a pre-specified follow-up point ≥7 days after enrollment. Although weight may be misclassified during diarrhea illness due to fluid loss, in the context of an RCT, groups were assumed to be balanced with regard to hydration status. Therefore, weight, WAZ, and WHZ were considered valid outcomes. Diarrhea duration (other than presence of diarrhea at a pre-specified time point beyond 7-days) and stool output were not included as outcomes because they were considered intermediate to the outcomes of interest in this review.
All titles and abstracts were screened by 2 reviewers (PBP and HEA) and abstracts of agreed-upon titles were examined for inclusion. Full texts of agreed-upon abstracts were reviewed for inclusion by RLB and HEA with final input from PBP. The following study-specific information was abstracted from included trials: intervention, control group, population, dates of enrollment, sample size, duration of follow up, reported outcomes, and data on effect sizes of relevant outcomes, and associated confidence intervals (CIs). Details on data abstraction and calculations are provided in the supplementary material for this manuscript (Additional file 1).
A modified Grading of Recommendations Assessment Development and Evaluation (GRADE) approach was developed to assess study design elements including sample size, number of participants lost to follow up or withdrawn from the study, and blinding and allocation concealment methods to evaluate the quality of studies. We did not assess the GRADE elements of directness or consistency, as these elements are specific to results reported within a given intervention and outcome category and this review assessed multiple interventions and outcomes. All trials started with 4 points because all were randomized controlled trials and 1 point was deducted for each of the following elements: sparse data (< 200 trial participants), > 5% loss-to-follow-up or withdraws, or lack of double-blinding. Reviewers (HA and RB) applied the modified GRADE system included in this review and categorized each study as high quality (4 points), moderate (3 points), low (2 points), or very low (1 point) based on their final score. In addition to the elements required for GRADE, from included trials we abstracted whether or not a primary endpoint was declared (and whether the primary endpoint was 1 of the endpoints included in this review) and any mention of power calculations for included outcomes.
Results
The Medline search returned 2815 titles, of which 693 abstracts and 432 full texts were reviewed, and 385 excluded based on full-text review (Fig. 1). Among the 314 studies that were eligible based on study location, design, and population (included based on first exclusion step), most (205 [65.2%]) were excluded for failure to meet our criteria for length of follow up (7 days or more) and 51 (16.2%) were excluded because no outcomes of interest were reported in the second exclusion phase.
Fig. 1.

Flow chart of included trials of diarrhea management interventions
Forty-six trials were included in this review, the majority (27 studies [58.7%]) of which were conducted in the WHO-classified Southeast Asia region [8–34], with 19 (70.4%) conducted in Bangladesh alone (Table 1). Seven studies (15.2%) were conducted in the Americas [35–41], 7 studies (15.2%) reported data from Africa [42–48], 2 from the Eastern Mediterranean (Pakistan) [49, 50] and 2 from Europe (Turkey) [51, 52]. One study was conducted in 3 countries (Ethiopia, Pakistan, and India) [53]. The majority of the trials were conducted in inpatient settings (35 studies, 76.1%). Five (10.9%) trials were community-based, and the remaining 6 (13.0%) were conducted in outpatient settings. The most common interventions included therapeutic zinc (15 studies [32.6%], 2 of which was assessed in the same trial as vitamin A), and high protein diets (9 studies [19.6%]). Probiotics were assessed in 5 studies (10.9%), and 5 trials evaluated lactose-free diets (10.9%). Four were trials of ORS formulations (8.7%), and 3 (6.5%) trials evaluated dietary supplements, including dietary fiber (2 studies), and glutamine (1 study). Three (6.5%) trials were of other dietary interventions, a semi-elemental diet and 2, 3-armed trials evaluated ready-to-use therapeutic food (RUTF) or micronutrient powder. Only 2 (4.3%) of the trials that fit our inclusion criteria evaluated antimicrobial treatments (1 antibiotic and 1 antiprotozoal). We did not find any trials of intravenous (IV) rehydration, antisecretory agents, or antiemetic agents that met our inclusion criteria. The sample size of included studies ranged from 18 to 8070 and only 11 (23.9%) of the 46 trials included more than 200 participants (1 ORS, 2 probiotic, 2 RUTF/micronutrient, 1 vitamin A + zinc, and 5 zinc trials). Just over half of included trials (52.2%) reported power/sample size calculations, the majority of which (11 [48%] of the 23) were powered for the outcome of diarrhea duration/stool output, outcomes not included in this systematic review.
Table 1.
Characteristics of included studies
| Reference [Ref #] | Country | Population | Intervention | Comparator | Number with follow up data | Pre-specified follow up time | Relevant outcomes measured and poweri | Modified GRADE score |
|---|---|---|---|---|---|---|---|---|
| Antimicrobial Intervention | ||||||||
| Gilman 1980 [8] | Bangladesh | Inpatient adults and children with blood, pus cells, and mucus in stool, 4 or more stools/day, and culture-confirmed Shigella infection | Low-dose ampicillin (50 mg/kg/day) | High-dose ampicillin (150 mg/kg/day) | 56 children | 21 days | Mortality (power/sample size calculations not reported) | Very lowΩ,ΦΨ |
| Amadi 2002 [42] | Zambia | Inpatient children 12–85 mo with diarrhea (at least 3 stools per day that take the shape of a container or can be poured) and Cryptosporidium oocysts | 5 mL of 20 g/L nitazoxanide oral suspension, twice daily for 3 days | Placebo | 96 | 8 days | Mortality (powered for outcome of clinical response) | ModerateΩ |
| Dietary Supplements | ||||||||
| Alam 2000 [26] | Bangladesh | Inpatient males 4–18 mo with acute non-dysenteric diarrhea | WHO ORS with dietary fiber(20 g/L Benefiber®) | Standard WHO-ORS | 150 | 7 days | Weight gain at day 7 from enrollment (powered for the outcome of stool output) | ModerateΩ |
| Rabbani 2001 [15] | Bangladesh | Severely malnourished (< 60% NCHS standard), inpatient male infants 5–12 mo with persistent diarrhea (> 3 loose stools/day for 14 days), treated with ciprofloxacin | Rice-based diet with dietary fiber (250 m/L cooked, green banana, 7 days; or rice-based diet with 1 g/kg to 8 g/kg of pectin supplement) 7 days | Calorically equivalent control diet: rice-based diet only, 7 days | 62 | At least 7 days, or until end of diarrhea | Proportions recovered from diarrhea [formed stool] at days 7, 8, 9, and 10 (powered for outcome of diarrhea recovery duration) | ModerateΩ |
| Yalcin 2004 [51] | Turkey | Inpatient children 6–24 mo with acute diarrhea | Glutamine supplement - 0.3 g/kg/day, for 7 days | Placebo | 143 | 3 months | Weight gain at day 30, 60, and 90 from enrollment (powered for the outcome of diarrhea duration) | LowΩ, ϑ |
| High Protein Diets | ||||||||
| Datta 1990 [9] | India | Inpatient children under 5 y/o with acute dysentery (visible blood and mucus in stools), treated with nalidixic acid | Extra servings of milk (30% of total daily caloric requirements), in addition to standard hospital diet | Standard hospital diet | 96 | 15 days | Weight and MUAC at day 15 (power/sample size calculations not reported) | Very lowΩ, Φ, ϑΨ |
| Kabir 1992 [10] | Bangladesh | Inpatient children 2–4 y/o with culture-confirmed Shigella dysentery, treated with nalidixic acid or other microbial | High protein diet (15% of total energy from protein), 21 days | Standard diet (7.5% of total energy from protein), 21 days | 22 | 21 days | Change in weight, height, WAZ, WHZ, HAZ, MUAC, and triceps skinfold thickness at day 21 from admission (power/sample size calculations not reported) | Very lowΩ, Φ, ϑΨ |
| Kabir 1993 [11] | Bangladesh | Outpatient children 2–5 y/o with acute diarrhea and culture-confirmed Shigella spp., treated with nalidixic acid or pivmecillinam | High protein diet (15% of total energy from protein), 21 days | Standard diet (7.5% of total energy from protein), 21 days | 69 | 21 days | Change in WHZ, WAZ, and HAZ at day 21 from admission (power/sample size calculations not reported) | Very lowΩ, Φ, ϑΨ |
| Mazumder 1997 [12] | Bangladesh | Malnourished (< 80% NCHS median), inpatient children 12–48 mo with bloody or bloody mucoid diarrhea and culture-confirmed Shigella, treated with nalidixic acid | High calorie and high protein diet, 4960 kJ/l for 10 days | Standard hospital diet, 2480 kJ/l for 10 days | 75 | 40 days | Percent change in WAZ and WHZ at 10, and 40 from admission (power/sample size calculations not reported) | LowΩ, Φ, Ψ |
| Nurko 1997 [36] | Mexico | Inpatient children 3–36 mo with persistent diarrhea (3 or more loose stools/day for 14 days or longer) and third-degree malnutrition (< 60% NCHS median), treated with TMP-SMX or metronidazole | High protein diet (2 groups: chicken-based diet, or soy-based diet)ii | Standard cultural dietary treatment for diarrhea (elemental diet or “Vivonex”) | 41 | 16 days minimum | Weight at end of intervention and at discharge; proportion with nutritional recoveryiii at end of intervention (powered for outcome of diarrhea duration) | Very low Ω, ϑ, Ψ |
| Kabir 1998 [13] | Bangladesh | Inpatient children 2–60 mo with acute bloody mucoid diarrhea, treated with nalidixic acid or pivmecillinam | High protein diet (15% of total energy from protein), 21 days | Standard protein diet (7.5% of total energy from protein), 21 days | 59 | 6 months post- intervention | Change in weight, height, WHZ, WAZ, and HAZ at 6 months compared to post-intervention measurements (power/sample size calculations not reported) | Very low Ω, Φ, ϑ, Ψ |
| Mazumder 2000 [14] | Bangladesh | Malnourished (< 80% of NCHS median) inpatient children 12–48 mo with acute bloody or mucoid diarrhea, treated with nalidixic acid of pivmecillinim | High calorie & protein milk-cereal formula (4960 kJ/l), 10 days | Control milk-cereal formula (2480 kJ/l), 10 days | 75 | 10 days | Percent change in WAZ at day 10, compared to admission WAZ (power/sample size calculations not reported) | Very lowΩ, ϑ, Ψ |
| Valentiner-Branth 2001 [43] | Guinnea-Bissau | Community-based children under 3 y/o with persistent diarrhea per mother’s report | Counseling on the importance of breastfeeding and of a nutritious diet, and a high protein millet gruel with a multivitamin tablet (including zinc), until the end of a 7 day period without diarrhea | Counseling on the importance of breastfeeding and of a nutritious diet | 101 | 9 months | Difference in knee-heel length, height and weight at end of intervention and day 90, compared to admission measurements (powered for outcome of diarrhea duration) | Very lowΩ, Φ, Ψ |
| Rollins 2007 [44] | South Africa | Inpatient HIV+ children 6–36 mo with persistent diarrhea (4 or more loose or watery stools/day, for 5 days or more) | Enhanced nutritional support: standard nutritional support + extra protein to provide 150 kcal/kg/day and 4.0–5.5 g protein/kg/day (as milk or powdered protein, depending on age), until diarrhea resolved | Standard nutritional support: maize porridge + milk formula, until diarrhea resolved | 104 | 26 weeks | Mortality, median change in weight-SDs ivand WAZ at 26 weeks; proportions underweight (WAZ < − 2 SDs) and stunted (LAZ < − 2 SDs) at 26 weeks (powered for outcome of weight change) | Very lowΩ, Φ, ϑ, Ψ |
| Lactose Free Diet | ||||||||
| Bhan 1988 [16] | India | Outpatient children 3–24 mo | Legume and cereal-based formula (lactose-free), until recovery or a minimum of 7 days | Calorically equivalent milk-based formula, until recovery or a minimum or 7 days | 57 | At least 7 days, or until end of diarrhea | Weight gain at day 7 and at recovery compared to admission weight (power/sample size calculations not reported) | Very lowΩ, Φ, ϑ, Ψ |
| Bhutta 1991 [50] | Pakistan | Outpatient males 6 mo - 3 yo with persistant diarrhea (increased frequeny and reduced consistency lasting 2 weeks or more) | Soy milk (lactose-free) for 7 days, followed by khitchri and yogurt for 7 days | Khitchri and yogurt for 14 days | 73 | 14 days | Weight gain at day 7 and 14 compared to admission weight (power/sample size calculations not reported) | Very lowΩ, Φ, ϑ, Ψ |
| Lozano 1994 [38] | Colombia | Inpatient children 1–24 mo with diarrhea (4 or more watery stools in a 24 h period) and dehydration | Lactose-free feeding formula, 21 days | Feeding formula with lactose, 21 days | 52 | 6 weeks post-discharge | Weight increment at 6 weeks (powered for outcomes of diarrhea duration) | Very lowΩ, Φ, ϑ, Ψ |
| Bhatnagar 1996 [17] | India | Inpatient \children 3–24 mo, with persistent diarrhea (3 or more liquid stools/day for 14 days) | Puffed rice cereal, sugar, oil, and milk protein, 120 h | Puffed rice cereal, sugar, oil, and egg white protein (lactose-free), 120 h | 116 | 4–6 weeks after discharge | Proportion of patients whose weight on day 7 was lower than at rehydration; probability of continuing diarrhea at each day to day 12 (power/sample size calculations not reported) | Very lowΩ, Φ, Ψ |
| de Mattos 2009 [37] | Brazil | Inpatient male infants 1–30 mo with persistent diarrhea (3 or more liquid stools per day for 14 days) | Amino-acid based diet or soy-based diet, or hydrolyzed protein-based dietv | Yogurt-based diet | 154 | 7 days post-discharge | Difference in weight gain and change in WHZ at discharge compared to admission measurements (powered for outcomes of stool output and diarrhea duration) | Very lowΩ, Φ, ϑ, Ψ |
| Other Dietary Interventions | ||||||||
| Eichenberger 1984 [35] | Brazil | Inpatient infants 1–11 mo with acute to subacute gastroenteritis with diarrhea | Semi-elemental diet with low osmolarity and high content of hydrolyzed lactalbumin | Standard hospital diet | 38 | 21 days | Weight at day 21 compared to weight at beginning of therapy (power/sample size calculations not reported) | Very low Ω, Φ, ϑ, Ψ |
| van der Kam 2016 [45] | Uganda | Non-malnourished, outpatient children 6–59 mo with diarrhea (3 or more loose stools [bloody or nonbloody] per 24 h by mothers’ report), malaria, or lower respiratory tract infections | Ready-to-use Therapeutic Foods (RUTF), plus instructions to feed the child an extra meal/day for 14 d; or micronutrient powder plus instructions to feed the child an extra meal/day for 14 d | An instruction to feed the child an extra meal/day for 14 d | 941 with diarrhea only | 6 months | Incidence of WHZ < − 2, MUAC < 115 mm, or nutritional oedema during follow up (powered for combined outcome of negative nutritional outcome)vi | Low ϑ, Ψ |
| van der Kam 2016 [46] | Nigeria | Non-malnourished or moderately malnourished outpatient children 6–59 mo with diarrhea (3 or more loose stools [bloody or nonbloody] per 24 h by mothers’ report), malaria, or lower respiratory tract infections | Ready-to-use Therapeutic Foods (RUTF), plus instructions to feed the child an extra meal/day for 14 d; or micronutrient powder plus instructions to feed the child an extra meal/day for 14 d | An instruction to feed the child an extra meal/day for 14 d | 1171 with diarrhea only | 6 months | For non-malnourished children at enrollment: Incidence of WHZ < − 2, MUAC < 115 mm, or nutritional oedema during follow up. For malnourished children at enrollment: Incidence of WHZ < − 3, MUAC < 115 mm, nutritional oedema. Or > 10% weight loss during follow up. Powered for combined outcome of negative nutritional outcomevii | Low ϑ, Ψ |
| Oral Rehydration Solution Formulations | ||||||||
| Santosham 1983 [39] | Panama | Inpatient 3 mo - 2 y/o who were well nourished, with acute diarrhea (more than 3 watery stools per day) | High potassium and chloride ORS, or standard WHO-ORS | Standard diet for diarrhea management (aerated beverages, bananas, cereals, and apple sauce) | 93 | 14 days | Weight at day 14, weight gain at day 14 as percent of enrollment weight (power/sample size calculations not reported) | Very lowΩ, Φ, Ψ |
| Ribeiro 1991 [40] | Brazil | Inpatient male infants less than 12 mo, with acute diarrhea and dehydration | Standard WHO-ORS with 30 mmol/L alanine | Standard WHO-ORS | 18 | 7 days | Weight gain at day 7 (power/sample size calculations not reported) | ModerateΩ |
| Faruque 1997 [21] | Bangladesh | Inpatient children 3–35 mo with acute non-dysenteric diarrhea | Glucose based ORS | Rice-powder based ORS | 471 | 16 days | Proportion with diarrhea at day 14, weight gain at day 16 (powered for outcomes of stool output, diarrhea duration and weight gain [70 g]) | Low Φ, Ψ |
| Alam 2009 [55] | Bangladesh | Severely malnourished (< 70% NCHS standard), inpatient infants 6–60 mo with acute diarrhea and culture-confirmed V. cholerae | Glucose-based ORS, or Glucose-based ORS plus amylase resistant starch | Rice-based ORS | 137 | 6 weeks | Time to attain 80% of median WLZ from enrollment; proportion with diarrhea at or after day 7 (power/sample size calculations not reported) | LowΩ, Ψ |
| Probiotics | ||||||||
| Boudraa 2001 [47] | Algeria | Inpatient children 3–24 mo with acute watery diarrhea (> 3 loose stools in the previous 24 h) | Standard formula fermented with L. bulgaricus and S. thermophilus (lactose and calorically equivalent) | Standard milk-based formula | 97 | 7 days | Weight gain at day 7 (power/sample size calculations not reported) | Very lowΩ, Φ, ϑ, Ψ |
| Villaruel 2007 [41] | Argentina | Outpatient children 3 mo - 2 yo, with acute diarrhea (3 or more liquid or loose stools in the preceding 24 h) | WHO-ORS and S. boulardii, 250 mg per day (patients < 1 yo) or 500 mg per day (patients 1 yo and older) | WHO-ORS and placebo | 72 | 1 month | Proportion of patients with diarrhea at or after day 7 (power/sample size calculations not reported) | LowΩ, ϑ |
| Misra 2009 [19] | India | Inpatient infants < 36 mo with diarrhea (more than 3 stools per day that take the shape of their container) | Lactobacillus rhamnosus GG (10^9 live bacteria) | Placebo | 207 | 6 weeks | Change in WHZ at 6 weeks(powered for outcomes of stool output and diarrhea duration) | High |
| Sindhu 2014 [20] | India | Children 6 m to 5 years with diarrhea testing positive for either rotavirus or Cryptosporidium infection | Lactobacillus rhamnuosus GG (10^10 organisms) | Placebo | 123 | 4 weeks | Proportions stunted (HAZ < − 2 SD), underweight (WAZ < − 2 SD), and wasted (WHZ < − 2 SD) at 4 weeks, proportion with diarrhea or severe diarrhea during follow-up (powered for outcome of L:M ratio) | ModerateΩ |
| Dinleyici 2014 [52] | Turkey | Inpatient children 3–60 mo with acute watery diarrhea | WHO-ORS + lactobacillus reuteri 17,938 (10^8 CFU) for 5 days | WHO-ORS only | 127 | 12 days | Proportion with diarrhea at day 12 (powered for outcome of diarrhea duration) | Very lowΩ, Φ,Ψ |
| Therapeutic Micronutrients (Vitamin A and Zinc)viii | ||||||||
| Faruque 1999 [34] | Bangladesh | Inpatient children 6 mo - 2 yo with acute diarrhea (3 or more liquid stools in the previous 24 h) | 4500 μg vitamin A, 15 day, 14.2 mg Zinc acetate, 15 days, or bothix | Placebo | 656 | 17 days | Proportion with diarrhea at day 7 and 16 (powered for outcome of diarrhea duration) | High |
| Khatun 2001 [22] | Bangladesh | Inpatient children 6 mo - 4 yo with persistent diarrhea (diarrhea for > 14 days duration) | Multivitamin (D, C, B1 B2 B6) syrup and 20 mg elemental zinc (as zinc acetate, 5 ml twice daily for 7 days), multivitamin syrup with Vit A (100,000 IU for children < 1 yo, 200,000 for children > 1 yo), or both | Multivitamin (D, C, B1 B2 B6) syrup only | 93 | 7 days | Weight at day 7, weight gain at day 7 compared to day 1, proportions with diarrhea at day 7 (powered for outcome of clinical recovery) | ModerateΩ |
| Therapeutic Micronutrients (Zinc Alone) | ||||||||
| Sazawal 1995 [23] | India | Inpatient children 6–35 mo, with acute diarrhea (at least 4 unformed stools in the preceding 24 h) | Multivitamin syrup (A, B2, B6, D3, E) plus zinc gluconate (20 mg of elemental zinc) | Multivitamin syrup (A, B2, B6, D3, E) only | 937 | At least 120 days | Proportion of diarrhea episodes that last longer than 7 days, proportion of diarrhea episodes taken to a physician during follow up (power/sample size calculations not reported) | High |
| Roy 1998 [24] | Bangladesh | Inpatient 3–24 mo with persistent diarrhea | Multivitamin syrup (Vit A, B1, B2, B3, B6, D, Ca) with 20 mg elemental zinc per day for 14 days | Multivitamin syrup (Vit A, B1, B2, B3, B6, D, Ca) only for 14 days | 141 | 15 days | Mortality, weight gain at discharge compared to admission weight, proportion with diarrhea after day 15 (powered for outcome of diarrhea duration) | Very lowΩ, Φ, ϑ |
| Bhutta 1999 [49] | Pakistan | Inpatient children 6–36 mo with persistent diarrhea | Multivitamin syrup (Vit A, B1, B2, B3, B6, B12, C, D, Ca) with 3 mg elemental zinc per kg per day for 28 days | Multivitamin syrup (Vit A, B1, B2, B3, B6, B12, C, D, Ca) only for 28 days | 77 | 28 days | Weight gain at day 7 and 14; overall weightincrement at day 14; MUAC at day 7 and 14; overall MUAC increment (powered for outcome of day 14 weight gain) | LowΩ, ϑ |
| Roy 1999 [25] | Bangladesh | Malnourished (< 76% of NCHS median), inpatient children 3–24 months with acute diarrhea | Multivitamin syrup (vit A, B1, B2, B6, D, and Ca) with 20 mg elemental zinc per day for 14 days | Multivitamin syrup (vit A, B1, B2, B6, D, and Ca) only for 14 days | 29 | 10 weeks | Weight gain at each week of for 8 weeks, length gain at each week for 8 weeks (power/sample size calculations not reported) | LowΩ, ϑ |
| Baqui 2002 [27] | Bangladesh | Community-based children 3–59 mo with diarrhea of any duration | ORS with 20 mg zinc per day, 14 days | ORS only | 8070 | 2 yearsx | Incidence of diarrhea, mortality (powered for the outcomes of diarrhea duration, diarrhea incidence, acute lower respiratory infections incidence, admission to hospital for diarrhoea or acute lower respiratory infections, and child mortality) | Low Φ, Ψ |
| Walker 2007 [53] | Ethiopia, Pakistan, and India | Infants 1–5 mo with acute diarrhea, identified through home visits by health workers and community based study clinics | ORS with 10 mg zinc sulfate, daily for 14 days | ORS with placebo | 1042 | 8 weeks | Weight at week 4 and 8, length at week 4 and 8, proportion of infants with ≥1 episode of any diarrhea, ≥ 2 episode of any diarrhea, or ≥1 episode of dysentery (any day with blood in the stool); incidence and prevalence of diarrhea; mortality (powered for anthropometry and morbidity outcomes) | High |
| Roy 2007 [28] | Bangladesh | Convalescent children 3–24 mo, after recovery from persistent diarrhea | Multivitamin syrup (Unspecified) with 20 mg elemental zinc, 14 days | Multivitamin syrup (unspecified) only, 14 days | 147 | 12 weeks | Mortality, gain in length and weight at 12 weeks, incidence of subsequent diarrhea episodes (power/sample size calculations not reported) | LowΩ, Φ, ϑ |
| Roy 2008 [29] | Bangladesh | Moderately malnourished (weight/age 61–75% of NCHS median), inpatient children age 12–59 m with acute bloody-mucoid diarrhea or febrile diarrhea, and lab-confirmed Shigella spp | Multivitamin syrup (A, D, B complex, Ca) with zinc acete (10 mg elemental Zn/5 mL), for 14 days | Multivitamin syrup (Vit A, D, B complex, Ca) only | 30xi | 6 months | Diarrhea incidence and duration of episodes during 6 mo follow up (power/sample size calculations not reported) | LowΩ, ϑ |
| Fajolu 2008 [48] | Nigeria | Outpatient children 6–24 mo with acute diarrhea (3 or more loose, liquid or watery stools in a 24 h period) | 20 mg of elemental zinc (zinc sulphate monohydrate) for patients > 1 y/o, 10 mg of elemental zinc, 14 days, for patients < 1 y/o | Placebo | 60 | 3 months | Weight gain at 3 months, number and duration of subsequent diarrhea episodes during follow up (power/sample size calculations not reported) | ModerateΩ |
| Larson 2010 [30] | Bangladesh | Community-based children 6–23 mo with acute diarrhea and culture-confirmed ETEC | 10 days of zinc (10 mg/d) + additional 3 months of zinc supplementation (10 mg/d) | 10 days of zinc (10 mg/d) only | 333 | 9 months | Incidence rate of diarrhea illness during follow up (powered for the incidence of acute upper respiratory tract infections) | Moderateϑ |
| Alam 2011 [31] | Bangladesh | Community-based children 4–59 mo with diarrhea (3 or more loose or liquid stools in the previous 24 h) | Short course zinc - 20 mg elemental zinc, 5 days | Standard course zinc - 20 mg elemental zinc, 10 days | 1622 | 90 days | Number of diarrheal episodes and days of diarrhea during follow up; proportion with at least 1 subsequent episode of diarrhea, prolonged diarrhea, or persistent diarrhea during follow up; day of onset of first subsequent diarrhea episode during follow up (powered for the outcome of diarrhea incidence) | High |
| Patel 2013 [32] | India | Outpatient children 6–59 mo with acute diarrhea (> 3 unformed stools in the previous 24 h per mother’s report) | Zinc (2 mg/kg/day) or zinc + copper (Zn 2 mg/kg/day + Cu 0.2 mg/kg/day), 14 days | Placebo | 724 | 12 weeks | Proportion with at least 1 diarrhea episode, 2 diarrhea episodes, or 1 dysentery episode during follow up; number and duration of subsequent diarrhea episodes; change in WAZ, WHZ, and HAZ from enrollment measurements every 2 weeks for 12 weeks (power/sample size calculations not reported) | High |
| Negi 2015 [33] | India | Children 5–12 yrs. presenting to pediatric emergency units with acute watery diarrhea (3 or more episodes of loose stools over 24 h of < 72 h duration), with some or severe dehydration, and having had no treatment | Zinc (20 mg/day) for 14 days | Placebo | 134 | 3 months | Risk of having at least 1 episode of diarrhea during follow up (power/sample size calculations not reported) | LowΩ, ϑ |
iOutcome listed are only the outcomes of interest for the present systematic review
iiDuration of diets was variable. Diets were started at low concentrations and were advanced every 48 hours if no sign of intolerance. If there were signs of intolerance, diets were maintained or decreased as necessary. When full concentrations were reached, the diet was given for an additional 7 days.
iiiDefined as when diarrhea had ceased and patient had consistent weight gain for at least 48 hours
ivDefined as age- and sex-specific weight standard deviation scores, from the National Center for Health Statistics median value
vAll diets were equivalent in calorie and protein composition
viStudy included children with multiple admission (not just diarrhea) therefore only included data for children who had diarrhea at time of treatment. Power was determined for all children (not stratified by diagnosis)
viiStudy included children with multiple admission (not just diarrhea) therefore only included data for children who had diarrhea at time of treatment. Power was determined for all children (not stratified by diagnosis)
viiiStudies in this intervention category are randomized controlled trials with a factorial design, evaluating both Vitamin A and Zinc
ixInvestigators included 2 strata of study subjects: A “standard dose stratum” with the dosages given, and a “High dose stratum” with 40 mg zinc acetate daily, 15 days (Vit A dosage was unchanged)
xDiarrhea morbidity data were collected from “samples of time periods” throughout the 2 year follow up period. Mortality rates were calculated using 11,881 child-years of person-time, and incidence rates were calculated using 41,788 child-weeks of person-time
xiThirty completed 6 month follow up; 50 completed 7-day clinical study
ΩSparse data (sample size is <200 participants total)
ΦBlinding and allocation process (not double-blind)
ϑFollow up and withdrawals (>5% of sample size)
ΨLack of placebo
Of the 46 clinical trials evaluated using the modified GRADE system, 6 (13.0%) scored high, 8 (17.4%) scored moderate, 11 (23.9%) scored low, and 21 (45.7%) scored very low (Table 1). The most common deduction was for sparse data (35 [76.1%]), followed by deductions related to follow-up and withdrawals (24 [52.2%]), or blinding/allocation process (21 [45.7%]).
Mortality
Seven studies (15.2%) presented data on post-acute mortality, with follow-up ranging from 8-days to 2 years. Four were trials of therapeutic zinc interventions, [24, 27, 28, 53], 2 antimicrobial treatments [8, 42], and 1 of a high protein diet [44]. Two of the zinc trials were large studies (8070 and 1042 subjects, respectively) [27, 53] but the remaining 5 included less than 150 participants (Fig. 2, Table 2). None of the 7 trials were adequately powered for a mortality endpoint. Only 1 trial, a cluster randomized trial of zinc, found a lower non-injury mortality rate in children living in communities randomized to ORS and zinc compared to those using ORS alone (relative risk [RR] = 0.49 [95% confidence interval {95% CI}: 0.25, 0.94]) [27]. The remaining 6 studies reported non-significant risk differences ranging in magnitude from 70 more to 105 less deaths per 1000 children [8, 44] and relative risks ranging from 0.18 to 1.34 [24, 44].
Fig. 2.

Effect of diarrhea management interventions on mortality (relative risk, risk difference, and associated 95% confidence interval)
Table 2.
Intervention effects on post-acute (≥7 days after enrollment) mortality, length, weight, and/or diarrhea presence
| Reference | Intervention | Comparator | Relevant Outcomes and Results | ||
|---|---|---|---|---|---|
| Antimicrobial Interventions | |||||
| Gilman 1980 [8] | Low dose ampicillin (50 mg/kg/day) | Standard dose ampicillin (150 mg/kg/day) | Mortality | Risk Difference (95% CI) | −0.11 (− 0.24, 0.03)i |
| Relative Risk (95% CI) | Undefined | ||||
| Amadi 2002 [42] | 5 mL of 20 g/L nitazoxanide, twice daily for 3 days | Placebo | Mortality | Risk Difference (95% CI) | −0.07 (− 0.21, 0.06) |
| Relative Risk (95% CI) | 0.58 (0.21, 1.63) | ||||
| Dietary Supplements | |||||
| Alam 2000 [26] | ORS with dietary fiber (Benefiber®) | WHO- ORS only | Difference in weight gain at day 7, g (95% CI) | 52 (−18.73, 122.73) | |
| Rabbani 2001 [15] | Rice-based diet with dietary fiber (green banana or pectin supplement), 7 days | Rice-based diet only | Proportions recovered from diarrhea (formed stool) at each day to day 10 | Higher in banana and pectin groups than in control groupii | |
| Yalcin 2004 [51] | Glutamine supplement, 0.3 g/kg/day, for 7 days | Placebo | Difference in weight gain at day 30, g (95% CI)iii | 130 (12.67, 247.33) | |
| Difference in weight gain at day 60, g (95% CI) | 45 (−80.80, 170.80) | ||||
| Difference in weight gain at day 90, g (95% CI) | 107 (−57.30, 271.30) | ||||
| High Protein Diets | |||||
| Datta 1990 [9] | High protein diet, length unspecified | Standard hospital diet | Difference in weight at day 15, kg (95% CI) | 0.30 (−0.18, 0.78) | |
| Difference in MUAC at day 15, cm (95% CI) | 0.00 (−0.37, 0.37) | ||||
| Kabir 1992 [10] | High protein diet (15% of total energy from protein), 21 days | Standard diet (7.5% of total energy from protein), 21 days | Difference in change in weight at day 21 from admission, kg (95% CI) | 0.47 (0.12, 0.82) | |
| Difference in change in height at day 21, from admission, cm (95% CI) | 0.09 (−0.57, 0.75) | ||||
| Difference in change in WAZ at day 21 from admission (95% CI) | 0.30 (0.03, 0.57) | ||||
| Difference in change in WHZ at day 21 from admission (95% CI) | 0.40 (0.05, 0.75) | ||||
| Difference in change in MUAC at day 21 from admission, cm (95% CI) | 0.44 (0.08, 0.80) | ||||
| Difference in change in triceps skinfold thickness at day 21 from admission, cm (95% CI) | 0.32 (−0.29, 0.93) | ||||
| Kabir 1993 [11] | High protein diet, 21 days | Standard protein diet, 21 days | Difference in change in WAZ at day 21, from admission (95% CI) | 0.23 (0.07, 0.39) | |
| Difference in change in WHZ at day 21, from admission (95% CI) | 0.25 (0.05, 0.45) | ||||
| Difference in change in HAZ at day 21, from admission (95% CI) | 0.90 (0.05, 0.13) | ||||
| Mazumder 1997 [12] | High calorie & high protein milk-cereal diet, 4960 kJ/l (10 days) | Standard diet, 2480 kJ/l (10 days) | Difference in percent change in WAZ at day 10 and 40, fromadmission (95% CI) | Day 10: 3.50 (1.86, 5.14) | |
| Day 40: 3.11 (0.92, 5.30) | |||||
| Difference in percent change in WHZ at day 10 and 40, from admission (95% CI) | Day 10: 3.76 (1.92, 3.60) | ||||
| Day 40: 3.34 (0.76, 5.90) | |||||
| Nurko 1997 [36] | High protein chicken-based diet or high protein soy-based diet (Nursoy formula)iv | Calorically equivalent standard “elemental diet” (Vivonex) | Difference in weight at end of protocol, gv (95% CI) | Comparing soy group to control | − 204 (− 1178.40, 770.40) |
| Comparing chicken group to control | −445 (− 1522.70, 632.70) | ||||
| Difference in weight at discharge from enrollment, g (95% CI) | Comparing soy group to control | −92 (− 1189.60, 1005.60) | |||
| Comparing chicken group to control | − 428 (− 1539.80, 683.80) | ||||
| Proportion with nutritional recoveryvi(RR [95%]) | Comparing soy group to control | 1.13 (0.79, 1.61) | |||
| Comparing chicken group to control | 1.20 (0.86, 1.7) | ||||
| Kabir 1998 [13] | High protein diet (15% of total energy from protein), 21 days | Standard protein diet (7.5% of total energy from protein), 21 days | Difference in change in weight at 6 mo, from post-intervention weight, kg (95% CI) | 0.10 (−0.24, 0.44) | |
| Difference in change in height at 6 mo, from post-intervention height, cm (95% CI) | 1.10 (0.56, 1.64) | ||||
| Difference in change in WAZ at 6 mo, from post-intervention WAZ (95% CI) | 0.07 (−0.17, 0.31) | ||||
| Difference in change in WHZ at 6 mo, from post-intervention WHZ (95% CI) | −0.09 (− 0.35, 0.17) | ||||
| Difference in change in HAZ at 6 mo, from post-intervention HAZ (95% CI) | 0.28 (0.12, 0.44) | ||||
| Mazumder 2000 [14] | High calorie & protein milk-cereal formula (4960 kJ/l), 10 days | Control milk-cereal formula (2480 kJ/l), 10 days | Difference in percent change in WAZ at day 10, from admission WAZ (95% CI) | 3.50 (2.08, 4.91) | |
| Valentiner-Branth 2001 [43] | Counseling on the importance of breastfeeding and of a nutritious diet, and a high protein millet gruel with a multivitamin tablet (including zinc), until the end of a 7 day period without diarrhea | Counseling on the importance of breastfeeding and of a nutritious diet | Difference in weight gain at end of intervention and day 90, g/wk.vii(95% CI) | Day 90 | 61.50 (49.20, 73.80) |
| End of intervention | 12.50 (7.70, 17.30) | ||||
| Difference in change in knee heel length at end of intervention and day 90, mm/y (95% CI) | Day 90 | 2.70 (−4.60, 10.00) | |||
| End of intervention | 7.50 (4.80, 10.20) | ||||
| Difference in change in height between groups at day 90, (cm/y)2 (95% CI)viii | 0.65 (0.11, 1.19) | ||||
| Rollins 2007 [44] | Standard nutritional support + extra protein to provide 150 kcal/kg/day and 4.0–5.5 g protein/kg/day | Standard nutritional support: maize porridge + milk formula | Mortality at 26 weeks | Relative risk | 1.34 (95% CI: 0.79, 2.27) |
| Risk difference | 7.4% (−4.7%,20.5%) | ||||
| Median change in weight- SDs ixat 26 weeks | Greater gain in intervention group (p < 0.001) | ||||
| Median change in WAZ at 26 weeks | Greater gain in intervention group (p < 0.05) | ||||
| Proportion underweight (WAZ < −2 SDs) at 26 weeks (Prevalence Ratio [95% CI]) | 0.48 (0.30, 0.77) | ||||
| Proportion stunted (LAZ < − 2 SDs) at 26 weeks (Prevalence Ratio[95% CI]) | 0.87 (0.67, 1.13) | ||||
| Lactose Free Diets | |||||
| Bhan 1988 [16] | Legume and cereal-based formula (lactose-free), until recovery or 7 days min | Calorically equivalent milk-based formula, until recovery or 7 days min | Difference in weight gain at day 7, g/kg admission weight/24 h (95% CI) | −3.20 (−6.86, 0.46) | |
| Difference in weight gain at recovery, g/kg admission weight/24 h (95% CI) | −3.80 (−7.15, −0.44) | ||||
| Bhutta 1991 [50] | Soy milk (lactose-free) for 7 days, followed by khitchri and yogurt for 7 days | Khitchri and yogurt for 14 days | Difference in weight gain at day 7 and 14, g/wk. (95% CI) | Day 7: −400 (− 559.40, − 240.60) | |
| Day 14: 385.7 (209.60, 561.80) | |||||
| Lozano 1994 [38] | Corn-based (lactose-free) formula, 21 days | Milk-based formula, 21 days | Difference in weight increment at 6 weeks, kg (95% CI) | −0.02 (− 0.30, 0.26) | |
| Bhatnagar 1996 [17] | Rice-based formula with egg white protein (lactose-free), until discharge | Rice-based formula with milk protein, until discharge | Proportion of patients whose weight on day 7 was lower than at rehydration (Prevalence Ratio [95% CI]) | 0.97 (0.06, 15.19) | |
| Probability of continuing diarrhea at each day to day 12 | No significant difference (p = 0.76)x | ||||
| de Mattos 2009 [37] | Amino-acid based diet, isolated soy-based, or hyrolyzed casein-based diet; until discharge | Yogurt-based dietxi until discharge | Difference in weight gain at discharge among groups at discharge | No difference among groupsxii | |
| Change in WHZ at discharge | Similar improvement in all groupsxiii | ||||
| Other Dietary Interventions | |||||
| Eichenberger 1984 [35] | Semi-elemental diet with low osmolarity and high hydrolyzed lactalbumin, at least 21 days | Standard hospital diet | Weight at day 21 compared to weight at beginning of therapy | Better in intervention groupxiv | |
| van der Kam 2016 (Uganda) [45] | RUTF, plus instructions to feed the child an extra meal/day for 14 d; or micronutrient powder plus instructions to feed the child an extra meal/day for 14 d | An instruction to feed the child an extra meal/day for 14 d | Relative Risk of first event of malnutrition (95% CI) | RUTF vs micronutrient group | 0.68 (0.37, 1.22) |
| RUTF vs control group | 0.62 (0.35, 1.10) | ||||
| Micronutrient group vs control | 0.92 (0.54, 1.54) | ||||
| van der Kam 2016 (Nigeria) [46] | RUTF, plus instructions to feed the child an extra meal/day for 14 d; or micronutrient powder plus instructions to feed the child an extra meal/day for 14 d | An instruction to feed the child an extra meal/day for 14 d | Relative Risk of first event of malnutrition (95% CI) | RUTF vs micronutrient group | 1.12 (0.84, 1.50) |
| RUTF vs control group | 0.91 (0.69, 1.20) | ||||
| Micronutrient group vs control | 0.81 (0.61,1.09xv) | ||||
| ORS Formulations | |||||
| Santosham 1983 [39] | High potassium/ high chloride ORS, or standard WHO-ORS, with regular diet | Standard diet for diarrhea management | Difference in weight at day 14, kg (95% CI) | Comparing high potassium/chloride to control | −0.3 (−1.45, 0.85) |
| Comparing standard ORS to control | −0.50 (− 1.86, 0.76) | ||||
| Difference in percent weight gain at day 14 (95% CI) | Comparing high potassium/chloride to control | 2.00 (1.57, 2.42) | |||
| Comparing standard ORS to control | 2.30 (1.82, 2.77) | ||||
| Ribeiro 1991 [40] | Alanine-based ORS | Standard WHO-ORS | Difference in weight gain at day 7, g (95% CI) | 18 (−94.37, 130.38) | |
| Faruque 1997 [21] | Glucose-based ORS | Rice powder-based ORS, equivalent in electrolyte content | Proportion with diarrhea at day 14 (RR [95% CI]) | 0.80 (0.21, 2.95) | |
| Difference in weight gain at day 16, g | Similar between groupsxvi | ||||
| Alam 2009 [55] | Glucose-based ORS, or glucose-based ORS with amylase-resistant starch (ARS) | Rice-based ORS | Difference in time to attain 80% of median WLZ, days (95% CI) | Difference between glucose and rice ORS | − 0.06 (− 1.19, 1.07) |
| Difference between glucose with amylase resistant starch and rice ORS | − 0.08 (− 1.20, 1.04) | ||||
| Proportion with diarrhea at or after day 7 (RR [95% CI]) | Risk in glucose ORS group compared to rice ORS group (RR, [95% CI]) | 1.00 (0.15, 6.86) | |||
| Risk in glucose with ARS group compared to rice ORS groups (RR, [95% CI]) | 0.49 (0.05, 5.27) | ||||
| Probiotics | |||||
| Boudraa 2001 [47] | Milk-based formula fermented with L. bulgaricus S. andthermophilus | Milk-based formula only | Difference in weight gain at day 7, g (95% CI) | 43 (− 109.18, 195.18) | |
| Difference in weight gain at day 7, g/kg (95% CI) | 4.4 (−5.50, 14.30) | ||||
| Villarruel 2007 [41] | S. boulardii capsules | Placebo | Proportion with diarrhea on day 7 (Prevalence Ratio [95% CI]) | 0.39 (0.20, 0.74) | |
| Proportion with diarrhea after day 7 (Prevalence Ratio [95% CI]) | 0.25 (0.07, 0.82) | ||||
| Misra 2009 [19] | L. rhamnosus GG 109 CFU | Placebo | Difference in change in WHZ at 6 weeks | No difference between groups (p = 0.06) | |
| Sindhu 2014 [20] | L. rhamnosus GG 1010 CFU | Placebo | Proportion with diarrhea at 4 weeks follow up (Prevalence Ratio [95% CI]) | 0.65 (0.40, 1.07) | |
| Proportion with severe diarrhea during follow-up (Prevalence Ratio [95% CI]) | 1.15 (0.65, 2.05) | ||||
| Proportion with diarrhea requiring hospitalization during follow-up (Prevalence Ratio [95% CI]) | 1.03 (0.54, 1.98) | ||||
| Proportion stunted (HAZ < −2 SD) at week 4 (Prevalence Ratio [95% CI]) | 1.77 (1.00, 3.13) | ||||
| Proportion wasted (WHZ < − 2 SD) at week 4 (Prevalence Ratio [95% CI]) | 0.53 (0.16, 1.71) | ||||
| Proportion underweight (WAZ < − 2 SD) at week 4 (Prevalence Ratio [95% CI]) | 1.66 (0.83, 3.30) | ||||
| Dinleyici 2014 [52] | ORS with L. reuteri 17,938 108 CFU | ORS only | Proportion with diarrhea at day 12 (Prevalence Difference [95% CI])xvii | 0.17 (0.08, 0.26) | |
| Therapeutic Micronutrients (Vitamin A and Zinc) | |||||
| Faruque 1999 [34] | Vitamin A (4500 μg retinol equivalent daily for 15 days), zinc acetate (14.2 mg daily for 15 days),xviiior bothxix | Placebo | Proportion with diarrhea on day 7 (Prevalence Ratio [95% CI]) | Zinc-supplemented vs. non-supplemented | 0.64 (0.43, 0.96) |
| Vitamin A –supplemented vs. non-supplemented | 0.78 (0.52, 1.49) | ||||
| Proportion with diarrhea on day 16 (Prevalence Ratio [95% CI]) | Zinc-supplemented vs. non-supplemented | 0.67 (0.24, 1.85) | |||
| Vitamin A –supplemented group vs. non-supplemented | 0.67 (0.24, 1.85) | ||||
| Khatun 2001 [22] | Multivitamin syrup with 20 mg elemental zinc (twice daily for 7 days), or multivitamin syrup with Vitamin Axx or both | Multivitamin syrup only | Difference in change in weight at day 7 compared to day 1, gxxi | Zinc group vs control | 0.11 kg (p = 0.045) |
| Vitamin A group vs control | 0.07 kg (p = 0.21) | ||||
| Zinc+Vitamin A vs. control | 0.06 kg (p = 0.074) | ||||
| Proportion with diarrhea at day 7, (Prevalence Ratio [95% CI]) | Zinc group vs. control | 0.23 (0.08, 0.71) | |||
| Vitamin A group vs. control | 0.92 (0.54, 1.59) | ||||
| Zinc+Vitamin A vs. control | 0.62 (0.31, 1.21) | ||||
| Therapeutic Micronutrients (Zinc alone) | |||||
| Sazawal 1995 [23] | Multivitamin syrup with 20 mg elemental zincxxii | Multivitamin syrup only | Proportion of episodes lasting longer than 7 days (Prevalence Ratio [95% CI]) | 0.87 (0.65, 1.16) | |
| Proportion of diarrhea episodes taken to a physician during follow up (Prevalence Ratio [95% CI]) | 0.78 (0.57, 1.07) | ||||
| Roy 1998 [24] | Multivitamin syrup with 20 mg elemental zinc, 14 days | Multivitamin syrup only | Mortality | Relative Risk (95% CI) | 0.18 (0.02, 1.49) |
| Risk Difference (95% CI) | −0.05 (− 0.11, 0.01) | ||||
| Change in weight at discharge, gxxiii | Mean body weight in intervention group was maintained while body weight decreased in control group | ||||
| Proportion with diarrhea after day 15 (RR [95% CI])xxiv | 0.99 (0.53, 1.88) | ||||
| Bhutta 1999 [49] | Multivitamin with 3 mg of elemental zinc per kg of body weight, 28 days | Multivitamin only | Difference in weight at day 7 and 14, kgxxv (95% CI) | Day 7: −0.57 (−1.14, − 0.002) | |
| Day 14: −0.46 (− 1.06, 0.14) | |||||
| Difference in overall weight increment at day 14, g/kg/day | 1.60 (− 1.48, 4.68) | ||||
| Difference in MUAC at day 7 and 14, cm (95% CI) | Day 7: −0.30 (− 0.98, 0.38) | ||||
| Day 14: −0.40 (−1.08, 0.28) | |||||
| Difference in overall MUAC increment, cm (95% CI) | 0.00 (−0.13, 0.13) | ||||
| Roy 1999 [25] | Multivitamin with 20 mg of elemental zinc, 14 days | Multivitamin only | Difference in weight gain at each week of 8 week follow up, g (95% CI) | Week 1: 30 (−204.70, 264.73) | |
| Week 2: −4 (− 202.60, 194.60) | |||||
| Week 3: −45 (−303.70, 213.70) | |||||
| Week 4: −60 (− 347.70, 227.70) | |||||
| Week 5: −79 (−361.40, 203.40) | |||||
| Week 6: −57 (− 354.38, 240.40) | |||||
| Week 7: −53 (− 352.70, 246.70) | |||||
| Week 8: −19.00 (− 394.15, 356.15) | |||||
| Difference in gain in length at week 8, mm | 4.40 mm, 30% greater gain (p < 0.03)xxvi | ||||
| Baqui 2002 [27] | ORS with 20 mg zinc per day, 14 days | ORS only | Incidence of diarrhea during 2 year follow up | RR (95% CI) | 0.85 (0.76, 0.96) |
| RD (95% CI)xxvii | 2.9 (0.80, 5.10)xxviii | ||||
| Mortality during 2 year follow up | RR (95% CI) | 0.49 (0.25, 0.94) | |||
| RD (95% CI) | 2.2 (0.60, 3.70)xxix | ||||
| Walker 2007 [53] | ORS with 10 mg zinc, 14 days | ORS with placebo | Difference in weight at week 4 and 8, kg (95% CI) | Week 4: 0.06 (−0.08, 0.20) | |
| Week 8: 0.06 (− 0.08, 0.20) | |||||
| Difference in length at week 4 and 8, cm (95% CI) | Week 4: −0.09 (− 0.61, 0.43) | ||||
| Week 8: −0.12 (− 0.63, 0.39) | |||||
| Proportion of infants with ≥1 episode of any diarrhea (RR [95% CI])xxx | 1.01 (0.92, 1.12) | ||||
| Proportion of infants with ≥2 episode of any diarrhea (RR [95% CI]) | 0.79 (0.67, 0.95)xxxi | ||||
| Proportion of infants with ≥1 episode of dysentery (any day with blood in the stool) (RR [95% CI]) | 2.10 (0.96, 4.61) | ||||
| Incidence of diarrhea (episodes/month) | Intervention group (mean ± SD) | 0.62 ± 0.68 | |||
| Control group (mean ± SD) | 0.61 ± 0.70 | ||||
| Prevalence of diarrhea (days/mo) | Intervention group (mean ± SD) | 2.68 ± 4.11 | |||
| Control group (mean ± SD) | 2.20 ± 3.19 | ||||
| Mortality | RR (95% CI) | 0.99 (0.01, 77.9) | |||
| RD (95% CI)xxxii | −0.18 (−66.42, 66.06) | ||||
| Roy 2007 [28] | Multivitamin with 10 mg zinc per 5 ml, 14 days | Multivitamin only | Difference in mean number of diarrhea episodes during 6 mo follow up (95% CI)xxxiii | − 0.33 (− 0.39, − 0.27) | |
| Percent gain in length at 12 weeks, mmxxxiv | Comparable between groups when all patient were compared (p = 0.6) | ||||
| 24% greater among underweight (WAZ ≤ 70% NCHS median) (p < 0.03) | |||||
| Mortality | RR (95% CI) | 0.84 (0.29,2.37) | |||
| RD (95% CI) | −0.01 (−0.10, 0.07) | ||||
| Roy 2008 [29] | Multivitamin with 20 mg zinc, 14 days | Multivitamin only | Geometric mean diarrhea incidence | Statistically significantly higher in control group (p = 0.03) | |
| Fajolu 2008 [48] | 20 mg zinc for patients > 1 y; 10 mg zinc for patients < 1 y | Placebo | Number of subsequent diarrhea episodes during 2 month follow up | Difference not significant (p = 0.53) | |
| Weight gain at 2 months, g | Higher in intervention group (p < 0.001) | ||||
| Larson 2010 [30] | 10 days therapeutic zinc (20 mg) followed by 3 mo supplementary zinc (10 mg) | 10 days therapeutic zinc (20 mg) followed by 3 mo supplementary zinc placebo | Diarrhea episodes during follow up,xxxv months 1–3 Risk Difference, [95% CI]) | −1.02 (0.26, 1.79) | |
| Diarrhea episodes during follow up, months 4–6 (Risk Difference, [95% CI]) | −0.37 (− 0.35, 1.07) | ||||
| Diarrhea episodes during follow up, months 7–9 (Risk Difference, [95% CI]) | −0.18 (− 0.41, 0.75) | ||||
| Diarrhea episodes during entire 9 month follow up (Risk Difference, [95% CI]) | −0.54 (0.07, 1.01) | ||||
| Alam 2011 [31] | Short course zinc – 20 mg zinc, 5 days | Standard course zinc – 20 mg zinc, 10 days | Difference in mean number of diarrhea episodes during 3 month follow up (95% CI) | 0.06 (− 0.07, 0.19) | |
| Difference in mean number of days of diarrhea during 3 month follow up (95% CI) | 0.2 (−0.35, 0.75) | ||||
| Proportion of children with at least 1 episode of diarrhea during 3 month follow up (RR [95% CI]) | 1.03 (0.95, 1.14) | ||||
| Proportion of children with prolonged diarrhea (≥ 7 days) (Prevalence Ratio [95% CI])xxxvi | 0.63 (0.50, 0.79) | ||||
| Proportion of children with persistent diarrhea (≥ 14 days) (Prevalence Ratio [95% CI]) | 0.63 (0.48, 0.81) | ||||
| Day of onset of first subsequent diarrhea episode during follow up | No difference between groupsxxxvii | ||||
| Patel 2013 [32] | Zinc (2 mg/kg/day) or zinc + copper (Zn 2 mg/kg/day + Cu 0.2 mg/kg/day), 14 days | Placebo | Proportion with at least 1 diarrhea episode during 3 month follow up (Prevalence Ratio [95% CI]) | Zinc group vs placebo | 1.01 (0.76, 1.33) |
| Zinc + Copper group vs placebo | 0.96 (0.72, 1.27) | ||||
| Proportion with at least 2 episodes of diarrhea during 3 month follow upxxxviii (Prevalence Ratio [95% CI]) | Zinc group vs placebo | 2.25 (1.10, 4.63) | |||
| Zinc group vs Zinc + Copper group | 1.12 (0.64, 1.97) | ||||
| Proportion with at least 1 dysentery episode during 3 month follow up (Prevalence Ratio[95% CI]) | Zinc group vs placebo | 1.31 (0.30, 5.77) | |||
| Zinc group vs Zinc + Copper group | 1.37 (0.31, 6.04) | ||||
| Difference in mean number of subsequent diarrhea episodes per child during 3 month follow up (95% CI) | Zinc group vs placebo | 0.08 (−0.05, 0.21) | |||
| Zinc + copper group vs placebo | 0.05 (−0.07, 0.17) | ||||
| Difference in change in WAZ at month 3 (95% CI) | Zinc group vs placebo | −0.1 (− 0.12, 0.10) | |||
| Zinc + copper group vs placebo | 0.06 (−0.04, 0.16) | ||||
| Difference in change in WHZ at month 3 (95% CI) | Zinc group vs placebo | −0.01 (− 0.18, 0.16) | |||
| Zinc + copper group vs placebo | 0.09 (−0.07, 0.25) | ||||
| Difference in change in HAZ at month 3 (95% CI) | Zinc group vs placebo | 0.02 (−0.09, 0.13) | |||
| Zinc + copper group vs placebo | 0.03 (−0.08, 0.14) | ||||
| Negi 2015 [33] | Zinc (20 mg/day) for 14 days | Placebo | Risk of having at least 1 episode of diarrhea during 3 mo follow up (Relative risk [95%]) | Among all subjects | 0.65 (0.37, 1.23) |
| Among zinc-deficient subjects (n = 60) | 0.65 (0.31, 1.38) | ||||
iEstimate may be interpreted as 11 fewer deaths per 100 children in the intervention group compared to the control group
iiQuantitative estimates not presented and reported p-values not specific to time-points of interest
iiiData presented were assumed to be mean ± SD
ivDuration of diets was variable. Diets were started at low concentrations and were advanced every 48 hours if no sign of intolerance. If there were signs of intolerance, diets were maintained or decreased as necessary. When full concentrations were reached, the diet was given for an additional 7 days.
vAppropriate data for calculation of weight gain or difference in weight gain not presented
viDefined as when diarrhea had ceased and patient had consistent weight gain for at least 48 hours
viiAll outcome measurements were compared against measurements at entry, when the child had had diarrhea for 14 days
viiiUnits were assumed to be cm/y due to description of results in the manuscript (rather than (cm/y)2 as presented in the study’s Four)
ixDefined as age- and sex-specific weight standard deviation scores, from the National Center for Health Statistics median value
xNo quantitative estimates given
xiAll diets were equivalent in caloric and protein content
xiiNo estimate or statistical significance given
xiiiNo estimate or statistical significance given
xivNo estimates or statistical significance is given
xvConfidence interval states in manuscript is (0.605, 0.090) which does not contain the relative risk estimate of 0.812 therefore have assumed the 0.090 was a typo and replaced with 1.090.
xviNo estimates or statistical significance given
xviiRR was undefined due to a “0” cell
xviiiThe authors changed the dose after 417 children were enrolled (dosages listed, analyzed as "standard strata" of subjects), and the remaining 273 children received a higher dose of zinc (analyzed as "high dose strata"): Vitamin A (4500 ug retinol equivalent daily for 15 days) and/or zinc acetate (40 mg daily for 15 days)
xixResults from comparison of zinc+vitamin A vs. placebo not reported (reported on zinc effect by combing the zinc alone and zinc+vitamin A group and reported on vitamin A effect by combining vitamin A alone with the zinc+vitamin A group).
xxVitamin A dosage was 100000 IU for children < 1 yo, and 200000 for children > 1 yo
xxiNo SDs or CIs given for differences. P-value for the difference between zinc group and control is 0.045; for the difference between vitamin A group and control is 0.207; and for the difference between zinc + vitamin A group is 0.074.
xxiiDuration of intervention is unclear
xxiiiData were presented but were not interpretable due to an ambiguous or incorrect title
xxivAssessed by proportion of patients with delayed recovery, with recovery defined as the passage of formed stool followed by 2 days without diarrhea
xxvFor this and all outcomes, data were not labeled. Data presented were assumed to be mean and SD based on labeled data on another figure in the paper
xxviNo SDs or CIs given. P< 0.05.
xxviiDifference in mean diarrhea incidence rates. Estimate may be interpreted as 2.9 more episodes per 100 child-years of observation were experienced in the control group compared to the intervention group
xxviiiCalculated values of lower and upper limits of 95% CI differed from what was represented in original publication
xxixDifference in mean mortality rates. Estimate may be interpreted as 2.2 more deaths per 1000 child years of observation experienced by the control group compared to the intervention group
xxxAll data presented are unadjusted. The authors’ results are discrepant from this table’s results, as authors adjust for original diarrhea episode lasting > 7 days, exclusive breastfeeding upon enrollment, and WLZ at beginning of follow up
xxxiCalculated values of lower and upper limits of 95% CI use data presented on unadjusted proportions and differed from what was represented in original publication
xxxiiEstimate may be interpreted as 0.18 deaths fewer in intervention group per 100,000 child-weeks of observation compared to control group
xxxiiiData presented was assumed to be mean ± SD
xxxivQuantitative estimates not presented
xxxvRisk differences may be interpreted as excess number of acute diarrhea episodes per child-year attributed to lack of zinc supplementation
xxxviThe authors reported "The proportion of prolonged (>=7 d) and persistent diarrhea episodes (>=14 d) did not vary between the 5-d (19 vs. 16%; P 0.08) and 10-d (12 vs. 10%; P = 0.14) groups" which suggests the p-values correspond to the comparison of persistent and prolonged among children treated with 5-days and among children treated with 10-days. We have instead assumed the appropriate comparisons are proportion of prolonged (19% vs. 12%, p-value=0.0001) and persistent (16% vs. 10%, p-value=0.0004) which would result in statistically significant differences (unlike what was reported).
xxxviiNo estimates or statistical significance given
xxxviiiEstimates calculated for relative risk of at least 1, 2, or dysenteric diarrhea episodes are discrepant from published results
Growth
Studies reported impact on growth in several different ways:
Height/Length, HAZ//LAZ
Ten studies presented data related to length or height, with follow-up time ranging from 21 days to 9 months and none reported sample size calculations/being powered for these outcomes (Table 1). Five trials evaluated a high protein diet, 4 therapeutic zinc and 1 probiotic. Of 4 studies that reported difference in change in (∆) HAZ/LAZ between intervention groups, 1 high protein diet trial reported a 0.9 z-score greater gain in HAZ/LAZ in the intervention group after 3 weeks of follow-up (95% CI: 0.05, 0.13), [11] but 2 high protein diet trials (with 3 and 29 weeks of follow-up) and a large zinc with 12 weeks of follow-up trial found no significant benefit (Fig. 3a) [10, 13, 32]. Four studies presented data on ∆ absolute height at follow-up, 2 of which were trials of high protein diets with follow-up times of 3 and 29 weeks. Of the 2 high protein diet trials, the trial with 29 weeks of follow-up found a benefit in height change (Fig. 3b) – a 1.10 cm greater change in height compared to the control groups (95% CI: 0.56, 1.64) [10, 13]. Of the other 2 studies evaluating height attainment, a trial of a high protein diet with micronutrients with 36 weeks of follow-up, and another of therapeutic zinc with 8 weeks of follow-up, only the former showed benefit (a greater gain in height of 0.65 cm in the intervention group [95% CI: 0.11, 1.19]) [43, 53]. Percent ∆length was evaluated in 2 therapeutic zinc studies, both of which found a significantly greater length gain among children treated with zinc, but this result was only among underweight children in 1 of the trials [25, 28]. Among 2 studies evaluating prevalence of stunting during follow-up, 1 found that the group treated with probiotics (L. rhamnosus GG) had higher stunting prevalence at 4 weeks of follow-up [54] and a high protein diet trial reported no significant difference at 26 weeks [44].
MUAC
Fig. 3.

a Effect of diarrhea management interventions on change in HAZ/LAZ (difference in change in HAZ/LAZ and 95% confidence interval). b Effect of diarrhea management interventions on change in height (difference in change in height (cm) and 95% confidence interval)
Four studies reported MUAC data during follow-up periods ranging from 15 to 28 days, 2 were high protein studies, 1 was a trial of therapeutic zinc, and 2 trials of RUTF/micronutrient (which assessed MUAC as 1 of the indicators of acute malnutrition). One of the high protein diet studies reported that children in the intervention group gained 0.44 cm more in MUAC on average compared to children given a standard protein diet (95% CI: 0.08, 0.80) [10]. However, neither the remaining high protein diet study nor the zinc trial reported a significant difference in MUAC during follow-up [9, 50]. None of the studies provided sample size estimates making it unclear whether they were adequately powered to detect differences in MUAC. Both trials of RUTF and micronutrient powder reported the incidence of acute malnutrition (WHZ < 2, MUAC < 115 mm, or oedema) to be similar across all combinations of groups (RUTF vs controls; micronutrients vs. controls, and RUTF vs. micronutrients) in the subgroup of children from both trials who had diarrhea at enrollment [45, 46].
WHZ, WAZ, or absolute weight
Thirty-two trials (74.4%) with follow-up periods ranging from 7 days to 29 weeks, reported data on weight, WAZ, or WHZ. Of these, 9 assessed a high protein diet, 7 assessed therapeutic zinc (including 1 which also assessed vitamin A), and 5 tested lactose-free diets. Four were trials of ORS formulations, 3 of probiotics, and 1 each of semi-elemental diet, glutamine, and dietary fiber. Of the 4 trials evaluating differences in ∆WAZ between study groups, 3 high protein and 1 therapeutic zinc trials, 2 (both high protein) reported a statistically significant improvement (ranging from 0.23 [11] to 0.3 z-scores [10]) compared to a standard diet (Fig. 4a) although none were explicitly powered for this outcome. The same 2 diet trials also reported a significant benefit in WHZ, with high protein groups gaining 0.25 [31] to 0.4 units [11] more in WHZ than the standard diet group (Fig. 4b) whereas the 2 zinc trials assessing ∆WHZ, 1 of which was explicitly powered to address WHZ, found no difference [32, 53]. Two additional trials assessed WHZ although did not present quantitative results for calculation of effect size and 95% confidence intervals; A probiotics trial concluded there was no difference in ∆WHZ at 6 weeks between the treated and untreated groups, [19] while a high protein diet trial reported a greater median ∆WAZ in children given high protein diets at 26 weeks of follow-up [44].
Fig. 4.

a Effect of diarrhea management interventions on change in WAZ (difference in change in WAZ and 95% confidence interval). b Effect of diarrhea management interventions on change in WHZ/WLZ (difference in change in WHZ/WLZ and 95% confidence interval). c Effect of diarrhea management interventions on weight gain (difference in weight gain [g] and 95% confidence interval). d Effect of diarrhea management interventions on weight at follow up (difference in weight [kg] and 95% confidence interval)
Twenty-two studies presented data on absolute weight gain (Fig. 4c) or weight at follow-up: 6 high protein diet trials, 6 zinc (1 of which also assessed vitamin A), 4 lactose free diets, 2 ORS, and 1 each of a probiotic, semi-elemental diet, dietary fiber, and glutamine. Three of the 6 high protein trials found a statistically significant improvement in weight associated with the intervention group, [10, 43, 44] as did 3 of the 6 zinc trials, [22, 25, 48] 1 of which also assessed vitamin A which did not appear to have a weight benefit [22]. Two of the 4 lactose-free diets [16, 50] and 1 of 2 ORS trials demonstrated a significant benefit in weight [39]. This trial found a greater percent improvement in weight 14 days after presentation in the groups of children treated with ORS (90 mmol/l or 50 mmol/l of sodium) vs. no ORS but did not find a statistically significant difference when measured as absolute difference in weight. Weight gain was significantly improved in the trial of a semi-elemental diet [35] and the single trial of glutamine found intervention children to have 130 g more weight gain than the placebo group at follow-up day 30, but not at days 60 or 90 of follow-up [51]. The single dietary fiber and probiotic trials evaluating weight gain did not find a significant effect [26, 47].
Recurrent or prolonged diarrhea at follow-up
Twenty studies (45.7% of total) reported on diarrhea frequencies during follow-up periods ranging from 7 days to 3 months. The majority were trials of therapeutic zinc (13), including 2 that also assessed vitamin A, followed by probiotic trials (3), ORS formulation (3 comparisons in 2 trials) and 1 diet fiber and 1 lactose-free diet. Only 4 of the trials explicitly described being powered to address diarrhea prevalence or incidence during follow-up [22, 27, 31, 53]. Figure 5 shows the 12 trials (providing 15 estimates due to 3 trials including 3 arms) that reported data on prevalence of diarrhea 7 days or more after presentation (8 zinc [2 of which also assessed vitamin A], 2 ORS (1 of which compared 3 formulations), and 2 probiotic). Only 2 zinc studies [22, 31] and 1 probiotic (Saccharomyces boulardii) trial found a reduction in diarrhea prevalence associated with the intervention [41]. The other 6 zinc trials [23, 24, 32–34, 53] and probiotic trial of Lactobacillus rhamnosus GG [54] did not find a significant effect on diarrhea prevalence during follow-up. The lactose-free diet reported no effect on the presence of diarrhea at day 12 (p = 0.76) but did not report specific prevalences [17]. The 2 trials assessing ORS formulations (providing 3 estimates) did not demonstrate a benefit [34, 55] nor did the 2 vitamin A trials [22, 34].
Fig. 5.
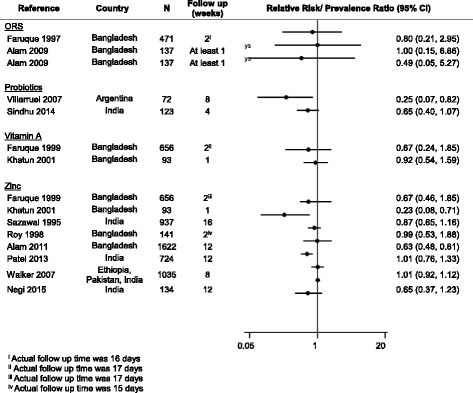
Effect of diarrhea management interventions on diarrhea morbidity during follow up (relative risk or prevalence ratio of diarrhea at specified time during follow up [95% CI])
Of studies reporting on diarrhea frequency indicators other than prevalence of diarrhea at follow-up, findings were heterogeneous. One study found that children given a rice-based diet with green banana or pectin (dietary fiber) were more likely to have recovered from diarrhea by day 5 of follow-up, while most children given the rice-based diet alone continued to have diarrhea until day 10 of follow-up [15]. Another found no children treated with Lactobacillus reuteri 17938 to have diarrhea beyond 7-days whereas 17.4% of children without probiotic treatment did have prolonged diarrhea [52]. A trial of 8070 community-based children found that those given zinc with ORS had 2.9 fewer episodes of diarrhea per 100 child-years (95%CI: 0.8, 5.1) than those given ORS alone [27]. A study contrasting 10 day therapeutic zinc (20 mg/day) with 3 months of supplemental zinc (10 mg/day) to the therapeutic zinc course alone found that the long term zinc reduced diarrhea incidence over a 9 month period by 21% (2.05 vs.2.59 episodes / child years) [30]. Compared to children given the multivitamin alone, children given a multivitamin with zinc had an average of 0.33 fewer subsequent diarrhea episodes (95% CI: -0.39, − 0.27) and diarrhea incidence was similarly reduced in the 6 month follow-up period [28, 29]. Conversely, a placebo-controlled trial of therapeutic zinc among 1042 children reported no difference in the mean number of subsequent diarrhea episodes during a 3 month follow-up period nor did 2 smaller zinc trials [29, 32, 48].
Discussion
While significant progress has been made over the past 25 years in reducing deaths attributed to diarrhea, there is increasing recognition that diarrhea is associated with mortality, subsequent morbidities, and malnutrition in the period after a diarrheal episode [56, 57]. These post-acute sequelae highlight the need, and opportunity, to identify interventions to reduce morbidity and mortality among children presenting with diarrhea. This systematic review appraised diarrhea intervention trials for evidence of effects on post-acute sequelae of diarrhea, including mortality, nutritional status, and diarrhea presence during an extended follow-up period.
We found very few trials that evaluated post-acute diarrheal mortality, and only 1 (of zinc) was explicitly powered to address mortality and found mortality benefit [27]. The other zinc trials did not report a mortality benefit. As summarized in a recent Cochrane review, zinc appears to reduce diarrhea duration, particularly in malnourished children, although the degree to which this effect translates to mortality benefit remains unknown [58]. Therapeutic zinc also appears to have limited to no efficacy on morbidity or growth in children under 6 months of age [53, 59].
Post-acute mortality was assessed in 2 trials of antibiotics that found no mortality benefit, yet were underpowered to do so. Both trials included less than 100 children and only 1 was placebo-controlled. The role of antibiotics in diarrhea management remains controversial. In the absence of diagnostics, diarrhea management guidelines recommend antibiotics only for dysentery or suspected cholera [60, 61]. Limiting antibiotics to these 2 indications may miss other serious enteric infections amenable to antibiotics [62, 63]. In practice however, many children without these indications are treated with an antibiotic, the benefits of which are not well understood [64]. Large placebo-controlled clinical trials are needed to determine the potential harm and/or benefit of antibiotics to reduce post-acute diarrhea morbidity and mortality.
Over 30 trials reported on growth outcomes. Dietary supplementation with macro- or micro-nutrients, high protein and lactose-free diets, and probiotics were assessed for effects on growth with mixed results. We found substantial variability in how growth outcomes were evaluated, making comparisons between studies challenging. Two of the 5 trials of dietary interventions found beneficial impacts on WAZ/WHZ with a high protein isocaloric diet. In a single study, glutamine demonstrated a signal of benefit at 1 time point which was not sustained. Most trials that assessed weight reported no intervention effect; perhaps because weight gain restored through hydration during the acute phase of diarrhea overshadowed weight gain from trialed interventions. High protein diets, either alone or in combination with micronutrients such as zinc, had a modest impact on short to medium term linear growth (3 weeks to 9 months). However, this effect was inconsistently demonstrated. High protein diets may restore the protein loss that can occur during and immediately after infection [65, 66]. Replacing protein may modify growth consequences of diarrhea by increasing protein availability or by influencing hormonal regulation [67–69]. The combination of high protein and zinc may restore integrity of damaged mucosal surfaces and improve nutrient absorption [70–72]. However evidence around the effect of zinc on markers of intestinal permeability, as measured by the lactulose to mannitol ratio, are inconsistent [49, 73, 74]. Specific amino acids may also be important; glutamine has been shown to protect against bacterial translocation through maintenance of the gut barrier in animal models [75–77].
Diarrhea during follow-up was the most commonly reported outcome assessed in this review. Numerous systematic reviews of therapeutic zinc on diarrheal outcomes have been conducted, all of which suggest some benefit [58, 78–80]. The effects of zinc on diarrhea at a specified day of follow-up were recently summarized in a Cochrane review and pooled relative risks of diarrhea at day 3, day 5, and day 7 associated with zinc all showed a statistically significant benefit [58]. Our review included diarrhea assessed at 7 days and beyond (7 days to 4 months) and found inconsistent results, perhaps demonstrating a waning in effect or sub-optimal statistical power at longer follow-up time points. Given therapeutic zinc is recommended for 14 days in current WHO management guidelines yet the data on benefit seems most pronounced within the first 7 days, days 7–14 of the currently recommended zinc course may need further evaluation.
Three of the 4 probiotic trials evaluating diarrhea outcomes demonstrated a benefit on diarrhea during follow-up (Saccharomyces boulardii, Lactobacillus reuteri 17938 and 1 of the 2 Lactobacillus rhamnosus GG trials). However the Lactobacillus rhamnosus GG trial that did not find a benefit in diarrhea during follow-up did report improvements in intestinal function (as measured by the lactulose to mannitol test) and higher immunoglobulin G (IgG) in the subgroup of children with rotavirus infection treated with the probiotic [54]. Most clinical trials of probiotics have been conducted in high-resource settings and have treated and followed children for less than 7 days [81, 82]. Although not included in this review because it was published after the search was conducted, a recent pilot study (n=76) conducted in Botswana found a greater increase in HAZ and reduced diarrhea recurrence over 60-days of follow-up among admitted children with diarrhea randomized to Lactobacillus reuteri 17938, [62]. The European Society for Pediatric Gastroenterology recently recommended probiotics, specifically Saccharomyces boulardii or Lactobacillus rhamnosus GG, to reduce the duration and intensity of gastroenteritis [83]. The mechanisms by which probiotics may decrease diarrheal symptoms are largely unknown, but may act by out-competing pathogenic enteric infections for nutrients, restoring gut barrier functions, and/or by restoring gut microbial balance.
This review had several limitations. Most trials, particularly trials used to evaluate mortality, were underpowered. A 2-armed clinical trial powered to detect a 50% reduction in a 3-month diarrheal case fatality rate of 2% would require over 4000 participants, a sample size far larger than most trials reporting mortality outcomes in this review and far smaller than sample sizes required to detect smaller intervention effects or lower case fatality rates. Many trials were excluded because of short length of follow-up and included trials had follow-up times ranging from 7-days to 9 months which could explain heterogeneity between studies, particularly studies of growth outcomes. Some interventions were more represented than others based on available clinical trial data. Markers of enteric function were not included in this review as pre-specified outcomes, despite a growing body of evidence suggesting that enteric dysfunction is linked to poor outcomes following acute illness [84]. Because of the heterogeneity in interventions, outcome measurements, and follow-up time, we did not calculate pooled measures of effect. For the same reason, we did not report a GRADE score for every individual result but rather for overall study quality, and most trials were graded as low or very low. Standardized measures of the nutritional consequences of diarrhea and diarrhea morbidity will be important to enable future meta-analyses. This review includes data from a wide range of geographic, demographic and epidemiologic settings. However, most included trials were conducted in Asia, with less than 15% of all included trials conducted in sub-Saharan Africa (SSA). Diarrhea-mortality rates are higher in SSA than in South Asia and recent projections of childhood mortality into 2030 predict that SSA will contribute to 60% of all childhood deaths [5, 57]. Host characteristics, such as nutritional status and HIV-infection/−exposure vary greatly between these regions making generalizability of intervention effect challenging [85–87].
Conclusions
In many resource-limited settings, diarrheal episodes in young children are frequent and are associated with increased risk of mortality as well as growth failure and risk of subsequent infections. The mechanisms by which diarrhea and underlying enteric infections lead to morbidity, malnutrition, and mortality are multifactorial, likely requiring multiple complementary interventions to reduce likelihood of recurrence or persistence, promote healing of the gut mucosa, and to replenish lost protein and nutrients. Well-designed, multi-factorial, clinical trials evaluating the extended impact of diarrhea management interventions are urgently needed to reduce the long-term risks associated with diarrhea.
Acknowledgements
We would like to thank the Global Center for Integrated Health of Women, Adolescents, and Children, the Kenya Research and Training Center, and the Center for AIDS Research Enterics Working group for their support during the preparation of this article.
Funding
Funding was provided by the Bill and Melinda Gates Foundation (OPP1132140) and the UW Global Center for Integrated Health of Women, Adolescents and Children (Global WACh). JLW and DMD are supported by the Childhood Acute Illness and Nutrition Network (CHAIN, OPP1131320). GJS is supported by a National Institute of Health mentoring award (grant number K24- HD054314) and PBP and GJS are supported by the International Core of the University of Washington Center for AIDS Research (CFAR; Seattle, WA, USA), an NIH funded program (P30 AI027757). The funders had no role in the study design, data abstraction, data interpretation, or writing of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CI
Confidence Interval
- GRADE
Grading of Recommendations Assessment Development and Evaluation
- HAZ
Height-for-age z-score
- LAZ
Length-for-age z-score
- LMICs
Low- and middle-income countries
- MSD
Moderate-to-severe diarrhea
- MUAC
Mid upper arm circumference
- PR
Prevalence Ratio
- RCT
Randomized controlled trial
- RR
Relative Risk
- RUTF
Ready-to-use therapeutic foods
- WAZ
Weight-for-age z-score
- WHZ
Weight-for-height z-score
- WLZ
Weight-for-length z-score
Additional file
Supplement. (DOCX 129 kb)
Authors’ contributions
PBP, JLW, DMD, and GJS conceived of the idea and developed the protocol for this review. All titles and abstracts were screened by PBP and HEA, RLB and HEA reviewed all abstracts and full text articles with final input from PBP. RLB and HEA abstracted data from, and conducted GRADE assessments of, included studies. All authors contributed to the development, reading, and approving the final version for publication.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s12889-018-5092-7) contains supplementary material, which is available to authorized users.
Contributor Information
Patricia B. Pavlinac, Email: ppav@uw.edu
Rebecca L. Brander, Email: rbrander@uw.edu
Hannah E. Atlas, Email: hatlas@uw.edu
Grace C. John-Stewart, Email: gjohn@uw.edu
Donna M. Denno, Email: ddenno@uw.edu
Judd L. Walson, Email: walson@uw.edu
References
- 1.Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the sustainable development goals. Lancet. 2016;388(10063):3027–3035. doi: 10.1016/S0140-6736(16)31593-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kotloff KL, Nataro JP, Blackwelder WC, Nasrin D, Farag TH, Panchalingam S, Wu Y, Sow SO, Sur D, Breiman RF, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the global enteric multicenter study, GEMS): a prospective, case-control study. Lancet. 2013;382:209–222. doi: 10.1016/S0140-6736(13)60844-2. [DOI] [PubMed] [Google Scholar]
- 3.Rahman AE, Molla M, Worku A, Hurt L, Kirkwood B, Mohan B, Bhutta Z, Raza F, Mrema S. Childhood diarrhoeal deaths in seven low- and middle-income countries. Bull World Health Organ. 2014;92:664–671. doi: 10.2471/BLT.13.134809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Checkley W, Buckley G, Gilman RH, Assis AM, Guerrant RL, Morris SS, Mølbak K, Valentiner-Branth P, Lanata CF, Black RE. Multi-country analysis of the effects of diarrhoea on childhood stunting. Int J Epidemiol. 2008;37:816–830. doi: 10.1093/ije/dyn099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liu L, Johnson H, Cousens S. Global, regional, and national causes of child mortality in 2000-2010: an updated systematic analysis. Lancet. 2015;385:430–440. doi: 10.1016/S0140-6736(14)61698-6. [DOI] [PubMed] [Google Scholar]
- 6.Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. doi: 10.1016/S0140-6736(13)60937-X. [DOI] [PubMed] [Google Scholar]
- 7.World Bank Group. Low & Middle Income Countries. World Bank. 2016. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- 8.Gilman R, Koster F, Islam S, McLaughlin J, Rahaman M. High- and low-dose Ampicillin therapy for treatment of severe dysentery due to Shigella dysenteriae type 1. Antimicrob Agents Chemother. 1980;17:402–405. doi: 10.1128/AAC.17.3.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Datta D, Datta P, Bhattacharya SK, Mitra U, Bhattacharya MK, Sen D, Sinha AK, Manna B, Mitra AK, Lahiri M, et al. Effect of protein rich diet during acute phase of dysentery. Indian J Public Health. 1990;34:1–5. [PubMed] [Google Scholar]
- 10.Kabir I, Butler T, Underwood LE, Rahman MM. Effects of a protein-rich diet during convalescence from shigellosis on catch-up growth, serum proteins, and insulin-like growth factor-I. Pediatr Res. 1992;32:689–692. doi: 10.1203/00006450-199212000-00014. [DOI] [PubMed] [Google Scholar]
- 11.Kabir I, Malek M, Mazumder RN, Rahman M, Mahalanabis D. Rapid during growth of children fed a high-protein convalescence from shigellosis13. Am J Clin Nutr. 1993;57:441–445. doi: 10.1093/ajcn/57.3.441. [DOI] [PubMed] [Google Scholar]
- 12.Mazumder RN, Hoque SS, Ashraf H, Kabir I, Wahed MA. Early feeding of an energy dense diet during acute shigellosis enhances growth in malnourished children. J Nutr. 1997;127:51–54. doi: 10.1093/jn/127.1.51. [DOI] [PubMed] [Google Scholar]
- 13.Kabir I, Rahman MM, Haider R, Mazumder RN, Khaled MA, Mahalanabis D. Increased height gain of children fed a high-protein diet during convalescence from shigellosis: a six-month follow-up study. J Nutr. 1998;128:1688–1691. doi: 10.1093/jn/128.10.1688. [DOI] [PubMed] [Google Scholar]
- 14.Mazumder RN, Ashraf H, Hoque SS, Kabir I, Majid N, Wahed MA, Fuchs GJ, Mahalanabis D: Effect of an energy-dense diet on the clinical course of acute shigellosis in undernourished children. Br J Nutr 2000, 84:775-779. [PubMed]
- 15.Rabbani GH, Teka T, Zaman B, Majid N, Khatun M, Fuchs GJ. Clinical studies in persistent diarrhea: dietary management with green banana or pectin in Bangladeshi children. Gastroenterology. 2001;121:554–560. doi: 10.1053/gast.2001.27178. [DOI] [PubMed] [Google Scholar]
- 16.Bhan MK, Arora NK, Khoshoo PR, Bhatnagar S, Sazawal S, Sharma K. Comparison of a lactose-free cereal-based formula and cow's milk in infants and children with acute gastroenteritis. J Pediatr Gastroenterol Nutr. 1988;7:208–213. doi: 10.1097/00005176-198803000-00009. [DOI] [PubMed] [Google Scholar]
- 17.Bhatnagar S, Bhan M, Singh K, Saxena S, Shariff M. Efficacy of milk-based diets in persistent diarrhea- a randomized, controlled trial. Pediatrics. 1996;98 [PubMed]
- 18.Alam NH, Islam S, Sattar S, Monira S, Desjeux J-F. Safety of rapid intravenous rehydration and comparative efficacy of 3 oral rehydration solutions in the treatment of severely malnourished children with dehydrating cholera. J Pediatr Gastroenterol Nutr. 2009;48:318–327. doi: 10.1097/MPG.0b013e318180af27. [DOI] [PubMed] [Google Scholar]
- 19.Misra S, Sabui T, Pal N. A randomized controlled trial to evaluate the efficacy of lactobacillus GG in infantile diarrhea. J Pediatr. 2009;155:129–132. doi: 10.1016/j.jpeds.2009.01.060. [DOI] [PubMed] [Google Scholar]
- 20.Sindhu KN, Sowmyanarayanan TV, Paul A, Babji S, Ajjampur SS, Priyadarshini S, Sarkar R, Balasubramanian KA, Wanke CA, Ward HD, et al. Immune response and intestinal permeability in children with acute gastroenteritis treated with lactobacillus rhamnosus GG: a randomized, double-blind, placebo-controlled trial. Clin Infect Dis. 2014;58(8):1107–1115. doi: 10.1093/cid/ciu065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Faruque AS, Hoque SS, Fuchs GJ, Mahalanabis D. Randomized, controlled, clinical trial of rice versus glucose oral rehydration solutions in infants and young children with acute watery diarrhoea. Acta Paediatr. 1997;86:1308–1311. doi: 10.1111/j.1651-2227.1997.tb14903.x. [DOI] [PubMed] [Google Scholar]
- 22.Khatun UH, Malek MA, Black RE, Sarkar NR, Wahed MA, Fuchs G, Roy SK. A randomized controlled clinical trial of zinc, vitamin a or both in undernourished children with persistent diarrhea in Bangladesh. Acta Paediatr. 2001;90:376–380. doi: 10.1080/080352501750126159. [DOI] [PubMed] [Google Scholar]
- 23.Sazawal S, Black RE, Bhan MK, Bhandari N, Sinha A, Jalla S. Zinc supplementation in young children with acute diarrhea in India. N Engl J Med. 1995;333:839–844. doi: 10.1056/NEJM199509283331304. [DOI] [PubMed] [Google Scholar]
- 24.Roy SK, Tomkins AM, Mahalanabis D, Akramuzzaman SM, Haider R, Behrens RH, Fuchs G. Impact of zinc supplementation on persistent diarrhoea in malnourished Bangladeshi children. Acta Paediatr. 1998;87:1235–1239. doi: 10.1111/j.1651-2227.1998.tb00943.x. [DOI] [PubMed] [Google Scholar]
- 25.Roy SK, Behrens RH, Haider R, Akramuzzaman SM, Mahalanabis D, Wahed MA, Tomkins AM. Impact of zinc supplementation on intestinal permeability in Bangladeshi children with acute diarrhoea and persistent diarrhoea syndrome. J Pediatr Gastroenterol Nutr. 1999;15:289–296. doi: 10.1097/00005176-199210000-00010. [DOI] [PubMed] [Google Scholar]
- 26.Alam NH, Meier R, Schneider H, Sarker SA, Bardhan PK, Mahalanabis D, Fuchs GJ, Gyr N. Partially hydrolyzed guar gum-supplemented oral rehydration solution in the treatment of acute diarrhea in children. J Pediatr Gastroenterol Nutr. 2000;31:503–507. doi: 10.1097/00005176-200011000-00010. [DOI] [PubMed] [Google Scholar]
- 27.Baqui AH, Black RE, El Arifeen S, Yunus M, Chakraborty J, Ahmed S, Vaughan JP. Effect of zinc supplementation started during diarrhoea on morbidity and mortality in Bangladeshi children: community randomised trial. BMJ. 2002;325(7372):1059. doi: 10.1136/bmj.325.7372.1059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Roy SK, Tomkins AM, Haider R, Behren RH, Akramuzzaman SM, Mahalanabis D, Fuchs GJ. Impact of zinc supplementation on subsequent growth and morbidity in Bangladeshi children with acute diarrhoea. Eur J Clin Nutr. 2007;53:529–534. doi: 10.1038/sj.ejcn.1600734. [DOI] [PubMed] [Google Scholar]
- 29.Roy SK, Raqib R, Khatun W, Azim T, Chowdhury R, Fuchs GJ, Sack DA. Zinc supplementation in the management of shigellosis in malnourished children in Bangladesh. Eur J Clin Nutr. 2008;62:849–855. doi: 10.1038/sj.ejcn.1602795. [DOI] [PubMed] [Google Scholar]
- 30.Larson CP, Nasrin D, Saha A, Chowdhury MI, Qadri F. The added benefit of zinc supplementation after zinc treatment of acute childhood diarrhoea: a randomized, double-blind field trial. Trop Med Int Health. 2010;15:754–761. doi: 10.1111/j.1365-3156.2010.02525.x. [DOI] [PubMed] [Google Scholar]
- 31.Alam DS, Yunus M, El Arifeen S, Chowdury HR, Larson CP, Sack DA, Baqui AH, Black RE. Zinc treatment for 5 or 10 days is equally efficacious in preventing diarrhea in the subsequent 3 months among Bangladeshi children. J Nutr. 2011;141:312–315. doi: 10.3945/jn.110.120857. [DOI] [PubMed] [Google Scholar]
- 32.Patel AB, Dibley MJ, Mamtani M, Badhoniya N, Kulkarni H. Therapeutic zinc and copper supplementation in acute diarrhea does not influence short-term morbidity and growth: double-blind randomized controlled trial. Pediatr Infect Dis J. 2013;32(1):91–93. doi: 10.1097/INF.0b013e31826fb32d. [DOI] [PubMed] [Google Scholar]
- 33.Negi R, Dewan P, Shah D, Das S, Bhatnagar S, Gupta P. Oral zinc supplements are ineffective for treating acute dehydrating diarrhoea in 5-12-year-olds. Acta Paediatr. 2015;104(8):e367–e371. doi: 10.1111/apa.12645. [DOI] [PubMed] [Google Scholar]
- 34.Faruque AS, Mahalanabis D, Haque SS, Fuchs GJ, Habte D. Double-blind, randomized, controlled trial of zinc or vitamin A supplementation in young children with acute diarrhoea. Acta Paediatr. 1999;88:154–160. doi: 10.1111/j.1651-2227.1999.tb01074.x. [DOI] [PubMed] [Google Scholar]
- 35.Eichenberger JR, Hadorn B, Schmidt B. A semi-elemental diet with low osmolarity and high content of hydrolyzed lactalbumin in the treatment of acute diarrhea in malnourished children. Arq Gastroenterol. 1984;21:130–135. [PubMed] [Google Scholar]
- 36.Nurko S, García-Aranda JA, Fishbein E, Pérez-Zúñiga MI. Successful use of a chicken-based diet for the treatment of severely malnourished children with persistent diarrhea: a prospective, randomized study. J Pediatr. 1997;131:405–412. doi: 10.1016/S0022-3476(97)80066-2. [DOI] [PubMed] [Google Scholar]
- 37.de Mattos Â, Ribeiro T, Mendes P, Valois S, Mendes C, Ribeiro H. Comparison of yogurt, soybean, casein, and amino acid-based diets in children with persistent diarrhea. Nutr Res. 2009;29:462–469. doi: 10.1016/j.nutres.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 38.Lozano J, Cespedes J. Lactose vs lactose free regimen in children with acute diarrhoae: a randomized controlled trial. Arch Latinoam Nutr. 1994;44 [PubMed]
- 39.Santosham M, Carrera E, Sack RB. Oral rehydration therapy in well nourished ambulatory children. Am J Trop Med Hyg. 1983;32:804–808. doi: 10.4269/ajtmh.1983.32.804. [DOI] [PubMed] [Google Scholar]
- 40.Ribeiro HCJ, Lifshitz F. Alanine-based oral rehydration therapy for infants with acute diarrhea. Pediatrics. 1991;118:S86–S90. doi: 10.1016/S0022-3476(05)81432-5. [DOI] [PubMed] [Google Scholar]
- 41.Villarruel G, Rubio DM, Lopez F, Cintioni J, Gurevech R, Romero G, Vandenplas Y. Saccharomyces boulardii in acute childhood diarrhoea: a randomized, placebo-controlled study. Acta Paediatr. 2007;96:538–541. doi: 10.1111/j.1651-2227.2007.00191.x. [DOI] [PubMed] [Google Scholar]
- 42.Amadi B, Mwiya M, Musuku J, Watuka A, Sianongo S, Ayoub A, Kelly P. Effect of nitazoxanide on morbidity and mortality in Zambian children with cryptosporidiosis: a randomised controlled trial. Lancet. 2002;360:1375–1380. doi: 10.1016/S0140-6736(02)11401-2. [DOI] [PubMed] [Google Scholar]
- 43.Valentiner-Branth P, Steinsland H, Santos G, Perch M, Begtrup K, Bhan MK, Dias F, Aaby P, Sommerfelt H, Mølbak K. Community-based controlled trial of dietary management of children with persistent diarrhea: sustained beneficial effect on ponderal and linear growth. Am J Clin Nutr. 2001;73:968–974. doi: 10.1093/ajcn/73.5.968. [DOI] [PubMed] [Google Scholar]
- 44.Rollins NC, Van Den Broeck J, Kindra G, Pent M, Kasambira T, Bennish ML. The effect of nutritional support on weight gain of HIV-infected children with prolonged diarrhoea. Acta Paediatr. 2007;96:62–68. doi: 10.1111/j.1651-2227.2006.00013.x. [DOI] [PubMed] [Google Scholar]
- 45.van der Kam S, Roll S, Swarthout T, Edyegu-Otelu G, Matsumoto A, Kasujja FX, Casademont C, Shanks L, Salse-Ubach N. Effect of short-term supplementation with ready-to-use therapeutic food or micronutrients for children after illness for prevention of malnutrition: a randomised controlled trial in Uganda. PLoS Med. 2016;13(2):e1001951. doi: 10.1371/journal.pmed.1001951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.van der Kam S, Salse-Ubach N, Roll S, Swarthout T, Gayton-Toyoshima S, Jiya NM, Matsumoto A, Shanks L. Effect of short-term supplementation with ready-to-use therapeutic food or micronutrients for children after illness for prevention of malnutrition: a randomised controlled trial in Nigeria. PLoS Med. 2016;13(2):e1001952. doi: 10.1371/journal.pmed.1001952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Boudraa G, Benbouabdellah M, Hachelaf W, Boisset M, Desjeux JF, Touhami M. Effect of feeding yogurt versus milk in children with acute diarrhea and carbohydrate malabsorption. J Pediatr Gastroenterol Nutr. 2001;33(3):307–313. doi: 10.1097/00005176-200109000-00015. [DOI] [PubMed] [Google Scholar]
- 48.Fajolu I, Emokpae A, Oduwole A, Silva B, Abidoye R, Renner J. Zinc supplementation in children with acute diarrhoea. Nig. Q. J. Hosp. Med. 2008;18:101–103. doi: 10.4314/nqjhm.v18i2.44997. [DOI] [PubMed] [Google Scholar]
- 49.Bhutta Z, Nizami SQ, Isani Z. Zinc supplementation in malnourished children with persistent diarrhea in Pakistan. Pediatrics. 1999;103 [DOI] [PubMed]
- 50.Bhutta Z, Molla A, Badruddin S. Dietary management of persistent diarrhea- comparison of a traditional rice-lentil based diet with soy formula. Pediatrics. 1991;88:1010–1018. [PubMed] [Google Scholar]
- 51.Yalçin SS, Yurdakök K, Tezcan I, Oner L. Effect of glutamine supplementation on diarrhea, interleukin-8 and secretory immunoglobulin a in children with acute diarrhea. J Pediatr Gastroenterol Nutr. 2004;38:494–501. doi: 10.1097/00005176-200405000-00007. [DOI] [PubMed] [Google Scholar]
- 52.Dinleyici EC, Vandenplas Y. Lactobacillus reuteri DSM 17938 effectively reduces the duration of acute diarrhoea in hospitalised children. Acta Paediatr. 2014;103:300–305. doi: 10.1111/apa.12515. [DOI] [PubMed] [Google Scholar]
- 53.Walker CL, Bhutta ZA, Bhandari N, Teka T, Shahid F, Taneja S, Black RE, Rasool S, Nizami SQ, Rongsen T, et al. Zinc during and in convalescence from diarrhea has no demonstrable effect on subsequent morbidity and anthropometric status among infants <6 mo of age. Am J Clin Nutr. 2007;85:887–894. doi: 10.1093/ajcn/85.3.887. [DOI] [PubMed] [Google Scholar]
- 54.Sindhu KNC, Sowmyanarayanan TV, Paul A, Babji S, Ajjampur SSR, Priyadarshini S, Sarkar R, Balasubramanian KA, Wanke CA, Ward HD, et al. Immune response and intestinal permeability in children with acute gastroenteritis treated with lactobacillus rhamnosus GG: A randomized, double-blind, placebo-controlled trial. Clin Infect Dis. 2014;58:1107–1115. doi: 10.1093/cid/ciu065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Alam S, Mushtaq M. Antibiotic associated diarrhea in children. Indian Pediatr. 2009;46(6):491–496. [PubMed] [Google Scholar]
- 56.Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2014; [DOI] [PubMed]
- 57.Kotloff KL, Nataro JP, Blackwelder WC, Nasrin D, Farag TH, Panchalingam S, Wu Y, Sow SO, Sur D, Breiman RF, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the global enteric multicenter study, GEMS): a prospective, case-control study. Lancet. 2013;382(9888):209–222. doi: 10.1016/S0140-6736(13)60844-2. [DOI] [PubMed] [Google Scholar]
- 58.Lazzerini M, Wanzira H. Oral zinc for treating diarrhoea in children. Cochrane Database Syst Rev. 2016;12:CD005436. doi: 10.1002/14651858.CD005436.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Fischer Walker CL, Bhutta ZA, Bhandari N, Teka T, Shahid F, Taneja S, Black RE, Zinc Study G. Zinc supplementation for the treatment of diarrhea in infants in Pakistan, India and Ethiopia. J Pediatr Gastroenterol Nutr. 2006;43(3):357–363. doi: 10.1097/01.mpg.0000232018.40907.00. [DOI] [PubMed] [Google Scholar]
- 60.Organization WH: Pocket book of hospital care for children: guidelines for the management of common illnesses second edition. In. Geneva, Switzerland: WHO; 2013. [PubMed]
- 61.Organization WH: Diarrhoea Treatment Guidelines. In. Geneva, Switzerland: WHO; 2005.
- 62.PPernica JM, Steenhoff AP, Mokomane M, et al. Rapid enteric testing to permit targeted antimicrobial therapy, with and without Lactobacillus reuteri probiotics, for paediatric acute diarrhoeal disease in Botswana: A pilot, randomized, factorial, controlled trial. PLoS One. 2017;12:e0185177. [DOI] [PMC free article] [PubMed]
- 63.Pavlinac PB, Denno DM, John-Stewart GC, Onchiri FM, Naulikha JM, Odundo EA, Hulseberg CE, Singa BO, Manhart LE, Walson JL. Failure of Syndrome-Based Diarrhea Management Guidelines to Detect Shigella Infections in Kenyan Children. J Pediatric Infect Dis Soc. 2016;(5, 4):366–74. [DOI] [PMC free article] [PubMed]
- 64.Rogawski ET, Platts-Mills JA, Seidman JC, John S, Mahfuz M, Ulak M, Shrestha SK, Soofi SB, Yori PP, Mduma E, et al. Use of antibiotics in children younger than two years in eight countries: a prospective cohort study. Bull World Health Organ. 2017;95(1):49–61. doi: 10.2471/BLT.16.176123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Weizman Z, Binsztok M, Fraser D, Deckelbaum RJ, Granot E. Intestinal protein loss in acute and persistent diarrhea of early childhood. J Clin Gastroenterol. 2002;34(4):427–429. doi: 10.1097/00004836-200204000-00008. [DOI] [PubMed] [Google Scholar]
- 66.Sarker SA, Wahed MA, Rahaman MM, Alam AN, Islam A, Jahan F. Persistent protein losing enteropathy in post measles diarrhoea. Arch Dis Child. 1986;61(8):739–743. doi: 10.1136/adc.61.8.739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lutter CK, Mora JO, Habicht JP, Rasmussen KM, Robson DS, Sellers SG, Super CM, Herrera MG. Nutritional supplementation: effects on child stunting because of diarrhea. Am J Clin Nutr. 1989;50(1):1–8. doi: 10.1093/ajcn/50.1.1. [DOI] [PubMed] [Google Scholar]
- 68.Gat-Yablonski G, Phillip M. Nutritionally-induced catch-up growth. Nutrients. 2015;7(1):517–551. doi: 10.3390/nu7010517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Soliman AT, ElZalabany MM, Salama M, Ansari BM. Serum leptin concentrations during severe protein-energy malnutrition: correlation with growth parameters and endocrine function. Metab Clin Exp. 2000;49(7):819–825. doi: 10.1053/meta.2000.6745. [DOI] [PubMed] [Google Scholar]
- 70.Chouraqui JP, Michard-Lenoir AP. Feeding infants and young children with acute diarrhea. Arch Pediatr. 2007;14(Suppl 3):S176–S180. doi: 10.1016/S0929-693X(07)80024-8. [DOI] [PubMed] [Google Scholar]
- 71.Berni Canani R, Buccigrossi V, Passariello A. Mechanisms of action of zinc in acute diarrhea. Curr Opin Gastroenterol. 2011;27(1):8–12. doi: 10.1097/MOG.0b013e32833fd48a. [DOI] [PubMed] [Google Scholar]
- 72.Bettger WJ, O'Dell BL. A critical physiological role of zinc in the structure and function of biomembranes. Life Sci. 1981;28(13):1425–1438. doi: 10.1016/0024-3205(81)90374-X. [DOI] [PubMed] [Google Scholar]
- 73.Alam AN, Sarker SA, Wahed MA, Khatun M, Rahaman MM. Enteric protein loss and intestinal permeability changes in children during acute shigellosis and after recovery: effect of zinc supplementation. Gut. 1994;35(12):1707–1711. doi: 10.1136/gut.35.12.1707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Tran CD, Hawkes J, Graham RD, Kitchen JL, Symonds EL, Davidson GP, Butler RN. Zinc-fortified oral rehydration solution improved intestinal permeability and small intestinal mucosal recovery. Clin Pediatr (Phila) 2015;54(7):676–682. doi: 10.1177/0009922814562665. [DOI] [PubMed] [Google Scholar]
- 75.Alverdy JA, Aoys E, Weiss-Carrington P, Burke DA. The effect of glutamine-enriched TPN on gut immune cellularity. J Surg Res. 1992;52(1):34–38. doi: 10.1016/0022-4804(92)90275-5. [DOI] [PubMed] [Google Scholar]
- 76.Barber AE, Jones WG, 2nd, Minei JP, Fahey TJ, 3rd, Moldawer LL, Rayburn JL, Fischer E, Keogh CV, Shires GT, Lowry SF. Harry M. Vars award. Glutamine or fiber supplementation of a defined formula diet: impact on bacterial translocation, tissue composition, and response to endotoxin. JPEN J Parenter Enteral Nutr. 1990;14(4):335–343. doi: 10.1177/0148607190014004335. [DOI] [PubMed] [Google Scholar]
- 77.Burke DJ, Alverdy JC, Aoys E, Moss GS. Glutamine-supplemented total parenteral nutrition improves gut immune function. Arch Surg. 1989;124(12):1396–1399. doi: 10.1001/archsurg.1989.01410120042009. [DOI] [PubMed] [Google Scholar]
- 78.Galvao TF, Thees MF, Pontes RF, Silva MT, Pereira MG. Zinc supplementation for treating diarrhea in children: a systematic review and meta-analysis. Rev Panam Salud Publica. 2013;33(5):370–377. doi: 10.1590/S1020-49892013000500009. [DOI] [PubMed] [Google Scholar]
- 79.Lamberti LM, Walker CL, Chan KY, Jian WY, Black RE. Oral zinc supplementation for the treatment of acute diarrhea in children: a systematic review and meta-analysis. Nutrients. 2013;5(11):4715–4740. doi: 10.3390/nu5114715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Walker CL, Black RE. Zinc for the treatment of diarrhoea: effect on diarrhoea morbidity, mortality and incidence of future episodes. Int J Epidemiol. 2010;39(Suppl 1):i63–i69. doi: 10.1093/ije/dyq023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Allen SJ, Martinez EG, Gregorio GV, Dans LF. Probiotics for treating acute infectious diarrhoea. Cochrane Database Syst Rev. 2010;11:CD003048. doi: 10.1002/14651858.CD003048.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Applegate JA, Fischer Walker CL, Ambikapathi R, Black RE. Systematic review of probiotics for the treatment of community-acquired acute diarrhea in children. BMC Public Health. 2013;13(Suppl 3):S16. doi: 10.1186/1471-2458-13-S3-S16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Guarino A, Ashkenazi S, Gendrel D, Lo Vecchio A, Shamir R, Szajewska H. European Society for Pediatric Gastroenterology, Hepatology, and nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59(1):132–152. doi: 10.1097/MPG.0000000000000375. [DOI] [PubMed] [Google Scholar]
- 84.Denno DM, VanBuskirk KM, Nelson ZC, Musser CA, Tarr PI.: Environmental enteric dysfunction: advancing current knowledge. St. Louis, MO: Washington University Libraries; 2016.
- 85.Collaborators GH, Wang H, Wolock TM, Carter A, Nguyen G, Kyu HH, Gakidou E, Hay SI, Mills EJ, Trickey A, et al. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980-2015: the global burden of disease study 2015. Lancet HIV. 2016;3(8):e361–e387. doi: 10.1016/S2352-3018(16)30087-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Pavlinac PB, John-Stewart GC, Naulikha JM, Onchiri FM, Denno DM, Odundo EA, Singa BO, Richardson BA, Walson JL. High-risk enteric pathogens associated with HIV infection and HIV exposure in Kenyan children with acute diarrhoea. AIDS. 2014;28(15):2287–2296. doi: 10.1097/QAD.0000000000000396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Mondal D, Haque R, Sack RB, Kirkpatrick BD, Petri WA., Jr Attribution of malnutrition to cause-specific diarrheal illness: evidence from a prospective study of preschool children in Mirpur, Dhaka, Bangladesh. Am J Trop Med Hyg. 2009;80(5):824–826. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.