

Abstract
Culture not only justifies the existence of libraries but also determines the level of funding libraries receive for development. Cultural appreciation of the importance of libraries encourages their funding; lack of such appreciation discourages it. Medical library development is driven by culture in general and the culture of physicians in particular. Nineteenth-century North American medical library funding reflected the impact of physician culture in three phases: (1) Before the dawn of anesthesia (1840s) and antisepsis (1860s), when the wisdom of elders contained in books was venerated, libraries were well supported. (2) In the last third of the nineteenth century, as modern medicine grew and as physicians emphasized the practical and the present, rather than books, support for medical libraries declined. (3) By the 1890s, this attitude had changed because physicians had come to realize that, without both old and new medical literature readily available, they could not keep up with rapidly changing current clinical practice or research. Thus, “The Medical Library Movement” heralded the turn of the century.
INTRODUCTION
The cultural patterns by which institutional medical libraries in the United States and Canada are funded (or not funded) today were established in the second half of the nineteenth century. The purpose of this paper is to show the development of these patterns. All libraries are products of money and culture, the integrated pattern of human knowledge, belief, and behavior built up and passed on from generation to generation. Since ancient Egypt and Babylon, libraries have served as an important medium for the preservation and transmission of culture as contained in the records of human knowledge. Medical libraries are products of the prevailing general culture, especially the culture of physicians. In the mid-nineteenth century, the culture of physicians in the Western World began to evolve into today's medical professionalism, which demands instant access to current information [1]. Medical libraries, private and public, since that time have grown into and have accurately reflected this modern medical culture.
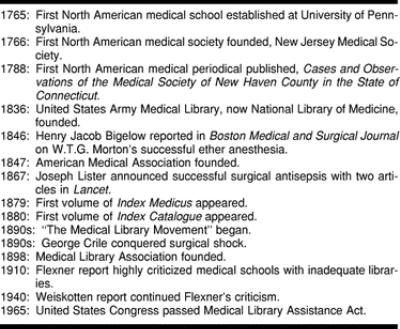
Changes in nineteenth century North American physicians' attitudes toward the support of medical libraries are discernible in three phases: (1) the pre-anesthesia, pre-antisepsis medical world, (2) the dawn of modern western medical attitudes, and (3) “The Medical Library Movement.” The dates of these three phases cannot be precise, because trends shift gradually, but the timeline in Figure 1 provides some benchmarks.
1. THE PRE-ANESTHESIA, PRE-ANTISEPSIS MEDICAL WORLD
Before 1846, medical educators in North America commonly believed that hands-on learning was not necessary, because medical students could learn anatomy and even clinical practice chiefly from books and lectures [2]. Physicians generally respected theoretical speculation alongside empirical science as a method of acquiring medical knowledge. The medical community venerated the literary tradition following the two most important books in the history of medicine: Andreas Vesalius's De humani corporis fabrica (1543), which originated the modern study of anatomy, and William Harvey's De motu cordis (1628), which revolutionized physiology. Post-Vesalian, post-Harveian books, containing the wisdom of the elders, were regarded as authorities on medical matters at least equal to, and perhaps greater than, clinical experience and direct observation. The early nineteenth century produced some of the keenest observers of anatomical and pathological fact the world has ever known. Twenty-first century physicians, primarily dependent upon a plethora of diagnostic instruments rather than their own five senses, can marvel at the accuracy and detail of, for example, William Wood Gerhard's intricate description of bronchitis [3]. Yet even the best observers in the nineteenth century deferred to the written record of past generations [4].
The progress of medical knowledge was slow until the revolutionary implementations of anesthesia in the 1840s and antisepsis in the late 1860s. In the aftermath of these developments and with the significant increase in surgical knowledge gained during the Civil War, an attitude grew among physicians that medical libraries were merely repositories of quaint curiosities and outdated information, that they had little clinical importance, and that current literature was disposable almost as soon as the next article or book appeared on the subject [5]. In 1875, at least one medical school bulletin took a quite condescending view toward antebellum medical literature, referring to its own institutional library as “especially rich in the medical literature of an earlier day” [6], but made no claims about the extent of its current medical literature, thus insinuating that there was no practical need for the library to maintain an up-to-date collection. Indeed, after about 1870, that library made no effort until the late 1890s to keep its collection current [7]. Such an attitude stood in sharp contrast to that which prevailed for the first half of the nineteenth century, whereby physicians generally held medical libraries in great esteem. In that era, medical education was chiefly by lecturing rather than demonstrating, by reading rather than doing, and by memorizing the wisdom of predecessors rather than direct clinical experience [8].
In the 1870s, physicians commonly believed that medical progress did not require libraries full of books and old journals but only modern clinical and experimental results reported in contemporary and quickly superseded medical periodical articles, whose disposability was suggested even by the substandard paper on which they were typically printed. Their attitude was gradually supplanted in the 1890s under the leadership of George Milbry Gould (1848–1922), William Osler (1849–1919), and Charles D. Spivak (1861–1927), among others [9].
The nineteenth century was an era of widespread interest in curiosities for their own sake, not only those intended for popular exhibit by P. T. Barnum and others but also those collected by physicians—such as Frank Hastings Hamilton (1813–1886), Joseph Leidy (1823–1891), Thomas Dent Mütter (1811–1859), and Isaac Parrish (1811–1852)—for their own pleasure and that of their professional colleagues. Private “pathological cabinets” were quite common at the time. Yet these curiosities—such as tumors in jars, bullet-shattered bones, Chang and Eng Bunker's conjoined liver, or anthropodermic bookbindings, which might seem bizarre, irreverent, or even criminal today—were not intended merely to entertain ghoulish physicians but to instruct. As such, they were intended to be protected and preserved alongside the medical books and journals themselves. Through most of the nineteenth century, medical libraries almost always existed in tandem with anatomical or pathological museums, and they were thought to go hand-in-hand as teaching tools [10].
Given the pre-anesthesia physicians' propensity toward “book-larnin” early in the nineteenth century, it was not difficult for medical schools to secure large donations of both money and books for their libraries. For example, in 1820, a relatively obscure backwoods American medical school, Transylvania University, received a donation of $17,000 for the purchase of books [11]. Using the 1967 United States consumer price index (CPI) of 100 as a benchmark, the 1820 CPI of 42, and the 1994 CPI of 444.6, that amount would be approximately $180,000 in 1994 dollars. Apparently, Transylvania University had little trouble financing its medical library before the Civil War [12]. In 1839, the same library received a gift of another $11,000. These two gifts resulted in the purchase of more than 10,000 books.
In the United States before the Civil War, few medical libraries were in the public sector. They were privately owned by hospitals, medical schools, pharmaceutical schools, medical societies, or individual physicians, not state-sponsored institutions. Societies, hospitals, and educational institutions relied mainly on donations for collection development and volunteers for labor. Cataloging was minimal. Books and journals were usually just displayed on shelves in small, dark, uncomfortable rooms, uncataloged but readily available to authorized persons. At best, they would be arranged in a gentleman's smoking room as a browsing collection, perhaps in alphabetical order or loosely grouped by subject, accession date, or size. The overhead for the upkeep of antebellum institutional medical libraries was small. A librarian was not necessary. A clerk or a servant recorded accessions in a ledger and reshelved volumes. Because little effort was expended to facilitate access and retrievability, books were in effect just “warehoused” [13].
With the possible exception of the library of the College of Physicians of Philadelphia, whose collection was built mainly on donations [14, 15], the greatest medical libraries in nineteenth-century North America (especially in the antebellum period) were owned by individuals. These great private medical libraries came into existence as physicians such as Anson Colman (fl. 1836), Samuel D. Gross (1805–1884), Hugh Lenox Hodge (1796–1873), Samuel Lewis (1813–1890), Osler, and Stephen Smith (1823–1922) recognized the need to protect, preserve, and publicize the rich heritage of what, since the 1840s, had become a very rapidly changing field [16, 17]. Many such private libraries, when bequeathed, came to be either the foundations or significant components of major institutional medical libraries. Colman's went to Geneva Medical College and Smith's went to its successor, the Syracuse University College of Medicine (both now SUNY Upstate Medical University); Lewis's and Gross's to the College of Physicians of Philadelphia; Osler's to McGill University; and Hodge's to several locations through the agency of his son, Hugh Lenox Hodge (1836–1881), and Gould. It is inconceivable that any of these institutional libraries could have become substantial repositories of medical knowledge without the foresight and generosity of such collectors. Yet for many personal medical libraries, especially after the Civil War, the death of the owner entailed the dispersal or destruction of the collection at the hands of ignorant or apathetic heirs.
2. THE DAWN OF MODERN WESTERN MEDICAL ATTITUDES
A typical physician of 1820 was likely to regard a seventeenth-century medical text as clinically important, but a typical physician of 1880 was unlikely to do so. Inspired by the incredible success of antisepsis and anesthesia in surgery and by the leap in medical and surgical knowledge that almost always follows a major war, many physicians born between about 1820 and 1845 saw, by the 1870s, little practical need to preserve the pre-antisepsis, pre-anesthesia literature, let alone enshrine it in institutional libraries. They did not neglect reading in the furtherance of their clinical practices, but while their predecessors preferred the venerable old medical books, supplemented with case reports in the journal literature, they tended to limit their reading to current state-of-the-art breakthroughs in their particular fields, as recorded in the journal literature [18].
At first, they were able to fill their professional reading needs with private journal subscriptions and book purchases, but as topics became more diverse and more narrowly circumscribed and as the literature on these topics grew, the next generation of physicians (Gould's generation, which came of age in the 1880s) discovered that as individuals they could not each keep up with all the current literature relevant to their respective clinical practices and thus had to rely upon libraries whether they wanted to or not. The last third of the nineteenth century was the beginning of the complex specialization in medicine recognized today—and the literature of the time, both in quantity and in orientation, accurately reflected that. The standard bibliography of nineteenth-century, North American medicine showed only 1,406 medical titles published in the 1840s but 10,378 in the 1890s [19]. Individual finances simply could not keep up with that explosion. As Charles Perry Fisher (1857–1940) noted during his tenure as librarian of the College of Physicians of Philadelphia, individual physicians practicing prior to 1879, when Index Medicus first appeared, were obliged to acquire and maintain private collections of medical journals, often at great expense, only to have these gatherings of a lifetime scattered and wasted after their deaths [20]. The increasing difficulty for physicians to maintain current professional literature collections on their own was even more pronounced on the frontier and in rural areas [21, 22].
Medical books tend to be more expensive than most books. This has always been the case. Medical libraries have always been hard pressed financially to keep their holdings comprehensive (or at least adequate) with regard to the current state of the clinical art. For example, in the July 1866 catalog of prominent Philadelphia medical publisher Henry C. Lea, prices ranged from $1.00 for small duodecimos such as a popular work on skin care to $14.00 for Joseph Maclise's Surgical Anatomy and $15.00 for the four-volume Cyclopaedia of Practical Medicine, with most of the standard texts costing in the vicinity of $4.00 to $6.00 [23]. A modern medical text might seem cheap at these prices, but not in the days when most trade books sold for less than a dollar, medical journal subscriptions typically ran between $5.00 and $10.00 per annum, and postage was figured in half-cents. Nowadays, a typical medical title could cost in the hundreds, and a typical medical journal subscription could cost in the thousands per annum. Unlike individual physicians, medical libraries cannot pass these costs on to their patients but must simply do without or else go begging. In this regard, institutional medical library management today is no different from the nineteenth century.
The generation of physicians and surgeons who came of age during the Civil War or shortly thereafter had little interest in preserving the records of bygone medical eras and believed that the typical contents of institutional medical libraries were of little or no clinical importance [24]. This generation dominated North American medical culture until the 1880s.
Yet, medicine is a conservative profession. For example, in the nineteenth century, it was a frequent conceit among the Fellows of the College of Physicians of Philadelphia that theirs was the most conservative organization in North America, not necessarily in the political sense but in the cultural sense.† Such conservativism could be detected in the kind of support given in the 1870s to the most prestigious medical libraries, such as the New York Academy of Medicine (NYAM) and the Army Medical Library (now the National Library of Medicine). The physicians of this generation, mostly rich and highborn, seemed to have been motivated, despite the remarkable medical and surgical progress of the Civil War and its immediate aftermath (progress in which many of them indeed participated), to protect and preserve “the way we did things,” in other words, the methods, results, and curiosities of their own bygone era, the antebellum American medical world. To illustrate this point, when the new library building of the NYAM was dedicated in October 1879, the average age of the sixteen participants‡ on the podium was sixty-one (average birth year 1818) [25], which meant that most of them were already established professionals when the Civil War broke out. The entire cost of this project was paid by subscriptions and donations, so that at the time of dedication “not a single cent of debt remained” [26].
In contrast to this prestigious medical society library of the 1870s, strongly supported by the “Old Guard,” the Syracuse University College of Medicine (SUCM) library was severely neglected from the 1870s to the mid-1890s, under the governance of much younger physicians, about half of whom had little or no antebellum medical or surgical experience. In 1872, the average age of the eighteen physicians§ on the original SUCM faculty was only forty-seven (average birth year 1825) [27]. The older faculty such as John Towler and Frederick Hyde supported the library, but, with the notable exception of John Van Duyn, most of the younger faculty gave little notice to it, and even Van Duyn's interest in the library was not manifested until much later in his career.
The younger physicians belonged mostly to the generation that provided such breakthroughs as first allowing women into the profession. They regarded themselves as progressive and perhaps even radical, both culturally and clinically, while the older generation offered such laments as this, in 1879: “We regret to be obliged to announce that at a meeting of councilors held on October 1, it was voted to admit women to the Massachusetts Medical Society” [28].
Despite the financial hardship on individual physicians who tried to maintain their own respective collections of medical literature, institutional medical libraries were generally neglected, even scorned, for much of the second half of the nineteenth century, except by a few sagacious physicians such as John Shaw Billings [29], James R. Chadwick, Samuel Smith Purple [30, 31], Spivak [32], and Joseph Meredith Toner. Throughout most of the nineteenth century, until the 1890s, the institutional medical library remained a low-budget item. Institutional acquisition of medical books was almost entirely by gift, by swapping duplicates, or by bulk purchase of used books, almost never by deliberate purchase of specific new titles.
Some of the slack in medical acquisitions was taken up by public libraries and other nonmedical institutional libraries. In the nineteenth century, some public libraries, even free libraries, had substantial medical collections. Gould, for one, vigorously advocated that public libraries should acquire medical titles [33]. But these collections eventually dwindled, mainly because public librarians could not meet the demands of physicians in either collection development or reference service. Billings noted in 1876 that the Boston Public Library had the best medical collection in the city, but that it was uncataloged and therefore difficult to use [34]. In 1875, an anonymous physician (perhaps Chadwick) argued for the creation of an easily consulted medical library in Boston, because:
Admirable as the Boston Public Library is (in some respects), it must be confessed that so far as its medical department is concerned a liberal expenditure of both time and patience is often required before the seeker can obtain, if he obtains at all, a sight of the book or journal required. [35]
This same article announced the organization of the Boston Medical Library Association (BMLA) in response to this perceived need.
With a few notable exceptions (e.g., the libraries of Transylvania University, Harvard University, the NYAM, and the BMLA) private institutional medical libraries in the mid- to late-nineteenth century tended not to have firm financial foundations. Although libraries had grown in size, funds for acquisition tended to be inadequate, and standards of service were almost nonexistent. In 1876, Chadwick reported on the situation of medical libraries in Boston [36]. Harvard relied on donations of volumes and money and was extremely well off. The Boston City Library's medical collection consisted mostly of donated volumes from Boston's sizeable community of physicians and was quite fortunate in both the variety and completeness of its journal runs. Four other medical libraries in Boston were funded by dues or by subscription, with varying degrees of success. In 1890, E. D. Ferguson reported that the Library of the New York State Medical Association was supported entirely by members' gifts of books, journals, and money [37].
As Billings's charismatic influence on the medical community grew, demand increased for the federal government to become involved, not in financing medical libraries but in financing a single, gigantic medical library. Should such a library be an outgrowth of the Army Medical Library, which Surgeon General Joseph Lovell (1788–1836) had begun, and thus be a separate entity? Or should it be just a department of the Library of Congress? This debate resounded through medical circles in the late 1870s and early 1880s [38]. For example, one article would explain the nature of the dispute [39]; another, noting the tendency of Congress to obey the wishes of physicians when these wishes were “tolerably unanimous and clearly expressed,” would urge that any national medical library remain separate from the Library of Congress [40].
Leading the political fight for the establishment and firm congressional support of a national medical library were not the younger physicians, readers of the current literature, but the Old Guard, whose main agenda was preserving old medical literature and honoring the pantheon of physicians. For example, Frederick Horner, who may have had ulterior motives insofar as he lived just across the Potomac in Alexandria, Virginia, gave lip service to the “original research” favored by young physicians, but his motivation was really that of the Old Guard:
We need a safe repository [independent of the Library of Congress] for the invaluable writings of the fathers of American medicine and surgery … and of the glorious galaxy of living men … [and this proposed facility should include a] hall for statuary and a gallery for portraits of eminent members of the profession. [41]
Considering options of involving the American Medical Association (AMA), the Library of Congress, and the Medical Society of the District of Columbia, Toner was in favor of venerating the entire medical tradition, but especially the North American medical tradition:
The value of books to the medical man cannot be over estimated. They are the inexhaustible fount of knowledge from which the discoveries of the day, and the accumulated experience of ages may be drawn. The physician whose studies lead him to consult early North American medical literature must be painfully struck with the perishable character of our professional literature, and the meagre or fragmentary collections which have been made. [42]
In 1882, Toner announced his gift of 20,000 volumes to the Library of Congress [43].
Billings was the real hero of this era [44]. The federal government became heavily involved in medical librarianship only during the Civil War, when Billings began to pursue his vision of making the surgeon general's library the greatest medical reference collection in the world. As early as the mid-1890s, the worldwide health care community generally acknowledged that he had achieved this goal [45], not only through developing the collection but also through his founding of Index Medicus in 1879 and Index Catalogue in 1880. Billings denied reports that he was the founder of the Army Medical Library, naming Lovell and Hammond as his predecessors, but acknowledged that between 1865, when he assumed office, and 1880, the holdings of that library grew from 1,800 to 50,000 volumes [46]. Even as early as 1878, one physician visiting the Army Medical Library expressed sheer amazement at the breadth and depth of the collection (e.g., bound volumes of pamphlets that had belonged to Claude Bernard). He praised Billings, the administration, and the ambiance of the library, which was then housed in the old Ford's Theatre, scene of the Lincoln assassination, and which was well on its way toward outgrowing those walls [47].
In 1876, George F. Shrady applauded one of Billings's pet projects, Index Catalogue, claiming that it would place the world's medical literature in front of those who could not travel to Washington [48]. In 1878, Shrady expressed the strong support of the medical community for Billings's plan to create this “index, as it were, of the medical literature of the world,” even at the then huge cost to the taxpayers of $25,000 for 3,000 copies each of the first two volumes [49]. The medical community's praises of Congress for its creation of a national medical library and for its funding of Index Catalogue were not in short supply.** By 1883, a groundswell of support for Billings's program had arisen in state medical societies and other professional medical organizations. Gross successfully offered a strongly worded resolution at the annual meeting of the Medical Society of the State of Pennsylvania urging Congress to appropriate money for “the erection of a fire-proof building to contain the library and museum of the Surgeon-General's Office,” noting with regret that such a bill had already once failed to be passed [50]. James Reeves offered a similar resolution to the Medical Society of West Virginia, which passed it unanimously [51].
3. "THE MEDICAL LIBRARY MOVEMENT"
Not until the 1890s, did North American medical schools realize that their own well-stocked and well-maintained medical libraries would be essential components of the rapid modernization of medical pedagogy, which began in the 1870s with the shift from proprietary schools to graded instruction [52]. While Albert T. Huntington could write in 1904 that “it is … only within the last decade that the medical library movement has become active and widespread,” treating the establishment of medical libraries as a fait accompli [53]; just a decade earlier he would have had to be more contentious to persuade his readers of the need for such institutions. Even though more North American medical libraries were founded in the 1890s than in the 1860s, 1870s, and 1880s combined [54], advocates such as William Browning remained polemical in their support of medical libraries, even as late as 1899 [55].
The lack of attention to medical libraries, the prevailing attitude not only in medical schools but throughout the entire medical community, gradually evolved into a “medical library movement,” a fusion of the aims of both the Old Guard and the younger physicians in a third generation of physicians, who saw the need both to protect and to venerate the tradition and to make readily and freely available to all practitioners the widest possible sampling of the published results of current research. Gould (b. 1848), Frank William Marlow (b. 1858), Osler (b. 1849), and Spivak (b. 1861) were among this third generation who rediscovered and reinvented the medical library. They resembled the first generation rather than the second insofar as they attached importance to the contents of medical libraries; but unlike the first generation, and indeed more like the second, they regarded these contents not as curiosities, historical documents, or hallmarks of medical tradition but as fundamental tools of current clinical practice. The ultimate impetus for the rebirth and growth of medical libraries in the 1890s was neither the veneration of tradition—as Purple, Horner, and their cohorts had imagined—nor the sheer growth of literature, nor the development of bibliographic science†† but rather the discovery that libraries were excellent means for current research [56]. This latter view predominates in the medical world today [57]. The attitude that medical libraries are research facilities rather than repositories has proved fundamental in the design, construction, and funding of medical libraries in the twentieth century [58].
Browning, Chadwick, Gould, Spivak, and others habitually referred to the trend of the 1890s as The Medical Library Movement [60]. They published a flurry of contentious articles in the medical press. For example, in 1895, Bayard Holmes argued for supporting the professionalization of medical librarianship and implored medical libraries to adopt the Dewey Decimal System [61]. In 1897, one of Spivak's many polemics urged individual, practicing physicians to assist with collection development (e.g., by writing and circulating want lists) [62]. In 1898, Gould argued that medical publishers should actively and financially support the promulgation and proliferation of institutional medical libraries, not only to enhance the quality of medical knowledge and patient care, especially in outlying areas, but also to help weed out the “utterly worthless medical literature” that sometimes found its way into physicians' hands, in other words, to create a new means of quality control for medical publishing itself [63]. In 1899, Browning pleaded for independent medical libraries to be established in towns and small cities and offered unqualified praise of Gould's interlibrary exchange program for duplicates and other unwanted titles [64].
Although there had been some pockets of North American medical culture, from as early as the 1870s, that were enlightened about the wider role and importance of modern medical libraries, Spivak, who surveyed 120 American medical schools in 1898, received reports of only twenty-four libraries affiliated with those schools [65]. Clearly, a crusade was needed. Directly addressing this perceived need, Gould, Osler, and a few others in the 1890s launched a vigorous effort to encourage physicians to take seriously the published heritage of medicine as useful, not only for purposes of learning history but even for current clinical practice, and in that spirit to bequeath their personal collections of books to medical schools and other health care institutions, especially because these institutions had few other means of acquiring books [66].‡‡ They and, even as early as the late 1890s, most other advocates of institutional medical libraries made similar claims for the current practical value of “old books” and encouraged the individuals who owned these medical journals and books not to throw them away when they retired from clinical practice and not to let their heirs decide what to do with them but rather to donate them to institutions that would preserve them, not only for the use of current practitioners but also for posterity.
Among the goals of The Medical Library Movement were to improve service, professionalize medical librarianship, establish standards, facilitate acquisition and barter of texts, broaden holdings, and encourage the proliferation of significant medical collections in outlying areas. Toward these goals, a committee of physicians and librarians founded the Medical Library Association (MLA) [67]. At the inaugural meeting of the MLA, on May 2, 1898, in Philadelphia, cofounder and first president Gould proposed the formation of eight standing committees, the first seven of which concerned the financing of library acquisitions:
(1) On Exchange of Library Duplicates. (2) For Securing Libraries of Retiring or Deceased Physicians. (3) For Securing and Distribution of Transactions of Medical Societies. (4) On Antiquarian Books and Auction Sales. (5) For Securing Endowments of Medical Libraries. (5) On Rare Works in Single Libraries. (6) For Supplying Special Information, Securing Useful Abstracts, etc. (8) On Library Management, Technic, Devices, Binding, etc. [68]
As medical libraries grew and their collections became more difficult to manage, complaints about service increased. Gone were the days when an entire collection could fit into a single reading room and be easily browsed. Readers demanded better, quicker service, that is, better accessibility, which could not be achieved without enhanced cataloging, which entailed hiring more medical librarians and enforcing higher standards and more rigorous training for them. The Medical Library Movement, in general, and MLA, in particular, soon made great strides toward ameliorating this situation. Of course, this necessary increase in both the number and skills of medical librarians had to involve a dramatic increase in personnel costs, and MLA dealt with that problem too. By the time of the pivotal Flexner report (1910) medical schools were simply expected to include strong, perennial funding for their libraries in their regular budgets—or else feel the blow of Abraham Flexner's hammer. His assessment of each school would have an immediate effect on its funding, foundation support, AMA approval, applicant pool, and viability. Flexner considered the library under the general heading of “laboratory facilities” [69]. For both Flexner and, thirty years later, Herman G. Weiskotten, following the spirit of Osler, the library was the centerpiece of any competent medical school [70, 71].
Yet, despite the approval of the AMA, state medical societies, the Carnegie Foundation, and other influential organizations, there was some reaction from the Old Guard against The Medical Library Movement. For example, Chadwick in 1896 felt the need to defend himself against charges that his view of medical libraries was too “prosaic” or “utilitarian,” that is, that he did not sufficiently venerate the tradition [72]. Nevertheless, Chadwick's own fundraising and proselytizing efforts were remarkably fruitful. Through his leadership, all resolutions for major improvements to the physical plant of the library presented at a special BMLA meeting in 1898 passed unanimously [73]. The financing of this massive five-year project was achieved entirely from dues, subscriptions, rents, and gifts. Chadwick considered it all a grand success [74].
CONCLUSION
Libraries cost money, no matter what type they are—private, societal, public, school, national, or special—and if the prevailing culture in any era does not value the contents or contributions of libraries, then they are not going to be funded [75].
As recently as 1988, a study of the economics of academic health sciences libraries in the United States had to belabor the obvious: “The continuance of the library as a resource for information, its management, acquisition and dissemination is only possible when based on firm financial foundation” [76]. More often than not, to actualize this possibility entails recourse to the vagaries and inconsistencies of government support.
North American physicians of the late nineteenth century came to appreciate medical libraries as fundamental tools of current clinical practice and research. They advocated improving and developing medical libraries and, for the first time, called for government financing and involvement in medical library development. Their advocacy resulted in significant government funding in the 1870s for what is now the National Library of Medicine. It was physicians who started and led The Medical Library Movement. In its earliest days, MLA involved roughly equal numbers of librarians and physicians. Many physicians, such as Marlow, were also librarians. Their crusade grew into not only MLA but also a dominant culture that professionalized medical librarianship and eventually, in 1965, brought about the passage of the United States Medical Library Assistance Act, which ensured adequate recurrent funding for health sciences libraries and laid a firm foundation for impressive development [77]. A position paper published in 1963 argued vigorously that federal money should be the mainstay of medical library budgets [78].
The willingness to involve the government in medical library development was only nascent in the 1870s, but, especially after the United States Army Medical Library was first recognized in the late 1870s and early 1880s and universally recognized by the mid-1890s as the most comprehensive medical collection in the world, that willingness has grown steadily. Because of physicians' involvement in, and support for, medical library development and their recognition of the relevance of libraries to clinical practice and research, medical libraries have evolved since the late nineteenth century into institutions that need government funding just to meet their minimal goals [79, 80]. Even in a world of digital resources and rapid technological changes, these physician-driven factors remain fundamental for the further development and prosperity of medical libraries.
Figure 1 Milestones in the development of U.S. medical libraries
Acknowledgments
The authors are grateful to Gretchen Worden, director of the Mütter Museum, for her help in preparing the final revisions.
Footnotes
* An earlier version of this paper was presented at the Thirteenth Annual Interdisciplinary Nineteenth Century Studies (INCS) meeting at Loyola University, New Orleans, Louisiana; April 18, 1998. A subsequent version won the MLA 1999 Murray Gottlieb Prize.
† See Summary of the Transactions of the College of Physicians of Philadelphia, 1844–1874, and Transactions of the College of Physicians of Philadelphia, 1875–1937; passim. The remark may have originated with David Hayes Agnew (1818–1892).
‡ The physicians were Henry W. Acland (b. 1815), James Anderson (b. 1798), Fordyce Barker (b. 1818), John Shaw Billings (b. 1838), Freeman J. Bumstead (b. 1826), William L. Detmold (b. 1808), Austin Flint (b. 1812), Samuel D. Gross (b. 1805), James R. Leaming (b. 1820), Willard Parker (b. 1800), Alfred C. Post (b. 1806), Samuel Smith Purple (b. 1822), George C. Shattuck, Jr. (b. 1813), T. Gaillard Thomas (b. 1831), Robert F. Weir (b. 1838), and William T. White (b. 1829).
§ The physicians were J. Otis Burt (b. 1835), Henry Darwin Didama (b. 1823), Joseph P. Dunlap (b. 1814), Hiram N. Eastman (b. 1810), Frederick Hyde (b. 1809), Miles Goodyear Hyde (b. 1841), John W. Lawton (b. ca. 1835), Alfred Mercer (b. 1820), Nelson Nivison (b. 1816), Roger W. Pease (b. 1828), William Tomlinson Plant (b. 1836), Wilfred W. Porter (b. 1826), John Van Pelt Quackenbush (b. 1819), Charles E. Rider (b. 1839), Edward B. Stevens (b. 1823), John Towler (b. 1811), John Van Duyn (b. 1843), and Hervey Backus Wilbur (b. 1820).
** For example, Committee of the Medical Society of the County of New York. The National Medical Library. Med Record (NY) 1878;13:220.
†† Dondale argued that the expansion of medical literature and the progress of bibliographic organization were the two main reasons for the proliferation of medical libraries in the 1890s, but he overlooked the psychological fact that people would not necessarily want, need, or support a benefit just because it existed. They must first become convinced of its value. Accordingly, it was the changing attitude of physicians toward the usefulness of medical literature that made medical libraries grow [59].
‡‡ For a brief appraisal of Gould's contributions to the medical library movement, see Wannarka MB. Dr. George Milbry Gould: ophthalmologist and first president of the Medical Library Association. Bull Hist Med 1968;42(3):265–71.
REFERENCES
- Starr P. The social transformation of American medicine. New York, NY: Basic Books, 1982:3–6,16–21,54–9,135–40,142,336. [Google Scholar]
- Norwood WF. Medical education in the United States before the Civil War. Philadelphia, PA: University of Pennsylvania Press, 1944:401. [Google Scholar]
- Gerhard WW. Lectures on the diagnosis, pathology, and treatment of the diseases of the chest. Philadelphia, PA: Haswell & Barrington, 1842. [Google Scholar]
- Billings JS. Literature and institutions. In: Clarke EH, Bigelow HJ, Gross SD, Thomas TG, Billings JS, eds. A century of American medicine: 1776–1876. Philadelphia, PA: H. C. Lea, 1876:293–4. [Google Scholar]
- Bell WJ. Private physicians and public collections: medical libraries in the United States before 1900. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:89,95–6. [PubMed] [Google Scholar]
- Syracuse University College of Medicine. Fourth annual catalogue, 1875–76. Syracuse, NY: William L. Rose, 1875:9. [Google Scholar]
- Luft E, Hawkins DK. Elizabeth Latimer Shrimpton, M.D. (1875–1955): unsung heroine of medical librarianship. Watermark. 1996 Summer; 19(3):85–7.erratum:. 1996 Fall; 19(4): 129. [PubMed] [Google Scholar]
- Norwood WF. Medical education in the United States before the Civil War. Philadelphia, PA: University of Pennsylvania Press, 1944:396 –402. [Google Scholar]
- Bell WJ. Private physicians and public collections: medical libraries in the United States before 1900. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:89,94–5. [PubMed] [Google Scholar]
- Billings JS. Literature and institutions. In: Clarke EH, Bigelow HJ, Gross SD, Thomas TG, Billings JS, eds. A century of American medicine: 1776–1876. Philadelphia, PA: H. C. Lea, 1876:353. [Google Scholar]
- Vance CA. The Transylvania Medical Library. Kentucky Med J. 1946 Nov; 44(11):366–7.Annals Surg. 1946 Apr; 123(4): 484. [PubMed] [Google Scholar]
- Henry R. Introduction. In: Catalogue of the Transylvania University Medical Library. Lexington, KY: Transylvania University Press, 1987:vi–x. [Google Scholar]
- Bell WJ. Private physicians and public collections: medical libraries in the United States before 1900. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:88. [PubMed] [Google Scholar]
- Greifenstein CB.. Personal email to Eric v.d. Luft from the historical reference librarian, the College of Physicians of Philadelphia, 1997 Apr 9 [Google Scholar]
- Crawford K.. Personal email to Eric v.d. Luft from the curator of archives and manuscripts, College of Physicians of Philadelphia, 1997 Apr 21 [Google Scholar]
- State University of New York Health Science Center at Syracuse [i.e., Upstate Medical University] Library. Thirty-five treasures of special collections. Kennett Square, PA: KNA Press, 1993:21,24–5. [Google Scholar]
- Cushing H. The life of Sir William Osler. Oxford, U.K.: Clarendon, 1925. [PMC free article] [PubMed] [Google Scholar]
- Dondale MF. Medical libraries. In: Doe J, Marshall ML, eds. Handbook of medical library practice. Chicago, IL: Medical Library Association and American Library Association, 1956:10. [Google Scholar]
- Cordasco F. American medical imprints, 1820–1910. Totowa, NJ: Rowman & Littlefield, 1985. [Google Scholar]
- Fisher CP.. Medical libraries, medical publishers, and the medical profession. Med Libr Hist J. 1904;2:192. [PMC free article] [PubMed] [Google Scholar]
- Baird VM. Books and the doctor in nineteenth-century Texas: some early attempts to establish medical libraries. Bull Med Libr Assoc. 1968 Oct; 56(4):428. [PMC free article] [PubMed] [Google Scholar]
- Peterson R.. The need of more medical reference libraries and the way in which they can be established. Bull Amer Acad Med. 1895–1897;2:129–30. [Google Scholar]
- Caption title:. Henry C. Lea's (late Lea & Blanchard's) classified catalogue of medical and surgical instruments; 32 pages, with index, listing 160 titles, bound with publisher's cloth edition of: Flint A. A treatise on the principles and practice of medicine, designed for the use of practitioners and students of medicine. Philadelphia, PA: Henry C. Lea, 1866. [Google Scholar]
- Flexner A. Medical education in the United States and Canada: a report to the Carnegie Foundation for the Advancement of Teaching. New York, NY: The Carnegie Foundation, 1910:82. [Google Scholar]
- Anonymous. Dedication of the new library hall of the New York Academy of Medicine, October 2, 1879. Boston Med & Surg J. 1879;101:526. [Google Scholar]
- Anonymous. Dedication of the new library hall of the New York Academy of Medicine, October 2, 1879. Boston Med & Surg J. 1879;101:527. [Google Scholar]
- Syracuse University College of Medicine. Annual announcement of the College of Physicians and Surgeons of the Syracuse University for the session of 1872–73:5. [Google Scholar]
- Anonymous. The admission of women to the state society. Boston Med & Surg J. 1879;101:527. [Google Scholar]
- Blake JB. From Surgeon General's bookshelf to National Library of Medicine: a brief history. Bull Med Libr Assoc. 1986 Oct; 74(4):318–24. [PMC free article] [PubMed] [Google Scholar]
- Bell WJ. Private physicians and public collections: medical libraries in the United States before 1900. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:91–2. [PubMed] [Google Scholar]
- Purple SS. Medical libraries: an address delivered before the New York Academy of Medicine, January 18, 1877, on taking the chair as president a second term. New York, NY: [s.n.], 1877. [Google Scholar]
- Miller G. Charles David Spivak's role in the development of medical libraries. Trans & Stud Coll Phys Phila. 1974 Jul; 42(1):81–7. [PubMed] [Google Scholar]
- Gould GM.. The union of medical and public libraries. Phila Med J. 1898;2:237–40. [Google Scholar]
- Billings JS. Literature and institutions. In: Clarke EH, Bigelow HJ, Gross SD, Thomas TG, Billings JS, eds. A century of American medicine: 1776–1876. Philadelphia, PA: H. C. Lea, 1876:352. [Google Scholar]
- Anonymous. A medical library association. Boston Med & Surg J. 1875;93:252. [Google Scholar]
- Chadwick JR.. The medical libraries of Boston. Boston Med & Surg J. 1876;95:543–9. [Google Scholar]
- Ferguson ED.. Sixth annual report of the Library Committee of the New York State Medical Association. Trans N Y St Med Assoc. 1890;7:568–83. [Google Scholar]
- Miles WD. A history of the National Library of Medicine: the nation's treasury of medical knowledge. Washington, DC: U.S. Government Printing Office, 1982. [Google Scholar]
- Anonymous. The National Medical Library and the Library of Congress. Med News (Phila) 1883;42:428–30. [Google Scholar]
- Anonymous. The National Medical Library. Med News (Phila) 1883;42:419–20. [Google Scholar]
- Horner F.. A plea for an American medical library. Med & Surg Reporter (Phila) 1878;38:449–50. [Google Scholar]
- Toner JM.. Report on the practicability of establishing a library of American medical works. Trans Amer Med Assoc. 1869;20:117. [Google Scholar]
- Anonymous. The Toner Library. Med News (Phila) 1882;40:561. [Google Scholar]
- Chapman CB. Order out of chaos: John Shaw Billings and America's coming of age. Boston, MA: Boston Medical Library, 1994. [Google Scholar]
- Spivak CD.. The medical libraries of the United States. Phila Med J. 1898;2:852. [Google Scholar]
- Billings JS.. Who founded the National Medical Library? Med Record (NY) 1880;17:298–9. [Google Scholar]
- L[ee] W.. Letter from Washington: medical matters in Washington: National Medical Library. Boston Med & Surg J. 1878;99:705–9. [Google Scholar]
- Shrady GF. The National Medical Library. Med Record (NY) 1876;11:447–8. [Google Scholar]
- Shrady GF. The National Medical Library. Med Record (NY) 1878;13:211–2. [Google Scholar]
- Gross SD.. Appropriation for the Library of the Surgeon-General's Office and Medical Museum. Med News (Phila) 1883;42:563. [Google Scholar]
- Reeves JS.. The Army Medical Museum and Library. Med Record (NY) 1883;23:544–5. [Google Scholar]
- Bell WJ. Private physicians and public collections: medical libraries in the United States before 1900. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:96–7. [PubMed] [Google Scholar]
- Huntington AT.. The medical library movement in the United States. Med Libr & Hist J. 1904;2:120. [PMC free article] [PubMed] [Google Scholar]
- Dondale MF. Medical libraries. In: Doe J, Marshall ML, eds. Handbook of medical library practice. Chicago, IL: Medical Library Association and American Library Association, 1956:5. [Google Scholar]
- Browning W.. Medical libraries. Phila Med J. 1899;3:1124–5. [Google Scholar]
- Dondale MF. Medical libraries. In: Doe J, Marshall ML, eds. Handbook of medical library practice. Chicago, IL: Medical Library Association and American Library Association, 1956:5. [Google Scholar]
- Chadwick JR.. The Boston Medical Library. Med Libr & Hist J. 1903;1:128. [PMC free article] [PubMed] [Google Scholar]
- Lipscomb CE. The library as laboratory. Bull Med Libr Assoc. 2001 Jan; 89(1):79–80. [PMC free article] [PubMed] [Google Scholar]
- Lucker JK. The evolution of research library buildings. Comput Meth Prog Bio. 1994 Sep; 44(3–4): 155–60. [DOI] [PubMed] [Google Scholar]
- Huntington AT.. The medical library movement in the United States. Med Libr & Hist J. 1904;2:128. [PMC free article] [PubMed] [Google Scholar]
- Holmes B.. The medical library for the medical school or the small community. Bull Amer Acad Med. 1895–1897;2:247–301. [Google Scholar]
- Spivak CD.. How every town may secure a medical library. Med News (NY) 1897;71:443–4. [Google Scholar]
- Gould GM.. Medical journalism and medical libraries. Phila Med J. 1898;1:1071–2. [Google Scholar]
- Browning W.. Medical libraries. Phila Med J. 1899;3:1124–1125. [Google Scholar]
- Spivak. The medical libraries of the United States, 71:852–3. [Google Scholar]
- Gould GM.. The organization and support of public medical libraries. Bull Amer Acad Med. 1897–1899;3:148–9. [Google Scholar]
- Connor J. Guardians of medical knowledge: the genesis of the Medical Library Association. Lanham, MD: Medical Library Association and Scarecrow Press, 2000. [Google Scholar]
- Anonymous. The history of the Medical Library Association. Bull Med Libr Assoc. 1911 Jul; 1(1):7. [PMC free article] [PubMed] [Google Scholar]
- Flexner A. Medical education in the United States and Canada: a report to the Carnegie Foundation for the Advancement of Teaching. New York, NY: The Carnegie Foundation, 1910:82. [Google Scholar]
- Weiskotten HG, Schwitalla AM, Cutter WD, and Anderson HH. Medical education in the United States, 1934–1939. Chicago, IL: American Medical Association, Council on Medical Education and Hospitals, 1940:88. [Google Scholar]
- Dondale MF. Medical libraries. In: Doe J, Marshall ML, eds. Handbook of medical library practice. Chicago, IL: Medical Library Association and American Library Association, 1956:13. [Google Scholar]
- Chadwick JR.. Medical libraries: their development and use. Boston Med & Surg J. 1896;134:104. [Google Scholar]
- Boston Medical Library Association. Special Meeting, Tuesday, November 29, 1898 [to plan the raising of funds for a new building]. Boston Med & Surg J. 1899. 140:16–21. [Google Scholar]
- Chadwick. The Boston Medical Library, 134:134–5. [Google Scholar]
- Belleh GS, Akhigbe OO. The impact of economic issues on Nigerian health sciences libraries. Bull Med Libr Assoc. 1991 Jul; 79(3):288–94. [PMC free article] [PubMed] [Google Scholar]
- Williams TL, Lemkau HL, and Burrows S. The economics of academic health sciences libraries: cost recovery in the era of big science. Bull Med Libr Assoc. 1988 Oct; 76(4):317–22. [PMC free article] [PubMed] [Google Scholar]
- Williams TL, Lemkau HL, and Burrows S. The economics of academic health sciences libraries: cost recovery in the era of big science. Bull Med Libr Assoc. 1988 Oct; 76(4):317. [PMC free article] [PubMed] [Google Scholar]
- Bloomquist H. The status and needs of medical school libraries in the United States. J Med Educ. 1963 Mar; 38(3):145–63. [PubMed] [Google Scholar]
- Koudelka JB. The genesis of the William H. Welch Medical Library and the Johns Hopkins Institute of the History of Medicine. In: Stevenson LG, ed. A celebration of medical history. Baltimore, MD: Johns Hopkins, 1982:69–76. [PubMed] [Google Scholar]
- Wannarka M. Medical collections in public libraries of the United States: a brief historical study. Bull Med Libr Assoc. 1968 Jan; 56(1):1–14. [PMC free article] [PubMed] [Google Scholar]