

Abstract
Background
The post cardiac arrest syndrome (PCAS) is responsible for the majority of in-hospital deaths following cardiac arrest (CA). The major elements of PCAS are anoxic brain injury and circulatory failure.
Objective
This study aimed to investigate the clinical characteristics of circulatory failure and inflammatory responses after out-of-hospital cardiac arrest (OHCA) and to identify patterns of circulatory and inflammatory responses, which may predict circulatory deterioration in PCAS.
Methods
This study is a single-center cohort study of 50 patients who receive intensive care after OHCA. The patients are followed for 5 days where detailed information from circulatory variables, including measurements by pulmonary artery catheters (PACs), is obtained in high resolution. Blood samples for inflammatory and endothelial biomarkers are taken at inclusion and thereafter daily. Every 10 min, the patients will be assessed and categorized in one of three circulatory categories. These categories are based on mean arterial pressure; heart rate; serum lactate concentrations; superior vena cava oxygen saturation; and need for fluid, vasoactive medications, and other interventions. We will analyze predictors of circulatory failure and their relation to inflammatory biomarkers.
Results
Patient inclusion started in January 2016.
Conclusions
This study will obtain advanced hemodynamic data with high resolution during the acute phase of PCAS and will analyze the details in circulatory state transitions related to circulatory failure. We aim to identify early predictors of circulatory deterioration and favorable outcome after CA.
Trial Registration
ClinicalTrials.gov: NCT02648061; https://clinicaltrials.gov/ct2/show/NCT02648061 (Archived by WebCite at http://www.webcitation.org/6wVASuOla)
Keywords: out-of-hospital cardiac arrest, critical care, hemodynamics, inflammation, biomarkers
Introduction
Post Cardiac Arrest Syndrome
Recent advances in cardiopulmonary resuscitation (CPR) have improved the chance of successful return of spontaneous circulation (ROSC) after cardiac arrest (CA) [1,2]. This implies that patients, who previously died during CPR, now obtain ROSC and are admitted to hospitals for further treatment. However, in-hospital mortality is unchanged at around 50% to 70% [3-5]. The post cardiac arrest syndrome (PCAS) is responsible for the majority of in-hospital deaths after CA. PCAS includes (1) brain injury, (2) myocardial dysfunction, and (3) systemic ischemia and reperfusion injury. In addition, the pathological process that caused the CA and other chronic diseases influences the clinical course of PCAS. Circulatory support after CA usually follows recommendations similar to those used for treatment of septic shock [6-9]. Septic shock and PCAS share some characteristics and experiences from the treatment of septic shock, such as emphasis on oxygen deliverance, which may be useful [10,11]. However, PCAS is a different clinical entity than septic shock, and circulatory failure after CA may have special characteristics [4]. This is exemplified by the need to perfuse the postischemic brain without unnecessary strain on the postischemic heart.
Inflammation and Circulatory Failure
Circulatory failure after CA is both due to cardiac etiologies and systemic inflammatory response elicited by the hypoxic insult and reperfusion, but the relative contribution of each factor is unknown. The balance between pro- and anti-inflammatory cytokine signals is important in the development of organ failure [12]. Several studies have explored cytokine plasma concentrations as biomarkers for severity, risk of organ failure, and mortality in sepsis [13-15]. By comparison, only 4 studies in humans, with data from 2 patient populations, have evaluated the inflammatory response in PCAS [10,16-18], and 2 studies have explored the endothelial activation and injury in relation to inflammation in PCAS [18,19]. Furthermore, none of these studies specifically investigated the relationship between endothelial injury, inflammatory response, and circulatory failure.
In a cohort study from 2002, 73 out of 165 normothermic patients treated for out-of-hospital cardiac arrest (OHCA) developed circulatory instability, with median onset 6.8 hours after OHCA. [20]. Low cardiac output (CO) and filling pressures characterized the circulatory instability. The CO improved after 24 hours but superimposed vasodilatation developed, requiring fluid administration and use of vasoactive medications. Most patients recovered within 3 days, and hemodynamic status did not predict neurologic outcome [20]. In a Norwegian study, these results were confirmed in hypothermic CA patients [21]. In contrast, in the Target Temperature Management Trial, which randomized CA patients to either 33°C or 36°C, the circulation of patients in both groups were characterized by vasoconstriction [5,22,23]. However, the variables in studies on circulatory failure after CA are highly dependent on the use of vasoactive medications, and some studies are difficult to interpret because of limited information about the use of these medications.
Rationale for a New Study
The International Liaison Committee on Resuscitation consensus statement from 2008 acknowledges the lack of knowledge about optimal treatment of PCAS and how to best deliver circulatory support after CA [4].
This protocol describes a study aimed to investigate patients with ROSC after OHCA, regarding (1) characteristics of circulatory failure in PCAS; (2) the endothelial and inflammatory response in PCAS; and (3) the relationship between circulatory failure and the inflammatory and endothelial response in PCAS.
Methods
Research Questions
This study will address the following research questions:
What are the characteristics of circulatory failure in PCAS?
What are the characteristics of transitions between different clinical circulatory states during PCAS?
What is the inflammatory response measured by inflammatory and endothelial biomarkers in PCAS?
Which clinical characteristics and biomarkers predict changes in clinical circulatory states?
Study Design
This study is a single-center, prospective, observational cohort study.
Setting
The study will take place at the intensive care unit (ICU) and the coronary care unit (CCU) at the St. Olav’s University Hospital, a tertiary referral university hospital in Trondheim, Norway, with a catchment population of 700,000.
Eligibility
Inclusion
All adult patients who are admitted to either the ICU or the CCU with obtained ROSC after OHCA will be considered for inclusion. Inclusion is performed immediately after arrival to the ICU or CCU.
Exclusion Criteria
Exclusion criteria are age <18 years, CA of septic or anaphylactic origin, sepsis within 24 hours before CA, pregnant women, transferred from other hospitals after OHCA, and decision to not initiate life-sustaining therapy after hospital arrival.
Censoring
Patients are censored from further follow-up if the patient undergoes acute cardiothoracic surgery or intervention with extracorporeal membranous oxygenation support or a ventricular assist device, at the time of death, if life-prolonging therapy is withdrawn or withheld, or when the patient is transferred to a general ward or another hospital. The reason for censoring is recorded, and all data obtained until censoring will be included in the analysis.
Sample Size
This is an observational study, and the frequency of abnormal biomarkers, circulatory states, and endpoints are largely unknown; therefore, no formal sample size calculation has been performed [24]. On the basis of a sample size from similar studies describing pathophysiology, we aim at including 50 patients [21,25].
Routine Post Cardiac Arrest Syndrome Treatment
General Consideration
The treatment of the patients is decided by the physician in charge and will not be changed due to the participation in the study. The routine treatment after OHCA at St. Olav’s University Hospital will be applied unless there are specific indications for alternative strategies. Routine care is briefly outlined below.
Specific Cardiac Interventions
For OHCA suspected to be caused by disease in the coronary arteries, procedures for revascularization are routinely considered and performed if decided by the cardiologist. All use of medications for cardiac diseases and for anticoagulation is decided by the cardiologist in charge of treatment.
Therapeutic Hypothermia
According to the current practice at St. Olav’s University Hospital, the target temperature is usually 36°C. Active temperature management is performed for 24 hours.
Sedation and Analgesia
Sedation is initiated with either propofol or midazolam, and analgesia with either fentanyl or remifentanil. Sedation is titrated to Motor Activity Assessment Scale (MAAS) 0-1 during active temperature management and later titrated to the lowest dose achieving adequate patient comfort [26]. A muscle relaxant, cisatracurium, is not routinely used, but initiated if shivering during cooling or rewarming, and if needed to achieve adequate ventilation.
Cardiovascular Support
The primary treatment goal for circulatory support is to ensure adequate circulation, as evaluated by clinical examination (eg, tachycardia, pallor, cold skin, capillary refill), a mean arterial blood pressure (MAP) ≥65 mm Hg, and a urine output of ≥0.5 mL·kg−1·h−1. Generally, circulatory optimization is achieved through fluid and vasopressor administration after the following algorithm: in the presence of hypotension and/or tachycardia, the first step is to assess signs of tissue hypoperfusion (eg, cold, clammy skin and extremities, prolonged capillary refill time, diminished urine output, increasing lactate and decreasing base excess, decreasing central/mixed venous oxygenation, and if not sedated—deteriorating mental status). If the physician suspects tissue hypoperfusion, volume status is assessed through the presence of stroke volume variation >10% (pulsus paradoxus) and/or echocardiographic assessment of the heart and the inferior caval vein. If increased preload is indicated, repeated fluid boluses of 250 mL are given until cardiac output (CO) does not respond. If a fluid load is not indicated or does not improve the perfusion, vasoactive medication is administered. The standard vasoactive medications are norepinephrine and/or dobutamine, depending on whether vasoconstrictive and/or inotropic effects are indicated. If the vasoplegia is not improved by a high dose of norepinephrine (≥0.5 μg·kg−1·min−1), vasopressin (0.4 mU·kg−1·min−1) is considered.
Respiratory Support
Ventilation is administered by a SERVOi ventilator (Maquet Siemens, Germany). Ventilation is either pressure controlled or pressure supported for patients who have adequate spontaneous ventilation. The ventilator settings are adjusted to a positive end-expiratory pressure (PEEP) level, which give the best arterial oxygen partial pressure (PaO2)/fraction of inspired oxygen (FiO2) ratio (usually PEEP is set at 8 cm H2 O at the start of ventilation), a plateau pressure to give a tidal volume of 6-8 mL/kg, a respiratory rate to give a PaCO2 within the normal range, and a FiO2 to give a O2 saturation above 95%. Tracheostomy is considered for patients who are difficult to wean from mechanical respiratory support, usually on days 8-10 of the ICU or CCU stay.
Nutrition
No nutrition is given on the day of arrival to the ICU or CCU. Enteral nutrition is given as soon as possible in increasing doses (from 500 kcal/day to 1000 kcal/day to 2000 kcal/day). If enteral nutrition is not feasible or nutrition targets cannot be reached within approximately 4 to 6 days, total parenteral nutrition is gradually introduced on the fourth day (25 kcal·kg−1·day−1). Before nutrition is started, the patients receive glucose 100 g/daily. Metabolic control of blood sugar is aimed at 5-10 mmol/L by a continuous infusion of insulin. Patients who use insulin on a regular basis will receive insulin at all times, and hypoglycemia is corrected with increased glucose or nutrition administration.
Infection Control
Antibiotics are not given routinely, but they are introduced if there is a clinical suspicion of an infection.
Assessment of Hypoxic Cerebral Injury
Assessment of hypoxic cerebral injury is primarily based on the combination of clinical signs, serum neuron-specific enolase concentrations, and neurophysiological examination of somatosensory evoked potentials. Other examinations, for example, magnetic resonance imaging, are performed when required. The evaluation of potential hypoxic cerebral injury is usually initiated on the third or fourth day after CA.
Intensive Care Unit Procedures
Airway suction is routinely performed once daily to secure patent airway and as needed if there are signs of excessive airway secretions. Airway suction is performed with a 10, 12, or 14 French scale catheter (depending on endotracheal tube size) through a closed suction system.
Shift of position is routinely performed every third hour.
Spontaneous breathing trials (SBTs) are considered in patients who have spontaneous respiration, airway patency, reversal of the cause of respiratory failure, no uncontrolled infection or metabolic disturbance, heart rate <120, systolic BP 90-180 mm Hg, oxygen saturation >90%, FiO2 <0.5, and positive end-expiratory pressure (PEEP) ≤8 cmH2 O. The SBT is performed using pressure-supported ventilation with inspiratory pressure support of approximately 8 cmH2 O and PEEP 6-8 cmH2 O for 10-30 min.
Study Procedure
Screening and Recruitment
Patients will be screened for eligibility and recruited at the time they are admitted to the ICU or CCU for intensive care after OHCA (Figure 1).
Figure 1.
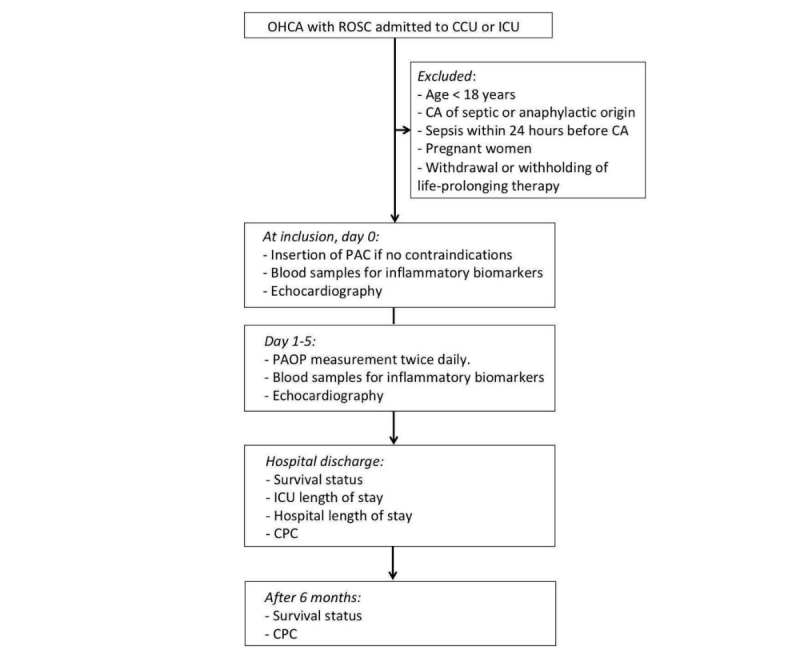
Flowchart summarizing patient enrollment and main study procedures. OHCA: out-of-hospital cardiac arrest; ROSC: return of spontaneous circulation; CCU: coronary care unit; ICU: intensive care unit; CA: cardiac arrest; PAC: pulmonary artery catheter; PAOP: pulmonary artery occlusion pressure; CPC: cerebral performance category.
Demographic and clinical data will be extracted from the patient’s medical records and documentation from emergency medical service (EMS) personnel involved in the treatment of CA. Registrations of clinical variables, as part of routine critical care from the time of ICU/CCU arrival until inclusion, will be used.
If there is no contraindication to insert a pulmonary artery catheter (PAC), the catheter is inserted as early as possible after inclusion.
Baseline Variables
At time of inclusion the following variables will be registered:
Patient characteristics: age, sex, ethnicity, weight, height, and premorbid cerebral performance category (CPC) [27,28]
Charlson Comorbidity Index [29]
Characteristics related to the CA (Utstein Style Template) [30]: location, witnessed arrest, time of emergency call, bystander CPR, time of EMS personnel arrival, initial monitored rhythm, time to first defibrillation, time to ROSC, presumed cardiac or noncardiac etiology, and medications given during or after CPR. End-tidal CO2 results, if applied
Temperature at admission
Known pulmonary aspiration during CPR
Interventions
Registrations During the Study Period
Clinical data are registered in the electronic ICU chart, Picis Critical Care Manager (Optum Inc, USA). After inclusion, the following variables will be recorded:
At the time of inclusion and every minute:
Basic vital measurements: heart rate and rhythm, invasive arterial blood pressure, pulmonary artery pressure, mixed venous oxygen saturation (SvO2, calibrated twice daily), central venous blood pressure, peripheral transcutaneous oxygen saturation, and temperature
Central hemodynamic measurements: CO and systemic vascular resistance (SVR), and corresponding indexed values (related to body-surface area)
Respiratory support: ventilator mode, respiratory rate, FiO2, minute ventilation, PEEP, and plateau pressure
At the time of inclusion and every following hour:
Fluid balance: fluid administrations, transfusions, and urine output
All medications
At the time of inclusion and every sixth hour:
Arterial blood gas analysis, including electrolytes
MAAS score
After 24 hours:
Simplified acute physiology score (SAPS) II [31]
At the time of inclusion and twice daily:
Pulmonary artery occlusion pressure
Central venous and mixed venous blood gas
At the time of inclusion and daily:
Standardized echocardiographic evaluation performed by a trained cardiologist
Intra-abdominal pressure
Clinical chemistry: white blood count, thrombocyte count, creatinine, blood urea nitrogen, C-reactive protein, troponin-T, probrain natriuretic peptide, bilirubin, albumin, and haptoglobin
Blood samples for inflammatory and endothelial biomarkers
Modified clinical pulmonary infection score (CPIS) [32]
Sequential organ failure assessment (SOFA) score [33]
Glasgow Coma Score [34]
Percutaneous coronary intervention, dialysis, and/or aorta balloon pump
Results from chest x-ray or other diagnostic imaging tools ordered during the hospital stay
Other events during the study period (eg, arrhythmias and seizures)
Biomarkers
As part of the study, we will establish a biobank for analysis of inflammatory and endothelial biomarkers. Blood samples will be taken at inclusion and every morning the 5 following days. After gentle mixing, the blood samples are placed vertical for 30 min in ambient temperature, and then centrifuged at 2200 g for 10 min. The supernatants are stored at −80°C within 1 hour from the time of sampling. During the study period, additional full blood will be drawn and stored at −80°C.
We will analyze the following biomarkers: interleukin (IL)-1β, IL-1 receptor antagonist (IL1-ra), IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12 (p70), IL-13, IL-15, IL-17, eotaxin, basic fibroblast growth factor, granulocyte-colony stimulating factor, granulocyte macrophage colony stimulating factor, interferon γ, interferon-inducible protein 10, monocyte chemotactic protein 1, macrophage inflammatory protein 1α and 1β, platelet derived growth factor-BB, regulated upon activation T cell expressed and secreted, tumor necrosis factor, vascular endothelial growth factor, syndecan-1, sE-selectin, heparan sulfate, hyaluronic acid, soluble trombomodulin, and sVE-cadherin. Other biomarkers of interest, identified later, may be included in the final analysis.
Follow-Up After Discharge From Hospital
Follow-up after discharge from the hospital will include the following:
ICU length of stay.
Hospital length of stay.
Survival status at hospital discharge and after 6 months.
CPC at hospital discharge and after 6 months.
Ethical Considerations
Research on critically ill patients, who are sedated or comatose and, therefore, not able to provide consent, calls for special ethical considerations. For the study, it is vital that clinical information is obtained from the initial critical stage of the disease. This study will not increase the overall risk for the patients, and the study is justifiable according to the World Medical Association’s Declaration of Helsinki regarding Ethical Principles for Medical Research Involving Human Subjects, June 1964, and its later amendments [35]. We will include patients in the study when they are admitted to the ICU/CCU and at the earliest feasible moment ask for consent from their relatives. Patients, who regain competency to give an informed consent, will later be asked for a deferred consent. This procedure is approved by the Regional Committee for Medical and Health Research Ethics, Central-Norway Health Region (REK Midt, No. 2015/1807).
Assessment of Safety
Besides establishing and calibrating PAC (Swan-Ganz CCOmbo, Edward Lifescience, USA) and drawing blood for analysis of inflammatory biomarkers at a maximum of 5 time points, the study does not involve other interventions differing from routine care after OHCA. The insertion of PAC induces some benefits and some risks. One of the benefits is the potential of improved circulatory monitoring and support, including a more precise administration of fluids and vasoactive medications. However, complications related to the placement of PAC have also been reported. In a Cochrane report, PAC was neither found to increase mortality or length of stay in the ICU or the hospital (high-quality evidence according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system for both the findings). The Acute Decompensated Heart Failure Syndromes Registry compared 502 patients with decompensated heart failure and PAC with 502 controls [36] and observed that the risk of all-cause death was lower in the PAC group than the control group (hazard ratio 0.3, 95% confidence interval (CI) 0.13-0.7). In a large study from Leipzig where 3730 patients with PAC who underwent cardiac surgery, only 0.1% experienced serious complications [37], a similar rate as transesophageal echocardiography (0.2%) [38]. The nursing-staff at ICU and CCU are trained in PAC care and extra lectures in PAC use will be given before and during the study. Only doctors, competent of PAC use, will perform measurements of pulmonary artery wedge pressure. We believe that the patients included will experience neither benefit nor harm by participating in this study.
Statistical Analysis Plan
Statistical Methods
Descriptive data are presented with either median or interquartile range, or mean with 95% CI, as appropriate. For missing observation of physiological variables (eg, blood pressure), a value corresponding to the mean of the observation before and after this time point will be applied. For biomarkers, the value 0 is attributed if a result is below the detection limits of the assay. Statistical analyses will be performed using Stata or R.
Circulatory State Transitions During Post Cardiac Arrest Syndrome
During critical illness, most patients go through different states of hemodynamic stability. We have categorized the circulatory state after CA in 3 different categories based on data obtained from routine care (Table 1). Every 10 min, a patient is classified according to the least favorable measurement at that time (eg, isolated MAP of 40 mm Hg is sufficient to classify a patient to have severely disturbed circulation).
Table 1.
Circulatory states.
| Variables | Circulation | ||
| Undisturbed | Disturbed | Severely disturbed | |
| Mean arterial pressure, mm Hg | ≥65 | 45-64 | <45 |
| Heart rate, bpm | 51-100 | <50, 101-130 | ≤40, >130 |
| Lactate, mmol/L | <2 | 2–4 | >4 |
| ScvO2, % | ≥65 | 50-64 | <50 |
| Fluid resuscitation, L/hours | <0.5 | 0.5-1.9 | ≥2 |
| Norepinephrine, μg·kg−1·min−1 | <0.1 | 0.1-0.29 | ≥0.3 |
| Dobutamine, μg·kg−1·min−1 | No | <10 | ≥10 |
| Vasopressin | No | No | Yes |
| Epinephrine | No | No | Yes |
| Levosimedan | No | No | Yes |
| Aorta balloon pump | No | No | Yes |
We will validate the appropriateness of the defined categories against the cardiac index.
Patients may go back and forth between the clinical states, defined in Table 1, corresponding to the severity of their illness and its progression (Figure 2), and the changes from one clinical state to another will be recorded. By using survival analysis methodology, we allow for right censoring, which means that the information from patients with limited follow-up time can be included in the analyses. A patient who is in a certain clinical state at time t might remain in the same state or change to one of 2 others at time t +1. In such multi-endpoint settings, the clinical states compete with each other, and the transitions over time are best studied with methods developed for competing risk analyses.
Figure 2.
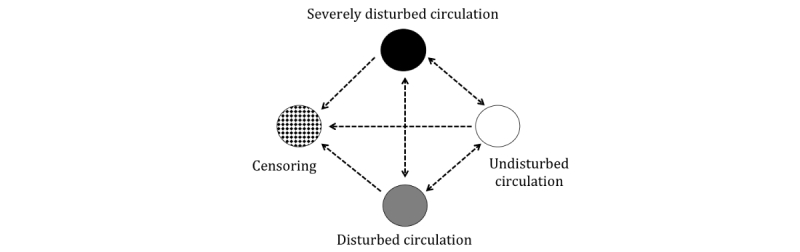
Possible transitions between circulatory states.
The Kaplan-Meier estimator accurately estimates the transition from one state to another, assuming that these 2 states describe all possible states. To be useful in a competing risk framework, the Kaplan-Meier estimator has been generalized into a matrix version, called the Aalen-Johansen estimator. To describe when, in time, most state transitions occur (ie, transition intensity), we will use the Nelson-Aalen estimator. The Nelson-Aalen estimator is a nonparametric estimator of the “cumulative hazard” of a given event, and it can be applied in a multi-state model.
Patterns Predictive of Deterioration in Circulatory State
We anticipate that not all patients will follow the same circulatory trajectory; during the study, some will deteriorate and some will improve in circulatory status, and during our observation, many will have several state transitions. We plan to analyze events before deteriorations to identify patterns of circulatory and inflammatory response measurements predictive of clinical state deteriorations. These patterns will be compared with those in patients who improve their circulatory status or remain unchanged.
To explore the predictive value of previous measurements to foresee a clinical deterioration, we will use 2 different approaches. The outcome variable will be dichotomized to deterioration versus no deterioration (status quo or improvement). First, we will test different timelags between measurements and deteriorations to see which is more informative (eg, 1 hour, 2 hours, 3 hours). For this analytic approach, we will use univariable and multivariable logistic regression. Second, we will use methods from survival analysis to assess continuous alterations in covariates on the outcome. For this analysis, we will use Aalen’s linear model, which is an intensity regression model. Variables from the 2 groups will also be explored in respect to its relation to mortality and CPC at discharge from hospital.
Relation Between Distributive Shock and Inflammatory Biomarkers
We will study the relationship between alterations in inflammatory and endothelial biomarkers and the changes in SVR, in CO, and the need for fluid replacement. As described above, patients with hypotension and low SVR will be treated with norepinephrine. Therefore, we will analyze potential independent biomarkers and other predictors of SVR adjusted for a dose of norepinephrine.
Vasoplegia might also occur as part of an infection, and CA patients are prone to aspiration and pneumonia after CPR. Therefore, we will calculate modified CPIS daily to describe how many patients develop clinical pneumonia.
Circulatory failure might also be due to structural heart defects (eg, mitral valve insufficiency). An experienced cardiologist will perform echocardiogram daily to assess the heart’s function.
Results
Patient inclusion started in January 2016.
Discussion
Rationale for This Study
This study will describe the hemodynamic and inflammatory response characteristics of circulatory failure in PCAS. On the basis of the findings, we will develop a prediction model for risk of circulatory failure in PCAS.
PACS after CA is frequent, and it is strongly associated with mortality after CA [4]. However, there is relatively limited information about the detailed circulatory disturbances in PACS, and principles for circulatory supports are partly transferred from other conditions, in particular, in the treatment of septic shock. Moreover, the expected course (eg, improvement or deterioration) of the circulation is not well understood. The clinical trajectory may be 2-phased: first, a low CO state, followed by a low peripheral resistance state, as previously proposed [20]. Alternatively, it may be one-phased: predominantly caused by either an isolated cardiac failure or an isolated vasoplegia. It is also not established which patients are at a higher risk for circulatory failure in the acute phase of PCAS.
Standard critical illness classification systems, such as SAPS II, SAPS III, acute physiology and chronic health evaluation (APACHE) II, SOFA, or New Early Warning (NEW) scores, are not applicable to describe circulatory changes during the acute phase of PCAS. SAPS and APACHE scores are developed to define risk at admission. SOFA and NEWS scores will reach a ceiling effect and not be able to differentiate between various degrees of circulatory failure in this population. Some researchers have used an extended SOFA circulatory score where 4 further increments are added to the standard circulatory SOFA score [39]. However, this score only includes arterial blood pressure and use of vasopressors, which may not encompass all relevant observations for circulatory stability. Therefore, this study classifies the patients into 3 circulatory groups: undisturbed, disturbed, or severely disturbed circulation based upon predefined values of mean blood pressure, heart rate, serum lactate concentration, ScvO2, use of fluid, vasoactive drugs, and the need for mechanical circulatory devices. Cut-off values were based upon relevant guidelines and clinical practice. All variables were selected because of their known relevance to circulatory failure and because they are easily available during routine monitoring of critically ill patients. More precise measures such as CO or SvO2 were not included, as these are usually not obtained in patients after CA.
The clinical trajectories in the acute phase of PCAS are heterogeneous, as seen from the lack of circulatory stability. Such changes can occur immediately after admittance to the ICU or later, at any time, in the clinical course. Thus, the patients are at constant risk. Limited information exists regarding the factors to identify which patients are at the highest risk of imminent clinical circulatory failure. Such factors may include characteristics of the CA episode or clinical observations in the ICU.
This study will establish which factors—demographic, CA-related variables, or clinical observations— will predict circulatory failure and, thus, assess circulatory stability during PCAS.
Expected Limitations
We recognize some limitations in this protocol. First, the study will obtain information about long-term outcomes and survival. However, this information will only be used to describe the cohort because of the limited number of patients. It would be of interest to study whether circulatory stability and inflammation during PCAS can also predict long-term outcomes, but such analyses should be done in larger cohorts. Second, this study is a single-center study, which limits the generalization of the findings. Third, the included patients are expected to have considerable variability in demographics and comorbidities, in characteristics of the CA, and thus also in PACS complications (eg, infections). Nevertheless, this is presumably the case in all PACS cohorts, and potential findings must be robust to such confounders to be of potential clinical use.
Conclusions
This study will obtain longitudinally advanced hemodynamic observations with high resolution during the acute phase of PCAS, and it will analyze the details of clinical transitions related to circulatory failure. Additionally, this study will also examine the relationship between inflammatory and endothelial biomarkers and circulatory failure in PCAS.
Acknowledgments
This work is funded by a research grant from the Norwegian University of Science and Technology and St. Olav’s University Hospital (Samarbeidsorganet HMN-NTNU).
Abbreviations
- APACHE
acute physiology and chronic health evaluation
- CA
cardiac arrest
- CCU
coronary care unit
- CO
cardiac output
- CPC
cerebral performance category
- CPIS
clinical pulmonary infection score
- CPR
cardiopulmonary resuscitation
- EMS
emergency medical service
- FiO2
fraction of inspired oxygen
- ICU
intensive care unit
- IL
interleukin
- MAAS
Motor Activity Assessment Scale
- MAP
arterial blood pressure
- NEW
new early warning
- OHCA
out-of-hospital cardiac arrest
- PAC
pulmonary artery catheter
- PCAS
post cardiac arrest syndrome
- PEEP
positive end-expiratory pressure
- ROSC
return of spontaneous circulation
- SAPS
simplified acute physiology score
- SBT
spontaneous breathing trials
- SOFA
sequential organ failure assessment
- SVR
systemic vascular resistance
- TBCS
transitions between circulatory states
Footnotes
Conflicts of Interest: None declared.
References
- 1.Hazinski MF, Nolan JP, Billi JE, Böttiger BW, Bossaert L, de Caen AR, Deakin CD, Drajer S, Eigel B, Hickey RW, Jacobs I, Kleinman ME, Kloeck W, Koster RW, Lim SH, Mancini ME, Montgomery WH, Morley PT, Morrison LJ, Nadkarni VM, O'Connor RE, Okada K, Perlman JM, Sayre MR, Shuster M, Soar J, Sunde K, Travers AH, Wyllie J, Zideman D. Part 1: Executive summary: 2010 International Consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010 Oct 19;122(16 Suppl 2):S250–75. doi: 10.1161/CIRCULATIONAHA.110.970897. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=20956249. [DOI] [PubMed] [Google Scholar]
- 2.Wissenberg M, Lippert FK, Folke F, Weeke P, Hansen CM, Christensen EF, Jans H, Hansen PA, Lang-Jensen T, Olesen JB, Lindhardsen J, Fosbol EL, Nielsen SL, Gislason GH, Kober L, Torp-Pedersen C. Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out-of-hospital cardiac arrest. J Am Med Assoc. 2013 Oct 02;310(13):1377–84. doi: 10.1001/jama.2013.278483. [DOI] [PubMed] [Google Scholar]
- 3.Botha J, O'Brien Y, Malouf S, Cole E, Ansari ES, Green C, Tiruvoipati R. The outcome and predictors of mortality in patients therapeutically cooled postcardiac arrest. J Intensive Care Med. 2016 Oct;31(9):603–10. doi: 10.1177/0885066614566792. [DOI] [PubMed] [Google Scholar]
- 4.Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Vanden HT. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008 Dec 2;118(23):2452–83. doi: 10.1161/CIRCULATIONAHA.108.190652. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=18948368. [DOI] [PubMed] [Google Scholar]
- 5.Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H, TTM Trial Investigators Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013 Dec 05;369(23):2197–206. doi: 10.1056/NEJMoa1310519. [DOI] [PubMed] [Google Scholar]
- 6.Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent J, Moreno R, Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013 Feb;39(2):165–228. doi: 10.1007/s00134-012-2769-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M, Early Goal-Directed Therapy Collaborative Group Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 08;345(19):1368–77. doi: 10.1056/NEJMoa010307. [DOI] [PubMed] [Google Scholar]
- 8.Gaieski DF, Band RA, Abella BS, Neumar RW, Fuchs BD, Kolansky DM, Merchant RM, Carr BG, Becker LB, Maguire C, Klair A, Hylton J, Goyal M. Early goal-directed hemodynamic optimization combined with therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest. Resuscitation. 2009 Apr;80(4):418–24. doi: 10.1016/j.resuscitation.2008.12.015. [DOI] [PubMed] [Google Scholar]
- 9.Jones AE, Shapiro NI, Kilgannon JH, Trzeciak S, Emergency Medicine Shock Research Network (EMSHOCKNET) investigators Goal-directed hemodynamic optimization in the post-cardiac arrest syndrome: a systematic review. Resuscitation. 2008 Apr;77(1):26–9. doi: 10.1016/j.resuscitation.2007.10.021. [DOI] [PubMed] [Google Scholar]
- 10.Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, Fraisse F, Dinh-Xuan AT, Carli P, Spaulding C, Dhainaut J, Cavaillon J. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002 Jul 30;106(5):562–8. doi: 10.1161/01.cir.0000023891.80661.ad. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=12147537. [DOI] [PubMed] [Google Scholar]
- 11.Adrie C, Laurent I, Monchi M, Cariou A, Dhainaou J, Spaulding C. Postresuscitation disease after cardiac arrest: a sepsis-like syndrome? Curr Opin Crit Care. 2004 Jun;10(3):208–12. doi: 10.1097/01.ccx.0000126090.06275.fe. [DOI] [PubMed] [Google Scholar]
- 12.Cho S, Choi J. Biomarkers of sepsis. Infect Chemother. 2014 Mar;46(1):1–12. doi: 10.3947/ic.2014.46.1.1. https://www.icjournal.org/DOIx.php?id=10.3947/ic.2014.46.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bozza FA, Salluh JI, Japiassu AM, Soares M, Assis EF, Gomes RN, Bozza MT, Castro-Faria-Neto HC, Bozza PT. Cytokine profiles as markers of disease severity in sepsis: a multiplex analysis. Crit Care. 2007;11(2):R49. doi: 10.1186/cc5783. https://ccforum.biomedcentral.com/articles/10.1186/cc5783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kellum JA, Kong L, Fink MP, Weissfeld LA, Yealy DM, Pinsky MR, Fine J, Krichevsky A, Delude RL, Angus DC, GenIMS Investigators Understanding the inflammatory cytokine response in pneumonia and sepsis: results of the Genetic and Inflammatory Markers of Sepsis (GenIMS) Study. Arch Intern Med. 2007;167(15):1655–63. doi: 10.1001/archinte.167.15.1655. http://europepmc.org/abstract/MED/17698689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pinsky MR, Vincent JL, Deviere J, Alegre M, Kahn RJ, Dupont E. Serum cytokine levels in human septic shock. Relation to multiple-system organ failure and mortality. Chest. 1993 Feb;103(2):565–75. doi: 10.1378/chest.103.2.565. [DOI] [PubMed] [Google Scholar]
- 16.Bro-Jeppesen J, Kjaergaard J, Wanscher M, Nielsen N, Friberg H, Bjerre M, Hassager C. The inflammatory response after out-of-hospital cardiac arrest is not modified by targeted temperature management at 33 °C or 36 °C. Resuscitation. 2014 Nov;85(11):1480–7. doi: 10.1016/j.resuscitation.2014.08.007. [DOI] [PubMed] [Google Scholar]
- 17.Bro-Jeppesen J, Kjaergaard J, Wanscher M, Nielsen N, Friberg H, Bjerre M, Hassager C. Systemic inflammatory response and potential prognostic implications after out-of-hospital cardiac arrest: a substudy of the target temperature management trial. Crit Care Med. 2015 Jun;43(6):1223–32. doi: 10.1097/CCM.0000000000000937. [DOI] [PubMed] [Google Scholar]
- 18.Bro-Jeppesen J, Johansson PI, Hassager C, Wanscher M, Ostrowski SR, Bjerre M, Kjaergaard J. Endothelial activation/injury and associations with severity of post-cardiac arrest syndrome and mortality after out-of-hospital cardiac arrest. Resuscitation. 2016 Oct;107:71–9. doi: 10.1016/j.resuscitation.2016.08.006. [DOI] [PubMed] [Google Scholar]
- 19.Fink K, Schwarz M, Feldbrügge L, Sunkomat JN, Schwab T, Bourgeois N, Olschewski M, von zur Mühlen C, Bode C, Busch H. Severe endothelial injury and subsequent repair in patients after successful cardiopulmonary resuscitation. Crit Care. 2010;14(3):R104. doi: 10.1186/cc9050. https://ccforum.biomedcentral.com/articles/10.1186/cc9050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Laurent I, Monchi M, Chiche J, Joly L, Spaulding C, Bourgeois B, Cariou A, Rozenberg A, Carli P, Weber S, Dhainaut J. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002 Dec 18;40(12):2110–6. doi: 10.1016/s0735-1097(02)02594-9. https://linkinghub.elsevier.com/retrieve/pii/S0735109702025949. [DOI] [PubMed] [Google Scholar]
- 21.Hovdenes J, Laake JH, Aaberge L, Haugaa H, Bugge JF. Therapeutic hypothermia after out-of-hospital cardiac arrest: experiences with patients treated with percutaneous coronary intervention and cardiogenic shock. Acta Anaesthesiol Scand. 2007 Feb;51(2):137–42. doi: 10.1111/j.1399-6576.2006.01209.x. [DOI] [PubMed] [Google Scholar]
- 22.Bro-Jeppesen J, Annborn M, Hassager C, Wise MP, Pelosi P, Nielsen N, Erlinge D, Wanscher M, Friberg H, Kjaergaard J, TTM Investigators Hemodynamics and vasopressor support during targeted temperature management at 33°C Versus 36°C after out-of-hospital cardiac arrest: a post hoc study of the target temperature management trial*. Crit Care Med. 2015 Feb;43(2):318–27. doi: 10.1097/CCM.0000000000000691. [DOI] [PubMed] [Google Scholar]
- 23.Bro-Jeppesen J, Hassager C, Wanscher M, Østergaard M, Nielsen N, Erlinge D, Friberg H, Køber L, Kjaergaard J. Targeted temperature management at 33°C versus 36°C and impact on systemic vascular resistance and myocardial function after out-of-hospital cardiac arrest: a sub-study of the Target Temperature Management Trial. Circ Cardiovasc Interv. 2014 Oct;7(5):663–72. doi: 10.1161/CIRCINTERVENTIONS.114.001556. http://circinterventions.ahajournals.org/cgi/pmidlookup?view=long&pmid=25270900. [DOI] [PubMed] [Google Scholar]
- 24.Norman G, Monteiro S, Salama S. Sample size calculations: should the emperor's clothes be off the peg or made to measure? Br Med J. 2012 Aug 23;345:e5278. doi: 10.1136/bmj.e5278. [DOI] [PubMed] [Google Scholar]
- 25.Gando S, Nanzaki S, Morimoto Y, Kobayashi S, Kemmotsu O. Out-of-hospital cardiac arrest increases soluble vascular endothelial adhesion molecules and neutrophil elastase associated with endothelial injury. Intensive Care Med. 2000 Jan;26(1):38–44. doi: 10.1007/s001340050009. [DOI] [PubMed] [Google Scholar]
- 26.Devlin J, Boleski G, Mlynarek M, Nerenz D, Peterson E, Jankowski M, Horst H, Zarowitz B. Motor Activity Assessment Scale: a valid and reliable sedation scale for use with mechanically ventilated patients in an adult surgical intensive care unit. Crit Care Med. 1999 Jul;27(7):1271–5. doi: 10.1097/00003246-199907000-00008. [DOI] [PubMed] [Google Scholar]
- 27.Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975 Mar 01;1(7905):480–4. doi: 10.1016/s0140-6736(75)92830-5. [DOI] [PubMed] [Google Scholar]
- 28.- A randomized clinical trial of calcium entry blocker administration to comatose survivors of cardiac arrest. Design, methods, and patient characteristics. The Brain Resuscitation Clinical Trial II Study Group. Control Clin Trials. 1991 Aug;12(4):525–45. doi: 10.1016/0197-2456(91)90011-a. [DOI] [PubMed] [Google Scholar]
- 29.Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994 Nov;47(11):1245–51. doi: 10.1016/0895-4356(94)90129-5. [DOI] [PubMed] [Google Scholar]
- 30.Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, Bossaert LL, Brett SJ, Chamberlain D, de Caen AR, Deakin CD, Finn JC, Gräsner J, Hazinski MF, Iwami T, Koster RW, Lim SH, Ma MH, McNally BF, Morley PT, Morrison LJ, Monsieurs KG, Montgomery W, Nichol G, Okada K, Ong MEH, Travers AH, Nolan JP, Utstein Collaborators Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015 Nov;96:328–40. doi: 10.1016/j.resuscitation.2014.11.002. [DOI] [PubMed] [Google Scholar]
- 31.Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. J Am Med Assoc. 1993;270(24):2957–63. doi: 10.1001/jama.270.24.2957. [DOI] [PubMed] [Google Scholar]
- 32.Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000 Aug;162(2 Pt 1):505–11. doi: 10.1164/ajrccm.162.2.9909095. [DOI] [PubMed] [Google Scholar]
- 33.Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996 Jul;22(7):707–10. doi: 10.1007/BF01709751. [DOI] [PubMed] [Google Scholar]
- 34.Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974 Jul 13;2(7872):81–4. doi: 10.1016/s0140-6736(74)91639-0. [DOI] [PubMed] [Google Scholar]
- 35.WMA. [2018-01-03]. WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects Internet http://www.wma.net/en/30publications/10policies/b3/index.html . [PubMed]
- 36.Sotomi Y, Sato N, Kajimoto K, Sakata Y, Mizuno M, Minami Y, Fujii K, Takano T, investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) Registry Impact of pulmonary artery catheter on outcome in patients with acute heart failure syndromes with hypotension or receiving inotropes: from the ATTEND Registry. Int J Cardiol. 2014 Mar 01;172(1):165–72. doi: 10.1016/j.ijcard.2013.12.174. [DOI] [PubMed] [Google Scholar]
- 37.Bossert T, Gummert JF, Bittner HB, Barten M, Walther T, Falk V, Mohr FW. Swan-Ganz catheter-induced severe complications in cardiac surgery: right ventricular perforation, knotting, and rupture of a pulmonary artery. J Card Surg. 2006;21(3):292–5. doi: 10.1111/j.1540-8191.2006.00235.x. [DOI] [PubMed] [Google Scholar]
- 38.Kallmeyer IJ, Collard CD, Fox JA, Body SC, Shernan SK. The safety of intraoperative transesophageal echocardiography: a case series of 7200 cardiac surgical patients. Anesth Analg. 2001 May;92(5):1126–30. doi: 10.1097/00000539-200105000-00009. [DOI] [PubMed] [Google Scholar]
- 39.Annborn M, Bro-Jeppesen J, Nielsen N, Ullén S, Kjaergaard J, Hassager C, Wanscher M, Hovdenes J, Pellis T, Pelosi P, Wise MP, Cronberg T, Erlinge D, Friberg H, TTM-trial investigators The association of targeted temperature management at 33 and 36°C with outcome in patients with moderate shock on admission after out-of-hospital cardiac arrest: a post hoc analysis of the Target Temperature Management trial. Intensive Care Med. 2014 Sep;40(9):1210–9. doi: 10.1007/s00134-014-3375-8. [DOI] [PubMed] [Google Scholar]