

ABSTRACT
Preservation of an intact labrum and reconstruction of a deficient or worn acetabular labrum are accepted techniques in modern hip surgery. If the remaining labrum is very thin, its intact tip can be preserved and its volume restored with a ligamentum teres graft. Technique and preliminary results of this augmentation technique are presented. Labral augmentation was performed in 16 hips (11 rights) in 16 patients (7 males, mean age 29 years) during surgical dislocation for treatment of femoroacetabular impingement. The acetabular index, lateral center edge angle, asphericity angle and acetabular retroversion index were determined on preoperative X-rays and magnetic resonance imaging. The pre- and postoperative Merle d’Aubigné and Postel score (MdA) was calculated and the Oxford Hip Score (OHS) obtained after 1 year. There were seven Grade 1 and nine Grade 0 hips (Tönnis classification). Mean lateral center edge was 29°. The mean acetabular index was 1.85°. Mean asphericity angle was 62.5°. Mean acetabular retroversion index was 23.4%. Mean MdA improved from 14.5 preoperatively to 17 at 1 year (P < 0.0001). Mean OHS after 1 year was 42. Previous surgery was a risk factor for inferior results: OHS was 44.5 in hips without versus 26 in hips with previous surgery. Mean MdA improved from 15 to 17.5 in patients without previous surgery versus 14 to 16 for the group with previous surgery. Augmentation of the labrum using ligamentum teres shows good clinical results after 1 year. Patients with previous hip surgery had inferior results.
INTRODUCTION
The acetabular labrum enlarges the acetabular surface and provides additional stability to the hip joint [1]. While animal studies suggested that regeneration of the labrum after partial excision to the bone is possible, there seems to be no such potential for regeneration in humans [2]. In joint preserving hip surgery, the labrum is usually reattached to the acetabulum with bone anchors when it is torn or degenerated [3]. If the remaining labrum is too thin or extensively damaged, treatment options include resection or reconstruction with grafts. Most techniques for labral reconstruction use auto- or allografts to replace the original labrum. Different studies report good clinical outcomes regarding hip function, patient satisfaction and reduction of pain after labral reconstruction. While long-term results are still missing, preservation or reconstruction of the labrum is nowadays recommended by most authors in order to preserve its function as a stabilizer of the hip joint [4].
Recent studies focussing on the suction seal effect of the labrum underline the importance of an intact labrum regarding intraarticular fluid pressurization. Pressurization of the interstitial fluid within the cartilage protects the cartilage from load, while pressurization of the intraarticular fluid decreases friction between the acetabulum and the femoral head [5–7]. It has been shown that labral tears lead to a reduction in fluid pressurization in the hip joint. The group of Philippon et al. demonstrated that intra-articular fluid pressure is increased by labral repair while it is drastically reduced after partial or complete labral resection [8]. In an experimental setting, reconstruction of the labrum with iliotibial band autograft lead to an intra-articular fluid pressurization similar to a normal hip with an intact labrum [9, 10]. The same can be expected when restoration of the suction seal can be achieved by labral augmentation using the ligamentum capitis femoris.
There are concerns that with segmental reconstruction of the labrum the hoop stress cannot be restored because of the interruption of the circumferential fibres. The rationale of this technique is that with the preservation of the intact tip of the labrum the hoop stress capability is maintained and the sealing effect of the labrum is improved by adding volume with a graft of the ligamentum teres between the bony rim and the preserved part of the labrum [11]. We present the technique and the preliminary results after 1 year.
MATERIALS AND METHODS
From April 2013 to December 2015, we performed labral augmentation with ligamentum teres in 16 hips (11 rights) in 16 patients (7 males, mean age 29 years) during surgical dislocation for the treatment of femoroacetabular impingement (FAI). Indication for surgery was symptomatic FAI syndrome with groin pain and typical radiographic findings as it has been stated in the Warwick Agreement on FAI syndrome [12]. The indication for labral augmentation was a thin (1–2 mm) labrum which seemed to provide an insufficient seal without additional augmentation. The final decision whether labral augmentation was necessary or not was made intraoperatively. Routine preoperative diagnostics included an ap pelvic X-ray, lateral cross-table view of the hip and MR arthrography. The joint degeneration was graded according to the Tönnis classification for osteoarthritis. The acetabular index (AI), the lateral center edge (LCE) angle, and the acetabular retroversion index (ARI) were measured on the conventional radiographs preoperatively [13]. The preoperative asphericity angle (AA) was measured on the radial sequences of the MR arthrography and on the cross-table view conventional radiograph. Measurement of the AI, LCE and AA was repeated on the postoperative X-rays that included an ap pelvic view and a lateral cross-table view of the hip. The type of impingement was classified as pincer, cam or combined. An asphericity angle >55° was considered a cam-deformity. A pincer impingement was defined by an LCE >35° or a retroversion index of more than 33%. Intraoperatively, the type of acetabular damage and labral damage was graded according to Beck (Tables I and II) [14].
Table I.
Beck classification of cartilage damage
| Beck classification of cartilage damage | ||
|---|---|---|
| Grade | Description | Criteria |
| 0 | Normal | Macroscopically sound cartilage |
| 1 | Malacia | Roughening of surface, fibrillation |
| 2 | Debonding | Loss of fixation to subchondral bone, macroscopically sound cartilage; carpet phenomenon |
| 3 | Cleavage | Loss of fixation to subchondral bone, frayed edge, thinning of the cartilage, flap |
| 4 | Defect | Full-thickness defect |
Table II.
Beck classification of labral damage
| Beck classification of labral damage | ||
|---|---|---|
| Grade | Description | Criteria |
| 0 | Normal | Macroscopically sound labrum |
| 1 | Degeneration | Thinning or localized hypertrophy, fraying, discoloration |
| 2 | Full-thickness tear | Complete avulsion from the acetabular rim |
| 3 | Detachment | Separation between acetabular and labral cartilage, preserved attachment to bone |
| 4 | Ossification | Osseous metaplasia, localized or circumferential |
Radiographic and clinical follow-up was done at 6 weeks and 1 year postoperatively. The Merle d’Aubigné and Postel score (MdA) was calculated preoperatively and at the 1 year follow-up. A score of 15–18 indicates a good to excellent result, 12–14 a fair result and less than 12 points a poor result [15]. The Oxford Hip Score (OHS) was obtained at the 1 year follow-up with a score higher than 40 indicating an acceptable result [16]. One patient developed neurologic problems related to a neurogenic tumor during the follow-up period. In this patient, the OHS was not acquired.
Surgical technique
In all cases, surgery was performed by the same surgeon (M.B.). After performing a surgical dislocation with the technique of Ganz et al. [17], the ligamentum teres is resected from the fovea of the femoral head. Adherent fatty tissue and the synovial cover are removed from the ligament. It is then cut longitudinally in the center leaving a small hinge in the middle, yielding a graft twice as long as the original ligament with a width of 4–5 mm. The labrum is then sharply detached from the acetabulum and trimming of the bony acetabulum is performed as needed. The ligamentum teres graft is sutured in between the acetabulum and the remaining labrum using bone anchors (Fig. 1). Detachment of the labrum and augmentation with the ligamentum teres graft is shown in the intraoperative photographs (Figs 2–5). After correction of the offset on the femur, the femoral head is reduced and the hip tested for stability and impingement-free motion. If the suction seal is restored after the labral augmentation, a characteristic suction seal sound can be heard when trying to dislocate the hip again. At the end of surgery, the joint capsule is closed loosely and the greater trochanter reattached with two 3.5 mm screws. There were no intraoperative complications. All trochanters healed during the follow-up period. The postoperative rehabilitation protocol included partial weight bearing with 15 kg for 4 weeks and increasing weight bearing during the following 2 weeks as tolerated. The range of motion was limited to 90° of flexion, 20° internal and external rotation for the first 4 weeks and gradually increased thereafter. A continuous passive motion machine was applied from the first day after surgery and the hip was regularly mobilized on a stationary bike after discharge from the hospital during the first 6 weeks. Three patients had screw removal at the greater trochanter. One patient had an additional hip arthroscopy for removal of intraarticular adhesions 1 year after surgery. After the second surgery, the residual pain improved, but not completely. In none of the hips any signs of disturbed wound healing or infection were noted.
Fig. 1.
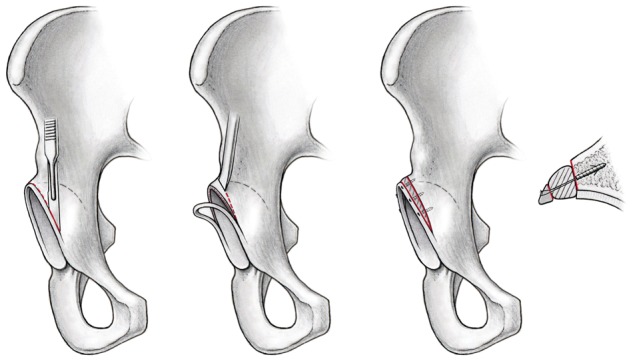
The degenerated labrum is detached from the acetabulum. Rim trimming is performed if necessary. The labrum is then augmented with the ligamentum teres graft and reattached with bone anchors.
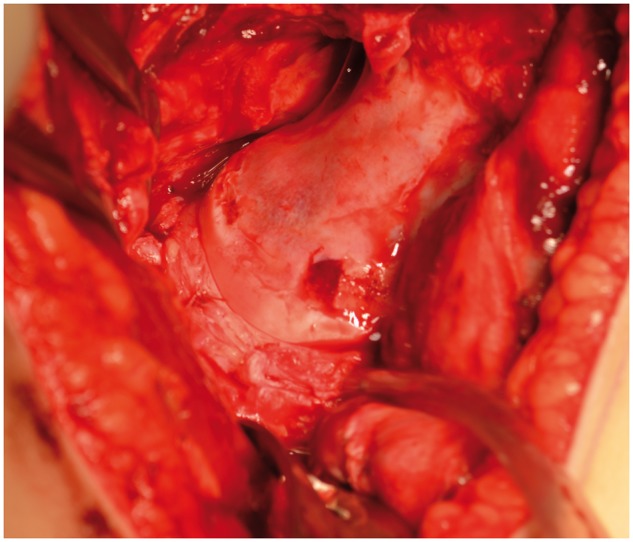
Fig. 2.
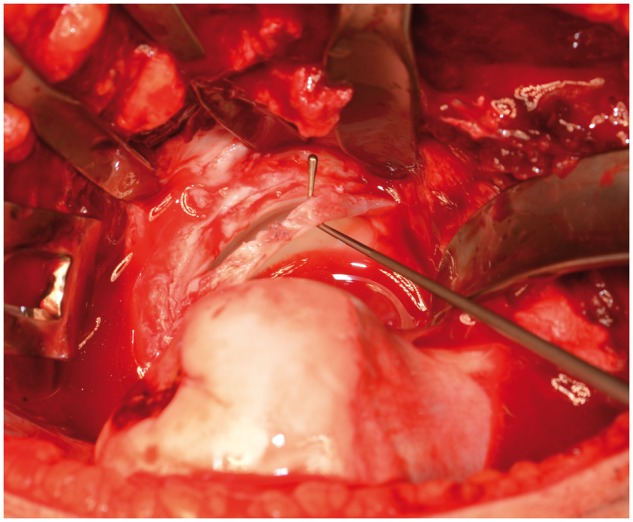
Intraoperative photograph showing the detached labrum.
Fig. 3.
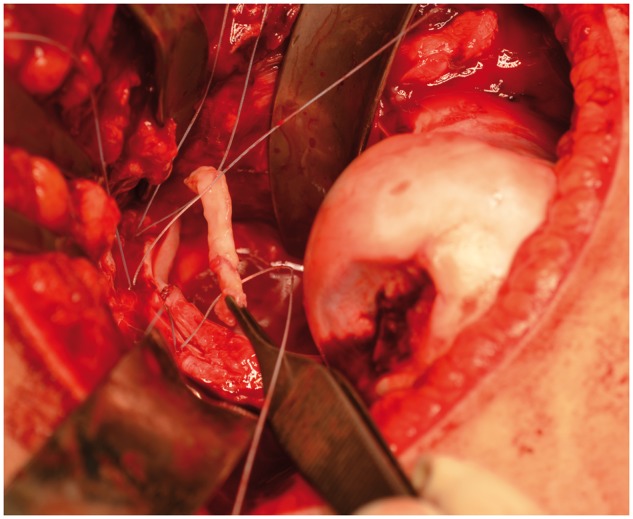
Intraoperative photograph. The ligamentum teres graft is sutured between the labrum and the acetabular rim.
Fig. 4.
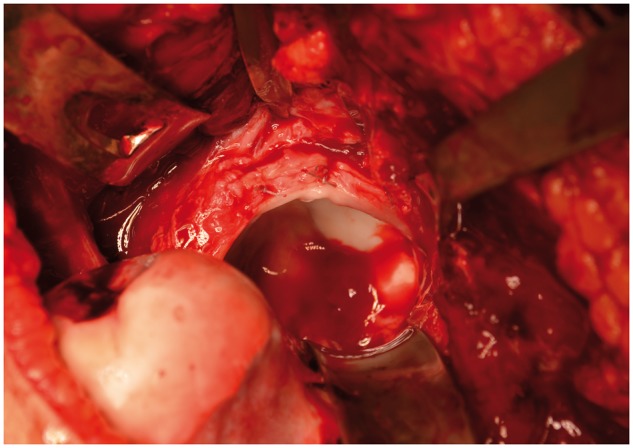
Intraoperative photograph with the ligamentum teres graft in its final position.
Fig. 5.
Intraoperative photograph after reduction of the femoral head.
RESULTS
Patients’ demographic data and the results of the measurements and clinical sores are summarized in Table III. Of the 16 hips included in this study, 10 hips had a cam morphology with an asphericity angle >55°. One hip only showed characteristics of a pincer impingement with the LCE >35° and ARI >33% and five hips were combined impingement hips. There were seven Grade 1 and nine Grade 0 hips according to the Tönnis classification for osteoarthritis. Four hips had previous surgery (three hip arthroscopy, one had two previous hip arthroscopies and a periacetabular osteotomy).
Table III.
Patient demographics and results of radiographic measurements and clinical scores
| Patient | Age | Gender | Side | FAI | Tönnis grade | Cartilage —Beck | Labrum —Beck | AI (°) | LCE (°) | ARI (%) | AA pre (MRI) (°) | AA pre (X-ray) (°) | AI postop (°) | LCE post (°) | AA post (X-ray) (°) | MdA pre | MdA post | OHS post | Previous surgeries |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 27 | M | Right | Cam | 0 | 0 | 1 | 10 | 26 | 31 | 62 | 40 | 10 | 24 | 37 | 14 | 17 | 42 | Arthroscopy |
| 2 | 18 | F | Right | Mixed | 0 | 0 | 4 | −1 | 28 | 38 | 68 | 43 | 0 | 25 | 42 | 15 | 18 | 35 | 0 |
| 3 | 40 | F | Right | Cam | 1 | 3 | 3 | −1 | 31 | 14 | 73 | 43 | 4 | 27 | 43 | 13 | 11 | 17 | Arthroscopy |
| 4 | 35 | M | Left | Cam | 1 | 3 | 4 | 5 | 26 | 15 | 65 | 55 | 9 | 23 | 51 | 16 | 18 | 45 | 0 |
| 5 | 23 | M | Left | Cam | 1 | 3 | 1 | 8 | 25 | 25 | 80 | 67 | 12 | 23 | 47 | 15 | 17 | a | Arthroscopy |
| 6 | 30 | M | Right | Mixed | 1 | 0 | 1 | −1 | 35 | 6 | 59 | 62 | 1 | 33 | 42 | 13 | 18 | 44 | 0 |
| 7 | 16 | F | Right | Mixed | 0 | 0 | 1 | 1 | 42 | 36 | 65 | 40 | 3 | 34 | 40 | 15 | 18 | 48 | 0 |
| 8 | 19 | F | Right | Pincer | 0 | 0 | 1 | −3 | 39 | 32 | 52 | 46 | 4 | 25 | 40 | 14 | 15 | 26 | Arthroscopy, PAO |
| 9 | 29 | F | Left | Cam | 0 | 0 | 2 | 5 | 29 | 20 | 61 | 50 | 7 | 28 | 50 | 14 | 15 | 29 | 0 |
| 10 | 35 | F | Right | Cam | 0 | 3 | 1 | 2 | 29 | 22 | 62 | 59 | 4 | 27 | 42 | 15 | 17 | 47 | 0 |
| 11 | 34 | M | Right | Cam | 1 | 3 | 4 | 2 | 27 | 30 | 63 | 55 | 2 | 26 | 46 | 16 | 18 | 47 | 0 |
| 12 | 26 | M | Right | Mixed | 1 | 3 | 1 | 3 | 36 | 14 | 106 | 56 | 1 | 28 | 50 | 15 | 17 | 46 | 0 |
| 13 | 36 | F | Left | Cam | 0 | 0 | 1 | 9 | 29 | 35 | 56 | 53 | 9 | 23 | 42 | 14 | 18 | 48 | 0 |
| 14 | 26 | F | Right | Mixed | 1 | 0 | 1 | −1 | 36 | 40 | 61 | 54 | 3 | 28 | 45 | 13 | 17 | 36 | 0 |
| 15 | 31 | F | Right | Cam | 0 | 0 | 1 | 0 | 33 | 5 | 55 | 51 | 2 | 27 | 44 | 15 | 17 | 34 | 0 |
| 16 | 31 | M | Left | Cam | 0 | 3 | 1 | 7 | 28 | 20 | 74 | 58 | 8 | 26 | 45 | 14 | 17 | 34 | 0 |
MRI, magnetic resonance imaging.
aOHS not acquired in one patient due to tumor-related neurologic problems newly developed during the follow up period.
The mean LCE was 29° (SD 4.9, range 25–39). The mean AI was 1.85° (SD 3.9, range −0.5 to 9.9). The mean AA was 62.5° (SD 12.4, range 52–106). The mean ARI was 23.4% (SD 10.8, range 6.4–40.0). The MdA score improved from mean 14.5 (SD 0.93, range 13–16) preoperatively to 17 (SD 1.75, range 11–18) at 1 year (P < 0.0001) (Fig. 6). The main improvement in the MdA score was due to a reduction of pain with good walking ability and hip ROM pre- and postoperatively. The mean OHS after 1 year was 42 (SD 9.1, range 17–48).
Fig. 6.

Boxplot of the pre- and postoperative Merle d’Aubigné and Postel score.
Previous surgery was a risk factor for inferior results. Hips without previous surgery had a mean OHS of 44.5 (SD 6.6, range 29–48) versus 26 (SD 10.3, range 17–42) in the hips with previous surgery at the 1 year follow-up. Regarding the MdA score, the mean score improved from 15 (SD 1.0, range 13–16) preoperatively to 17.5 (SD 0.8, range 17–18) in Group 1 without previous surgery versus 14 (SD 0.7, range 13–15) to 16 (SD 2.4, range 11–17) for Group 2 with previous surgery (Fig. 7). Whether this is statistically significant was not calculated because of the small sample size (four hips) with previous surgery.
Fig. 7.

Boxplot diagram comparing the pre- and postoperative MdA score for Group 1 (with previous surgery) and Group 2 (no previous surgery).
DISCUSSION
The principle findings of this study are (i) that labral augmentation with ligamentum capitis femoris can adequately restore the labrum and its sealing function and (ii) that this technique yields good clinical results after 1 year. Both arthroscopic and open impingement surgery aim to treat the underlying pathology of patients with FAI. Besides correcting the cam deformity on the femoral neck and trimming the bony acetabulum for correction of the pincer deformity, the labral pathology has to be addressed adequately. Labral degeneration occurs at different stages and can be observed more often in the pincer and combined impingement population than in patients with pure cam impingement [18]. A number of recent studies have focused on the suction seal effect of the labrum. It is hypothesized that an intact labrum, besides giving primary stability to the hip adds to additional stability through this suction seal effect. When distraction forces act upon the hip joint, a negative fluid pressure in the articular fluid is created, thus giving additional stability between the femoral head and the acetabulum. This negative fluid pressurization can only function when the seal that is created by the labrum is intact [9]. It has been shown that the integrity of the labral seal can be restored by means of labral reconstruction [5, 8, 9]. For this, open and arthroscopic techniques have been advocated, most of them using a graft to reconstruct the deficient labrum.
While labral reconstruction replaces a section of the damaged labrum in its full thickness, the labral augmentation technique preserves part of the original labrum, which was shown previously to be intact [11]. The tip of the damaged labrum is preserved and augmented by a graft. The rationale of the technique is (i) to maintain the hoop stress capability by preserving the intact tip of the labrum and (ii) to improve the sealing effect of the labrum by adding volume to it. This is achieved by placing a ligamentum teres graft between the bony rim and the preserved part of the labrum. The ligamentum teres is an ideal graft for this as it can easily be harvested during surgical hip dislocation and has no additional morbidity. An alternative source for a graft that can be used in the same way is the fascia lata. With the open approach, the restoration of the suction seal effect can be easily controlled by dislocating the hip again after performing the augmentation. A characteristic vacuum sound is heard if the seal is restored correctly. This gives additional confirmation of a technically good reconstruction. The open technique also allows to readjust graft and suture placement in order to achieve a functional reconstruction.
We observed inferior results regarding the clinical outcomes in the patient group with previous hip surgery. In all patients who had hip arthroscopies with cam resection and labral refixation before, we saw a variable degree of intraarticular adhesions. In two cases, the offset correction was not carried out completely by the arthroscopic procedure. In one patient, the magnetic resonance imaging revealed extensive intraarticular adhesions and a recurrence of the offset pathology as well as additional osteophytes at the femoral head–neck junction 1 year after hip arthroscopy. In the same patient, the actabular labrum was clumsy with an insufficient suction seal. After open surgery with labral augmentation, the residual pain resolved to some degree and clinical scores improved. However, we suspect that the inferior results in these four patients might be related to the formation of intraarticular adhesions and to the incomplete correction of the deformity which in turn led to a persistence of FAI symptoms and progression of cartilage damage. 50% of patients in this group had OA Grade 1, while only 42% had Grade 1 OA in the group with no previous surgery. Obviously, the patients with previous surgeries had a longer history of hip pain before the labral augmentation was performed. In this context, it can be discussed if a certain degree of chronification of pain could add to the inferior results in this group.
Our results regarding the clinical scores are comparable to the clinical outcome reported in a previous study that used the ligamentum capitis femoris for labral reconstruction instead of labral augmentation [19].
Limitations of the study are due to its retrospective nature. The study group consists of a relatively small number of patients and has a limited follow-up period. We did not include a control group. On one hand, it would be difficult to compare the results of our study group to another patient group requiring surgical hip dislocation. Also, we did not aim to compare our results to other techniques. The purpose of this study was to present the technique of labral augmentation using the ligamentum teres and to report on our initial results after 1 year. The results are based on the adequate restoration of the suction seal which is directly tested intraoperatively and on clinical results. However, there are no objective tests to report on the effect of the labral augmentation on the restoration of the suction seal.
The intraoperative findings after performing labral augmentation with the technique described demonstrated an adequate restoration of the suction seal. The overall clinical results after a 1 year follow-up were good. When compared with patients without previous surgery, patients who had undergone failed joint preserving hip surgery before had inferior results.
ACKNOWLEDGEMENT
We thank K. Oberli for creation of the line drawings.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1. Bsat S, Frei H, Beaulé PE.. The acetabular labrum. Bone Joint J 2016; 98-B: 730–5. [DOI] [PubMed] [Google Scholar]
- 2. Miozzari HH, Celia M, Clark JM. et al. No regeneration of the human acetabular labrum after excision to bone. Clin Orthop Relat Res 2015; 473: 1349–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Espinosa N, Beck M, Rothenfluh DA. et al. Treatment of femoro-acetabular impingement: preliminary results of labral refixation. J Bone Joint Surg Am 2007; 89: 36–53. [DOI] [PubMed] [Google Scholar]
- 4. Haddad B, Konan S, Haddad FS.. Debridement versus re-attachment of acetabular labral tears: a review of the literature and qualitative analysis. Bone Joint J 2014; 96-B: 24–30. [DOI] [PubMed] [Google Scholar]
- 5. Cadet ER, Chan AK, Vorys GC. et al. Investigation of the preservation of the fluid seal effect in the repaired, partially resected, and reconstructed acetabular labrum in a cadaveric hip model. Am J Sports Med 2012; 40: 2218.. [DOI] [PubMed] [Google Scholar]
- 6. Ferguson SJ, Bryant JT, Ganz R. et al. An in vitro investigation of the acetabular labral seal in hip joint mechanics. J Biomech 2003; 36: 171–8. [DOI] [PubMed] [Google Scholar]
- 7. Ferguson SJ, Bryant JT, Ganz R. et al. The acetabular labrum seal: a proroelastic finite element model. Clin Biomech 2000; 15: 463–8. [DOI] [PubMed] [Google Scholar]
- 8. Nepple JJ, Philippon MJ, Campbell KJ. et al. The hip fluid seal - Part II: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surg Sports Traumatol Arthrosc 2014; 22: 730–6. [DOI] [PubMed] [Google Scholar]
- 9. Philippon MJ, Nepple JJ, Campbell KJ. et al. The hip fluid seal - Part I: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip fluid pressurization. Knee Surg Sports Traumatol Arthrosc 2014; 22: 722–9. [DOI] [PubMed] [Google Scholar]
- 10. Philippon MJ, Briggs KK, Hay CJ. et al. Arthroscopic labral reconstruction in the hip using iliotibial band autograft: technique and early outcomes. Arthroscopy 2010; 26: 750–6. [DOI] [PubMed] [Google Scholar]
- 11. Ito K, Leunig M, Ganz R.. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004; 429: 262–71. [DOI] [PubMed] [Google Scholar]
- 12. Griffin DR, Dickenson EJ, O'Donnell J. et al. The Warwick agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med 2016; 50: 1169–76. [DOI] [PubMed] [Google Scholar]
- 13. Beck M, Kalhor M, Leunig M. et al. Hip morphology influences the pattern of damage to the acetabular cartilage. J Bone Joint Surg Br 2005; 87: 1012–8. [DOI] [PubMed] [Google Scholar]
- 14. Tannast M, Siebenrock KA, Anderson SE.. Femoroacetabular impingement: radiographic diagnosis - what the radiologist should know. AJR 2007; 188: 1540–52. [DOI] [PubMed] [Google Scholar]
- 15. D’Aubigné RM, Postel M.. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg Am 1954; 36:451–75. [PubMed] [Google Scholar]
- 16. Murray DW, Fitzpatrick R, Rogers K. et al. The use of the Oxford hip and knee scores. J Bone Joint Surg Br 2007; 89: 1010–4. [DOI] [PubMed] [Google Scholar]
- 17. Ganz R, Gill TJ, Gautier E. et al. Surgical dislocation of the adult hip. J Bone Joint Surg Br 2001; 83: 1119–24. [DOI] [PubMed] [Google Scholar]
- 18. Beck M, Leunig M, Parvizi J. et al. Anterior femoroacetabular impingement: mid- term results of surgical treatment. Clin Orthop 2004; 418: 67–73. [PubMed] [Google Scholar]
- 19. Camenzind RS, Steurer-Dober I, Beck M.. Clinical and radiographical results of labral reconstruction. J Hip Preserv Surg; 2: 401–9. [DOI] [PMC free article] [PubMed] [Google Scholar]