

Abstract
Background
Based on successive Health Interview Surveys (HIS), it has been demonstrated that also in Belgium obesity, measured by means of a self-reported body mass index (BMI in kg/m2), is a growing public health problem that needs to be monitored as accurately as possible. Studies have shown that a self-reported BMI can be biased. Consequently, if the aim is to rely on a self-reported BMI, adjustment is recommended. Data on measured and self-reported BMI, derived from the Belgian Food Consumption Survey (FCS) 2014 offers the opportunity to do so.
Methods
The HIS and FCS are cross-sectional surveys based on representative population samples. This study focused on adults aged 18–64 years (sample HIS = 6545 and FCS = 1213). Measured and self-reported BMI collected in FCS were used to assess possible misreporting. Using FCS data, correction factors (measured BMI/self-reported BMI) were calculated in function of a combination of background variables (region, gender, educational level and age group). Individual self-reported BMI of the HIS 2013 were then multiplied with the corresponding correction factors to produce a corrected BMI-classification.
Results
When compared with the measured BMI, the self-reported BMI in the FCS was underestimated (mean 0.97 kg/m2). 28% of the obese people underestimated their BMI. After applying the correction factors, the prevalence of obesity based on HIS data significantly increased (from 13% based on the original HIS data to 17% based on the corrected HIS data) and approximated the measured one derived from the FCS data.
Conclusions
Since self-reported calculations of BMI are underestimated, it is recommended to adjust them to obtain accurate estimates which are important for decision making.
Keywords: Body mass index, Self-reporting, Validity, Misclassification, Correction
Background
Obesity is major public health problem [1–4]. Epidemiological studies have shown that a body mass index (BMI, the most commonly used indicator for relative weight among adults [5]) of 25–30 kg/m2 increases the risk of morbidity (cardiovascular diseases, type 2 diabetes and some types of cancer) and mortality [3, 4, 6]. A BMI of 30 or higher will further increase these risks [7]. In light of this growing problem, it is necessary to measure and monitor the prevalence of obesity in the general population as accurate as possible [4]. According to the national Health Interview Survey (HIS) of 2013 14% of the Belgian population can be considered as obese. Moreover, since the first survey in 1997, this proportion has increased with 27% [8].
The BMI calculated in the HIS is based on self-reported height and weight collected by means of a questionnaire. Such an approach is commonly used in large epidemiological studies [9–12] because collecting self-reported data is more feasible and less expensive than collecting objective measurements [2, 13–15]. Nevertheless, the inaccuracy of self-reported data has been well investigated. Generally, participants tend to overestimate their height and to underestimate their weight, in particular those being overweight or obese, resulting in an underestimation of their actual BMI [6, 7, 16–19]. Consequently, those individuals are misclassified into a lower BMI-category which leads to an underestimation of the prevalence of obesity in the population [3, 4, 13, 14, 20, 21]. Social desirability can largely explain this phenomenon and some subpopulation groups (women, youngsters and high educated people) are more prone to it [6, 7, 13, 15, 16, 18, 22]. In Belgium, ‘prevention and health promotion’ is organised at regional level. For policy decisions and prevention programmes, especially in high-risk subpopulations, it is crucial to obtain BMI estimates that are as accurate as possible in order to draw reliable conclusions [23, 24]. If the aim is to continue to rely on self-reported HIS data, it is thus recommended to adjust those estimates so that they approximate measured data [21, 25].
In 2014, a national Food Consumption Survey (FCS) was conducted in Belgium. Both measured and self-reported body height and weight were collected, making it possible to study potential differences between measured and self-reported BMI, and accordingly to estimate the degree of BMI-misclassification. This was an opportunity to investigate reporting bias at national level in Belgium.
The objective of this study is to calculate correction factors based on FCS data by comparing the self-reported and measured BMI and to apply these factors to the self-reported BMI of the HIS. Although studies have stated that correction equations should not be applied across datasets [2, 17, 18], our study assumes that it is feasible in a certain context (e.g. same time span, similar target population and equivalent sampling method). We also assume that the corrected self-reported BMI of the HIS will be more valid, resulting in a more accurate BMI-classification.
Methods
Survey methodology
This study focused on adults aged 18–64 years, since the FCS targeted the Belgian population of 3–64 years and the relative weight of children and youngsters is not yet stable [26]. The HIS and the FCS are both cross-sectional surveys. The last HIS was conducted in 2013, the last FCS in 2014. A sample of the population was selected, targeting all persons residing in Belgium without restriction on their place of birth, nationality or other characteristics. Both surveys used quarterly updates of the National Population Registry as sample frame. A multistage clustered sample design was applied in both surveys involving a geographical stratification, a selection of municipalities within the provinces and of respondents within municipalities. The difference between the two surveys was that in the HIS the respondents were selected at household level (maximum 4 persons per household) and in the FCS at individual level. The use of matched substitution of non-participating respondents/households ensured the realisation of the predefined net-sample size and composition. Proxies were allowed in both studies. The methodology of the HIS has been described by Demarest et al. [27] and that of the FCS by Bel et al. [28]. Both surveys were carried out in line with the Belgian privacy legislation and approved by the ethical committee of Ghent University.
Study populations
In the HIS, a total of 10,829 citizens was interviewed, 6747 of them belonging to the age group 18–64 years. The overall participation rate at household level was 57%. Self-reported body height and weight were collected using a Computer Assisted Personal face-to-face Interview (CAPI) at the participant’s home. The following questions were asked: ‘How tall are you without clothes and shoes? (cm)’ and ‘How much do you weight without clothes? (kg)’. Pregnant women were asked to report their weight before pregnancy. Cases with a missing or invalid height and/or weight were excluded from the analysis (pregnant women could not be excluded). The final HIS sample contained 6545 individuals.
The participation rate of the FCS was 37%. Overall 3297 citizens participated, of which 1270 in the age group 18–64 years. This survey collected both self-reported and measured body height (in cm) and weight (in kg) for the same individuals using a CAPI, also at their home. Trained dieticians were used as interviewers and to gather the measured data. During the first 24-h food recall interview, body height and weight were self-reported. Participants were informed that their height and weight would be measured during the second home visit. The time lapse between the first and the second home visit was minimal 2 and maximal 4 weeks. During the second home visit, the anthropometric measurements were taken following a standardized protocol. The respondents were measured with light clothes and without shoes. Height was accurately measured to 0.5 cm using a stadiometer (type SECA 213 (Seca gmbh & co. kg, Hamburg, Germany)) and weight to 0.1 kg using an electronic scale (type SECA 815 and 804 (Seca gmbh & co. kg, Hamburg, Germany)). After excluding pregnant women and cases with a missing or invalid self-reported/measured height and/or weight, the study sample comprised 1213 individuals.
Background variables
Studies have demonstrated that demographic, cultural and social characteristics of a population can influence the accuracy of self-reported data [3, 4, 7, 13, 15, 22]. Therefore the analyses also took into account, in both the HIS and the FCS, the following background variables: region of residency, gender, educational level, and age group. The educational level is based on the International Standard Classification of Education (ISCED) whereby the low educated people have at most a higher secondary education and the high educated people at least a post-secondary or tertiary education. A comparison was made of the distribution of the participants by background variables according to the study sample (HIS 2013 versus FCS 2014).
Misreporting of the self-reported BMI in the FCS
The FCS dataset contains both measured and self-reported BMI, calculated respectively from the height and weight. The magnitude of misreporting of the BMI at population level was estimated. This was expressed in terms of the absolute difference, calculated as the mean measured BMI minus the mean self-reported BMI (negative in case of over-reporting and positive in case of under-reporting), and in terms of the relative difference, calculated as the mean measured BMI divided by the mean self-reported BMI. These calculations were stratified by the combination of four background variables: region (3) * gender (2) * educational level (2) * age group (3), resulting in 36 strata.
Misreporting of the mean BMI consequently lead to misclassification. According to the criteria of the World Health Organization (WHO), participants were categorized as underweight (BMI < 18.50), normal weight (BMI 18.50–24.99), overweight (BMI 25.00–29.99) or obese (BMI ≥ 30.00) [29]. The validity of the self-reported BMI-classification was evaluated by cross-tabulating the measured BMI-categories with the self-reported BMI-categories. The sensitivity and specificity of the obesity class was also assessed.
Correcting the self-reported BMI in the HIS
Giacchi et al. [30] proposed a simple and economical procedure for adjusting the bias in the self-reported BMI. This procedure was applied to adjust the self-reported BMI of the HIS. Based on the FCS, a correction factor by stratum was calculated as the ratio between the measured and the self-reported BMI (the relative difference described earlier). Then, this correction factor was multiplied with the individual self-reported BMI of the HIS. In this way, a corrected BMI was produced for the HIS for the specific strata (region * gender * educational level * age group). To avoid having small numbers by strata, the categories by background variable were rather large. Producing a corrected BMI based on a corrected height and a corrected weight is very similar to a directly corrected BMI (used in this study). Both methods can be applied [20].
A Bland Altman plot analysis [31] was used to quantify the agreement between the measured BMI and the self-reported BMI of the FCS. Potential variation was assessed by the mean difference (đ) and the standard deviation (s) of the differences: đ ± 2 s, referring to the limits of agreement. A comparison was made with a Bland Altman plot between the measured BMI and the corrected self-reported BMI of the FCS (calculated in a similar way as the corrected BMI of the HIS). An improvement of the variation will be an argument for applying this correction factor on the HIS data.
Based on these corrected BMI’s, a new BMI-classification was generated for the HIS. The prevalence of obesity was then aggregated by background variable. The significant difference (based on the 95% confidence interval (CI)) was assessed between the obesity prevalence estimated with the corrected self-reported BMI of the HIS and the prevalence based on the measured BMI of the FCS.
All the analyses were performed with SAS® 9.2 [32]. For calculating the mean (PROC SURVEYMEANS) and the prevalence (PROC SURVEYFREQ) the complex survey design (weighting, clustering, and stratification) was taken into account.
Results
Distribution of the study samples by background variables
When comparing the distribution of the two study samples by different background variables (Table 1), it is most important to mention that in the HIS, the Brussels Region was oversampled, while in the FCS such oversampling was not foreseen.
Table 1.
Distribution (number and proportion) of the study samples by background variables
| HIS 2013 | FCS 2014 | ||||
|---|---|---|---|---|---|
| Background variables | N | % | N | % | |
| Region of residency | Flemish Region | 2113 | 32.3 | 702 | 57.9 |
| Brussels Region | 1911 | 29.2 | 90 | 7.4 | |
| Walloon Region | 2521 | 38.5 | 421 | 34.7 | |
| Gender | Males | 3188 | 48.7 | 596 | 49.1 |
| Females | 3357 | 51.3 | 617 | 50.9 | |
| Education | Low level | 3503 | 52.5 | 556 | 45.8 |
| High level | 3042 | 46.5 | 657 | 54.2 | |
| Age group | 18–34 years | 2155 | 32.9 | 456 | 37.6 |
| 35–50 years | 2397 | 36.6 | 414 | 34.1 | |
| 51–64 years | 1993 | 30.5 | 343 | 28.3 | |
| Total | 6545 | 100.0 | 1213 | 100.0 | |
Misreporting of the self-reported BMI in the FCS
Regarding the absolute differences, the mean self-reported BMI was significantly underestimated with almost one unit (0.96 kg/m2) when compared with the mean measured BMI (only 3% of the strata overestimated their self-reported BMI: males of 51–64 years in the Brussels Region with a low and high education level). Misreporting, expressed in absolute and relative differences, of the mean BMI by strata is presented in Table 2.
Table 2.
Misreporting of the mean self-reported BMI by strata, FCS 2014
| Region | Gender | Education | Age group | Mean measured BMI | Mean self-reported BMI | Abs. diff. a | Rel. diff.b |
|---|---|---|---|---|---|---|---|
| Total | Total | Total | Total | 26.17 (25.79–26.55) | 25.20 (24.85–25.56) | 0.96 (0.87–1.06) | 1.038 (1.034–1.042) |
| Flemish Region | Males | Low level | 18–34 | 24.41 (22.96–25.85) | 24.21 (22.75–25.66) | 0.20 (− 0.08–0.48) | 1.009 (0.996–1.022) |
| 35–50 | 27.41 (25.63–29.18) | 26.40 (24.85–27.96) | 1.00 (0.26–0.48) | 1.038 (1.018–1.057) | |||
| 51–64 | 28.82 (27.68–29.96) | 27.94 (26.85–29.03) | 0.88 (0.43–1.33) | 1.032 (1.017–1.048) | |||
| High level | 18–34 | 23.79 (23.08–24.50) | 23.07 (22.41–23.72) | 0.73 (0.44–1.01) | 1.031 (0.019–1.044) | ||
| 35–50 | 26.28 (25.30–27.27) | 25.60 (24.69–26.52) | 0.68 (0.49–0.88) | 1.027 (1.019–1.034) | |||
| 51–64 | 26.20 (25.15–27.25) | 25.35 (24.33–26.37) | 0.85 (0.50–1.21) | 1.034 (1.019–1.049) | |||
| Females | Low level | 18–34 | 26.02 (23.79–28.25) | 24.60 (22.88–26.32) | 1.42 (0.50–2.33) | 1.056 (1.024–1.088) | |
| 35–50 | 26.58 (24.33–28.84) | 25.26 (22.99–27.52) | 1.33 (0.76–1.90) | 1.056 (1.034–1.079) | |||
| 51–64 | 28.51 (25.92–31.10) | 27.00 (24.52–29.48) | 1.51 (1.10–1.92) | 1.057 (1.041–1.073) | |||
| High level | 18–34 | 22.87 (21.98–23.76) | 22.10 (21.29–22.91) | 0.77 (0.37–1.17) | 1.034 (1.017–1.052) | ||
| 35–50 | 24.91 (23.84–25.97) | 23.98 (23.02–24.94) | 0.92 (0.63–1.22) | 1.038 (1.026–1.050) | |||
| 51–64 | 25.67 (23.96–27.39) | 24.51 (23.06–25.95) | 1.16 (0.73–1.60) | 1.045 (1.030–1.060) | |||
| Brussels Region | Males | Low level | 18–34 | 25.60 (21.21–29.99) | 24.93 (21.65–28.20) | 0.67 (− 1.22–2.57) | 1.025 (0.952–1.098) |
| 35–50 | 25.04 (20.39–29.68) | 24.16 (11.40–36.92) | 0.88 (− 7.24–8.99) | 1.038 (0.691–1.384) | |||
| 51–64 | 25.03 (19.38–30.68) | 25.19 (20.53–29.85) | −0.16 (− 1.30–0.97) | 0.992 (0.948–1.036) | |||
| High level | 18–34 | 24.30 (22.03–26.57) | 22.96 (21.78–24.15) | 1.34 (− 0.31–2.98) | 1.057 (0.986–1.128) | ||
| 35–50 | 25.39 (24.05–26.54) | 24.62 (23.82–25.42) | 0.67 (−0.22–1.57) | 1.028 (0.993–1.063) | |||
| 51–64 | 23.99 (19.25–28.74) | 24.19 (20.48–27.91) | −0.20 (− 1.75–1.35) | 0.987 (0.913–1.061) | |||
| Females | Low level | 18–34 | 25.67 (18.97–32.37) | 24.98 (17.75–32.21) | 0.69 (− 0.20–1.58) | 1.033 (0.987–1.079) | |
| 35–50 | 33.54 (6.95–60.14) | 32.17 (6.71–57.63) | 1.38 (−0.58–3.34) | 1.043 (0.976–1.110) | |||
| 51–64 | 27.35 (17.42–37.28) | 25.60 (17.73–33.46) | 1.75 (− 1.02–4.53) | 1.062 (0.978–1.147) | |||
| High level | 18–34 | 22.87 (18.24–27.51) | 22.03 (18.36–25.70) | 0.85 (−0.23–1.92) | 1.033 (1.000–1.066) | ||
| 35–50 | 25.64 (20.44–30.84) | 24.13 (19.77–28.48) | 1.51 (0.40–2.62) | 1.056 (1.019–1.092) | |||
| 51–64 | 25.66 (19.95–31.36) | 24.63 (19.23–30.04) | 1.02 (−0.24–2.29) | 1.041 (0.987–1.094) | |||
| Walloon Region | Males | Low level | 18–34 | 24.93 (23.71–26.16) | 24.37 (23.31–25.43) | 0.56 (0.16–0.96) | 1.022 (1.007–1.038) |
| 35–50 | 28.73 (26.21–31.25) | 27.44 (24.78–30.11) | 1.28 (0.83–1.73) | 1.051 (1.029–1.072) | |||
| 51–64 | 28.02 (26.80–29.25) | 26.89 (25.80–27.98) | 1.14 (0.62–1.65) | 1.043 (1.023–1.062) | |||
| High level | 18–34 | 25.28 (23.37–27.19) | 24.69 (22.84–26.53) | 0.59 (0.32–0.86) | 1.022 (1.012–1.033) | ||
| 35–50 | 28.49 (25.85–31.12) | 27.70 (25.14–30.26) | 0.79 (0.55–1.02) | 1.029 (1.020–1.037) | |||
| 51–64 | 29.85 (27.21–32.49) | 28.33 (25.95–30.70) | 1.52 (0.84–2.20) | 1.053 (1.033–1.073) | |||
| Females | Low level | 18–34 | 25.00 (22.40–27.60) | 24.19 (21.74–26.63) | 0.81 (0.31–1.32) | 1.034 (1.012–1.056) | |
| 35–50 | 27.62 (25.37–29.88) | 26.30 (24.02–28.58) | 1.32 (0.52–2.12) | 1.051 (1.022–1.081) | |||
| 51–64 | 27.50 (25.97–29.03) | 26.18 (24.58–27.78) | 1.32 (0.62–2.02) | 1.053 (1.020–1.085) | |||
| High level | 18–34 | 24.59 (21.06–28.13) | 23.60 (20.14–27.06) | 0.99 (0.34–1.65) | 1.040 (1.017–1.063) | ||
| 35–50 | 25.49 (23.30–27.67) | 24.25 (22.26–26.25) | 1.23 (0.81–1.65) | 1.050 (1.034–1.066) | |||
| 51–64 | 27.71 (25.65–29.77) | 26.61 (24.38–28.83) | 1.10 (0.63–1.58) | 1.043 (1.025–1.061) |
aAbsolute difference: mean measured BMI – mean self-reported BMI
bRelative difference: mean measured BMI / mean self-reported BMI
The overall misclassification was 16.2%. Among the obese people, 26.5% reported themselves as overweight and 1.3% as normal weight. The sensitivity of self-reported information on obesity was 72.2% and the specificity was 99.6%.
Correction of the self-reported BMI in the HIS
The Bland Altman plot analysis indicates that the 95% limits of agreement between the measured BMI and the self-reported BMI of the FCS ranged from − 2.18 to 4.10. After correcting the self-reported BMI, this range has changed to − 3.09 to 3.10, indicating a more homogenous variation. The underestimation of the self-reported BMI has decreased which will improve the BMI-classification. This positive impact is an argument to also apply this correction factor on the HIS data (Fig. 1).
Fig. 1.
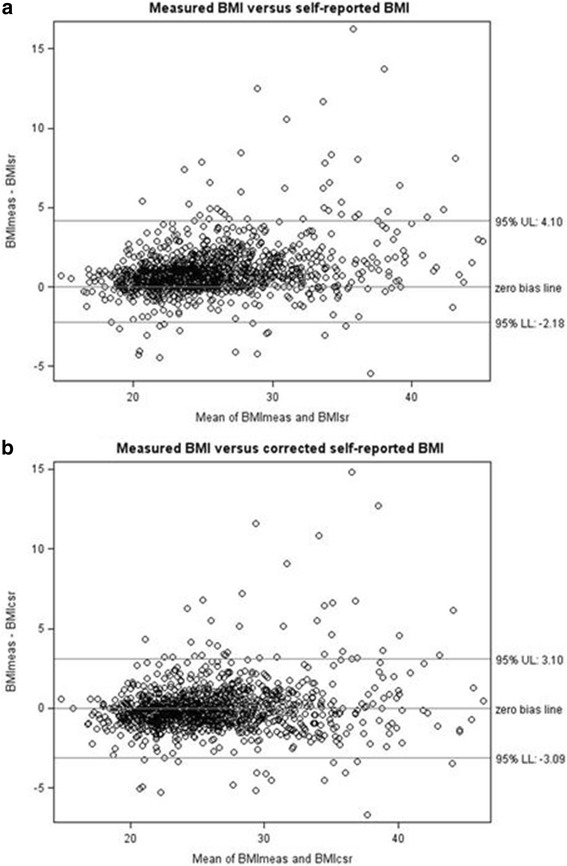
New proposition: Quantification of the agreement between the measured BMI and the self-reported BMI (a) compared to the measured BMI and the corrected self-reported BMI (b), Bland-Altman plots, FCS 2014
The prevalence of obesity according to the measured and self-reported BMI of the FCS versus the self-reported and corrected BMI of the HIS by background variables is presented in Table 3. According to the measured FCS data, 19.4% (16.6%–22.2%) of the Belgian adult population aged 18–64 years was obese, a figure significantly higher in comparison with the HIS results (12.8% (11.6%–14.0%)). When looking at the corrected estimate, the HIS obesity prevalence increased to 17.4% (16.1%–18.8%) which was no longer significantly different from the FCS measured one.
Table 3.
Obesity prevalence (and 95% CI) according to the measured and self-reported BMI of the FCS versus the self-reported and corrected BMI of the HIS by background variables
| Background variables | FCS measured | FCS self-reported | HIS self-reported | HIS corrected | |
|---|---|---|---|---|---|
| Total | 19.4 (16.6–22.2) | 14.1 (11.7–16.5) a | 12.8 (11.6–14.0) a | 17.4 (16.1–18.8) | |
| Region | Flemish Region | 18.2 (14.8–21.6) | 11.3 (8.6–13.9) a | 11.4 (9.6–13.2) a | 16.1 (14.1–18.2) |
| Brussels Region | 14.1 (4.7–23.5) | 13.4 (4.1–22.1) | 12.1 (10.3–13.8) | 15.2 (13.2–17.1) | |
| Walloon Region | 23.5 (18.0–28.9) | 19.7 (14.6–24.8) | 15.5 (13.5–17.4) a | 20.4 (18.3–22.6) | |
| Gender | Males | 18.6 (14.8–22.3) | 14.0 (10.7–17.3) | 12.7 (11.0–14.5) a | 15.9 (14.0–17.8) |
| Females | 20.3 (16.1–24.4) | 14.2 (10.6–17.8) | 12.9 (11.3–14.4) a | 18.9 (17.0–20.8) | |
| Education | Low level | 26.8 (22.0–31.5) | 19.0 (14.9–23.1) | 17.1 (15.3–18.9) a | 22.1 (20.1–24.0) |
| High level | 13.8 (10.5–17.1) | 10.4 (7.5–13.2) | 7.9 (6.4–9.5) a | 12.2 (10.3–14.0) | |
| Age group | 18–34 years | 12.4 (8.3–16.6) | 9.2 (5.5–13.0) | 7.8 (5.9–9.6) | 10.1 (8.1–12.1) |
| 35–50 years | 20.8 (16.0–25.5) | 17.6 (13.0–22.1) | 13.3 (11.3–15.3) a | 18.2 (16.0–20.4) | |
| 51–64 years | 25.0 (19.4–30.6) | 14.9 (10.7–19.1) a | 17.8 (15.5–20.2) | 24.6 (21.9–27.3) | |
aSignificantly different from FCS measured
The self-reported obesity prevalence of the HIS was significantly different from the FCS measured one in the Flemish Region (11.4% (9.6%–13.2%) versus 18.2% (14.8%–21.6%)) and the Walloon Region (15.5% (13.5%–17.4%) versus 23.5% (18.0%–28.9%)). The corresponding corrected prevalences are no longer significantly different (respectively 16.1% (14.1%–18.2%) and 20.4% (18.3%–22.6%)). Also the corrected obesity prevalence for both men and women (respectively 15.9% (14.0%–17.8%) and 18.9% (17.0%–20.8%)) approximated the measured obesity prevalence (respectively 18.6% (14.8%–22.3%) and 20.3% (16.1%–24.4%)). Furthermore, an increase of the self-reported obesity prevalence of the HIS was observed after correction for both educational levels: from 17.1% (15.3%–18.9%) to 22.1% (20.1%–24.0%) for the low educated people and from 7.9% (6.4%–9.5%) to 12.2% (10.3%–14.0%) for the high educated people. These corrected self-reported prevalences were closer to the FCS measured ones (respectively 26.8% (22.0%–31.5%) and 13.8% (10.5%–17.1%)), whereby also the significant differences disappeared. Finally, the self-reported obesity prevalence in the age group 35–50 years (13.3% (11.3%–15.3%)) was underestimated and was significantly different from the measured obesity prevalence (20.8% (16.0%–25.5%)). After correction, the self-reported obesity prevalence in the HIS increased to 18.2% (16.0%–20.4%) and the differences were no longer significant with the measured FCS estimates.
Discussion
The BMI measured in the FCS 2014 served as golden standard. Overall, the self-reported BMI was underestimated in the FCS 2014. The underestimation with one BMI-unit is within the range of other studies [16, 24]. Hence, the prevalence of obesity was underestimated when based on self-reported BMI which is in accordance with many other studies as well [3, 13, 17–19]. The misclassification frequency is an appropriate way to assess the accuracy of self-reported BMI [24]. Especially obese people had the tendency to underestimate their BMI. As in other studies, a very high specificity was observed for obesity (5;23;25). However, the value for the sensitivity was lower, in line with other studies (5;9;25).
Data from the FCS lend itself to estimate a simple correction factor (measured BMI/self-reported BMI) which improves the accuracy of the self-reported BMI. Since the FCS and the HIS were conducted in comparable conditions (same time span, target population and sampling method), this correction factor could be applied to the individual self-reported BMI of the HIS, the second objective of this study. Other studies affirm that external applicability of a correction factor can be done under certain conditions [17, 24, 33].
Via this correction procedure, the ultimate goal of this study, to improve the accuracy of the self-reported BMI-classification in the HIS, was achieved. The corrected obesity prevalence of the HIS (17.2%) approximated the one of the golden standard (19.4%). This implies that the problem of obesity in Belgium is 4% points higher than initially thought based on self-reported HIS data. The significant differences between the corrected obesity prevalence and the golden standard also disappeared after correction for the following subgroups: the Flemish and the Walloon Region, both genders, the low educated people as well as the high educated people and the age group 35–50 years.
Because of some shortcomings of this study, the prevalence of obesity could possibly be higher. First of all, the participants of the FCS knew indeed when responding to the questions about their height and weight, that they would be measured and weighed at a later stage. Reporting under such circumstances presumably lead to more truthful data [17, 34]. This effect could be even strengthened by the fact that the FCS is a specific nutrition survey by a professional dietician (versus a general health survey by an interviewer). In this case the correction factor is probably underestimated [2, 14]. Second, the participation rate of both surveys was rather small, especially for the FCS (37%). The low participation rate of the FCS can be explained by the context of the survey: the HIS is a general health survey, but the focus of the FCS is on nutrition and the participation to this survey is more intensive (two visits, a food diary, measurements). Moreover, it has been shown that people who refuse to participate are more often obese, which could also bias the estimates [19, 25]. Since participation to both surveys is not mandatory, it would be desirable to develop strategies to improve the response rate among the population [20]. Some other limitations of this study are the fact that the questions used to assess height and weight in the FCS were less clearly defined and could therefore be slightly different from the questions used in the HIS, and the fact that the selection of the respondents at household level in the HIS may introduce some clustering in the results on BMI. Finally, the distribution of the two samples by region does not completely correspond, especially for the Brussels Region. The smaller strata in the FCS for this region lead to bigger confidence intervals and probably to less accurate estimates of the correction factor.
The results demonstrate that caution is needed when interpreting the obesity prevalence deduced from self-reported height and weight. Underestimation of the obesity prevalence gives a distorted image of the real health burden, which is problematic for policy making [2, 15, 22, 24]. Although preference is given to measured height and weight for assessing the obesity prevalence accurately, it is not always possible to collect such data because of practical and budgetary reasons, especially in large and recurrent population surveys [17, 35]. Therefore, height and weight collected through interview remains an essential tool [22, 28, 35, 36]. However, in this situation it is worth applying a correction factor to the self-reported BMI in order to increase the accuracy of the information and obtain more reliable estimates of the obesity prevalence. Since certain subgroups have a bigger influence on misreporting then others, it is important to determine this correction factor by specific background variables.
Other studies also recommend adjustment of self-reported data as a reasonable alternative when measurements are not feasible [3, 15, 20, 21, 25, 35–37]. Nevertheless, the correction factors of the FCS 2014 will likely not be applicable to the self-reported data of the forthcoming HIS’s since studies have indicated that reporting bias may change over time and should therefore be updated regularly [3, 17, 20, 25]. Awareness and attention to the problem of obesity, but also the “normalizing” of overweight which change people’s perception of their weight status, could have an effect on the way how people respond [2]. Therefore, for the next HIS, measuring height and weight in a random subsample could be very useful in order to assess and apply new correction factors to the whole population.
Conclusions
Through the national Food Consumption Survey (FCS) 2014, the bias of the self-reported BMI related to the measured BMI could be assessed in Belgium. Based on these data, a simple correction factor (measured BMI/self-reported BMI) was estimated. Applying this correction factor on the self-reported BMI of the national Health Interview Survey (HIS) 2013 led to a more accurate estimation of the obesity prevalence, which is important for decision making. Therefore regular adjustment of self-reported obesity estimates is recommended.
Acknowledgements
The Belgian National Health Interview Survey is a project conducted in collaboration with the FSP Economy – Statistics Belgium that is responsible for drawing the sample and the fieldwork management.
The Belgian National Food Consumption Survey 2014-2015 is a collaboration between the Scientific Institute of Public Health, the Federal Public Service Health, Food chain safety and Environment, and the European Food Safety Agency.
Funding
No specific funding was received for this study.
Availability of data and materials
Access to the micro data of the Belgian National Health Interview Survey is described on the following website: https://his.wiv-isp.be/SitePages/Acces_microdata.aspx
The data of the Belgian National Food Consumption Survey 2014–2015 [Data file and code book] are obtainable under conditions from the following website: https://fcs.wiv-isp.be/SitePages/Database.aspx
Abbreviations
- BMI
Body mass index
- CI
Confidence interval
- FCS
Belgian National Food Consumption Survey
- HIS
Belgian National Health Interview Survey
Authors’ contributions
SDr and SD conceived the framework of the study. SDr performed the statistical analyses and drafted the manuscript. All authors contributed to the interpretation of the results and to the critical revision of the manuscript. All the authors approved the final version of the manuscript.
Ethics approval and consent to participate
Both surveys were carried out in line with the Belgian privacy legislation and approved by the ethical committee of Ghent University. The fact that individuals are willing to participate to the survey, is the consent.
Consent for publication
There are no details on individual participants within the manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
S. Drieskens, Phone: 00.32.2.642.50.25, Email: Sabine.Drieskens@wiv-isp.be
S. Demarest, Email: Stefaan.Demarest@wiv-isp.be
S. Bel, Email: Sarah.Bel@wiv-isp.be
K. De Ridder, Email: Karin.DeRidder@wiv-isp.be
J. Tafforeau, Email: Jean.Tafforeau@wiv-isp.be
References
- 1.The challenge of obesity in the WHO European region and the strategies for response: summary. Edited by Branca F, Nikogosian H, Lobstein T. 1–323. 2007. World Health Organization.
- 2.Connor GS, Tremblay MS: the bias in self-reported obesity from 1976 to 2005: a Canada-US comparison. Obesity (Silver Spring) 2010, 18: 354–361. [DOI] [PubMed]
- 3.Nyholm M, Gullberg B, Merlo J, Lundqvist-Persson C, Rastam L, Lindblad U. The validity of obesity based on self-reported weight and height: implications for population studies. Obesity (Silver Spring) 2007;15:197–208. doi: 10.1038/oby.2007.536. [DOI] [PubMed] [Google Scholar]
- 4.Roberts RJ. Can self-reported data accurately describe the prevalence of overweight? Public Health. 1995;109:275–284. doi: 10.1016/S0033-3506(95)80205-3. [DOI] [PubMed] [Google Scholar]
- 5.Drieskens S, Van der Heyden J, Demarest S, Tafforeau J. Is the different time trend (1997-2008) of the obesity prevalence among adults in the three Belgian regions associated with lifestyle changes? Arch Public Health. 2014;72:18. doi: 10.1186/2049-3258-72-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jacobson BH, DeBock DH. Comparison of body mass index by self-reported versus measured height and weight. Percept Mot Skills. 2001;92:128–132. doi: 10.2466/pms.2001.92.1.128. [DOI] [PubMed] [Google Scholar]
- 7.Niedhammer I, Bugel I, Bonenfant S, Goldberg M, Leclerc A. Validity of self-reported weight and height in the French GAZEL cohort. Int J Obes Relat Metab Disord. 2000;24(9):1111–1118. doi: 10.1038/sj.ijo.0801375. [DOI] [PubMed] [Google Scholar]
- 8.Drieskens S. Etat nutritionnel. Dans: Gisle L, Demarest S (éd.). Enquête de Santé 2013. Rapport 2: Comportements de santé et style de vie. WIV-ISP, Bruxelles, 2014.
- 9.Galuska DA, Serdula M, Pamuk E, Siegel PZ, Byers T. Trends in overweight among US adults from 1987 to 1993 - a multistate telephone survey. Am J Public Health. 1996;86:1729–1735. doi: 10.2105/AJPH.86.12.1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash R, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763–778. doi: 10.1056/NEJMoa055643. [DOI] [PubMed] [Google Scholar]
- 11.Vital signs: State-specific obesity prevalence among adults - United States, 2009. MMWR Morb Mortal Wkly Rep 2010 Aug 6; 59(30): 951–955. [PubMed]
- 12.Neovius K, Johansson K, Kark M, Tynelius P, Rasmussen F. Trends in self-reported BMI and prevalence of obesity 2002-10 in Stockholm County, Sweden. Eur J Pub Health. 2013;23:312–315. doi: 10.1093/eurpub/cks128. [DOI] [PubMed] [Google Scholar]
- 13.Krul AJ, Daanen HAM, Choi H. Self-reported and measured weight, height and body mass index (BMI) in Italy, the Netherlands and North America. Eur J Pub Health. 2011;21:414–419. doi: 10.1093/eurpub/ckp228. [DOI] [PubMed] [Google Scholar]
- 14.McAdams MA, van Dam RM, Hu FB. Comparison of self-reported and measured BMI as correlates of disease markers in US adults. Obesity (Silver Spring) 2007;15:188–196. doi: 10.1038/oby.2007.504. [DOI] [PubMed] [Google Scholar]
- 15.Connor GS, Tremblay M, Moher D, Gorber B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: a systematic review. Obes Rev. 2007;8:307–326. doi: 10.1111/j.1467-789X.2007.00347.x. [DOI] [PubMed] [Google Scholar]
- 16.Bolton-Smith C, Woodward M, Tunstall-Pedoe H, Morrison C. Accuracy of the estimated prevalence of obesity from self reported height and weight in an adult Scottish population. J Epidemiol Community Health. 2000;54:143–148. doi: 10.1136/jech.54.2.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shields M, Connor Gorber S, Janssen I, Tremblay MS. Bias in self-reported estimates of obesity in Canadian health surveys: an update on correction equations for adults. Health Rep. 2011;22(3):35–45. [PubMed] [Google Scholar]
- 18.Visscher TL, Viet AL, Kroesbergen IH, Seidell JC. Underreporting of BMI in adults and its effect on obesity prevalence estimations in the period 1998 to 2001. Obesity (Silver Spring) 2006;14:2054–2063. doi: 10.1038/oby.2006.240. [DOI] [PubMed] [Google Scholar]
- 19.Faeh D, Marques-Vidal P, Chiolero A, Bopp M. Obesity in Switzerland: do estimates depend on how body mass index has been assessed? Swiss Med Wkly. 2008;138(13–14):204–210. doi: 10.4414/smw.2008.12065. [DOI] [PubMed] [Google Scholar]
- 20.Dutton DJ, McLaren L. The usefulness of "corrected" body mass index vs. self-reported body mass index: comparing the population distributions, sensitivity, specificity, and predictive utility of three correction equations using Canadian population-based data. BMC Public Health. 2014;14:430. doi: 10.1186/1471-2458-14-430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kuskowska-Wolk A, Bergström R, Boström G. Relationship between questionnaire data and medical records of height, weight and body mass index. Int J Obes Relat Metab Disord. 1992;16(1):1–9. [PubMed] [Google Scholar]
- 22.Lucca A, Moura EC. Validity and reliability of self-reported weight, height and body mass index from telephone interviews. Cad Saude Publica. 2010;26:110–122. doi: 10.1590/S0102-311X2010000100012. [DOI] [PubMed] [Google Scholar]
- 23.Hill A, Roberts J. Body mass index: a comparison between self-reported and measured height and weight. J Public Health Med. 1998;20:206–210. doi: 10.1093/oxfordjournals.pubmed.a024744. [DOI] [PubMed] [Google Scholar]
- 24.Gosse MA. How accurate is self-reported BMI? Nutr Bull. 2014;39:105–114. doi: 10.1111/nbu.12075. [DOI] [Google Scholar]
- 25.Connor Gorber S, Shields M, Tremblay MS, Mcdowell I. The feasibility of establishing correction factors to adjust self-reported estimates of obesity. Health Rep. 2008;19(3):71–82. [PubMed] [Google Scholar]
- 26.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240–1243. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Demarest S, Van der Heyden J, Charafeddine R, Drieskens S, Gisle L, Tafforeau J. Methodological basics and evolution of the Belgian health interview survey 1997-2008. Arch Public Health. 2013;71:24. doi: 10.1186/0778-7367-71-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bel S, Van den Abeele S, Lebacq T, Ost C, Brocatus L, Stievenart C, et al. Protocol of the Belgian food consumption survey 2014: objectives, design and methods. Arch Public Health. 2016;74:20. doi: 10.1186/s13690-016-0131-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Obesity: Preventing and Managing the Global Epidemic. Edited by World Health Organization. Technical Report Series 854. 2011. Geneva, Switzerland. [PubMed]
- 30.Giacchi M, Mattei R, Rossi S. Correction of the self-reported BMI in a teenage population. Int J Obes Relat Metab Disord. 1998;22:673–677. doi: 10.1038/sj.ijo.0800646. [DOI] [PubMed] [Google Scholar]
- 31.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. doi: 10.1016/S0140-6736(86)90837-8. [DOI] [PubMed] [Google Scholar]
- 32.SAS/STAT 9.2 User's Guide. Cary, NC, USA: 2008.
- 33.Liechty JM, Bi X, Qu A. Feasibility and validity of a statistical adjustment to reduce self-report bias of height and weight in wave 1 of the add health study. BMC Med Res Methodol. 2016;16:124. doi: 10.1186/s12874-016-0227-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rowland ML. Self-reported weight and height. Am J Clin Nutr. 1990Dec;52(6):1125–33. [DOI] [PubMed]
- 35.Perez A, Gabriel K, Nehme EK, Mandell DJ, Hoelscher DM. Measuring the bias, precision, accuracy, and validity of self-reported height and weight in assessing overweight and obesity status among adolescents using a surveillance system. Int J Behav Nutr Phys Act. 2015;12(Suppl 1):S2. doi: 10.1186/1479-5868-12-S1-S2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Stommel M, Schoenborn CA. Accuracy and usefulness of BMI measures based on self-reported weight and height: findings from the NHANES & NHIS 2001-2006. BMC Public Health. 2009;9:421. doi: 10.1186/1471-2458-9-421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ezzati M, Martin H, Skjold S, Vander HS, Murray CJ. Trends in national and state-level obesity in the USA after correction for self-report bias: analysis of health surveys. J R Soc Med. 2006;99:250–257. doi: 10.1177/014107680609900517. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Access to the micro data of the Belgian National Health Interview Survey is described on the following website: https://his.wiv-isp.be/SitePages/Acces_microdata.aspx
The data of the Belgian National Food Consumption Survey 2014–2015 [Data file and code book] are obtainable under conditions from the following website: https://fcs.wiv-isp.be/SitePages/Database.aspx