

Abstract
Objectives. To examine the relationship between sexual violence and transactional sex and assess the impact of social support on this relationship among female transnational migrants in Cape Town, South Africa.
Methods. In 2012 we administered a behavioral risk factor survey using respondent-driven sampling to transnational migrant women aged between 16 and 39 years, born outside South Africa, living in Cape Town, and speaking English, Shona, Swahili, Lingala, Kirundi, Kinyarwanda, French, or Somali.
Results. Controlling for study covariates, travel-phase sexual violence was positively associated with engagement in transactional sex (adjusted prevalence ratio [APR] = 1.38; 95% confidence interval [CI] = 1.07, 1.77), and social support was shown to be a protective factor (APR = 0.84; 95% CI = 0.75, 0.95). The interaction of experienced sexual violence during migration and social support score was APR = 0.85 (95% CI = 0.66, 1.10). In the stratified analysis, we found an increased risk of transactional sex among the low social support group (APR = 1.56; 95% CI = 1.22, 2.00). This relationship was not statistically significant among the moderate or high social support group (APR = 1.04; 95% CI = 0.58, 1.87).
Conclusions. Programs designed to strengthen social support may reduce transactional sex among migrant women after they have settled in their receiving communities.
Population mobility has been shown to be associated with sexual risk in resource-poor populations around the world,1 and these risks are likely contributing to the high rates of sexually transmitted infections and HIV/AIDS documented in many migrant populations.2,3 Evidence also suggests that female migrants shoulder a higher burden of sexually transmitted infections and HIV/AIDS than do their male counterparts.4 Although the exact mechanisms that shape disparities in negative sexual health outcomes among migrant populations are unclear, gendered experiences of sexual risk factors, in particular migrant women’s experience of transactional sex and sexual violence, may be driving this increased burden among female migrants.
Transactional sex and sexual violence can be defined in several ways. We used an informal conceptualization of transactional sex, in which sex can be exchanged for money and goods and services. Women who engage in this form of transactional sex may be less likely to be viewed as sex workers.5 We defined sexual violence as sexual activity in which consent is not obtained or freely given (also referred to as rape or forced sex). Transactional sex and sexual violence can result in numerous negative sexual health outcomes; both are frequently typified by low rates of condom use in South Africa,6,7 which can result in unwanted pregnancies, unsafe abortions, and HIV and sexually transmitted infections. Sexual abuse and violence have also been found to be associated with future engagement in riskier sexual activity.8,9 Furthermore, there is some evidence to suggest a link between sexual violence and transactional sex; studies have shown that engaging in survival sex is often associated with a previous history of sexual victimization.10,11
Transnational migrant women are at increased risk for engaging in transactional sex and experiencing sexual violence. Transnational migrants often experience hurdles accessing legitimate employment because of language barriers and lack of legal documentation, and the marginalized status of many female migrants has caused transactional sex to become a main tool for survival.12,13 Sexual violence is often used as a tool of war,14 and these practices have been shown to be prevalent in informal migrant settlements.15 Transnational female migrants may also be exposed to sexual violence while attempting to illegally cross country borders.13
Receiving social support may influence both transactional sex and sexual violence. Studies have reported inverse relationships between higher levels of social support and engagement in transactional sex,16,17 and perceived social support has been shown to reduce the impact of sexual violence on negative mental health outcomes.18 However, to date no studies have investigated social support’s influence on the relationship between sexual violence and transactional sex. Furthermore, social support can be a tenuous resource for cross-border migrants, because established support delivery systems are frequently disrupted when individuals move from long-standing communities to often isolating environments in host communities.19,20 This difficulty accessing social support coupled with its potential influence on sexual risks make understanding the relationships between social support, transactional sex, and sexual violence among cross-border migrants particularly critical.
The migration phases framework was developed to better understand how the complex nature of the migration process affects migrant risk environments.21 In addition, the migration phases framework aims to identify intervention opportunities that can occur throughout the migration process.21 Using migration phases framework concepts, we examined the relationship between experiencing sexual violence during the migration process (travel phase) and engaging in transactional sex in receiving communities (destination phase). We also investigated whether receiving social support acts as an effect modifier on the relationship between sexual violence and recent transactional sex.
METHODS
We obtained data for our analysis from a cross-sectional study conducted in 2012 among transnational migrant women residing in Cape Town, South Africa. The sampling procedure and study methods are described elsewhere.22 Briefly, women were eligible to participate if they were aged between 16 and 39 years, were born outside South Africa, lived in Cape Town, and were able to speak one of the following 8 study languages: English, Shona, Swahili, Lingala, Kirundi, Kinyarwanda, French, or Somali. We screened participants for study eligibility, and then they completed a behavioral risk assessment survey that we administered using an audio computer-assisted self-interview.
We recruited participants using respondent-driven sampling, which is a form of chain referral sampling capable of reaching members of hidden populations. It allows investigators to obtain a broadly representative sample when a reliable sampling frame is lacking.23,24 Recruitment into this study began with 11 nonrandomly selected seeds. The initial seeds were highly social, well-regarded members of the study population. We asked seeds and subsequent participation recruits to recruit up to 4 members of their social networks. This process continued until the desired sample size was reached. The recruitment process produced 1029 migrant women, 935 (91%) of whom participated in the study.
Measures
The main dependent variable was self-reported recent transactional sex. We constructed this variable from a series of questions that asked whether participants had exchanged sex for money, food, clothing, transportation, school fees, housing, prepaid telephone vouchers, or other material goods with their most recent sexual partner. Approximately one third (37%; n = 285) of the sample reported exchanging sex for at least 1 of these 8 goods or services, and we collapsed data from the individual question items to construct a dichotomous indicator for “any” transactional sex. Among the participants who reported any transactional sex, the number of types of transactional sex ranged from 1 to 8 (mean = 4.1; SD = 2.6). To assess travel-phase sexual violence, we asked each participant if she had been forced to have sex against her will during the journey from her home country to South Africa. We coded participants who responded yes to this question as a “1” and those who responded no as a “0.”
We assessed perceived social support using the 19-item Medical Outcomes Study Social Support Scale.25 We asked respondents about positive social interactions and receiving tangible, affective, informational, and emotional support over the past 4 weeks through 19 questions items. Response options on a 5-point Likert scale ranged from “none of the time” to “all of the time.” Overall scores ranged from 1 to 5, and the scale had a Cronbach α of 0.95, indicating high reliability. For the purposes of the subgroup analysis, we dichotomized the social support variable into “low” (score < 3) versus “moderate to high” (score ≥ 3) levels of support. This cutoff corresponded to receiving each type of support a minimum of “some of the time” on average and has been used previously to define moderate to high support on the Medical Outcomes Study scale.26
We assessed additional covariates as potential confounders. Demographic characteristics included age, marital status, education level, relative income level, and housing status since arriving in South Africa. Migration-related factors included length of time in South Africa, whether the participant arrived in South Africa through a legal border entry point, and country of origin. We assessed push–pull factors by asking women to select their main reason for migrating (for work or educational opportunities, to escape an unhappy home life, to avoid political persecution, or some other reason). Behavioral risk factors included having multiple (≥ 2) partners in the past 3 months and alcohol use. For all study measures of sexual behavior, “sex” referred to vaginal or anal intercourse.
Statistical Analysis
To analyze respondent-driven sampling data, we used each respondent’s social network size and recruiter characteristics to adjust for differential probabilities of recruitment into the study.23,24 We used the Respondent-Driven Sampling Analysis Tool, version 7.1 (Cornell University, Ithaca, NY) to generate individualized sample weights to weight the transactional sex variable in all Poisson regression models. After generating the individualized weights, we excluded 171 women (18%) from the analysis because of missing data on at least 1 key variable, yielding a final analytic sample of 764. Comparisons between included and excluded participants across demographic factors and the main study variables revealed no statistically significant differences, suggesting that their exclusion did not contribute any selection bias to this analysis.
We constructed unweighted descriptive statistics for all variables. We used Poisson regression to estimate unadjusted prevalence ratios (UPRs) between study covariates and recent engagement in transactional sex. We included factors found to be significantly associated with transactional sex (P < .05) in unadjusted models in multivariable models that assessed the relationship between recent transactional sex and sexual violence. To test for moderation, we included a term for the interaction of sexual violence and social support score in the final adjusted Poisson regression model. We also conducted a stratified analysis to test whether there was differential variation in the relationship between travel-phase sexual violence and destination-phase transactional sex across the dichotomized categories of social support. We calculated PRs and corresponding P values for all unadjusted and adjusted models using Stata version 12 (StataCorp LP, College Station, TX).
RESULTS
Table 1 provides the unweighted descriptive statistics for the study covariates, which are not representative of the underlying target population and summarize only the analytic sample. The overall prevalence of transactional sex in the sample was 37% (n = 285); 10% (n = 77) reported experiencing sexual violence during their journey to South Africa. The mean Medical Outcomes Study Social Support Scale score was 2.97 (SD = 0.96). The mean sample age was 28.5 (SD = 5.9) years. The majority of women were married (72%; n = 547), had a high school education or less (75%; n = 576), and reported only having enough money for food and basic household items (49%; n = 375). Approximately one quarter of women had resided in South Africa for 2 years or less (26%; n = 197), and 46% (n = 354) had illegally crossed the border into South Africa. One third of the sample (33%; n = 255) reported always living in a shelter or on the street in South Africa. Twenty-eight percent of the sample reported that their main reason for leaving their home country was to search for work or education (n = 216). Only 7% (n = 52) of women reported consuming 3 or more drinks each day, and 23% (n = 176) reporting having 2 or more partners in the past 3 months.
TABLE 1—
Transactional Sex, Sexual Violence, Social Support, and All Study Covariates Among Transnational Female Migrants: Cape Town, South Africa, 2012
| Variable | % (No.) or Mean (SD; Range) |
| Transactional sex with one’s most recent sexual partner | |
| Any | 37 (285) |
| None | 63 (479) |
| Sexual violence during migration process | |
| Did not experience | 90 (687) |
| Experienced | 10 (77) |
| MOS Social Support Scale score | 2.97 (0.96; 1–5) |
| Age, y | 28.50 (5.90; 16–39) |
| Marital status | |
| Not married | 28 (217) |
| Married | 72 (547) |
| Poverty scale | |
| Not enough money for food | 39 (295) |
| Enough money for food and basic items | 49 (375) |
| Enough money for basic items and luxuries | 12 (94) |
| Education status | |
| > high school | 25 (188) |
| ≤ high school | 75 (576) |
| Housing stability in South Africa | |
| Always in a private home | 33 (255) |
| At least some time in shelter or on the street | 33 (254) |
| Always in a shelter or on the street | 33 (255) |
| Recent migrants | |
| > 2 y in South Africa | 74 (567) |
| ≤ 2 in South Africa | 26 (197) |
| Border crossing | |
| Legal | 54 (410) |
| Illegal | 46 (354) |
| Country of origin | |
| Zimbabwe | 19 (146) |
| Congo or Democratic Republic of Congo | 53 (408) |
| Rwanda | 15 (116) |
| Burundi | 8 (64) |
| Other | 4 (30) |
| Push–pull factors | |
| Political persecution or other | 45 (345) |
| Work and education | 28 (216) |
| Unhappy home life | 27 (203) |
| Multiple partners in past 3 mo | |
| < 2 | 77 (588) |
| ≥ 2 | 23 (176) |
| Drinks per d | |
| 0 | 80 (608) |
| 1–2 | 14 (104) |
| ≥ 3 | 7 (52) |
Note. MOS = Medical Outcomes Study. The sample size was n = 764.
UPRs are found in Table 2. Experiencing travel-phase sexual violence was associated with an 83% increased risk of engaging in transactional sex with one’s most recent partner in Cape Town (UPR = 1.83; 95% confidence interval [CI] = 1.46, 2.29). Receiving social support was shown to reduce risk of transactional sex in the unadjusted analysis, with a 1-unit increase in social support score corresponding to a 17% decrease in risk of transactional sex (UPR = 0.83; 95% CI = 0.74, 0.94). Several covariates were also significantly associated with transactional sex in the unadjusted analysis. Being older was associated with a decreased risk of transactional sex with one’s most recent partner (UPR = 0.97; 95% CI = 0.95, 0.99).
TABLE 2—
Unadjusted and Adjusted Prevalence Ratios of the Risk of Transactional Sex With One’s Most Recent Sexual Partner Among Transnational Female Migrants: Cape Town, South Africa, 2012
| Variable | Any Transactional Sex (n = 285), % (No.) or Mean (SD; Range) | No Transactional Sex (n = 479), % (No.) or Mean (SD; Range) | UPR (95% CI) | APR (95% CI) |
| Sexual violence during migration process | ||||
| Did not experience | 82 (235) | 94 (452) | 1.0 (Ref) | 1.0 (Ref) |
| Experienced | 18 (50) | 6 (27) | 1.83 (1.46, 2.29) | 1.38 (1.07, 1.77) |
| MOS Social Support Scale score | 2.81 (0.92; 1–5) | 3.06 (0.97; 1–5) | 0.83 (0.74, 0.94) | 0.84 (0.75, 0.95) |
| Age, y | 27.20 (5.80; 16–39) | 29.20 (5.90; 16–39) | 0.97 (0.95, 0.99) | 0.97 (0.75, 0.95) |
| Marital status | ||||
| Not married | 32 (91) | 26 (126) | 1.0 (Ref) | |
| Married | 68 (194) | 74 (353) | 0.86 (0.67, 1.10) | |
| Poverty scale | ||||
| Not enough money for food | 41 (118) | 37 (177) | 1.0 (Ref) | |
| Enough money for food and basic items | 48 (137) | 50 (238) | 0.90 (0.70, 1.15) | |
| Enough money for basic items and luxuries | 11 (30) | 13 (64) | 0.81 (0.53, 1.24) | |
| Education status | ||||
| >high school | 23 (65) | 26 (123) | 1.0 (Ref) | |
| ≤ high school | 77 (220) | 74 (356) | 1.03 (0.90, 1.19) | |
| Housing stability in South Africa | ||||
| Always in a private home | 25 (71) | 38 (184) | 1.0 (Ref) | 1.0 (Ref) |
| At least some time in a shelter or on the street | 36 (103) | 33 (151) | 1.65 (1.18, 2.29) | 1.47 (1.07, 2.04) |
| Always in a shelter or on the street | 40 (111) | 30 (144) | 1.68 (1.23, 2.28) | 1.30 (0.95, 1.77) |
| Recent migrants | ||||
| > 2 y in South Africa | 69 (296) | 77 (371) | 1.0 (Ref) | 1.0 (Ref) |
| ≤ 2 y in South Africa | 31 (89) | 23 (108) | 1.07 (1.02, 1.12) | 1.25 (0.98, 1.59) |
| Border crossing | ||||
| Legal | 50 (142) | 56 (268) | 1.0 (Ref) | |
| Illegal | 50 (143) | 44 (211) | 1.11 (0.88, 1.41) | |
| Country of origin | ||||
| Zimbabwe | 20 (57) | 19 (89) | 1.0 (Ref) | |
| Congo or Democratic Republic of Congo | 53 (150) | 54 (258) | 0.99 (0.73, 1.34) | |
| Rwanda | 14 (41) | 16 (75) | 1.07 (0.74, 1.54) | |
| Burundi | 8 (24) | 8 (40) | 0.96 (0.57, 1.61) | |
| Other | 5 (13) | 4 (17) | 1.12 (0.61, 2.05) | |
| Push–pull factors | ||||
| Political persecution or other | 39 (112) | 49 (233) | 1.0 (Ref) | 1.0 (Ref) |
| Work or education | 31 (87) | 27 (129) | 1.29 (0.96, 1.73) | 1.14 (0.86, 1.50) |
| Unhappy home life | 30 (86) | 24 (117) | 1.38 (1.04, 1.83) | 1.25 (0.96, 1.63) |
| Multiple partners in past 3 mo | ||||
| < 2 | 63 (178) | 86 (410) | 1.0 (Ref) | 1.0 (Ref) |
| ≥ 2 | 37 (107) | 14 (69) | 1.61 (1.28, 2.04) | 1.36 (1.08, 1.72) |
| Drinks per d | ||||
| 0 | 74 (210) | 83 (398) | 1.0 (Ref) | 1.0 (Ref) |
| 1–2 | 14 (40) | 13 (64) | 0.99 (0.68, 1.43) | 0.96 (0.68, 1.36) |
| ≥ 3 | 12 (35) | 4 (17) | 1.72 (1.25, 2.37) | 1.45 (1.03, 2.03) |
Note. APR = adjusted prevalence ratio; CI = confidence interval; MOS = Medical Outcomes Study; UPR = unadjusted prevalence ratio. The sample size was n = 764.
We found an increased risk of transactional sex for migrants who had lived in South Africa for 2 years or less (UPR = 1.07; 95% CI = 1.02, 1.12), who reported their main reason for leaving their home country was to escape an unhappy home life (UPR = 1.38; 95% CI = 1.04, 1.83), who had 2 or more partners in the past 3 months (UPR = 1.61; 95% CI = 1.28, 2.04), who consumed 3 or more drinks per day (UPR = 1.72; 95% CI = 1.25, 2.37), and who were marginally housed in South Africa either some of the time (UPR = 1.65; 95% CI = 1.18, 2.29) or all the time (UPR = 1.68; 95% CI = 1.23, 2.28) compared with women who never lived on the street or in a shelter.
After controlling for the significant relationships found in the unadjusted analysis, the relationship between travel-phase sexual violence and recent transactional sex was attenuated but remained statistically significant (adjusted prevalence ratio [APR] = 1.38; 95% CI = 1.07, 1.77). Receiving social support also remained a statistically significant protective factor after controlling for the included covariates, with a 1 unit increase in the social support score corresponding to a 16% reduction in risk (APR = 0.84; 95% CI = 0.75, 0.95). To test whether social support acts as an effect modifier on the relationship between travel-phase sexual violence and destination-phase transactional sex, we entered a term for the interaction of social support and sexual violence into the multivariable model (APR = 0.85; 95% CI = 0.66, 1.10; Table 3). Discussions in the statistical literature have argued that interaction terms in nonlinear models should not be evaluated on the basis of the magnitude or statistical significance of the coefficient.27 Therefore, we estimated the marginal effect of experiencing sexual violence on predicted probabilities for engagement in transactional sex from this model across the range of social support scores.
TABLE 3—
Adjusted Prevalence Ratios (APRs) for Transactional Sex With One’s Most Recent Sexual Partner by Level of Social Support: Cape Town, South Africa, 2012
| Low Social Supporta (n = 380) |
Moderate to High Social Supportb (n = 384) |
||||||
| Sexual Violence During Migration | Full Sample (n = 764), APR (95% CI) | Any Transactional Sex (n = 159), % (No.) | No Transactional Sex (n = 221), % (No.) | APR (95% CI) | Any Transactional Sex (n = 126), % (No.) | No Transactional Sex (n = 258), % (No.) | APR (95% CI) |
| Did not experience | 1.0 (Ref) | 76.1 (121) | 92.8 (205) | 1.0 (Ref) | 90.5 (114) | 95.7 (247) | 1.0 (Ref) |
| Experienced | 2.06 (1.13, 3.75) | 23.9 (38) | 7. 2 (16) | 1.56 (1.22, 2.00) | 9.5 (12) | 4.3 (11) | 1.04 (0.58, 1.87) |
Note. CI = confidence interval; MOS = Medical Outcomes Study. All models were adjusted for age, living situation in South Africa, recent migrant status, push–pull factor, number of partners in the past 3 mo, and alcohol use. For level of social support, interaction of experienced sexual violence during migration process and social support score was 0.85 (0.66–1.10).
Score < 3 on the MOS Social Support Scale.
Score ≥ 3 on the MOS Social Support Scale.
Figure 1 displays these results graphically to aid in interpretation. Table A (available as a supplement to the online version of this article at http://www.ajph.org) provides predicted probabilities at 4 different cutpoints in the social support scale score. At a social support scale score of 1.25, there is an estimated 34-percentage-point increase in the predicted probability of engaging in transaction sex for women who experienced travel-phase sexual violence versus those who did not (sexual violence: predicted probability = 0.84; 95% CI = 0.64, 1.04 vs non sexual violence: predicted probability = 0.50; 95% CI = 0.38, 0.62). However, this gap decreases as social support scale scores increase, which suggests that perceived social support does attenuate the relationship between sexual violence and transactional sex. At a score of 4.25, the difference in predicted probabilities of engaging in transactional sex by experience of sexual violence is minimal and not statistically significant (sexual violence: predicted probability = 0.34; 95% CI = 0.16, 0.51; no sexual violence: predicted probability = 0.32; 95% CI = 0.24, 0.40).
FIGURE 1—
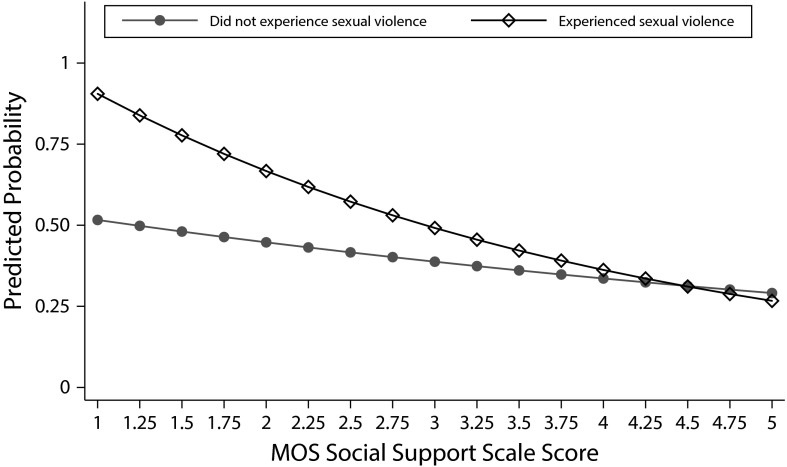
Predicted Marginal Effects of Increasing Levels of Social Support on the Predicted Probability of Engaging in Destination-Phase Transactional Sex by Experience of Sexual Violence During the Migration Process
Note. MOS = Medical Outcomes Study.
To further test whether perceived social support acts as an effect modifier of this relationship, we conducted a stratified analysis (Table 3). We ran separate models among the subgroup of participants who received low levels of social support (social support score < 3; n = 380) and the subgroup who received moderate to high levels (social support score ≥ 3; n = 384). We adjusted all models for age, living situation in South Africa, recent migrant status, push–pull factor, number of partners in the past 3 months, and alcohol use.
The stratified analysis revealed an increased risk of recent transactional sex among the low social support group, with women who experienced travel-phase sexual violence being 1.56 times more likely to engage in transaction sex in Cape Town after adjusting for the included covariates (APR = 1.56; 95% CI = 1.22, 2.00). Among women who received moderate to high levels of social support, the relationship between sexual violence and recent transactional sex was no longer statistically significant in the adjusted model (APR = 1.04; 95% CI = 0.58, 1.87).
DISCUSSION
More than a third of the study sample reported engaging in transactional sex with their most recent sexual partner, and 1 in 10 women reported experiencing sexual violence during their migration to South Africa. Both of these estimates are higher than the reported prevalence of transactional sex and sexual violence among general populations of women in South Africa.11,28 The health-associated consequences of these events are myriad and may include physical symptoms and injuries, mental health trauma, and transmission of HIV and other sexually transmitted infections.29
We found a strong relationship between travel-phase sexual violence and recent transactional sex in Cape Town. This finding is supported by previous research connecting prior traumatic sexual experiences with current risk behaviors.8–11 Although histories of premigration trauma among women have been shown to be associated with sexual risk behaviors after migration,30 this is among the first studies to explicitly link these 2 highly prevalent migration-related risks among migrant women.
We also add to the literature documenting the protective effects of social support. We observed a persistent negative relationship between perceived social support and recent transactional sex. It may be that women with higher levels of support are more likely to rely on social network members for tangible goods and services than to receive them through transactional sex. Social support was shown to act as an effect modifier on the relationship between travel-phase sexual violence and destination-phase transactional sex. In the stratified analysis, migrant women in the low social support group who experienced sexual violence during their journey to South Africa remained more likely to engage in recent transactional sex in Cape Town. However, this relationship did not exist among women in the moderate to high social support group.
Social support’s influence on health outcomes and behaviors has been hypothesized to occur through 2 pathways: either it can have a direct impact on health outcomes regardless of an individual’s psychological status, or it can buffer the negative impact of events.31 In the context of this study, social support’s influence on the relationship between travel-phase sexual violence and destination-phase transactional sex is likely operating through the buffering hypothesis. Evidence suggests that psychological consequences of sexual violence, such as posttraumatic stress disorder and depression, may mediate the relationship between previous sexual trauma and sexual risk behavior.30,32 Furthermore, some have suggested that experiences of sexual violence have the potential to instill the idea that sex is a commodity to be exchanged for goods or other services.33 Thus, the differential impact of travel-phase sexual violence by level of social support may stem from the influence of social support on the psychological effects of experiencing sexual violence. Receiving social support may help to buffer the intensity of these psychological consequences or even prevent them from occurring.
Limitations
Although we attempted to assess sexual risk factors at 2 separate migration phases, survey length and time restraints did not allow an exhaustive assessment of risks during all the phases of the migration process. This is problematic because risk behaviors and social support in the predeparture phase also likely have important effects on both travel- and destination-phase risks. For example, women who engaged in transactional sex in the predeparture phase are a particularly vulnerable subgroup, and this vulnerability could also have placed them at higher risk for travel-phase sexual violence and destination-phase transactional sex. Furthermore, the cross-sectional nature of our analysis did not allow us to investigate any causal links between travel-phase sexual violence and destination-phase transactional sex, only associations.
Several study limitations likely led to an underestimation of the true prevalence of transactional sex and sexual violence in this population. First, self-report of sensitive behaviors and traumatic events is often subject to underreporting bias. Second, we used a narrow definition of sexual violence. It is likely that a larger proportion of women experienced other types of travel-phase sexual violence. Finally, measuring transactional sex only with one’s most recent partner likely resulted in underestimation, especially for migrants who had been living in South Africa for long periods of time. Because respondent-driven sampling relies on recruitment through social networks, it may have underrepresented some subgroups of women who are isolated from the larger network of female migrants in Cape Town. This includes younger women, women in controlling relationships, and women who very recently arrived in Cape Town.
Conclusions
Research is needed that further investigates the relationships between sexual risk factors throughout the migration process using longitudinal methods. Our study results have implications for the design of interventions aimed at decreasing sexual risk among transnational migrant women. A large proportion of women reported engaging in transactional sex. This suggests a need for interventions aimed at providing safe housing options and increasing economic opportunities for migrant women in the hopes that women may be less likely to turn to transactional sex partners for tangible goods and services.
Furthermore, there is a critical need for efforts to prevent the occurrence of sexual violence against female migrants, such as making resources available that increase the likelihood of migrant women’s safe passage. These efforts include providing temporary shelter, food, and medical services along frequently traveled migration routes, regardless of whether women are traveling by documented or undocumented means, and it is essential that these efforts occur both within and between South Africa and sending communities.
Interventions that employ strategies such as creating activities that promote group membership, running support groups, and providing participatory training have been shown to be effective in increasing social support and social capital among women in South Africa.34,35 These interventions have also been shown to be successful in reducing depression and intimate partner violence among women.34,35 Thus, another potential intervention strategy is to help increase social support for migrant women once they arrive in South Africa, with the hope that this increased support will help buffer any negative psychological effects resulting from travel-phase sexual violence or other trauma. Organizations that currently provide services for migrants and are well trusted in the community may be most effective in delivering these interventions.
Finally, the additive effect of a 3-pronged approach that aims to increase economic stability, reduce sexual violence, and increase social support for migrant women might be an especially effective strategy in reducing the prevalence of transactional sex among female transnational migrants in South Africa. Future research is also needed to assess the appropriateness of these intervention strategies among other migrant populations.
ACKNOWLEDGMENTS
This research was supported by the President’s Emergency Plan for AIDS Relief through the Centers for Disease Control and Prevention ([CDC] cooperative agreement 5U2GPS001137-4).
Note. The findings and conclusions in this research are those of the authors and do not necessarily represent the official position of the CDC.
HUMAN PARTICIPANT PROTECTION
The University of Cape Town Research Ethics Committee and New York University’s University Committee on Activities Involving Human Subjects approved this study. We obtained written informed consent from all participants.
REFERENCES
- 1.Weine SM, Kashuba A. Labor migration and HIV risk: a systematic review of the literature. AIDS Behav. 2012;16(6):1605–1621. doi: 10.1007/s10461-012-0183-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen XS, Peeling RW, Yin YP, Mabey DC. The epidemic of sexually transmitted infections in China: implications for control and future perspectives. BMC Med. 2011;9:111. doi: 10.1186/1741-7015-9-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Camlin CS, Hosegood V, Newell M, McGrath N, Bärnighausen T, Snow R. Gender, migration and HIV in rural KwaZulu-Natal, South Africa. PLoS One. 2010;5(7):e11539. doi: 10.1371/journal.pone.0011539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liu H, Li X, Stanton B et al. Risk factors for sexually transmitted disease among rural-to-urban migrants in China: implications for HIV/sexually transmitted disease prevention. AIDS Patient Care STDS. 2005;19(1):49–57. doi: 10.1089/apc.2005.19.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Harcourt C, Donovan B. The many faces of sex work. Sex Transm Infect. 2005;81(3):201–206. doi: 10.1136/sti.2004.012468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jewkes R, Dunkle K, Nduna M et al. Factors associated with HIV sero-status in young rural South African women: connections between intimate partner violence and HIV. Int J Epidemiol. 2006;35(6):1461–1468. doi: 10.1093/ije/dyl218. [DOI] [PubMed] [Google Scholar]
- 7.Zembe YZ, Townsend L, Thorson A et al. “Money talks, bullshit walks” interrogating notions of consumption and survival sex among young women engaging in transactional sex in post-apartheid South Africa: a qualitative enquiry. Global Health. 2013;9:28. doi: 10.1186/1744-8603-9-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kalichman SC, Gore-Felton C, Benotsch E, Cage M, Rompa D. Trauma symptoms, sexual behaviors, and substance abuse: correlates of childhood sexual abuse and HIV risks among men who have sex with men. J Child Sex Abus. 2004;13(1):1–15. doi: 10.1300/J070v13n01_01. [DOI] [PubMed] [Google Scholar]
- 9.Simoni JM, Sehgal S, Walters KL. Triangle of risk: urban American Indian women’s sexual trauma, injection drug use, and HIV sexual risk behaviors. AIDS Behav. 2004;8(1):33–45. doi: 10.1023/b:aibe.0000017524.40093.6b. [DOI] [PubMed] [Google Scholar]
- 10.Shannon K, Kerra T, Allinottc S, Chettiarc J, Shovellerb J, Tyndalla M. Social and structural violence and power relations in mitigating HIV risk of drug-using women in survival sex work. Soc Sci Med. 2008;66(4):911–921. doi: 10.1016/j.socscimed.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 11.Dunkle KL, Jewkes RK, Brown HC, Gray GE, McIntryre JA, Harlow SD. Transactional sex among women in Soweto, South Africa: prevalence, risk factors and association with HIV infection. Soc Sci Med. 2004;59(8):1581–1592. doi: 10.1016/j.socscimed.2004.02.003. [DOI] [PubMed] [Google Scholar]
- 12.Krishnan S, Dunbar M, Minnis A, Medlin C, Gerdts C, Padianac N. Poverty, gender inequities, and women’s risk of human immunodeficiency virus/AIDS. Ann N Y Acad Sci. 2008;1136:101–110. doi: 10.1196/annals.1425.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bronfman MN, Leyva R, Negroni MJ, Rueda CM. Mobile populations and HIV/AIDS in Central America and Mexico: research for action. AIDS. 2002;16(suppl 3):S42–S49. doi: 10.1097/00002030-200212003-00007. [DOI] [PubMed] [Google Scholar]
- 14.Algasseer N, Dresden E, Keeney G, Warren N. Status of women and infants in complex humanitarian emergencies. J Midwifery Womens Health. 2004;49(4 suppl 1):7–13. doi: 10.1016/j.jmwh.2004.05.001. [DOI] [PubMed] [Google Scholar]
- 15.Becker JU, Theodosis C, Kulkarni R. HIV/AIDS, conflict and security in Africa: rethinking relationships. J Int AIDS Soc. 2008;11(1):3. doi: 10.1186/1758-2652-11-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Campbell C. Selling sex in the time of AIDS: the psychosocial context of condom use by sex workers on a Southern African mine. Soc Sci Med. 2000;50(4):479–494. doi: 10.1016/s0277-9536(99)00317-2. [DOI] [PubMed] [Google Scholar]
- 17.Latkin CA, Hua W, Forman VL. The relationship between social network characteristics and exchanging sex for drugs or money among drug users in Baltimore, MD, USA. Int J STD AIDS. 2003;14(11):770–775. doi: 10.1258/09564620360719831. [DOI] [PubMed] [Google Scholar]
- 18.Coker AL, Watkins KW, Smith PH, Brandt HM. Social support reduces the impact of partner violence on health: application of structural equation models. Prev Med. 2003;37(3):259–267. doi: 10.1016/s0091-7435(03)00122-1. [DOI] [PubMed] [Google Scholar]
- 19.Deren S, Shedlin M, Kang SY, Cortes DE. HIV risk and prevention among Hispanic immigrants in New York: the salience of diversity. Subst Use Misuse. 2011;46(2–3):254–263. doi: 10.3109/10826084.2011.523215. [DOI] [PubMed] [Google Scholar]
- 20.Munyewende P, Rispel LC, Harris B, Chersich M. Exploring perceptions of HIV risk and health service access among Zimbabwean migrant women in Johannesburg: a gap in health policy in South Africa? J Public Health Policy. 2011;32(suppl 1):S152–S161. doi: 10.1057/jphp.2011.36. [DOI] [PubMed] [Google Scholar]
- 21.Zimmerman C, Kiss L, Hossain M. Migration and health: a framework for 21st century policy-making. PLoS Med. 2011;8(5):e1001034. doi: 10.1371/journal.pmed.1001034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Townsend L, Giorgio M, Zembe Y, Cheyip M, Mathews C. HIV prevalence and risk behaviours among foreign migrant women residing in Cape Town, South Africa. AIDS Behav. 2014;18(10):2020–2029. doi: 10.1007/s10461-014-0784-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Heckathorn D. Respondent driven sampling: a new approach to the study of hidden populations. Soc Probl. 1997;44(2):174–199. [Google Scholar]
- 24.Salganik M, Heckathorn D. Sampling and estimation in hidden populations using respondent-driven sampling. Sociol Methodol. 2004;34(1):193–240. [Google Scholar]
- 25.Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J Pers Assess. 1990;55(3–4):610–617. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]
- 26.Rees CA, Karter AJ, Young BA. Race/ethnicity, social support, and associations with diabetes self-care and clinical outcomes in NHANES. Diabetes Educ. 2010;36(3):435–445. doi: 10.1177/0145721710364419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ai C, Norton EC. Interaction terms in logit and probit models. Econ Lett. 2003;80(1):123–129. [Google Scholar]
- 28.Jewkes R, Abrahams N. The epidemiology of rape and sexual coercion in South Africa: an overview. Soc Sci Med. 2002;55(7):1231–1244. doi: 10.1016/s0277-9536(01)00242-8. [DOI] [PubMed] [Google Scholar]
- 29.Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331–1336. doi: 10.1016/S0140-6736(02)08336-8. [DOI] [PubMed] [Google Scholar]
- 30.Steel J, Herlitz C, Matthews J et al. Pre-migration trauma and HIV-risk behavior. Transcult Psychiatry. 2003;40(1):91–108. doi: 10.1177/1363461503040001006. [DOI] [PubMed] [Google Scholar]
- 31.Cohen S. Psychosocial models of the role of social support in the etiology of physical disease. Health Psychol. 1988;7(3):269–297. doi: 10.1037//0278-6133.7.3.269. [DOI] [PubMed] [Google Scholar]
- 32.Nduna M, Jewkes R, Dunkle K, Shai N, Colman I. Associations between depressive symptoms, sexual behaviour and relationship characteristics: a prospective cohort study of young women and men in the Eastern Cape, South Africa. J Int AIDS Soc. 2010;13(1):44. doi: 10.1186/1758-2652-13-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kalmuss D. Nonvolitional sex and sexual health. Arch Sex Behav. 2004;33(3):197–209. doi: 10.1023/B:ASEB.0000026620.99306.64. [DOI] [PubMed] [Google Scholar]
- 34.Petersen I, Bhana A, Baillie K. The feasibility of adapted group-based interpersonal therapy (IPT) for the treatment of depression by community health workers within the context of task shifting in South Africa. Community Ment Health J. 2012;48(3):336–341. doi: 10.1007/s10597-011-9429-2. [DOI] [PubMed] [Google Scholar]
- 35.Pronyk PM, Hargreaves JR, Kim JC et al. Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: a cluster randomised trial. Lancet. 2006;368(9551):1973–1983. doi: 10.1016/S0140-6736(06)69744-4. [DOI] [PubMed] [Google Scholar]