

Abstract
Background
Cardiovascular outcomes vary between urban and rural hospitals, with worse outcomes in rural settings.
Objectives
To examine if in-hospital mortality for hospitalization for atrial fibrillation (AF) varied between urban and rural hospitals.
Methods
A cross-sectional examination of patients who were hospitalized for AF was performed in the National Inpatient Sample (NIS) between 2012 and 2014 to compare in-hospital mortality in patients admitted to urban versus rural hospitals. Patients with a principal International Classification of Diseases, 9th Revision discharge diagnosis of AF were included. Hospitals were classified as urban or rural based on core-based statistical areas. In-hospital mortality was defined as death due to any cause.
Results
A total of 248,731 (mean age=69 years; 78% white; 48% female) admissions for AF were identified. Of these, 218,946 (88%) were from urban hospitals and 29,785 (12%) were from rural hospitals. Patients admitted to rural hospitals had a 17% increased risk of death compared with urban hospitals in a multivariable model which accounted for differences in patient characteristics and potential confounders (OR=1.17, 95%CI=1.04, 1.32). Similar results were obtained in a propensity score-matched analysis, and in subgroup analyses by sex, race, and region.
Conclusions
In-hospital mortality for AF is higher in rural compared with urban hospitals. Further research is needed to understand this finding, and to develop targeted strategies to reduce mortality in patients admitted for AF in rural hospitals.
Keywords: rural, atrial fibrillation, hospitalization, in-hospital mortality, outcomes
INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia encountered by the practicing clinician, with an estimated prevalence of 3 to 6 percent in the United States.1 A recent examination of national hospitalization rates for AF has shown that AF hospitalizations have increased exponentially in the United States from 2000 to 2010.2 Despite the reported increases in AF hospitalizations, the in-hospital mortality among those admitted has decreased.2
Several reports have suggested that the quality of care, and subsequently the outcomes for patients admitted for cardiovascular diseases, varies between urban and rural hospitals.3–8 Whether differences for in-hospital mortality also exist in patients admitted for AF is currently unknown. Less than optimal care of AF patients has been reported in rural compared with urban areas,9 which supports the possibility of poorer outcomes in AF patients admitted to rural hospitals. Therefore, we examined the influence of rurality on in-hospital mortality among patients hospitalized for AF using data from the National Inpatient Sample (NIS), a national all-payer administrative database.
METHODS
Study Design and Cohort
NIS is a database of a sample of discharged patients from United States community hospitals. The NIS approximates a 20-percent stratified sample of all discharges, and excludes rehabilitation and long-term acute care hospitals. NIS data is drawn from 44 states, plus the District of Columbia, representing more than 96 percent of the United States population. Due to the complex study design, sampling weights are provided to compute national estimates. NIS contains clinical and nonclinical data elements for each hospital stay, including the following: primary and secondary diagnoses and procedures; patient demographic data; hospital characteristics; expected payment source; total charges; discharge status; length of stay; and severity and comorbidity measures. Inpatient data are typically available from discharge abstracts. The NIS contains information on all patients, regardless of payer. Researchers and policymakers use the NIS to make national estimates of health care utilization, access, charges, quality, and outcomes, and data are available from 1988 through 2014. The database is maintained by the Agency for Healthcare Research and Quality (AHRQ). Annual data quality assessments of the NIS are routinely performed to guarantee the internal validity of the database.
This analysis was a cross-sectional examination of the NIS database of AF hospitalizations between 2012 and 2014 to determine if admission to a rural hospital was associated with an increased risk of in-hospital mortality compared with patients admitted to urban hospitals. Hospitalizations with a primary diagnosis code of AF were included, and we did not consider patients with secondary codes for AF. AF diagnoses were identified by International Classification of Diseases, 9th Revision Codes 427.31 and 427.32. We included all AF hospitalizations in patients ≥18 years of age. Patients with missing age, sex, or in-hospital mortality data were excluded. Additionally, to obtain accurate in-hospitality mortality data for the hospital of admission, patients who were transferred to another acute care hospital at the time of discharge were excluded. This included transfer to a different acute care hospital or other health facility (e.g., skilled nursing facility). This study was approved by the institutional review board at Emory University.
Hospital and Patient Characteristics
Patient data included age, sex, race (e.g., white, black, and other), and insurance status (e.g., Medicare, Medicaid, Private, Self-pay/other). Urban-rural classification of hospitals was based on core based statistical area (CBSA) codes. Hospitals residing in counties with a CBSA type of metropolitan (areas that contain at least 1 urbanized area of 50,000 or more population) were considered urban, while hospitals with a CBSA type of micropolitan (at least one urban cluster that has a population of 10,000–50,000) or non-core (not metropolitan or mircopolitan) were classified as rural.10 Hospitals were also classified according to Census regions: Northeast; Midwest; South; and West. Comorbid conditions were identified by the AHRQ comorbidity database. The identification of these conditions are based on International Classification of Diseases-9-CM diagnoses and diagnosis-related group information listed on the discharge record. Using the standard logic of the Elixhauser Comorbidity Software,11 coexisting medical conditions are identified that are not directly related to the principal diagnosis, or main reason for admission, and are likely to represent conditions that originated prior to admission. Comorbid conditions identified from administrative claims data generally agree with patient chart data for recording of comorbidities,12 and similar methods were used by the Centers for Medicare and Medicaid Services for calculating their 30-day heart failure mortality measure.13 The following comorbid conditions were included in this analysis: obesity, hypertension, diabetes, heart failure, chronic lung disease, peripheral vascular disease, renal failure, liver disease, hypothyroidism, depression, alcohol abuse, and anemia.
Outcomes
The main outcome of interest was in-hospital mortality which was defined as death due to any cause during hospitalization. AF procedures during the same hospitalization were identified by International Classification of Diseases, 9th Revision Codes and included external electrical cardioversion (99.61) and catheter ablation (37.34). We also examined the 5 most common secondary diagnoses for patients hospitalized for AF. International Classification of Diseases, 9th Revision Codes were used to identify these diagnoses, and the following were identified in the overall AF cohort: heart failure (428.xx), hypertension (401.xx), hyperlipidemia (272.xx), diabetes (250.xx), and acute kidney injury (584.xx).
Statistics
Baseline characteristics were compared by urban-rural status. Survey-specific statements (SURVEYFREQ, SURVEYMEANS) were used to obtain descriptive statistics. Statistical significance for continuous variables was tested using the t-test procedure and the Rao-Scott chi-square method for categorical variables. The frequencies of external electrical cardioversions and catheter ablations also were compared by rural versus urban status, and in subgroups of sex (men vs. women), race (white, black, other), and region (Northwest, Midwest, South, and West). A multivariable logistic regression model for survey data (SURVEYLOGISTIC) was used to compute the multivariable risk of death in patients admitted for AF in rural versus urban hospitals, accounting for hospital-level clustering of patients and the sampling design using CLUSTER and STRATA statements, respectively. The multivariable model included the following covariates: age, sex, race, insurance, hospital region, obesity, hypertension, diabetes, heart failure, chronic lung disease, peripheral vascular disease, renal failure, liver disease, hypothyroidism, depression, alcohol abuse, and anemia. We also performed a propensity score-matched analysis using multivariable logistic regression to predict the probability of being seen in rural versus urban hospitals using the same covariates in the primary analysis, and a 1:1 matching was performed (N=58,896). The primary analysis was then repeated in the propensity score-matched cohort. A sensitivity analysis was performed by excluding patients who had either external electrical cardioversion or catheter ablation due to the relatively low mortality rate associated with these procedures. Secondary analyses were performed to determine if the in-hospital risk of death associated varied by sex, race, or region, by computing interaction terms. An additional analysis also was performed to determine if the 5 most common secondary diagnoses identified in the total cohort varied by rural versus urban hospital status. Statistical significance, including interaction terms, was defined as p < 0.05. Data were analyzed using SAS Version 9.4 (Cary, NC).
RESULTS
A total of 285,138 admissions with a primary AF diagnosis were identified between 2012 and 2014. There were 36,407 patients who were transferred to different facilities at discharge. Patients from rural hospitals were more likely to be transferred to a different acute care hospital at discharge than those seen in urban hospitals (18% vs. 12%; p<0.001). The final sample included 248,731 (mean age=69 years; 78% white; 48% female) admissions for AF. There were 218,946 (88%) AF admissions from urban hospitals and 29,785 (12%) AF admissions from rural hospitals. The baseline characteristics of AF hospitalizations stratified by rural versus urban status are shown in Table 1. The baseline characteristics of the propensity score-matched cohort are shown in Supplemental Table 1.
Table 1.
Patient Characteristics (N=248,731)
| Characteristic | Urban Hospital (n=218,946) |
Rural Hospital (n=29,785) |
P-value* |
|---|---|---|---|
|
| |||
| Age, mean, years (SE) | 69 (0.04) | 70 (0.08) | <0.001 |
|
| |||
| Female (%) | 48 | 52 | <0.001 |
|
| |||
| Race | |||
| White (%) | 77 | 84 | |
| Black (%) | 8 | 4 | |
| Other (%) | 15 | 12 | <0.001 |
|
| |||
| Payment type | |||
| Medicare (%) | 64 | 70 | |
| Medicaid (%) | 5 | 4 | |
| Private (%) | 25 | 20 | |
| Self-pay or other (%) | 6 | 6 | <0.001 |
|
| |||
| Region | |||
| Northeast (%) | 21 | 14 | |
| Midwest (%) | 24 | 32 | |
| South (%) | 39 | 45 | |
| West (%) | 16 | 9 | <0.001 |
|
| |||
| Obesity (%) | 18 | 16 | <0.001 |
|
| |||
| Hypertension (%) | 70 | 70 | 0.20 |
|
| |||
| Diabetes (%) | 26 | 27 | <0.001 |
|
| |||
| Heart failure (%) | <1 | <1 | 0.69 |
|
| |||
| Chronic lung disease (%) | 22 | 26 | <0.001 |
|
| |||
| Peripheral vascular disease (%) | 7 | 6 | 0.010 |
|
| |||
| Renal failure %) | 14 | 13 | <0.001 |
|
| |||
| Liver disease (%) | 1.9 | 1.6 | <0.001 |
|
| |||
| Hypothyroidism (%) | 16 | 17 | <0.001 |
|
| |||
| Depression (%) | 8 | 10 | <0.001 |
|
| |||
| Alcohol abuse (%) | 5 | 4 | <0.001 |
|
| |||
| Anemia (%) | 12 | 12 | 0.38 |
Statistical significance tested using the t-test procedure for continuous data and the Rao-Scott chi-square test for categorical data.
SE=standard error.
Urban hospitals were more likely to report direct external electrical cardioversion and catheter ablation procedures than rural hospitals (Table 2). The percentage of AF admissions that used these procedures did not vary by sex, race, or region (Table 2).
Table 2.
Atrial Fibrillation Procedures Performed during Hospitalization
| Procedure | Urban | Rural | P-value* |
|---|---|---|---|
|
| |||
| External Electrical Cardioversion (%) | 8 | 4 | <0.001 |
|
| |||
| Sex | |||
| Men (%) | 9 | 5 | <0.001 |
| Female (%) | 6 | 3 | <0.001 |
|
| |||
| Race | |||
| White (%) | 8 | 4 | <0.001 |
| Black (%) | 6 | 2 | <0.001 |
| Other (%) | 6 | 4 | 0.001 |
|
| |||
| Region | |||
| Northwest (%) | 9 | 6 | <0.001 |
| Midwest (%) | 9 | 5 | <0.001 |
| South (%) | 7 | 2 | <0.001 |
| West (%) | 6 | 3 | <0.001 |
|
| |||
| Catheter Ablation (%) | 9 | 1 | <0.001 |
|
| |||
| Sex | |||
| Men (%) | 11 | 2 | <0.001 |
| Female (%) | 7 | 1 | <0.001 |
|
| |||
| Race | |||
| White (%) | 9 | 1 | <0.001 |
| Black (%) | 8 | 1 | <0.001 |
| Other (%) | 9 | 1 | <0.001 |
|
| |||
| Region | |||
| Northwest (%) | 9 | 3 | <0.001 |
| Midwest (%) | 9 | 1 | <0.001 |
| South (%) | 9 | 1 | <0.001 |
| West (%) | 9 | <1 | <0.001 |
Statistical significance tested using the Rao-Scott chi-square test.
AF=atrial fibrillation.
The proportion of patients who died during hospitalization for AF in rural and urban hospitals are shown in (Figure 1). A higher percentage of patients admitted for AF died in rural versus urban hospitals (1.3% vs. 1.0%, p<0.001) (Figure 1). Patients admitted to rural hospitals (OR=1.17, 95%CI=1.04, 1.32) had an increased risk of death compared with urban hospitals in our multivariable model which accounted for differences in patient characteristics (Table 3). The risk of death among patients admitted to rural hospitals remained increased compared with urban hospitals after exclusion of patients who had either external electrical cardioversion or catheter ablation procedures performed (OR=1.14, 95%CI=1.01, 1.28). Similar results were observed in a propensity score-matched cohort, and in subgroup analyses by sex, race, and region (Table 3). Additionally, differences were observed in the 5 most common secondary diagnoses. Patients admitted to urban hospitals for AF were more likely to have secondary diagnoses of heart failure, hyperlipidemia, and acute kidney injury than those from rural hospitals (Table 4).
Figure 1. In-Hospital Morality Associated with Atrial Fibrillation Hospitalization, 2012–2014.
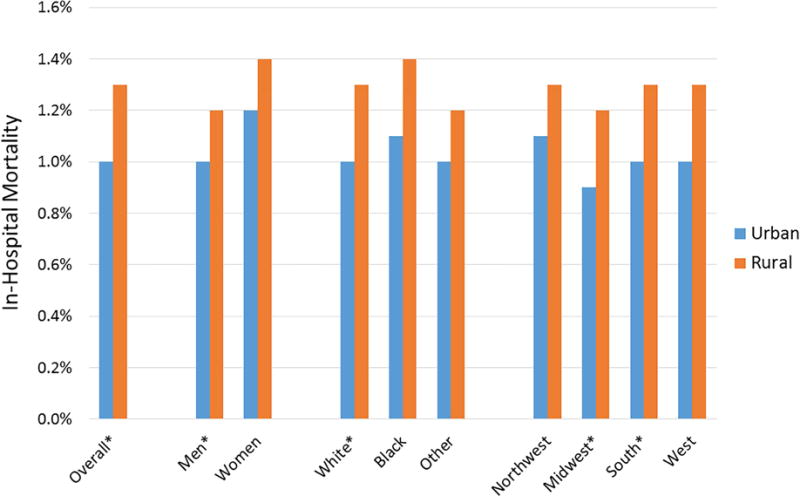
*Statistically significant difference (p<0.05) and comparisons made using the Rao-Scott chi-square test.
AF=atrial fibrillation.
Table 3.
Risk of In-Hospital Mortality Associated with Hospitalization for Atrial Fibrillation in Rural versus Urban Hospitals*
| Group | OR† (95%CI) |
P-interaction | OR‡ (95%CI) |
P-interaction |
|---|---|---|---|---|
|
| ||||
| All | 1.17 (1.04, 1.32) | 1.19 (1.01, 1.39) | ||
|
| ||||
| Sex | ||||
| Men | 1.26 (1.06, 1.50) | 0.30 | 1.41 (1.10, 1.80) | 0.10 |
| Women | 1.11 (0.96, 1.29) | 1.06 (0.87, 1.30) | ||
|
| ||||
| Race | ||||
| White | 1.18 (1.04, 1.34) | 0.75 | 1.23 (1.03, 1.46) | 0.48 |
| Black | 1.13 (0.66, 1.94) | 0.68 (0.31, 1.48) | ||
| Other | 1.07 (0.77, 1.49) | 1.12 (0.72, 1.74) | ||
|
| ||||
| Region | ||||
| Northwest | 1.12 (0.83, 1.52) | 0.78 | 1.17 (0.76, 1.79) | 0.60 |
| Midwest | 1.25 (1.01, 1.54) | 1.39 (1.03, 1.86) | ||
| South | 1.12 (0.94, 1.33) | 1.11 (0.88, 1.41) | ||
| West | 1.26 (0.88, 1.80) | 1.11 (0.68, 1.81) | ||
Estimates represent the odds of death in rural compared with urban hospitals in the overall sample and in subgroups.
Adjusted for age, sex, race, insurance, hospital region, obesity, hypertension, diabetes, heart failure, chronic lung disease, peripheral vascular disease, renal failure, liver disease, hypothyroidism, depression, alcohol abuse, and anemia.
Results of 1:1 propensity score-matched analysis. Propensity score was computed using multivariable logistic regression with the following variables: age, sex, race, insurance, hospital region, obesity, hypertension, diabetes, heart failure, chronic lung disease, peripheral vascular disease, renal failure, liver disease, hypothyroidism, depression, alcohol abuse, and anemia (N=58,896).
CI=confidence interval; OR=odds ratio.
Table 4.
Five Most Common Secondary Diagnoses
| Diagnosis | Total | Urban | Rural | P-value* |
|---|---|---|---|---|
| Heart failure (428.XX) | 16.7 | 16.7 | 16.1 | 0.048 |
| Hypertension (401.XX) | 7.0 | 6.9 | 7.9 | <0.001 |
| Hyperlipidemia (272.XX) | 4.4 | 4.5 | 3.2 | <0.001 |
| Diabetes (250.XX) | 3.8 | 3.8 | 3.6 | 0.38 |
| Acute kidney injury (584.XX) | 2.9 | 3.0 | 2.2 | <0.001 |
Statistical significance tested using the Rao-Scott chi-square test. Comparisons made between urban and rural AF hospitalizations.
AF=atrial fibrillation.
DISCUSSION
In this analysis from NIS, the risk of in-hospital mortality for patients admitted for AF was higher in rural compared with urban hospitals. Our findings did not vary by sex, race, or region. Additionally, we observed urban-rural differences in the utilization of common AF procedures. Overall, our data suggest that urban-rural differences exist in the care for patients who are hospitalized for AF.
The risk of in-hospital mortality for patients admitted for AF has decreased over recent years.2 Explanations for the observed decline, despite an increasing number of hospitalizations,2 are related to temporal differences in AF treatment. For example, rates of external electrical cardioversion have increased, and this therapy was associated with reductions in hospital mortality for patients admitted for AF.14 Additionally, the use of catheter ablation has increased in the United States.15 Furthermore, due to the fact that patients hospitalized for AF are likely to die from cardiovascular complications,16 improvements in overall cardiovascular care in the United States possibly explain the mortality reduction observed in AF hospitalization.17, 18
Despite recent reductions in hospital mortality for patients with AF, the findings of the current analysis suggest that urban-rural differences exists in the risk of death among patients who are hospitalized for AF. The reasons for the increased risk of death in rural hospitals are unclear. However, differences in practice patterns possible explain this finding. The utilization of external electrical cardioversion and catheter ablation varied greatly between urban and rural hospitals. Although the indications for these procedures will depend on individual patient characteristics (e.g., elective versus non-elective admission), the urban-rural differences observed in the percentage of patients who received these therapies likely reflects variation in treatment selection. Additionally, patients in rural communities are less likely to receive care from specialists,19 and this would explain the lower proportion of patients who received these common AF procedures in rural hospitals. This also suggests that urban-rural differences exist in the overall care for hospitalized patients with AF. Furthermore, we identified heart failure as the most common secondary diagnosis in rural and urban patients. Due to the known urban-rural differences in the care of heart failure patients,6, 8 it is possible that the care for this common comorbid condition varied between rural and urban patients, and negatively influenced hospital survival in AF patients from rural settings.
Urban-rural differences in the care for patients with cardiovascular diseases have been well-described.3–8 Our data extend prior literature to include the care for the hospitalized patient with AF. This finding has important implications for clinical care, as we have identified a group of patients in which hospital outcomes vary greatly by urban-rural status. Therefore, hospitalization for AF possibly represents an area for practice improvement in rural hospitals. This is extremely important as patients in rural regions do not rely on the majority of their care from urban centers.19 Additionally, these data are of interest to policy makers with aims to reduce mortality in rural regions. Residents from rural regions are more likely to rely on public sources of health insurance, and variation in quality of cardiovascular care and access to medical care exist.5, 20 This would result in AF patients who are more likely to present to a hospital for AF care rather than an outpatient clinic. Therefore, reductions in hospital mortality for AF possibly would be observed with improvements in access to care in rural regions, as they would be less likely to rely on hospital care for AF.
The current analysis should be interpreted in the context of several limitations. Hospitalizations for AF were identified by International Classification of Diseases, 9th Revision Codes, and despite the accuracy of these codes to identify AF events,21 misclassification remains a possibility. We were unable to distinguish between cases of new-onset and preexisting AF, and the results may vary by this factor. The duration of AF events (e.g., paroxysmal) was not available in our dataset, and the findings of this analysis possibly vary by this factor. Urban-rural classification of hospitals was based on CBSA codes, and this classification scheme possibly is incomplete. The AHRQ comorbidity database was used to identify comorbid conditions, and the misclassification of these conditions is possible. Additionally, we were unable to determine the cause of death, and it is possible that some of the deaths were unrelated to AF. We were not able to account for the severity of comorbid conditions that were included in our multivariable model. In an attempt to obtain accurate in-hospitality mortality data for the hospital of admission, patients were excluded if they were transferred to another acute care hospital at the time of discharge, and this method possibly was incomplete. Furthermore, the absolute mortality rates were relatively small between rural and urban hospitals, and the clinical significance remains uncertain.
In conclusion, patients admitted for AF to rural hospitals have an increased risk of mortality compared with patients admitted to urban hospitals. Further research is needed to understand the reasons for this finding, and suggest that improvement in AF care in rural hospitals is needed to further reduce the risk of mortality associated with hospital admission for AF.
Supplementary Material
Acknowledgments
None.
Funding: Research reported in this publication was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under award number F32-HL134290. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: None
References
- 1.Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. doi: 10.1001/jama.285.18.2370. [DOI] [PubMed] [Google Scholar]
- 2.Patel NJ, Deshmukh A, Pant S, et al. Contemporary trends of hospitalization for atrial fibrillation in the United States, 2000 through 2010: implications for healthcare planning. Circulation. 2014;129:2371–2379. doi: 10.1161/CIRCULATIONAHA.114.008201. [DOI] [PubMed] [Google Scholar]
- 3.Sheikh K, Bullock C. Urban-rural differences in the quality of care for medicare patients with acute myocardial infarction. Arch Intern Med. 2001;161:737–743. doi: 10.1001/archinte.161.5.737. [DOI] [PubMed] [Google Scholar]
- 4.Baldwin LM, MacLehose RF, Hart LG, Beaver SK, Every N, Chan L. Quality of care for acute myocardial infarction in rural and urban US hospitals. J Rural Health. 2004;20:99–108. doi: 10.1111/j.1748-0361.2004.tb00015.x. [DOI] [PubMed] [Google Scholar]
- 5.Baldwin LM, Chan L, Andrilla CH, Huff ED, Hart LG. Quality of care for myocardial infarction in rural and urban hospitals. J Rural Health. 2010;26:51–57. doi: 10.1111/j.1748-0361.2009.00265.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gamble JM, Eurich DT, Ezekowitz JA, Kaul P, Quan H, McAlister FA. Patterns of care and outcomes differ for urban versus rural patients with newly diagnosed heart failure, even in a universal healthcare system. Circ Heart Fail. 2011;4:317–323. doi: 10.1161/CIRCHEARTFAILURE.110.959262. [DOI] [PubMed] [Google Scholar]
- 7.Kulshreshtha A, Goyal A, Dabhadkar K, Veledar E, Vaccarino V. Urban-rural differences in coronary heart disease mortality in the United States: 1999–2009. Public Health Rep. 2014;129:19–29. doi: 10.1177/003335491412900105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Teng TH, Katzenellenbogen JM, Hung J, Knuiman M, Sanfilippo FM, Geelhoed E, Hobbs M, Thompson SC. Rural-urban differentials in 30-day and 1-year mortality following first-ever heart failure hospitalisation in Western Australia: a population-based study using data linkage. BMJ Open. 2014;4:e004724. doi: 10.1136/bmjopen-2013-004724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Flaker GC, McGowan DJ, Boechler M, Fortune G, Gage B. Underutilization of antithrombotic therapy in elderly rural patients with atrial fibrillation. Am Heart J. 1999;137:307–312. doi: 10.1053/hj.1999.v137.91403. [DOI] [PubMed] [Google Scholar]
- 10.Slifkin RT, Randolph R, Ricketts TC. The changing metropolitan designation process and rural America. J Rural Health. 2004;20:1–6. doi: 10.1111/j.1748-0361.2004.tb00001.x. [DOI] [PubMed] [Google Scholar]
- 11.Moore BJ, White S, Washington R, Coenen N, Elixhauser A. Identifying Increased Risk of Readmission and In-hospital Mortality Using Hospital Administrative Data: The AHRQ Elixhauser Comorbidity Index. Med Care. 2017;55:698–705. doi: 10.1097/MLR.0000000000000735. [DOI] [PubMed] [Google Scholar]
- 12.Quan H, Parsons GA, Ghali WA. Validity of information on comorbidity derived rom ICD-9-CCM administrative data. Med Care. 2002;40:675–685. doi: 10.1097/00005650-200208000-00007. [DOI] [PubMed] [Google Scholar]
- 13.Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, Roman S, Normand SL. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with heart failure. Circulation. 2006;113:1693–1701. doi: 10.1161/CIRCULATIONAHA.105.611194. [DOI] [PubMed] [Google Scholar]
- 14.Rochlani YM, Shah NN, Pothineni NV, Paydak H. Utilization and Predictors of Electrical Cardioversion in Patients Hospitalized for Atrial Fibrillation. Cardiol Res Pract. 2016;2016:8956020. doi: 10.1155/2016/8956020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kneeland PP, Fang MC. Trends in catheter ablation for atrial fibrillation in the United States. J Hosp Med. 2009;4:E1–5. doi: 10.1002/jhm.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fauchier L, Samson A, Chaize G, Gaudin AF, Vainchtock A, Bailly C, Cotte FE. Cause of death in patients with atrial fibrillation admitted to French hospitals in 2012: a nationwide database study. Open Heart. 2015;2:e000290. doi: 10.1136/openhrt-2015-000290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rogers WJ, Frederick PD, Stoehr E, Canto JG, Ornato JP, Gibson CM, Pollack CV, Jr, Gore JM, Chandra-Strobos N, Peterson ED, French WJ. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156:1026–1034. doi: 10.1016/j.ahj.2008.07.030. [DOI] [PubMed] [Google Scholar]
- 18.Chen J, Dharmarajan K, Wang Y, Krumholz HM. National trends in heart failure hospital stay rates, 2001 to 2009. J Am Coll Cardiol. 2013;61:1078–1088. doi: 10.1016/j.jacc.2012.11.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chan L, Hart LG, Goodman DC. Geographic access to health care for rural Medicare beneficiaries. J Rural Health. 2006;22:140–146. doi: 10.1111/j.1748-0361.2006.00022.x. [DOI] [PubMed] [Google Scholar]
- 20.Casey MM, Thiede Call K, Klingner JM. Are rural residents less likely to obtain recommended preventive healthcare services? Am J Prev Med. 2001;21:182–188. doi: 10.1016/s0749-3797(01)00349-x. [DOI] [PubMed] [Google Scholar]
- 21.Alonso A, Agarwal SK, Soliman EZ, Ambrose M, Chamberlain AM, Prineas RJ, Folsom AR. Incidence of atrial fibrillation in whites and African-Americans: the Atherosclerosis Risk in Communities (ARIC) study. Am Heart J. 2009;158:111–117. doi: 10.1016/j.ahj.2009.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.