

Abstract
Background
Lightweight and portable devices that objectively measure concussion-related impairments could improve injury detection and critical decision-making in contact sports and the military, where brain injuries commonly occur but remain underreported. Current standard assessments often rely heavily on subjective methods such as symptom self-reporting. Head-mounted wearables, such as smartglasses, provide an emerging platform for consideration that could deliver the range of assessments necessary to develop a rapid and objective screen for brain injury. Standing balance assessment, one parameter that may inform a concussion diagnosis, could theoretically be performed quantitatively using current off-the-shelf smartglasses with an internal accelerometer. However, the validity of balance measurement using smartglasses has not been investigated.
Objective
This study aimed to perform preliminary validation of a smartglasses-based balance accelerometer measure (BAM) compared with the well-described and characterized waist-based BAM.
Methods
Forty-two healthy individuals (26 male, 16 female; mean age 23.8 [SD 5.2] years) participated in the study. Following the BAM protocol, each subject performed 2 trials of 6 balance stances while accelerometer and gyroscope data were recorded from smartglasses (Glass Explorer Edition). Test-retest reliability and correlation were determined relative to waist-based BAM as used in the National Institutes of Health’s Standing Balance Toolbox.
Results
Balance measurements obtained using a head-mounted wearable were highly correlated with those obtained through a waist-mounted accelerometer (Spearman rho, ρ=.85). Test-retest reliability was high (intraclass correlation coefficient, ICC2,1=0.85, 95% CI 0.81-0.88) and in good agreement with waist balance measurements (ICC2,1=0.84, 95% CI 0.80-0.88). Considering the normalized path length magnitude across all 3 axes improved interdevice correlation (ρ=.90) while maintaining test-retest reliability (ICC2,1=0.87, 95% CI 0.83-0.90). All subjects successfully completed the study, demonstrating the feasibility of using a head-mounted wearable to assess balance in a healthy population.
Conclusions
Balance measurements derived from the smartglasses-based accelerometer were consistent with those obtained using a waist-mounted accelerometer. Additional research is necessary to determine to what extent smartglasses-based accelerometry measures can detect balance dysfunction associated with concussion. However, given the potential for smartglasses to perform additional concussion-related assessments in an integrated, wearable platform, continued development and validation of a smartglasses-based balance assessment is warranted. This approach could lead to a wearable platform for real-time assessment of concussion-related impairments that could be further augmented with telemedicine capabilities to integrate professional clinical guidance. Smartglasses may be superior to fully immersive virtual reality headsets for this application, given their lighter weight and reduced likelihood of potential safety concerns.
Keywords: postural balance, wearable technology, accelerometry, mild traumatic brain injury
Introduction
Background
Mild traumatic brain injury (mTBI), also known as concussion, is a common injury in both sports, with an estimated annual incidence of 1.6-3.8 million in the United States alone [1], and modern war, with 297,478 diagnoses in US service members between 2000 and 2016 [2]. Prompt identification of a concussed individual and removal from activity is the most effective method to facilitate rapid recovery immediately following injury [3-6]. Unrecognized and untreated mTBI can put athletes and service members at greater risk for more substantial TBI, as well as chronic encephalopathy, later [7-10]. Unfortunately, failure to detect concussions in a timely fashion is common in both the sporting arena [11,12] and military [13], as the immediate symptoms can be subtle and difficult to detect.
Concussion is considered one of the most complex injuries in sports medicine to diagnose, assess, and manage [14]. Accurate diagnosis and recovery monitoring of concussion is further complicated as recommended assessments, including the Standardized Concussion Assessment Tool (SCAT) and Military Acute Concussion Evaluation (MACE), rely heavily on patient symptom self-reporting [15]. Concussions can escape detection in committed athletes who are motivated to remain in the game [16], which further highlights the need for unbiased and objective sideline assessments [17]. In a military setting, service members who experience concussions are frequently under severe levels of physiological and emotional stress and may be unable to recognize or recall symptoms [13]. Injuries are frequently embedded in longer, continuous missions, where removing oneself from active combat to report a mild injury often does not occur [13]. Furthermore, concussion assessments commonly used in these settings, including MACE, lack diagnostic utility as early as 12 hours after injury [18]. Thus, improved, more objective methods for detection and recovery monitoring following concussions are a priority for both athletic organizations [19-21] and US Department of Defense health care providers [22-24].
Approach
Concussion diagnosis and recovery monitoring requires a multifaceted and multimodal approach [25]. Concussion results in a range of clinical signs and symptoms, including impaired movement, balance, oculomotor function, attention, memory, and emotional functioning [26]. Unbiased and objective assessments of reaction time, balance, oculomotor function, and heart rate variability using an automated, digitized platform could substantially enhance the field recognition of concussion [25,27]. Although any single measure may not be precise enough to confidently diagnose concussion, a standardized combination of these measures could produce a sufficient concussion diagnostic metric. A lightweight and portable tool combining appropriate measures in a rapid assessment battery would be useful in both contact sports and the battlefield, where fast-paced and disorganized environments often obscure incidents of injury [25,28].
Considering the variety of assessments necessary, we examined whether smartglasses, an emerging computing platform, could be leveraged to provide a lightweight, portable, and wearable solution for measuring concussion-related impairments. Smartglasses, such as Glass (Google/X, Mountain View, CA), typically have a built-in 9-axis inertial measurement unit (IMU) that includes a 3-axis accelerometer, along with a gyroscope and magnetometer. Accelerometer-based balance assessments have garnered increased attention because of the widespread availability of accelerometers as a component of consumer smartphones [29,30]. The balance accelerometer measure (BAM) was developed as part of the National Institutes of Health’s (NIH) Standing Balance Toolbox to provide a low-cost assessment [31], which can be administered through the use of an iOS app. Likewise, the Sway balance app [32-36] for iOS was designed to provide an easily accessible method for quantitative balance assessment and has obtained FDA (Food and Drug Administration) clearance.
Smartglasses could enable self-administered balance assessments, as well as rehabilitative feedback, by providing real-time audio/visual instruction to the user while monitoring balance via the IMU. Although balance would only be one component of a concussion diagnostic metric, smartglasses could also deliver other relevant assessments, including vestibulo-ocular and cognitive assessments. Smartglasses could also serve as a processing hub for integration with other wearable sensors, including wearable electrophysiological devices. Finally, smartglasses could enable remote/telemedicine concussion diagnosis. A medical professional could receive data from the wearable sensor platform while communicating in real time with the injured or some untrained personnel to determine the need for further care [37].
Goal of This Study
In this report, we sought to determine to what extent smartglasses-based balance measurement corresponded with a consumer smartphone attached at the waist, as in the NIH Toolbox Standing Balance Test. The objective of this study was to demonstrate the feasibility of obtaining quantitative balance measurements with smartglasses. These results could motivate future research in how smartglasses may be used to measure balance dysfunction and other concussion-related impairments. Although there exist multiple static balance protocols, the NIH Toolbox Standing Balance Test stances were used in this proof-of-concept study, given the availability of detailed methods and reference data available [31,38,39] for comparison between devices.
Methods
Subjects
A total of 42 individuals participated in this study (Table 1). Procedures were approved by the Asentral, Inc. Institutional Review Board (Newburyport, MA, USA) and the US Army Human Research Protection Office. Subjects were recruited from the public. An informed consent form describing the nature of the study, as well as the exclusion criteria, was completed by all participants.
Table 1.
Subject demographics (N=42).
| Demographics | Mean (SD, range) or n (%) |
| Age in years, mean (SD, range) | 23.8 (5.2, 18-37) |
| Gender, female, n (%) | 16 (38) |
| Height in inches, mean (SD, range) | 68 (3, 62-76) |
| Weight in pounds, mean (SD, range) | 152 (32, 110-241) |
Participants were required to be between the ages of 18 and 39 years, weigh no more than 250 pounds, and possess normal hearing and normal or corrected-to-normal vision. Each of these criteria was confirmed by participant self-report. Participants were excluded if they reported any preexisting condition that may alter their ability to balance normally. A set of specific conditions that could affect balance were described for participants. Specific conditions listed for participants included multiple sclerosis, Parkinson’s disease, Huntington’s disease, other movement disorders, stroke, cervical spine or physical mobility issues, more than 1 fall in the past 6 months not as a result of an accident, current pregnancy, dizziness or vertigo, any lower extremity injury that required medical attention in the last 3 months, and any surgeries within the last year. All participants attested they were not taking any medication to lower blood pressure or to control a heart problem. All participants also attested they were not under instruction by a supervising physician to avoid full/unrestricted physical activity. Individuals were also screened based on self-report for history of a diagnosed seizure disorder (or any seizures within the last 3 years), as well as extreme sensory sensitivity. All participants also attested to having no diagnosed macular degeneration, glaucoma, or cataracts, or any chronic or acute conditions resulting in pain, including diabetes or a history of joint replacement.
Experimental Setup
Before administering the BAM protocol, subjects were outfitted with a gait belt. An Android smartphone (Samsung Galaxy S5, Samsung Galaxy S6, or LG Electronics/Google Nexus 5) was attached to the gait belt using a protective case with clip. The smartphone was attached upright, with the screen facing away from the subject. The subject was also given a pair of Glass Explorer Edition (henceforth, Glass) by the facilitator to wear. Subjects who normally wore glasses were given the option to wear Glass over or without their regular glasses. Subjects were asked to read a sentence on the display screen to confirm the screen was adjusted properly. A test exercise was administered on Glass to ensure subjects could (1) operate Glass by tapping on the side and (2) could hear a tone played from Glass.
The BAM protocol was administered as previously described [39]. The BAM protocol includes 6 standing conditions: (1) solid surface, feet together, eyes open, and (2) eyes closed; (3) foam surface (Airex Balance Pad, Specialty Foams, Switzerland), feet together, eyes open, and (4) eyes closed; (5) solid surface, tandem standing, eyes open, and (6) eyes closed (Figure 1). During each stance, all subjects were asked to stand quietly for 60 seconds and to look (in eyes-open conditions) at a symbol placed centrally at eye level 1 m from the subject. Subjects were instructed by the facilitator regarding stance following the instructions adapted from the NIH Toolbox Standing Balance Test [31,40]. Stance was also described on the smartglasses display screen. Subjects initiated each set of data collection by tapping the side of the smartglasses. A timer was displayed on Glass showing time remaining and a tone was played at the end of each timed stance. All subjects completed 2 attempts of all stances on the same day.
Figure 1.
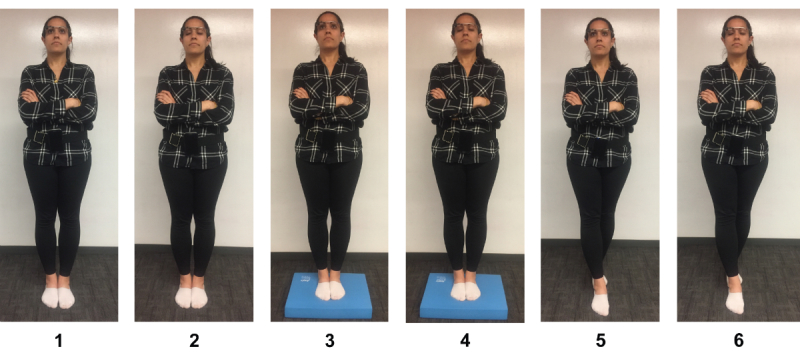
Balance accelerometer measure (BAM) protocol conditions. (1, 2) Feet together on a firm surface used for conditions 1 (eyes open) and 2 (eyes closed). (3, 4) Feet together on a foam surface used for conditions 3 (eyes open) and 4 (eyes closed). (5, 6) Feet in tandem stance on a firm surface used for conditions 5 (eyes open) and 6 (eyes closed).
A trained study facilitator was present during the study and was ready to prevent the participant from falling. The study facilitator observed participants for failure to hold the demonstrated pose. Failures were recorded if (1) participant’s arms came off his/her chest, (2) participant’s knees bent, (3) participant’s feet moved out of original position (move or swivel out or are lifted), (4) participant bent forward at the waist (more than 45°), (5) participant opened his/her eyes during an eye-closed pose, or (6) participant says something like “I cannot do that” or “I do not feel safe trying that.”
Data Acquisition
An Android app was developed to synchronize recording of device IMU data between smartglasses and the waist-mounted smartphone (Figure 2). The app was installed on both Glass and the Android smartphones before testing. The app allowed Glass to pair with a smartphone via Bluetooth. Messages sent via Bluetooth from Google Glass to the smartphone were used to initiate a timer on Google Glass and begin storing IMU values (sampled at 50 Hz).
Figure 2.
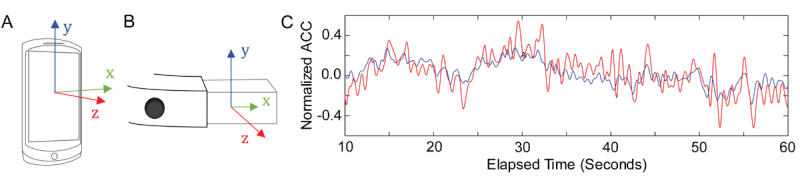
Accelerometer data (ACC) collection with smartphone and smartglasses. (A) Axes of accelerometer on Android smartphone compared with (B) Glass. (C) Example comparison of low-pass filtered ACC (z-axis) collected during a trial of condition 6 in Glass (red) compared with waist-mounted smartphone (blue).
Upon completion of each stance, time-stamped IMU data were saved on the device as a comma-delimited plain text file. When running on Google Glass, the app provides instructions on stance, a timer, and a tone that plays at the end of each stance session. At the end of each study session, data were transferred from respective devices to secure cloud storage.
Data Analysis
Data files were imported into MATLAB 2016b (MathWorks, Native, MA, USA) for analysis, which included use of the Signal Processing Toolbox, the Statistics and Machine Learning Toolbox, and custom scripts. The first 10 seconds of data were discarded to ensure stability of measures (50 seconds of data total). Accelerometer data (ACC) from each trial was low-pass filtered using a fourth-order, Butterworth filter with a cutoff frequency of 1.25 Hz [39]. The normalized path length (NPL; mG/sec; higher values indicate more sway) of the anterior-posterior (AP) postural sway data was calculated as previously described [39]. NPL was also calculated from the combined ACC magnitude.
Trials recorded as failures by the study facilitator were excluded from further analysis. Smartglasses-based measurements of NPL along different axes were compared with smartphone measurements using Spearman rank correlation coefficient [41]. For comparison of differences between stances, the nonparametric Kruskal-Wallis test was used to compare mean ranks [42,43]. Normality of measurements within stance conditions was evaluated by the Anderson-Darling test [44]. Significant differences between correlation coefficients were determined by treating them as Pearson coefficients and using the standard Fisher z-transformation to compare using a standard normal procedure [45]. Test-retest reliability of NPL measurements was estimated for each condition between the 2 sessions by calculating the 2-way random, single-measure intraclass correlation coefficient, ICC2,1, and corresponding 95% CI [46,47]. NPL was standardized as previously described [39], and the composite score was calculated by adding together the standardized values across all 6 conditions.
Results
Measurement of Anterior-Posterior Sway with Smartglasses Correlates With Measurement at Waist
All 42 subjects successfully passed both trials on conditions 1 through 3, similar to previous reports [39]. Both trials of the eyes closed/foam surface condition (condition 4) were passed successfully by 37 subjects (88%). One subject failed a trial of the eyes-open/tandem stance condition (condition 5). Thirty subjects (71%) successfully passed 2 trials of the eyes closed/tandem stance condition (condition 6). All observed failures were recorded as feet moving out of the original position and/or arms coming off the chest. Overall, 2 trials on all 6 conditions were successfully passed by 28 subjects (66%).
NPL AP sway measured from the head was strongly correlated (Spearman rank correlation coefficient=.85) with NPL AP sway measured from the waist (Figure 3). Mean NPL AP sway measured from the waist was in good agreement with previously reported values [39], although we observed a higher mean for condition 6. The mean (SD) composite score was 21.4 (18.0), which was in good agreement with the previously reported value of 19.6 (15.3) for healthy subjects.
Figure 3.
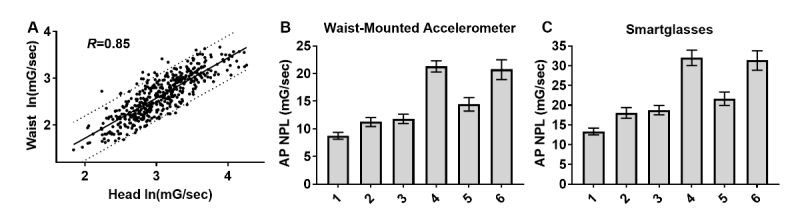
Anterior-posterior (AP) sway measured with smartglasses is highly correlated with waist-based accelerometry. (A) AP sway measured from the head was strongly correlated with AP sway measured from the waist (pooled data from all conditions with 95% prediction bands). Geometric mean and 95% CI for waist-based (B) and head-based (C) measurements of AP normalized path length (NPL) by condition.
Although NPL measured from the head was generally larger than NPL measured from the waist in each trial, mean NPL AP sway measured from the head in each condition was observed to follow a similar trend as the means measured from the waist. Significant differences (Kruskal-Wallis, P<.001) were found between each set of eyes-open and eyes-closed conditions as well as between standing on feet together/firm surface compared with foam surface or tandem stance.
Correlation Between Measurements Was Significantly Stronger When Calculating Normalized Path Length From All Three Axes
Measuring sway along the ACC’s AP axis was previously shown to be sufficient to differentiate healthy subjects from subjects with vestibular disorders [39]. However, the additional ACC acquired from commercial off-the-shelf (COTS) smart devices may further enhance measurement accuracy, particularly along the mediolateral x-axis. Indeed, the NPL calculated using all 3 axes (total NPL) was found to have a significantly stronger correlation (Spearman rank correlation coefficient=.90, P<.001) between head- and waist-based measurements (Figure 4). Mean total NPL measured in each condition followed similar trends as using AP NPL only for both waist- and head-based measurements.
Figure 4.
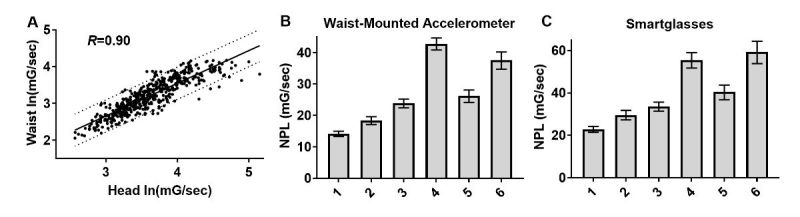
Total sway magnitude measured with smartglasses is highly correlated with waist-based accelerometry. (A) Total sway measured from head was more strongly correlated with sway measured from the waist. Geometric mean and 95% CI for waist-based (B) and head-based (C) measurement of total normalized path length (NPL) by condition.
Test-Retest Reliability of Measures Were Comparable Between Head and Waist
Previously, the test-retest reliability of NPL AP measured from the waist was found to be generally good (ICC≥0.74) across all conditions, except for condition 6 [39]. Here, same-day test-retest reliability of AP NPL measured from the head with smartglasses was found to be very good (Figure 5), with an ICC2,1 (95% CI) of 0.85 (0.81-0.88). This was comparable to our estimation of the test-retest reliability of waist-based AP NPL, which was 0.84 (0.80-0.88), agreeing with previously reported values.
Figure 5.
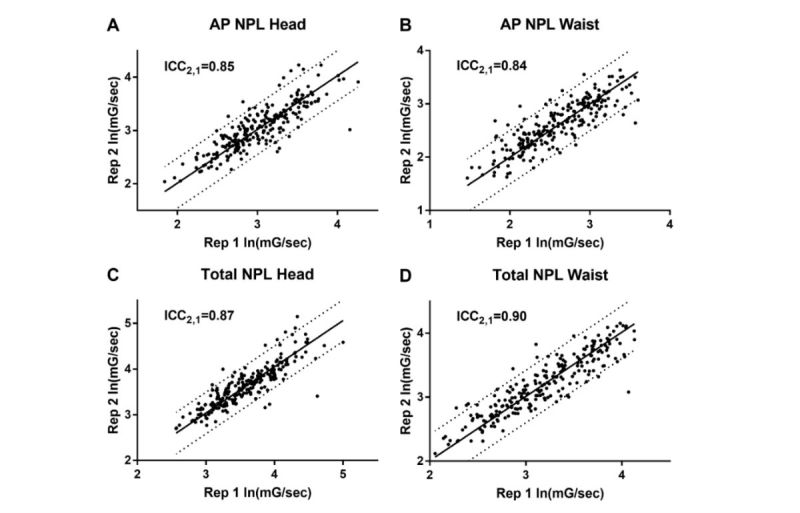
Head-mounted smartglasses have comparable test-retest reliability to waist-mounted balance accelerometer measurement. Test-retest intraclass correlation coefficient, ICC2,1, for accelerometer measures of postural sway along anterior-posterior (AP) (A=head, B=waist) and all axes (C=head, D=waist). NPL: normalized path length.
Using total NPL, we found a slight improvement in test-retest reliability in both head- and waist-based measurements. ICC2,1 (95% CI) was found to be 0.87 (0.83-0.90) in the case of head-based measurement, as opposed to 0.90 (0.88-0.92) in the case of waist-based measurement.
Discussion
Principal Findings
To the best of our knowledge, this is the first study assessing the feasibility of using COTS smartglasses to perform quantitative standing balance measurement. This study indicates that head-based measurement of AP or total sway with smartglasses following the BAM protocol produces similar results to waist-based measurement. This included similar relative differences between test conditions as well as similar test-retest reliability. Condition effects observed with this protocol previously supported the validity of waist AP NPL as a measure of balance. Similar to these previous findings, sway measured with smartglasses was larger with eyes closed than with eyes open for all stance conditions. Sway was also larger in tandem stance and on foam surface conditions compared with corresponding conditions with feet together on a firm surface. These condition effects previously indicated that ACC measured from the waist was sensitive to changes in the sensory modalities available for balance, including vision and somatosensation [48]. In this study, we demonstrate that head-based ACC measurement using COTS smartglasses has a comparable sensitivity for measuring these differences.
Comparison With Prior Work and Future Implications
The current wide availability of smartphones with IMU technology has made them an attractive platform to develop physical health assessments on. Along with standing balance, smartphone-based measurements are also being developed to objectively quantify a range of related functional mobility assessments [49-53]. Similarly, there are a growing number of dedicated wearables that have been developed to provide research- and clinical-grade balance, gait, full-body kinematics, and other functional mobility assessments. An important distinction between using the sensors in a smartphone compared with wearable hardware built for a specific function is that smartphones are already widely used by the population. Thus, smartphone-based assessments can be immediately accessible on this multifunctional platform. The multifunctional versatility of such a device could be particularly transformative in the battlefield, where there are practical limitations to amount of equipment that can be transported in various circumstances [28]. When considering the broader goal of having an objective balance assessment as only one component of a multifactorial concussion battery, neuroimaging and biomolecular assays could provide more definitive results and aid in differential diagnosis. However, the equipment needed to provide this level of certainty would be less practical for point-of-injury assessment and triage when a software-based assessment on a multipurpose device could sufficiently determine the need for additional care.
Leveraging the wide availability of COTS hardware to develop objective clinical assessments and rehabilitative strategies has motivated research into not just smartphones. The Nintendo Wii Balance Board [54-57] and Microsoft Kinect [58-60] are also being used in physical medicine. Indeed, there are now several FDA-cleared Kinect applications suitable for use in the clinic or at home that provide exercise guidance and remotely accessible patient performance metrics [61,62]. The sophistication of sensor-rich COTS hardware enables health care apps to be developed without the costs typically associated with dedicated health care equipment design, manufacturing, quality control, storage, distribution, etc. Admittedly, smartglasses are far from reaching the ubiquity of these devices. However, the market for smartglasses is projected to reach 3.4 million units by 2020, with health care being a major driver of smartglasses’ growth [63]. Smartglasses have been shown to be well tolerated in children and adults with autism spectrum disorder, providing evidence to support their use as an assistive device [64-66]. In the longer term, decline in costs, the solidification of applications and model features, and technology saturation of smartphone and tablet markets could push smartglasses to become a dominant consumer computing device [63]. It is this context, considering the potential future widespread availability of lightweight and portable head-mounted wearables, which motivates the research study described here.
Critically, it was not the objective of this study to determine whether smartglasses would provide a more sensitive measure than smartphones or act as a replacement for gold standard methods of clinical assessment. Rather, with this feasibility demonstrated, it can be discussed how smartglasses could have specific advantages over other COTS devices for assessment and rehabilitation of balance dysfunction related to brain injury. Recently, it was reported that a fully immersive head-mounted virtual reality (VR) system was successfully used to obtain repeatable balance assessment measurements in an elderly population [67]. Higher fall risk participants were found to change their tilt in the AP direction at a significantly higher rate. Although minimal simulator sickness was generally reported in this study, at least one participant dropped out of the study because of this issue. There were also significant differences in nausea pre- and postmeasurement. In terms of head-mounted wearables, smartglasses may be preferable to fully immersive VR headsets as they do not completely obscure external vision, which suggests they could be a safer alternative (Figure 6). Smartglasses could provide real-time feedback to correct balance instability during movement in an actual environment, such as through audio [68-70], and Glass has been shown to be feasible for external rhythmic cueing to improve gait in Parkinson’s patients [71]. Furthermore, fully immersive VR headsets often include foam that is pressed against the user’s face that can quickly become unsanitary, leading to hygiene concerns and the potential for disease transmission when used in a clinical setting [72]. Thus, smartglasses may be preferable in clinical use for not just balance assessment/feedback but also VR-based vestibular-ocular motor and cognitive assessments.
Figure 6.

Fully immersive head-mounted device compared with partially immersive smartglasses. Fully immersive virtual reality headsets, such as Oculus Rift (left), completely block external stimuli, limiting their use in concussed populations where dizziness, nausea, and sensitivity to light are common persistent symptoms. Smartglasses, such as Glass (right), could provide a safer, more portable, and lighter-weight alternative. Of note, Glass weighs only 1.3 ounces—more than 10 times less than Oculus Rift.
Limitations
This study is primarily a proof-of-concept demonstrating that measurements obtained from the IMU of a specific COTS head-mounted wearable (Glass) can provide quantitative balance measurements. These head-based measurements are comparable with waist-based measurements when following the NIH Standing Balance Toolbox protocol. This report only describes one quantitative balance measurement derived from accelerometry, NPL, although there are a variety of methods to preprocess these types of data [73]. A variety of subjective and objective assessments exist to both identify and characterize balance deficits [74]. A comprehensive characterization of measures obtainable from smartglasses against a clinical force plate system would provide a more thorough assessment of the concurrent validity of head-based measurement. Recently published pilot results from an elderly population using a force plate system support the potential for head-based measurement using COTS hardware in clinical assessment of balance [67].
Stances in the BAM protocol and NIH Standing Balance Toolbox were used in this study as a standard for preliminary comparison, given the availability of detailed methods and baseline data [31,38,39]. However, it has been previously suggested that as this protocol was not designed with the goal of concussion assessment, it may have limited use in this domain in comparison with other protocols. In one report, BAM was found not to effectively discriminate between healthy and concussed adolescents. Rather, expert scoring of the Balance Error Scoring System (BESS) protocol was able to identify patients from healthy participants with 60% sensitivity and 82% specificity [48]. The BESS protocol is similar to the BAM protocol with 6 conditions in total. However, in BESS, all conditions are performed with eyes closed and hands positioned on the hip, with 3 stances (feet together, single leg, and tandem stance) performed on both firm and foam surfaces. A modified BESS protocol, which eliminates the foam surface conditions, has been included as part of the SCAT sideline concussion evaluation since the second edition [75]. Although the modified BESS protocol may lack sensitivity, instrumenting the modified BESS with a waist-based inertial sensor led to superior diagnostic classification of recently concussed individuals compared with BESS alone, albeit in a relatively small sample size of 13 recently concussed individuals and 13 demographically matched controls [76]. In summary, future evaluations should consider whether other procedures are necessary, depending on study goals.
The study presented here is limited by its exclusive use of healthy subjects. Further research is necessary to determine whether measurements using a head-mounted device can detect deficits in postural sway related to specific medical conditions. Although the BAM protocol was unable to sufficiently discriminate concussed adolescents, postural sway as measured by waist-based BAM using this protocol was able to discriminate between persons with peripheral vestibular impairments and those without balance impairment [39]. In general, postural sway measurement alone currently lacks the sensitivity and specificity needed to confidently diagnose concussions. It is important to reiterate that our study goal was to demonstrate the feasibility of obtaining objective and quantitative measurements of postural sway with a head-mounted wearable. We hypothesize this would serve as only one component of a concussion assessment battery that could be automatically administered using COTS smartglasses as a platform.
Finally, although we determined that head-based measurement was generally consistent with waist-based measurement, head-based measurement might present additional challenges when administered outside carefully monitored conditions. For example, head-based measurement may be more sensitive to behavioral artifacts such as speech and shifting attention. It is important to mitigate these challenges by detecting and removing these artifacts to improve the internal validity of the assessment when used independently for clinical decision-making.
Conclusions
The accelerometer built into Glass is sufficient to provide standing balance measurements comparable with commercial smartphones. Accelerometry measurements obtained from the head, including the NPL of AP sway as well as the total NPL magnitude, resulted in similar condition effects as those obtained from the waist in a healthy adult population. Head-based measurement of balance using smartglasses could serve as one component of a wearable, multifactorial concussion assessment that has integrated instruction and feedback. This approach could improve the objective assessment of concussion symptoms in high-risk activities, including contact sports and warfare, where current standards often rely on subjective methods, including symptom self-report by the injured. Smartglasses may provide a safer, lighter-weight, more portable, and more hygienic alternative to fully occlusive head-mounted wearables, while providing a similar range of assessments for concussion detection, including cognitive and vestibular-ocular motor screens. Further research is necessary to demonstrate the ability of smartglasses to detect balance dysfunction stemming from concussion.
Acknowledgments
This study is based upon work supported by the United States Army Medical Research and Materiel Command under Contract No. W81XWH-14-C-0007 (awarded to TIAX, LLC). Additional work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Autism Research Program under Award No. W81XWH-17-1-0449. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense. The authors thank Alyk Moomaw for her help in preparing the manuscript. The authors thank Google, Inc for generous support and the Glass team at X (formerly Google X) for technical guidance on Glass development.
Abbreviations
- ACC
accelerometer data
- AP
anterior-posterior
- BAM
balance accelerometer measure
- BESS
Balance Error Scoring System
- COTS
commercial off-the-shelf
- FDA
Food and Drug Administration
- ICC
intraclass correlation coefficient
- IMU
inertial measurement unit
- MACE
Military Acute Concussion Evaluation
- mTBI
mild traumatic brain injury
- NIH
National Institutes of Health
- NPL
normalized path length
- SCAT
Standardized Concussion Assessment Tool
- VR
virtual reality
Footnotes
Conflicts of Interest: NTS is the owner of Brain Power, LLC, and has patent rights associated with some subject matters discussed.
References
- 1.Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375–8. doi: 10.1097/00001199-200609000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Defense and Veterans Brain Injury Center. 2016. [2017-12-28]. DoD Worldwide Numbers for TBI http://dvbic.dcoe.mil/dod-worldwide-numbers-tbi .
- 3.Johnson MA, Hawley JS, Theeler BJ. Management of acute concussion in a deployed military setting. Curr Treat Options Neurol. 2014 Sep;16(9):311. doi: 10.1007/s11940-014-0311-8. [DOI] [PubMed] [Google Scholar]
- 4.Wang Y, Chan RC, Deng Y. Examination of postconcussion-like symptoms in healthy university students: relationships to subjective and objective neuropsychological function performance. Arch Clin Neuropsychol. 2006 May;21(4):339–47. doi: 10.1016/j.acn.2006.03.006. http://linkinghub.elsevier.com/retrieve/pii/S0887-6177(06)00053-9. [DOI] [PubMed] [Google Scholar]
- 5.Landre N, Poppe CJ, Davis N, Schmaus B, Hobbs SE. Cognitive functioning and postconcussive symptoms in trauma patients with and without mild TBI. Arch Clin Neuropsychol. 2006 May;21(4):255–73. doi: 10.1016/j.acn.2005.12.007. http://linkinghub.elsevier.com/retrieve/pii/S0887-6177(06)00036-9. [DOI] [PubMed] [Google Scholar]
- 6.McCrea M, Iverson GL, McAllister TW, Hammeke TA, Powell MR, Barr WB, Kelly JP. An integrated review of recovery after mild traumatic brain injury (MTBI): implications for clinical management. Clin Neuropsychol. 2009 Nov;23(8):1368–90. doi: 10.1080/13854040903074652. [DOI] [PubMed] [Google Scholar]
- 7.Gaylord KM, Cooper DB, Mercado JM, Kennedy JE, Yoder LH, Holcomb JB. Incidence of posttraumatic stress disorder and mild traumatic brain injury in burned service members: preliminary report. J Trauma. 2008 Feb;64(2 Suppl):S200–5; discussion S205-6. doi: 10.1097/TA.0b013e318160ba42. [DOI] [PubMed] [Google Scholar]
- 8.Kraus JF, McArthur DL. Incidence and prevalence of, and costs associated with, traumatic brain injury. In: Rosenthal M, editor. Rehabilitation of the Adult and Child With Traumatic Brain Injury. Philadelphia, PA: F A Davis Co; 1999. pp. 3–18. [Google Scholar]
- 9.Hoge CW, Toboni HE, Messer SC, Bell N, Amoroso P, Orman DT. The occupational burden of mental disorders in the U.S. military: psychiatric hospitalizations, involuntary separations, and disability. Am J Psychiatry. 2005 Mar;162(3):585–91. doi: 10.1176/appi.ajp.162.3.585. [DOI] [PubMed] [Google Scholar]
- 10.Vasterling JJ, Proctor SP, Amoroso P, Kane R, Heeren T, White RF. Neuropsychological outcomes of army personnel following deployment to the Iraq war. J Am Med Assoc. 2006 Aug 2;296(5):519–29. doi: 10.1001/jama.296.5.519. [DOI] [PubMed] [Google Scholar]
- 11.McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004 Jan;14(1):13–7. doi: 10.1097/00042752-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 12.Williamson IJ, Goodman D. Converging evidence for the under-reporting of concussions in youth ice hockey. Br J Sports Med. 2006 Feb;40(2):128–32; discussion 128-32. doi: 10.1136/bjsm.2005.021832. http://europepmc.org/abstract/MED/16431999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014 Jun;10(3 Suppl):S97–104. doi: 10.1016/j.jalz.2014.04.012. https://linkinghub.elsevier.com/retrieve/pii/S1552-5260(14)00140-X. [DOI] [PubMed] [Google Scholar]
- 14.McCrory P, Meeuwisse W, Aubry M, Cantu B, Dvorak J, Echemendia R, Engebretsen L, Johnston K, Kutcher J, Raftery M, Sills A, Benson B, Davis G, Ellenbogen R, Guskiewicz K, Herring SA, Iverson G, Jordan B, Kissick J, McCrea M, McIntosh A, Maddocks D, Makdissi M, Purcell L, Putukian M, Schneider K, Tator C, Turner M. Consensus statement on Concussion in Sport--the 4th International Conference on Concussion in Sport held in Zurich, November 2012. J Sci Med Sport. 2013 May;16(3):178–89. doi: 10.1016/j.jsams.2013.02.009. https://linkinghub.elsevier.com/retrieve/pii/S1440-2440(13)00041-8. [DOI] [PubMed] [Google Scholar]
- 15.Coughlin SS. Post-Traumatic Stress Disorder and Chronic Health Conditions. Washington, DC: American Public Health Association; 2012. Post-traumatic stress disorder and traumatic brain injury. [Google Scholar]
- 16.Carroll L, Rosner D. The Concussion Crisis: Anatomy of a Silent Epidemic. New York, NY: Simon and Schuster; 2012. [Google Scholar]
- 17.Smith AM, Stuart MJ, Roberts WO, Dodick DW, Finnoff JT, Jorgensen JK, Krause DA. Concussion in ice hockey: current gaps and future directions in an objective diagnosis. Clin J Sport Med. 2017 Sep;27(5):503–9. doi: 10.1097/JSM.0000000000000412. [DOI] [PubMed] [Google Scholar]
- 18.Coldren RL, Kelly MP, Parish RV, Dretsch M, Russell ML. Evaluation of the military acute concussion evaluation for use in combat operations more than 12 hours after injury. Mil Med. 2010 Jul;175(7):477–81. doi: 10.7205/milmed-d-09-00258. [DOI] [PubMed] [Google Scholar]
- 19.Phillips T. The impact of litigation, regulation, and legislation on sport concussion management. Sport J. 2015:8. [Google Scholar]
- 20.Abdullah KG, Grady MS, Levine JM. Concussion and football: a review and editorial. Curr Neurol Neurosci Rep. 2015 Apr;15(4):11. doi: 10.1007/s11910-015-0535-3. [DOI] [PubMed] [Google Scholar]
- 21.Guskiewicz K, Teel E, McCrea M. Concussion: key stakeholders and multidisciplinary participation in making sports safe. Neurosurgery. 2014 Oct;75 Suppl 4:S113–8. doi: 10.1227/NEU.0000000000000494. [DOI] [PubMed] [Google Scholar]
- 22.Connelly C, Martin K, Elterman J, Zonies D. Early traumatic brain injury screen in 6594 inpatient combat casualties. Injury. 2017 Jan;48(1):64–9. doi: 10.1016/j.injury.2016.08.025. [DOI] [PubMed] [Google Scholar]
- 23.Carlson KF, Kehle SM, Meis LA, Greer N, Macdonald R, Rutks I, Sayer NA, Dobscha SK, Wilt TJ. Prevalence, assessment, and treatment of mild traumatic brain injury and posttraumatic stress disorder: a systematic review of the evidence. J Head Trauma Rehabil. 2011;26(2):103–15. doi: 10.1097/HTR.0b013e3181e50ef1. [DOI] [PubMed] [Google Scholar]
- 24.Ling GS, Ecklund JM. Traumatic brain injury in modern war. Curr Opin Anaesthesiol. 2011 Apr;24(2):124–30. doi: 10.1097/ACO.0b013e32834458da. [DOI] [PubMed] [Google Scholar]
- 25.McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, Cantu RC, Cassidy D, Echemendia RJ, Castellani RJ, Davis GA, Ellenbogen R, Emery C, Engebretsen L, Feddermann-Demont N, Giza CC, Guskiewicz KM, Herring S, Iverson GL, Johnston KM, Kissick J, Kutcher J, Leddy JJ, Maddocks D, Makdissi M, Manley GT, McCrea M, Meehan WP, Nagahiro S, Patricios J, Putukian M, Schneider KJ, Sills A, Tator CH, Turner M, Vos PE. Consensus statement on concussion in sport-the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017 Jun;51(11):838–47. doi: 10.1136/bjsports-2017-097699. [DOI] [PubMed] [Google Scholar]
- 26.Lovell MR, Iverson GL, Collins MW, Podell K, Johnston KM, Pardini D, Pardini J, Norwig J, Maroon JC. Measurement of symptoms following sports-related concussion: reliability and normative data for the post-concussion scale. Appl Neuropsychol. 2006;13(3):166–74. doi: 10.1207/s15324826an1303_4. [DOI] [PubMed] [Google Scholar]
- 27.Thompson JW, Hagedorn D. Multimodal analysis: new approaches to the concussion conundrum. J Clin Sport Psychol. 2012 Mar;6(1):22–46. doi: 10.1123/jcsp.6.1.22. [DOI] [Google Scholar]
- 28.Schmid KE, Tortella FC. The diagnosis of traumatic brain injury on the battlefield. Front Neurol. 2012 Jun 12;3:90. doi: 10.3389/fneur.2012.00090. doi: 10.3389/fneur.2012.00090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ozdalga E, Ozdalga A, Ahuja N. The smartphone in medicine: a review of current and potential use among physicians and students. J Med Internet Res. 2012 Sep 27;14(5):e128. doi: 10.2196/jmir.1994. http://www.jmir.org/2012/5/e128/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shah N, Aleong R, So I. Novel use of a smartphone to measure standing balance. JMIR Rehabil Assist Technol. 2016 Mar 29;3(1):e4. doi: 10.2196/rehab.4511. http://rehab.jmir.org/2016/1/e4/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rine RM, Schubert MC, Whitney SL, Roberts D, Redfern MS, Musolino MC, Roche JL, Steed DP, Corbin B, Lin CC, Marchetti GF, Beaumont J, Carey JP, Shepard NP, Jacobson GP, Wrisley DM, Hoffman HJ, Furman G, Slotkin J. Vestibular function assessment using the NIH Toolbox. Neurology. 2013 Mar 12;80(11 Suppl 3):S25–31. doi: 10.1212/WNL.0b013e3182872c6a. http://europepmc.org/abstract/MED/23479540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Patterson JA, Amick RZ, Thummar T, Rogers ME. Validation of measures from the smartphone sway balance application: a pilot study. Int J Sports Phys Ther. 2014 Apr;9(2):135–9. http://europepmc.org/abstract/MED/24790774. [PMC free article] [PubMed] [Google Scholar]
- 33.Amick RZ, Chaparro A, Patterson JA, Jorgensen MJ. Test-retest reliability of the SWAY Balance Mobile Application. J Mob Technol Med. 2015 Jul 16;4(2):40–7. doi: 10.7309/jmtm.4.2.6. [DOI] [Google Scholar]
- 34.Amick RZ, Patterson JA, Jorgensen MJ. Sensitivity of tri-axial accelerometers within mobile consumer electronic devices: a pilot study. Int J Appl Sci Technol. 2013;3(2):97–100. doi: 10.13140/2.1.1568.8324. http://ijastnet.com/journals/Vol_3_No_2_February_2013/14.pdf. [DOI] [Google Scholar]
- 35.Burghart M, Craig J, Radel J, Huisinga J. Reliability and validity of a mobile device application for use in sports-related concussion balance assessment. Curr Res Concussion. 2017;4(1):e1–6. doi: 10.1055/s-0036-1597914. [DOI] [Google Scholar]
- 36.Vincenzo JL, Glenn JM, Gray SM, Gray M. Balance measured by the sway balance smart-device application does not discriminate between older persons with and without a fall history. Aging Clin Exp Res. 2016 Aug;28(4):679–86. doi: 10.1007/s40520-015-0471-8. [DOI] [PubMed] [Google Scholar]
- 37.Mitrasinovic S, Camacho E, Trivedi N, Logan J, Campbell C, Zilinyi R, Lieber B, Bruce E, Taylor B, Martineau D, Dumont EL, Appelboom G, Connolly Jr ES. Clinical and surgical applications of smart glasses. Technol Health Care. 2015;23(4):381–401. doi: 10.3233/THC-150910. [DOI] [PubMed] [Google Scholar]
- 38.Slotkin J, Kallen M, Griffith J, Magasi S, Salsman H, Nowinski C, Gershon R. NIH Toolbox Technical Manual. Bethesda, MD: National Institutes of Health; 2012. Sep 27, NIH Toolbox Standing Balance Test. [Google Scholar]
- 39.Marchetti GF, Bellanca J, Whitney SL, Lin JC, Musolino MC, Furman GR, Redfern MS. The development of an accelerometer-based measure of human upright static anterior- posterior postural sway under various sensory conditions: test-retest reliability, scoring and preliminary validity of the Balance Accelerometry Measure (BAM) J Vestib Res. 2013;23(4-5):227–35. doi: 10.3233/VES-130490. [DOI] [PubMed] [Google Scholar]
- 40.Reuben DB, Magasi S, McCreath HE, Bohannon RW, Wang YC, Bubela DJ, Rymer WZ, Beaumont J, Rine RM, Lai JS, Gershon RC. Motor assessment using the NIH Toolbox. Neurology. 2013 Mar 12;80(11 Suppl 3):S65–75. doi: 10.1212/WNL.0b013e3182872e01. http://europepmc.org/abstract/MED/23479547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zar JH. Spearman rank correlation. In: Armitage P, Colton T, editors. Encyclopedia of Biostatistics. Chichester, England: John Wiley & Sons; 1998. [Google Scholar]
- 42.Vargha A, Delaney HD. The Kruskal-Wallis test and stochastic homogeneity. J Educ Behav Stat. 1998 Jan 1;23(2):170–92. doi: 10.3102/10769986023002170. [DOI] [Google Scholar]
- 43.Kruskal WH, Wallis WA. Use of ranks in one-criterion variance analysis. J Am Stat Assoc. 1952;47(260):583–621. doi: 10.1080/01621459.1952.10483441. [DOI] [Google Scholar]
- 44.Anderson TW, Darling DA. A test of goodness of fit. J Am Stat Assoc. 1954;49:765–9. doi: 10.2307/2281537. [DOI] [Google Scholar]
- 45.Myers L, Sirois MJ. Encyclopedia of Statistical Sciences. New York, NY: Wiley; 2006. Spearman correlation coefficients, differences between. [Google Scholar]
- 46.Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979 Mar;86(2):420–8. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- 47.Zoeller T. Mathworks. [2017-12-28]. Intraclass correlation coefficient with confidence intervals https://www.mathworks.com/matlabcentral/fileexchange/26885-intraclass-correlation-coefficient-with-confidence-intervals?requestedDomain=www.mathworks.com .
- 48.Furman GR, Lin CC, Bellanca JL, Marchetti GF, Collins MW, Whitney SL. Comparison of the balance accelerometer measure and balance error scoring system in adolescent concussions in sports. Am J Sports Med. 2013 Jun;41(6):1404–10. doi: 10.1177/0363546513484446. http://europepmc.org/abstract/MED/23585486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Madhushri P, Dzhagaryan AA, Jovanov E, Milenkovic A. A Smartphone Application Suite for Assessing Mobility. Conf Proc IEEE Eng Med Biol Soc; 18 October 2016; Orlando, FL, USA. 2016. [DOI] [PubMed] [Google Scholar]
- 50.Mellone S, Tacconi C, Chiari L. Validity of a smartphone-based instrumented Timed Up and Go. Gait Posture. 2012 May;36(1):163–5. doi: 10.1016/j.gaitpost.2012.02.006. [DOI] [PubMed] [Google Scholar]
- 51.Lupton SD, Gimpel S, Jerzy R, Brunton LL, Hjerrild KA, Cosman D, Goodwin RG. Characterization of the human and murine IL-7 genes. J Immunol. 1990 May 1;144(9):3592–601. [PubMed] [Google Scholar]
- 52.Madhushri P, Dzhagaryan A, Jovanov E, Milenkovic A. An mHealth tool suite for mobility assessment. Information. 2016;7(3):47. doi: 10.3390/info7030047. [DOI] [Google Scholar]
- 53.Rehan YA, Gumaa M. Validity and reliability of smartphone applications for clinical assessment of the neuromusculoskeletal system. Expert Rev Med Devices. 2017 Jun;14(6):481–93. doi: 10.1080/17434440.2017.1325319. [DOI] [PubMed] [Google Scholar]
- 54.Gil-Gómez JA, Lloréns R, Alcañiz M, Colomer C. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: a pilot randomized clinical trial in patients with acquired brain injury. J Neuroeng Rehabil. 2011 May 23;8:30. doi: 10.1186/1743-0003-8-30. https://jneuroengrehab.biomedcentral.com/articles/10.1186/1743-0003-8-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Goble DJ, Cone BL, Fling BW. Using the Wii Fit as a tool for balance assessment and neurorehabilitation: the first half decade of “Wii-search”. J Neuroeng Rehabil. 2014 Feb 8;11:12. doi: 10.1186/1743-0003-11-12. https://jneuroengrehab.biomedcentral.com/articles/10.1186/1743-0003-11-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Prosperini L, Fortuna D, Giannì C, Leonardi L, Marchetti MR, Pozzilli C. Home-based balance training using the Wii balance board: a randomized, crossover pilot study in multiple sclerosis. Neurorehabil Neural Repair. 2013;27(6):516–25. doi: 10.1177/1545968313478484. [DOI] [PubMed] [Google Scholar]
- 57.Wright WG, McDevitt J, Tierney R, Haran FJ, Appiah-Kubi KO, Dumont A. Assessing subacute mild traumatic brain injury with a portable virtual reality balance device. Disabil Rehabil. 2017 Jul;39(15):1564–72. doi: 10.1080/09638288.2016.1226432. [DOI] [PubMed] [Google Scholar]
- 58.Lange B, Chang CY, Suma E, Newman B, Rizzo AS, Bolas M. Development and evaluation of low cost game-based balance rehabilitation tool using the Microsoft Kinect sensor. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:1831–4. doi: 10.1109/IEMBS.2011.6090521. [DOI] [PubMed] [Google Scholar]
- 59.Paavola JM, Oliver KE, Ustinova KI. Use of X-box Kinect gaming console for rehabilitation of an individual with traumatic brain injury: a case report. J Nov Physiother. 2013;3:129. doi: 10.4172/2165-7025.1000129. [DOI] [Google Scholar]
- 60.Venugopalan J, Cheng C, Stokes TH, Wang MD. Kinect-based rehabilitation system for patients with traumatic brain injury. Conf Proc IEEE Eng Med Biol Soc. 2013;2013:4625–8. doi: 10.1109/EMBC.2013.6610578. http://europepmc.org/abstract/MED/24110765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Kvedar JC, Fogel AL, Elenko E, Zohar D. Digital medicine's march on chronic disease. Nat Biotechnol. 2016 Mar;34(3):239–46. doi: 10.1038/nbt.3495. [DOI] [PubMed] [Google Scholar]
- 62.Baumel A, Birnbaum ML, Sucala M. A systematic review and taxonomy of published quality criteria related to the evaluation of user-facing eHealth programs. J Med Syst. 2017 Aug;41(8):128. doi: 10.1007/s10916-017-0776-6. [DOI] [PubMed] [Google Scholar]
- 63.Global Industry Analysts, Inc Strategyr. [2018-01-02]. Smart Augmented Reality (AR) Glasses - A Global Strategic Business Report http://www.strategyr.com/Smart_Augmented_Reality_AR_Glasses_Market_Report.asp .
- 64.Keshav NU, Salisbury JP, Vahabzadeh A, Sahin NT. Social communication coaching smartglasses: well tolerated in a diverse sample of children and adults with autism. JMIR Mhealth Uhealth. 2017 Sep 21;5(9):e140. doi: 10.2196/mhealth.8534. http://mhealth.jmir.org/2017/9/e140/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Liu R, Salisbury JP, Vahabzadeh A, Sahin NT. Feasibility of an autism-focused augmented reality smartglasses system for social communication and behavioral coaching. Front Pediatr. 2017 Jun 26;5:145. doi: 10.3389/fped.2017.00145. doi: 10.3389/fped.2017.00145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kinsella BG, Chow S, Kushki A. Evaluating the usability of a wearable social skills training technology for children with autism spectrum disorder. Front Robot AI. 2017 Jul 12;4:31. doi: 10.3389/frobt.2017.00031. [DOI] [Google Scholar]
- 67.Saldana SJ, Marsh AP, Rejeski WJ, Haberl JK, Wu P, Rosenthal S, Ip EH. Assessing balance through the use of a low-cost head-mounted display in older adults: a pilot study. Clin Interv Aging. 2017 Aug 26;12:1363–70. doi: 10.2147/CIA.S141251. doi: 10.2147/CIA.S141251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Fino PC, Peterka RJ, Hullar TE, Murchison C, Horak FB, Chesnutt JC, King LA. Assessment and rehabilitation of central sensory impairments for balance in mTBI using auditory biofeedback: a randomized clinical trial. BMC Neurol. 2017 Feb 23;17(1):41. doi: 10.1186/s12883-017-0812-7. https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-017-0812-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Dozza M, Horak FB, Chiari L. Auditory biofeedback substitutes for loss of sensory information in maintaining stance. Exp Brain Res. 2007 Mar;178(1):37–48. doi: 10.1007/s00221-006-0709-y. [DOI] [PubMed] [Google Scholar]
- 70.Dozza M, Chiari L, Horak FB. Audio-biofeedback improves balance in patients with bilateral vestibular loss. Arch Phys Med Rehabil. 2005 Jul;86(7):1401–3. doi: 10.1016/j.apmr.2004.12.036. [DOI] [PubMed] [Google Scholar]
- 71.Zhao Y, Nonnekes J, Storcken EJ, Janssen S, van Wegen EE, Bloem BR, Dorresteijn LD, van Vugt JP, Heida T, van Wezel RJ. Feasibility of external rhythmic cueing with the Google Glass for improving gait in people with Parkinson's disease. J Neurol. 2016 Jun;263(6):1156–65. doi: 10.1007/s00415-016-8115-2. http://europepmc.org/abstract/MED/27113598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Martin-Lutz OH, Burmeister C, dos Santos LF, Morkisch N, Dohle C, Krüger J. Application of head-mounted devices with eye-tracking in virtual reality therapy. CDBME. 2017;3(1):53–6. doi: 10.1515/cdbme-2017-0012. https://www.degruyter.com/view/j/cdbme.2017.3.issue-1/cdbme-2017-0012/cdbme-2017-0012.xml. [DOI] [Google Scholar]
- 73.Mancini M, Salarian A, Carlson-Kuhta P, Zampieri C, King L, Chiari L, Horak FB. ISway: a sensitive, valid and reliable measure of postural control. J Neuroeng Rehabil. 2012 Aug 22;9:59. doi: 10.1186/1743-0003-9-59. http://www.jneuroengrehab.com/content/9//59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Mancini M, Horak FB. The relevance of clinical balance assessment tools to differentiate balance deficits. Eur J Phys Rehabil Med. 2010 Jun;46(2):239–48. http://www.minervamedica.it/index2.t?show=R33Y2010N02A0239. [PMC free article] [PubMed] [Google Scholar]
- 75.McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, Cantu R. Consensus Statement on Concussion in Sport: the 3rd International Conference on Concussion in Sport held in Zurich, November 2008. Br J Sports Med. 2009 May;43 Suppl 1:i76–90. doi: 10.1136/bjsm.2009.058248. [DOI] [PubMed] [Google Scholar]
- 76.King LA, Horak FB, Mancini M, Pierce D, Priest KC, Chesnutt J, Sullivan P, Chapman JC. Instrumenting the balance error scoring system for use with patients reporting persistent balance problems after mild traumatic brain injury. Arch Phys Med Rehabil. 2014 Feb;95(2):353–9. doi: 10.1016/j.apmr.2013.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]