

Abstract
Ankyloblepharon-ectodermal defect-cleft lip/cleft palate (AEC) syndrome is one of the variants of ectodermal dysplasia. It is an autosomal dominant disorder comprising of ankyloblepharon, ectodermal dysplasia, and cleft palate or cleft lip. In 1976, it wasfirst described by Hay and Wells, therefore also known as Hay–Wells syndrome. The characteristic feature of this syndrome is “ankyloblepharon filiforme adnatum”, which refers to the partial thickness fusion of the eyelid margins. The “curly hair-ankyloblepharon-nail disease (CHAND) syndrome” is a clinical variant of AEC syndrome. We report a rare case of a 7-year-old girl child who presented with history of abnormal dentition, 20 nail dystrophy, and light-colored, sparse curly hairs since birth. Parents gave history that at the time of birth, her both eyelids were fused partially, which was surgically corrected by an ophthalmologist at 1 month of age. There was no history of hypohidrosis or anhidrosis, heat intolerance, cleft lip or cleft palate. Microscopy of the hair shaft found “bubbly hair” morphology. This case is unique as it is a rare presentation, and awareness should be there for this constellation of findings so that the systemic associations can be investigated. “Bubble hair” morphology on microscopy is a unique feature in this rare autosomal recessive condition.
Key words: Ankyloblepharon-ectodermal defect-cleft lip/cleft palate syndrome, bubbly hair, curly hair-ankyloblepharon-nail disease syndrome, syndactyly, twenty nail dystrophy
INTRODUCTION
Ankyloblepharon-ectodermal defect-cleft lip/cleft palate (AEC) syndrome is one of the variants of ectodermal dysplasia. It is an autosomal dominant disorder comprising of ankyloblepharon, ectodermal dysplasia, and cleft palate or cleft lip. In 1976, it was first described by Hay and Wells, therefore also known as Hay–wells syndrome.[1] It is the result of missense mutation in TP63 which affects p63 SAM of the gene. Other associated epidermal appendages abnormality includes mild hypohidrosis, hypotrichosis, hypodontia or anodontia, complete dystrophic or absent nails. The characteristic feature of this syndrome is “ankyloblepharon filiforme adnatum,” which refers to the partial thickness fusion of the eyelid margins.[2] The “curly hair-ankyloblepharon-nail disease (CHAND) syndrome” is a clinical variant of AEC syndrome,3 which stands for Ankyloblepharon-ectodermal defects-cleft lip/palate. It is also the result of missense mutation in the SAM domain of p63.
We report a 7-year-old Indian girl, the second child of nonconsanguineous parents, who has all the features of a rare clinical variant of AEC syndrome, i.e., CHAND syndrome.
CASE REPORT
A 7-year-old Indian girl is the second child of healthy, nonconsanguineous parents born at full term, presented with history of abnormal dentition, 20 nail dystrophy, and light-colored, sparse curly hairs since birth. She was born at 37 weeks by normal delivery. Her birthweight was 2000 g and length was 46.5 cm. Parents gave history that at the time of birth, her both eyelids were fused partially, which was surgically corrected by an ophthalmologist at 1 month of age. Physical examination found she had hypopigmented, sparse, curled hair, absent eyebrows both sides in lateral two-third part and sparse in medial one-third part, sparse eyelashes, thin lips with short vermillion border of upper lip [Figure 1], dystrophic fingernails and toenails [Figure 2], abnormal dentition, and syndactyly bilateral fourth and fifth toes. She had normal opthalmological, ear-nose-throat examination with normal abdominal ultrasound, echocardiogram, and G-banded karyotype. The microscopy of her hair shaft showed “bubbly hair” morphology [Figure 3].
Figure 1.

Patient face showing hypopigmented, sparse, curled hair, absent eyebrows, and thin lips with short vermillion border of upper lip with abnormal dentition
Figure 2.

Nail dystrophy with syndactyly
Figure 3.
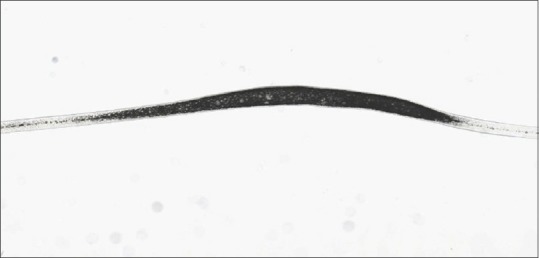
Hair shaft showing “bubbly hair” on microscopy
There was no history of hypohidrosis or anhidrosis, heat intolerance, cleft lip or cleft palate. Patients had normal mental development with no physical development delay. There was no history of any other members affected in the family including patient's parents suggestive of autosomal recessive inheritance.
DISCUSSION
The clinical features with which the patient presented are consistent with the diagnosis of AEC syndrome although she does not have any cleft lip or cleft palate, explaining the concept of variable expressivity in AEC syndrome. Till this date, approximately 23 patients have been found to have this rare clinical variant described in the literature.[3,4,5,6,7,8,9,10,11,12,13,14] The most constant and characteristic presentation in this syndrome is ankyloblepharon. Literature shows that there is overlap between different ectodermal syndromes such as Rapp–Hodgkin[11] and Bowen–Armstrong[14] and AEC syndromes, suggesting that a single entity can have variable expressions. CHAND syndrome is also a variant of AEC syndrome with a variable presentation. Literature also proves that the presence of cleft palate and cleft lip is not always obligatory. The characteristic feature between these two syndromes is the type of hair, which is brittle, wiry, and coarse in AEC syndrome and blonde, thin, and curly in CHAND syndrome. According to one literature by Seres-Santamaria et al.,[7] Hay–Wells syndrome can occur as a result of germinal mosaicism which can lead to recurrence of disease in the family. This study reported two siblings who had ectodermal dysplasia, ankyloblepharon, cleft palate/uvula, and additionally pits lower lip and alveolar synechiae, suggesting a recessive pattern of inheritance with a new clinical feature. Another similar study by Ohishi et al.[15] in 1991 reported woolly hair and atrophic nails and ankyloblepharon with new feature in the form of alveolar synechia and pits in lips in the second child born of consanguineous marriage, which again suggested its autosomal recessive mode of inheritance. The microscopic feature of bubbly hair morphology has not been mentioned in literature and seems to be a unique feature in our patient. Bubble hair is generally seen in acquired conditions in the form of air bubbles in the hair shaft after thermal injury to hair shaft.[16] The presence of air cleft in the hair shaft in a congenital condition was also not found despite adequate literature search.
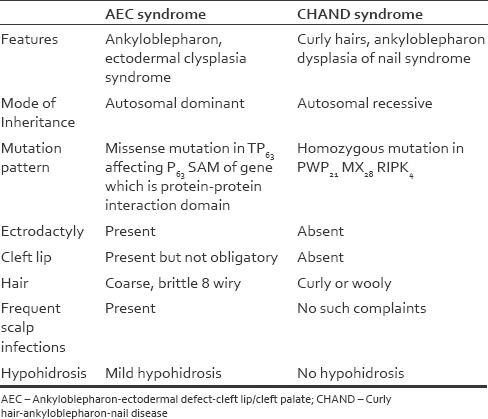
In CHAND syndrome, the exact pattern of inheritance is not clearly defined. Earlier believed to be autosomal dominant, but subsequently, a study conducted by Toriello et al.[17] indicated that it is autosomal recessive. This variation in clinical expression produces difficulty in making diagnosis, especially when encountered with a sporadic case and without distinctive features of AEC syndrome like cleft lip/palate. The specific differentiation features between AEC Syndrome and CHAND syndrome are highlighted in Table 1.
Table 1.
Difference between ankyloblepharon-ectodermal defect-cleft lip/cleft palate syndrome and clinical overlapping in the ectodermal dysplasias syndrome
This patient has presented with the unique cluster of signs and symptoms which fits into a rare CHAND syndrome; however, an additional bubble hair makes this presentation different from the conventional cases.
CONCLUSION
All cases of CHAND syndrome should be thoroughly investigated for associations with other syndromes and anomalies. Genetic evaluation of the affected person is essential for better understanding of the disease. “Bubble hair” morphology on microscopy is a unique feature in this autosomal recessive condition.
Limitations
The exact point mutation could not be ascertained for conclusive evidence of this condition being an autosomal recessive rather than a point mutation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hay RJ, Wells RS. The syndrome of ankyloblepharon, ectodermal defects and cleft lip and palate: An autosomal dominant condition. Br J Dermatol. 1976;94:277–89. doi: 10.1111/j.1365-2133.1976.tb04384.x. [DOI] [PubMed] [Google Scholar]
- 2.Weiss AH, Riscile G, Kousseff BG. Ankyloblepharon filiforme adnatum. Am J Med Genet. 1992;42:369–73. doi: 10.1002/ajmg.1320420324. [DOI] [PubMed] [Google Scholar]
- 3.Bertola DR, Kim CA, Sugayama SM, Albano LM, Utagawa CY, Gonzalez CH, et al. AEC syndrome and CHAND syndrome: Further evidence of clinical overlapping in the ectodermal dysplasias. Pediatr Dermatol. 2000;17:218–21. doi: 10.1046/j.1525-1470.2000.01756.x. [DOI] [PubMed] [Google Scholar]
- 4.Spiegel J, Colton A. AEC syndrome: Ankyloblepharon, ectodermal defects, and cleft lip and palate. Report of two cases. J Am Acad Dermatol. 1985;12:810–5. doi: 10.1016/s0190-9622(85)70100-4. [DOI] [PubMed] [Google Scholar]
- 5.Shwayder TA, Lane AT, Miller ME. Hay-wells syndrome. Pediatr Dermatol. 1986;3:399–402. doi: 10.1111/j.1525-1470.1986.tb00549.x. [DOI] [PubMed] [Google Scholar]
- 6.Martinez Martinez R, Ornelas-Arana ML, Garcia GP. AEC Syndrome: Ankyloblepharon ectodermal defect cleft palate defect (syndrome: Hay-Wells) Bol Med Hosp Infant Mex. 1989;46:349–50. [PubMed] [Google Scholar]
- 7.Seres-Santamaria A, Arimany JL, Muñiz F. Two sibs with cleft palate, ankyloblepharon, alveolar synechiae, and ectodermal defects: A new recessive syndrome? J Med Genet. 1993;30:793–5. doi: 10.1136/jmg.30.9.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Greene SL, Michels VV, Doyle JA. Variable expression in ankyloblepharon-ectodermal defects-cleft lip and palate syndrome. Am J Med Genet. 1987;27:207–12. doi: 10.1002/ajmg.1320270123. [DOI] [PubMed] [Google Scholar]
- 9.Satoh K, Tosa Y, Ohtsuka S, Onizuka T. Ankyloblepharon, ectodermal dysplasia, cleft lip and palate (AEC) syndrome: Surgical corrections with an 18-year follow-up including maxillary osteotomy. Plast Reconstr Surg. 1994;93:590–4. [PubMed] [Google Scholar]
- 10.Vanderhooft SL, Stephan MJ, Sybert VP. Severe skin erosions and scalp infections in AEC syndrome. Pediatr Dermatol. 1993;10:334–40. doi: 10.1111/j.1525-1470.1993.tb00394.x. [DOI] [PubMed] [Google Scholar]
- 11.Cambiaghi S, Tadini G, Barbareschi M, Menni S, Caputo R. Rapp-hodgkin syndrome and AEC syndrome: Are they the same entity? Br J Dermatol. 1994;130:97–101. doi: 10.1111/j.1365-2133.1994.tb06891.x. [DOI] [PubMed] [Google Scholar]
- 12.Mancini AJ, Paller AS. What syndrome is this? Ankyloblepharon, ectodermal dysplasia, cleft lip and palate (Hay–Wells) syndrome. Pediatr Dermatol. 1997;14:403–5. doi: 10.1111/j.1525-1470.1997.tb00994.x. [DOI] [PubMed] [Google Scholar]
- 13.Martinez-Frias ML, Bermejo MM, Garce's AA, Romero MP, Sanchez EB, Azcorra MU. Hay-Wells syndrome, frequency in Spain and review of the literature. An Esp Pediatr. 1996;45:101–4. [PubMed] [Google Scholar]
- 14.Zenteno JC, Venegas C, Kofman-Alfaro S. Evidence that AEC syndrome and bowen – Armstrong syndrome are variable expressions of the same disease. Pediatr Dermatol. 1999;16:103–7. doi: 10.1046/j.1525-1470.1999.99009.x. [DOI] [PubMed] [Google Scholar]
- 15.Ohishi M, Kai S, Ozeki S, Tashiro H. Alveolar synechia, ankyloblepharon, and ectodermal disorders: An autosomal recessive disorder? Am J Med Genet. 1991;38:13–5. doi: 10.1002/ajmg.1320380104. [DOI] [PubMed] [Google Scholar]
- 16.Brown VM, Crounse RG, Abele DC. An unusual new hair shaft abnormality: “bubble hair”. J Am Acad Dermatol. 1986;15:1113–7. doi: 10.1016/s0190-9622(86)70275-2. [DOI] [PubMed] [Google Scholar]
- 17.Toriello HV, Lindstrom JA, Waterman DF, Baughman FA. Re-evaluation of Chands. J Med Genet. 1979;16:316–7. doi: 10.1136/jmg.16.4.316. [DOI] [PMC free article] [PubMed] [Google Scholar]