

Abstract
Coronary sinus defects refer to interatrial communications that lie out of the confines of the atrial septum and leads from left to right shunt through the ostium of the coronary sinus. When associated with persistent left superior vena cava (PLSVC), mild systemic desaturation may occur depending on the extent of unroofing of the coronary sinus. Isolated defects without PLSVC are rare. Three-dimensional echocardiographic and surgical images are presented.
Keywords: Atrial septal communication, coronary sinus defect, three-dimensional echo, unroofed coronary sinus
INTRODUCTION
Unroofed coronary sinus allows shunt from the left to right atrium through the ostium of the coronary sinus.[1] This interatrial communication that lies out of the confines of the atrial septum is called coronary sinus defect or Raghib defect.[2] This lesion may be associated with heterotaxy syndromes and persistent left superior vena cava (PLSVC), which allows some systemic desaturation.[3] The degree of desaturation depends on the presence of PLSVC and extent of unroofing of the coronary sinus.[3] Isolated-coronary sinus defects are rare in the absence of these associations.[4,5,6] A three-dimensional echocardiographic image of an isolated coronary sinus defect is presented with surgical correlation.
CASE REPORT
A 5-year-old female child presented with mild-effort intolerance, normal pulse oximeter saturation of 99%, mild cardiomegaly, a wide, fixed split second heart sound and an ejection systolic outflow murmur. A chest radiograph showed cardiomegaly, dilated pulmonary arteries, and plethora. Electrocardiogram showed sinus rhythm with normal cardiac axis and rSR’ pattern in V1. Echocardiography revealed an enlarged ostium of the coronary sinus, which was shunting left to right. There was an unroofing of the terminal portion of the coronary sinus, where the left atrial blood entered the dilated coronary sinus [Figure 1]. Contrast echocardiography from the left arm excluded a PLSVC. The right atrium and the right ventricle were dilated without evidence of pulmonary arterial hypertension. Three-dimensional echocardiogram confirmed a posteroinferior atrial wall defect in the region of the ostium of the coronary sinus [Figure 2], establishing the diagnosis of isolated coronary sinus atrial septal defect, which was surgically confirmed [Figure 3]. The defect was surgically corrected by autologous pericardial patch closure of the enlarged ostium of the coronary sinus through a median sternotomy.
Figure 1.
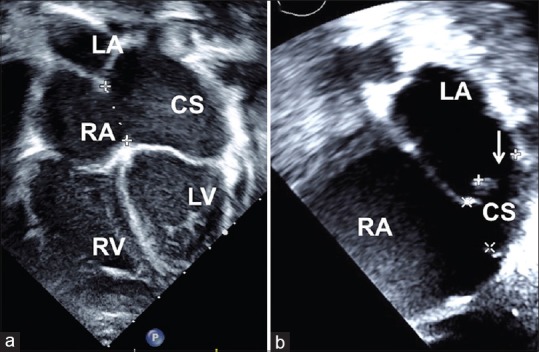
Four chamber(a) view shows dilated right atrium and right ventricle, dilated coronary sinus. The terminal unroofing of the coronary sinus is demonstrated by arrow in the subxiphoid image, (b) RA-right atrium, LA-left atrium, CS-coronary sinus, RV-right ventricle, LV-left ventricle
Figure 2.
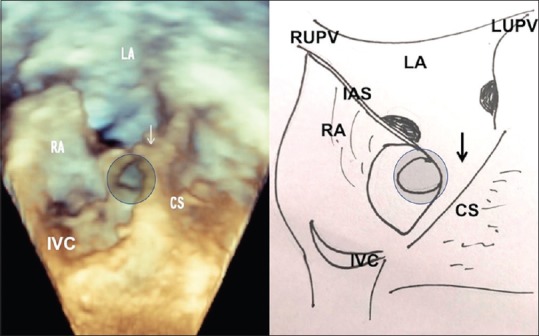
Volume rendered three-dimensional echo after cropping the anterior half of both atria shows the enlarged coronary sinus ostium, through which the terminal unroofing is seen (circle). The pulmonary veins drain in the posterior wall of LA. The atrial septum is intact. RA: Right atrium, LA: Left atrium, CS: Coronary sinus, IVC: Inferior vena cava, LUPV: Left upper pulmonary vein, RUPV: Right upper pulmonary vein, IAS: Interatrial septum
Figure 3.
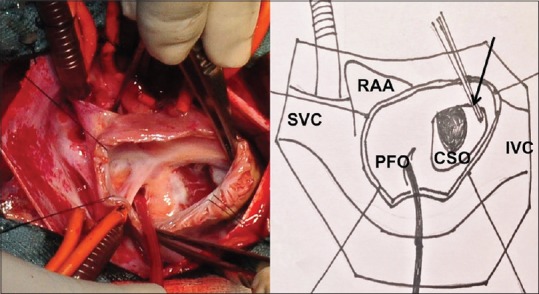
Surgical view after opening the right atrium below the right atrial appendage and cannulation of the SVC and IVC, demonstrates terminal unroofing of the coronary sinus shown by arrow after inferiorly stretching its CSO with a forceps. A sucker is passed through the PFO into the left atrium. CSO: Coronary sinus ostium, PFO: Patent foramen ovale, IVC: Inferior vena cava, SVC: Superior vena cava, RAA: Right atrial appendage
DISCUSSION
Coronary sinus defects located posteroinferior to the oval fossa are extremely rare interatrial communications and are often associated with PLSVC.[1,2,3,4] This is caused by a defect in the embryonic left-arteriovenous fold which forms a common wall between coronary sinus and the left atrium. They may be unrecognizable, when they occur in any form of atrioventricular septal defects. Complete unroofing of coronary sinus is described as Type I or II in the presence or absence of PLSVC, respectively.[3] Partial unroofing is described as Type III or IV when the mid or terminal portion of the coronary sinus is involved.[3] Our patient is, an example of Type IV defect, delineated by three-dimensional echocardiography. On a parasternal long-axis view, a round structure in the posterior-left atrioventricular groove can be a dilated coronary sinus or descending aorta. It is differentiated clearly on apical or subxiphoid views and a dilated coronary sinus is an indicator to suspect the possibility of this rare defect. In the presence of PLSVC, surgical reroofing of the defect or intraatrial baffle after identifying the precise margins of the unroofed portion is needed. The margins can be identified by injection of fluorescein through the left-atrial cannula passed through the patent oval foramen and identification through the ostium of the coronary sinus.[7] In the absence of PLSVC, correction is simple and involves patch closure of the ostium of the coronary sinus. Increased awareness, recent three-dimensional imaging, and contrast echocardiography-aid diagnosis of this rare anomaly.[4,5,6]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Foster ED, Baeza OR, Farina MF, Shaher RM. Atrial septal defect associated with drainage of left superior vana cava to left atrium and absence of the coronary sinus. J Thorac Cardiovasc Surg. 1978;76:718–20. [PubMed] [Google Scholar]
- 2.Raghib G, Ruttenberg HD, Anderson RC, Amplatz K, Adams P, Jr, Edwards JE, et al. Termination of left superior vena cava in left atrium, atrial septal defect, and absence of coronary sinus; a developmental complex. Circulation. 1965;31:906–18. doi: 10.1161/01.cir.31.6.906. [DOI] [PubMed] [Google Scholar]
- 3.Kirklin JW, Barratt Boyes BG. Unroofed coronary sinus syndrome. In: Kirklin JW, Barrat-Boyes BG, editors. Cardiac Surgery. 1st. New York: John Wiley & Sons; 1986. pp. 533–40. [Google Scholar]
- 4.Del Bene MR, Barletta G. Echocardiographic diagnosis of coronary sinus type atrial septal defect. A case report. Minerva Cardioangiol. 1997;45:315–8. [PubMed] [Google Scholar]
- 5.Takahashi H, Sakamoto T, Amano K, Hada Y, Serizawa T, Tomaru T, et al. Coronary sinus type atrial septal defect diagnosed by two-dimensional color Doppler echocardiography: A case report. J Cardiogr. 1985;15:1283–91. [PubMed] [Google Scholar]
- 6.De la Espriella-Juan R, Payá-Serrano R, Cubillos-Arango A, Bochard-Villanueva B, Sánchez-Álvarez S, Morell-Cabedo S, et al. Coronary sinus atrial septal defect in a 65-year-old woman: Diagnosis by two- and three-dimensional echocardiography. Rev Port Cardiol. 2017;36:67–8. doi: 10.1016/j.repc.2016.02.009. [DOI] [PubMed] [Google Scholar]
- 7.Mathew T, Kundan S, Abdulsamad MI, Menon S, Dharan BS, Jayakumar K, et al. Multiple muscular ventricular septal defects: Use of fluorescein dye to identify residual defects. Ann Thorac Surg. 2014;97:e27–8. doi: 10.1016/j.athoracsur.2013.10.059. [DOI] [PubMed] [Google Scholar]