

Abstract
Young men who have sex with men (YMSM) are disproportionately impacted by HIV/AIDS and have elevated rates of substance use. Parenting practices, such as knowledge of child whereabouts and monitoring of behavioral rules, protect against these outcomes among heterosexual youth. This article examined the relationship between these parenting practices and substance use and HIV risk behaviors among YMSM. Data are reported from three similar studies of YMSM: ChiGuys (ages 14-18), Crew 450 (ages 16-22), and RADAR (ages 16-29). The ChiGuys and RADAR studies report cross-sectional analyses, whereas Crew 450 reports latent growth curve analyses. In ChiGuys and Crew 450, participants reported significantly higher scores for parental knowledge of general activities than parental knowledge of gay-specific activities. Parental knowledge of general activities was significantly associated with less binge drinking in both samples and with condomless sex in the ChiGuys sample. Parental monitoring was significantly associated with less marijuana use and condomless sex in younger RADAR participants (16-18 years) and with less drug use in older participants (>18 years). Findings support the need for further research on the influences of parents on YMSM health risk behaviors and the value of exploring family- and parent-interventions to address YMSM health.
Keywords: gay, bisexual, adolescent, alcohol, marijuana
Young men who have sex with men (YMSM) are at disproportionate risk for HIV/AIDS and substance use1,2. Among 13-24 year olds in the U.S., YMSM accounted for over 80% of diagnoses of HIV infection in 20143 and showed a 10% increase in the rate of diagnoses from 2010-20144. Annual incidence of 4.11% has been reported among YMSM ages 16-22 years5 and a simulation model of the epidemic predicted ongoing increases in HIV incidence over the next decade6. YMSM are more likely to use alcohol and drugs and are more likely to initiate use at earlier ages than their heterosexual peers2,7,8. In a review of HIV among YMSM, drug use overall and drug use prior to sex were two of the strongest predictors of condomless sex9. Drug use, particularly “club drugs” (i.e., ecstasy, methamphetamine, etc.), has shown large effects on increased condomless sex10-13. Marijuana has increasingly gained attention for its positive association with condomless sex in both adolescent14,15 and adult samples of MSM16-18. Associations with alcohol consumption have been conflicting, although binge drinking has produced consistent positive associations with condomless sex9,19.
Prior research has studied factors that increase risk for HIV and substance use among YMSM, but has paid limited attention to factors that are protective or that promote resiliency20-23. Theories that address the contexts and systems of influences in the lives of young people, such as Ecological Systems Theory24, highlight the importance of the family-system in adolescent health and wellbeing. While there has been substantial research on the influence of parent-child relationships and interactions on heterosexual adolescent sexual health and substance use, this has received very little research attention among YMSM9,20,25.
Two recent meta-analyses have been published on the influence of parenting practices on adolescent sexual health. One meta-analysis of 52 studies of over 25,000 adolescents found a small overall association (r = .10) between parent-adolescent sexual communication and adolescent safer sex behavior26. Moderation analyses revealed larger effects for girls (r = .12) than boys (r = .04), which raises questions about the effectiveness of parent-child communication about sex for promoting boys’ sexual health. The second meta-analysis included 30 studies of over 40,000 adolescents and found that higher parental knowledge about the adolescent’s activities and whereabouts was associated with increased condom use, but parental monitoring, or tracking and enforcing rules for adolescent behaviors (e.g., homework, using drugs or alcohol), was not27. There was significant heterogeneity in effect sizes across studies, suggesting further research is needed that can help build a literature where effect moderators can be identified. Neither of these meta-analyses reported results specifically for YMSM, and child sexual orientation was not reported as a coding variable.
A number of studies have examined if interventions to change parenting practices can reduce adolescent sexual risk taking. A systematic review of this literature identified five randomized control trials (RCTs) of parent-based interventions and nine family-based RCTs28. Parent-based interventions showed preliminary evidence of effectiveness, whereas few of the family-based interventions were effective. Notably, the CDC’s compendium of evidence-based HIV risk reduction interventions includes two family-based interventions designed to reduce risk with Hispanic29,30 and Black adolescents31. Both of these programs also reported effects on reducing adolescent substance use32,33.
Considerable research over the preceding three decades has shown an association between parenting practices and children’s initiation and use of substances34,35. Furthermore, numerous RCTs have been conducted on parent and family interventions and a review found all of these programs focused on setting strict rules against underage substance use, improving parent–child communication, and monitoring children’s’ activities36. A meta-analysis of these programs that included 116 manuscripts reported a small-to-moderate overall effect37.
Bouris and colleagues21 reviewed the literature on parental influences on sexual risk and substance use among lesbian, gay, and bisexual youth. None of the reviewed studies focused on parental monitoring, despite it being a primary focus in research with heterosexual youth. Instead, the parental influences studied including parent-child emotional connectedness, parental disapproval of sexual risk behaviors, and parents’ knowledge and reaction to their child’s sexual orientation. Few significant associations with sexual risk taking were found. In the first study to examine the effects of parental monitoring and knowledge on sexual risk taking among YMSM, Thoma and Huebner38 found that among YMSM that were out to their parents, parental monitoring had no effect on condomless anal sex (CAS). However, for those YMSM who were not out to parents, monitoring increased engagement in CAS. The authors suggested that parental monitoring may increase risk because, in the context of YMSM trying to maintain secrecy, it might be more difficult to plan for sex and thereby obtain and use condoms consistently38. Qualitative research with sexual and gender minority adolescents has found that many parents enforce a code of silence about sex, which may hamper their ability to monitor their children’s risk behaviors39. In terms of substance use, Bouris and colleagues21 identified five articles in their review. These studies suggest parent rejection is a risk factor for substance use and parental support may show a protective effect.
Across these studies several patterns can be distilled. First, there has been very little research on parental influences on YMSM health, and most existing studies have focused on emotional aspects of the relationship such as rejection/acceptance or support, rather than parenting practices like monitoring. Very few of these studies have included YMSM under age 18, which is an important drawback given the developmental salience of parents among adolescents versus emerging adults40. Second, the pattern of results suggests that parenting practices that have shown relatively consistent relationships in the general adolescent literature (i.e., knowledge) may operate differently among YMSM38,41. Third, the failure to replicate effects found in general samples of youth and inconsistencies in findings across the few studies of YMSM suggest that approaches that can enhance scientific rigor and reproducibility, such as multiple replication studies in similar samples, should be utilized when possible. Fourth, there has been a near absence of longitudinal research in this area.
The purpose of this article is to examine the relationship between two central aspects of parenting practice, knowledge of child whereabouts and monitoring of behavioral rules, and YMSM substance use and HIV risk behaviors. In the interest of examining the robustness of results, this article reports data from three complementary studies of YMSM. Two of the studies (ChiGuys and Crew 450) use measures of perceived parental knowledge of participant whereabouts, whereas the other study (RADAR) uses a measure of parental monitoring focused on enforcement of rules. Our measure of parental knowledge expands on prior research by examining both knowledge of general activities (e.g., checking in with parents before going out) and knowledge of gay-specific activities (e.g., telling parents about going to a gay event). This distinction is important because prior studies have suggested parenting practices for YMSM may operate differently than for heterosexual adolescents precisely because parents are less aware and understanding of gay venues and social contexts. All three studies include YMSM under the age of 18, but the differing ages of the samples allowed for examination of robustness of effects across the developmental spectrum from adolescence into emerging adulthood. Two of these studies report cross-sectional analyses and one reports longitudinal analyses that allowed for examination of prospective effects of parental knowledge over developmental time.
Methods
Participants and Procedures
Data for the current study were taken from three samples of YMSM in Chicago. First, Crew 450 was a longitudinal study designed to analyze the prevalence, course, and predictors of a syndemic of psychosocial health issues linked to HIV among YMSM (N=450)5,42. Participants were aged 16-20 at baseline and were recruited via targeted in-person outreach, geosocial network applications, and peer-incentivized snowball sampling. Measures of parental knowledge were only administered if participants reported living with their parent or guardian, and as such the 52% of participants who met this criterion were included in analyses (analytic N = 233). Data were collected using a computer assisted self-interview (CASI).
Second, the ChiGuys study sample was a 2015 pilot of the CDC’s National HIV Behavioral Surveillance study43 to examine the feasibility of collecting data from MSM aged 14-18 years44. Participants (N=231) were recruited through online advertisements (37%) and respondent driven sampling (63%). After screening eligible, participants completed an interviewer administered survey and HIV test. Only participants in the ChiGuys sample that answered the parental knowledge items were included in the present study (N=225).
The third study included was RADAR, an ongoing longitudinal cohort study of YMSM that aims to understand multilevel influences on HIV risk and substance use. This cohort is being formed (current N=981) by merging three existing studies of YMSM, two of which were the Crew 450 and ChiGuys samples described above. The third cohort consisted of YMSM from Project Q245, who were aged 16-20 at baseline and were recruited using respondent driven sampling. In addition to inviting participants in Project Q2, Crew 450, and ChiGuys to join the RADAR cohort, the cohort sample is being expanded by venue- and peer-based recruitment of 16-20 year old YMSM and referral of serious romantic partners by existing cohort members. Data were collected using a computer assisted self-interview (CASI). In this manuscript we report analyses of the baseline RADAR study data where participants range in age from 16-29. There were two participants who did not answer the parental monitoring items and were not included in analyses.
All three studies shared the following eligibility criteria: 1) male sex assigned at birth; 2) previous sexual encounter with a male, identification as gay or bisexual, or same-sex attracted; and 3) English speaking. All studies were approved by the Institutional Review Board with waivers of parental permission46. In these analyses, we report cross-sectional analyses from the ChiGuys and RADAR studies. In Crew 450, we utilize five waves of longitudinal data, including baseline and four follow-up waves, each separated by six months (1-year retention 83.7%; 2-year retention 75.5%).
Measures
Outness and Parental Rejection
Participants in all three studies were asked if they were out about their sexual orientation to their mother, their father, or both. In the ChiGuys and RADAR samples, participants who reported being out to a parent were then asked about each parent’s response on a one to four scale ranging from “Very Positive” to “Very Negative.” Parental rejection was scored as the mean of each parents’ reaction, or a single parent’s reaction when only one reaction was described.
Parental Knowledge
Parental knowledge was measured in both the ChiGuys and Crew 450 sample using the five-item parental knowledge subscale of the Parenting Style Questionnaire (PSQ)47,48. The parental knowledge subscale asked about parental knowledge of adolescent behavior such as “How often do your parents/caregivers check in with you to see what you are up to?” Questions on the PSQ were measured on a five-point scale with response options “Never or almost never,” “Occasionally,” “About half the time,” “Often,” and “Always or almost always” coded as zero to four. Alphas were acceptable in both ChiGuys (α = .81) and Crew 450 (α = .83). In order to measure parental knowledge as it related to knowledge of adolescent’s attendance of gay events and with gay friends, we modified questions on the PSQ to create a separate three-item scale that measured gay-specific parental knowledge. The gay-specific scale also had adequate reliability in both samples (ChiGuys: α = .78; Crew 450: α = .90). Mean composites were created for both parental knowledge and gay-specific parental knowledge.
Parental Monitoring
In the RADAR sample, parental monitoring was measured with the eight-item Poor Family Management (PFM) subscale from the Family Risk and Protective Factors section of the Communities that Care study49-51. The PFM includes questions about parent’s monitoring behaviors such as “If I skip school, I will be caught by my parents/caregivers.” Response options were on a four-point scale from “Strongly disagree” to “Strongly agree” coded as one to four. For participants over the age of 18, the questions on the PFM were reworded in the past tense (i.e., “The rules in my family are clear” became “The rules in my family were clear”). The PFM scale had adequate reliability for the sample as a whole (α = .83) as well as for participants 18 years and under (α = .83) and 19 and over (α = .83). A mean composite was created from the eight items.
Binge Drinking
In the ChiGuys sample, participants were asked to report the number of times in the previous 30 days they had binge drank, defined as five or more drinks on a single occasion. Participants who reported that they had never had a drink were coded as zero. In the Crew 450 sample, participants were asked “During the past six months, how often did you have five or more drinks containing alcohol within a two-hour period?” Response options ranged from zero to nine and included “zero days,” “one or two days in the past six months,” “three to five days in the past six months,” “One day a month,” “two to three days a month,” “One day a week,” “Two days a week,” “three to four days a week,” “five to six days a week,” and “Everyday.” Participants in the RADAR sample were asked “How often do you have six or more drinks on one occasion?” in the previous six months. Response options were coded as zero to four and included “Never,” “Less than monthly,” “Monthly,” “Weekly,” and “Daily or almost daily.”
Marijuana Use
Participants in the ChiGuys sample were asked to report how often they had used marijuana in the past 12 months on an eight-point scale (coded as zero to seven) with response options “Never,” “Less than once a month,” “Once a month,” “More than once a month,” “Once a week,” “More than once a week,” “Once a day,” and “More than once a day.” Participants who reported having never used marijuana were coded as zero. In the Crew 450 sample, participants were asked “During the past six months, how many times did you use marijuana?” Response options were coded zero to six and included “zero times,” “one to two times in past six months,” “Once a month or less (three to six times in past six months),” “two or three times a month,” “one or two times a week,” “three to five times a week,” and “Everyday or almost everyday.” In the RADAR sample, participants were asked “On how many occasions have you used marijuana (also called weed or pot) in the past 30 days?” with response options “0,” “1-2,” “3-5,” “6-9,” “10-19,” “20-39,” and “40 or more” (coded zero to seven).
Drug Use
To assess drug use in the ChiGuys sample, a dichotomous variable was created such that participants who reported using cocaine, crack, methamphetamine, non-prescription downers or pain killers, ecstasy, heroin, or poppers in the previous 12 months were coded as one, and participants who reported no drug use in that period were coded as zero. The dichotomous variable was formed in this sample because of the low level of endorsement of individual drugs. Drug use in the Crew 450 sample was measured by assigning participants the value of the drug (cocaine, heroin, methamphetamines, opiates, non-prescription depressives, non-prescription stimulants, psychedelics, ecstasy, GHB, ketamine, inhalants, and poppers) that they endorsed using the most frequently in the previous six months. Response options were coded zero to six and included “zero times,” “one to two times in past six months,” “Once a month or less,” “two or three times a month,” “one or two times a week,” “three to five times a week,” and “Everyday or almost everyday.” In the RADAR sample, a quantity variable was created based on the number of unique drugs (cocaine, heroin, methamphetamines, GHB, ketamine, poppers, inhalants, hallucinogens, and ecstasy) participants endorsed using in the previous six months (range: zero to nine).
Condomless Anal Sex
In all three samples, participants were administered the HIV Risk Assessment of Sexual Partnerships (H-RASP)52. The H-RASP is an assessment of sexual behavior and associated situational and contextual factors that was designed for YMSM to report partner-specific data. Participants were asked to report on the number of unprotected anal sex acts with their last three partners. A sum score was created across partners for each participant. Participants were also asked to report their total number of unprotected anal sex partners. In the ChiGuys sample, these questions were specific to the previous 12 months. In the Crew 450 and RADAR samples, the questions were specific to the previous six months.
Statistical Analyses
Concurrent associations between parental knowledge and substance use and sexual risk taking outcomes were analyzed in the ChiGuys sample using negative binomial and logistic regression analyses in SPSS 23. Negative binomial models were used in order to account for the non-normal distribution of count data. Zero-inflated negative binomial models were fit for CAS acts and the zero-inflation component was not significant and including it did not change the pattern of count effects. For the sake of parsimony and broadest understanding of analyses and results, the negative binomial regression model are reported. The effects of parental knowledge on change over time in substance use and sexual risk taking outcomes in the Crew 450 sample was tested by regressing baseline parental knowledge onto latent growth curves created for each risk behavior from the five waves of data. This analysis was accomplished in MPlus v. 7.31 using time scores to create individually varying assessment schedules for each participant and account for differences in age at the start of Crew 450. Time scores were based on participant age at each wave and were centered at age 16 (youngest age at enrollment). In MPlus, maximum likelihood allowed for use of all available data in consideration of some degree of missingness. The last set of analyses were conducted with the RADAR sample and were used to test for associations between parental monitoring and substance use and sexual risk outcomes. Negative binomial and linear regression in SPSS were used. The analyses were run for the full sample and then run separately for participants 18 years and under (N = 171) and participants 19 and over (N = 510) in order to test whether the effects of parental monitoring were more apparent for participants who were minors.
In all analyses, age, race/ethnicity, and bisexual sexual orientation status were included as covariates. Race/ethnicity was dummy coded as separate variables representing identification as Black/African American, Hispanic/Latino, and a combined variable representing all other racial groups, with White as the reference group. Bisexual status was coded as one if participants identified as bisexual and zero if participants identified as any other sexual orientation.
Results
Demographics and Descriptive Statistics
Demographics for the ChiGuys, Crew 450, and RADAR samples are reported in Table 1. Mean ages of the samples reflect the age inclusion criteria for each study, with ChiGuys the youngest (M = 17.12 years), then Crew 450 (M = 18.52), then RADAR (M = 21.47). Each of the samples were comprised of a majority of race/ethnic minority and gay-identified participants. As explained in the measures section, only Crew 450 participants who lived with a parent/guardian were asked about parental knowledge and therefore 100% of Crew 450 participants in the analytic sample lived with a parent/guardian. Reflecting the young age of the ChiGuys sample (14-18 years), the majority (92.4%) lived with a parent/guardian, whereas the proportion was much lower (34.8%) in the older (16-29 years) RADAR sample.
Table 1.
Analytic Sample Demographics
| ChiGuys | Crew 450 | RADAR | |
|---|---|---|---|
|
| |||
| N (%) | N (%) | N (%) | |
| Race | |||
| White | 100 (44.4) | 24 (10.3) | 386 (39.3) |
| Black | 92 (40.9) | 128 (54.9) | 442 (45.1) |
| Other | 25 (11.1) | 17 (7.3) | 153 (15.6) |
| Ethnicity | |||
| Hispanic | 82 (36.4) | 64 (27.5)* | 292 (29.8) |
| Sexual Orientation | |||
| Gay | 144 (64.0) | 176 (75.5) | 676 (68.9) |
| Bisexual | 74 (32.9) | 45 (19.3) | 210 (21.4) |
| Other | 7 (3.1) | 12 (5.2) | 95 (9.7) |
| Live w/ Parent | 208 (92.4) | 233 (100.0) | 341 (34.8) |
| Age, M (SD) | 17.12 (.95) | 18.54 (1.37) | 21.52 (3.74) |
Note: Seven participants in the ChiGuys sample did not identify their race/ethnicity so are excluded.
Hispanic/Latino identity was included in the same question as race and therefore is mutually exclusive with the categories of race.
In a paired-samples t-test, parental knowledge of general activities was significantly higher compared to the parental knowledge of gay-specific activities in both the ChiGuys (Mean Difference = .76, t = 8.21, p < .001) and Crew 450 (Mean Difference = .56, t = 6.37, p < .001) samples, indicating YMSM were significantly more likely to talk to parents about general whereabouts and activities than those that were related to gay venues and friends. Scale mean scores indicate that on average participants reported telling parents about general activities slightly more than half the time, and gay-specific events between “occasionally” and “about half the time.” In the ChiGuys sample, age was significantly negatively associated with parental knowledge (Std. Beta = −.20, p < .01) and bisexual participants reported significantly higher parental knowledge compared to participants who identified as gay or “other” (Std. Beta = .17, p < .05). There were no significant race/ethnicity differences. Similar to the ChiGuys sample, in the Crew 450 sample age at baseline was significantly negatively associated with parental knowledge (Std. Beta = −.24, p <.001). There were no differences based on race/ethnicity or sexual orientation in the Crew 450 sample. In an independent samples t-test, there was no significant difference between RADAR participants 18 years and under and participants 19 and over on the parental monitoring scale (Mean Difference = −.09, p = .15). There were also no significant differences based on race/ethnicity or sexual orientation.
Descriptive statistics for outcome variables are shown in Table 2 for ChiGuys and Table 4 for RADAR. Descriptive statistics for the Crew 450 sample are shown in Table 3 in the form of intercepts for baseline values of each outcome in the latent growth curve model.
Table 2.
Multivariate Negative Binomial and Logistic Regression Models for the ChiGuys Sample
| Binge Drinking (30 days)1 | Marijuana Use (12 Months)1 | Other Drugs (12 Months)2 | CAS Acts (3 Months)1 | # CAS Partners (12 Months)1 | |
|---|---|---|---|---|---|
| M (SD) | |||||
|
| |||||
| 1.20 (3.45) | 1.67 (2.18) | .19 (.39) | 3.93 (14.42) | .81 (2.34) | |
|
| |||||
| Effect Estimates (95% CI) | |||||
|
| |||||
| Age | 1.98 (1.29:3.05)** | 1.12 (0.93:1.35) | 1.32 (0.87:1.99) | 1.99 (1.21:3.27)** | 1.50 (0.99:2.29) |
| Black | 0.23 (0.11:0.48)*** | 1.24 (0.89:1.75) | 0.51 (0.23:1.11) | 0.82 (0.34:1.95) | 1.79 (0.83:3.83) |
| Hispanic | 0.59 (0.24:1.47) | 0.89 (0.59:1.34) | 1.31 (0.62:2.74) | 2.38 (0.97:5.83) | 0.60 (0.27:1.32) |
| Age | 0.66 (0.21:2.07) | 1.33 (0.79:2.23) | 0.46 (0.13:1.68) | 0.79 (0.24:2.63) | 2.00 (0.57:7.05) |
| Bisexual | 1.80 (0.84:3.83) | 1.29 (0.88:1.90) | 2.41 (1.14:5.08)* | 1.27 (0.47:3.42) | 0.60 (0.27:1.34) |
| PSQ Knowledge | 0.68 (0.47:1.00)* | 0.89 (0.75:1.06) | 0.75 (0.53:1.07) | 0.58 (0.40:0.84)** | 0.84 (0.61:1.15) |
NOTE:
p < .05,
p < .01,
p < .001
Negative binomial model with effect estimate as event rate ratios
Logistic regression model with effect estimate as odds ratio. CAS = Condomless Anal Sex. PSQ = Parental Style Questionnaire.
Table 4.
Multivariate Negative Binomial and Linear Regression Models for RADAR Sample
| Binge Drinking (6 Months)2 | Marijuana Use (Last 30 Days)1 | Hard Drugs Used (6 Months)1 | CAS Acts (6 Months)1 | # CAS Partners (6 Months)1 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||||||
| Full Sample |
18 and Under |
19 and Over |
Full Sample |
18 and Under |
19 and Over |
Full Sample |
18 and Under |
19 and Over |
Full Sample |
18 and Under |
19 and Over |
Full Sample |
18 and Under |
19 and Over |
|
|
| |||||||||||||||
| M (SD) | |||||||||||||||
| 1.01 (1.03) |
.79 (.95) |
1.09 (1.04) |
2.85 (2.56) |
2.26 (2.30) |
3.07 (2.62) |
.34 (.78) |
.26 (.69) |
.37 (.82) |
17.82 (42.44) |
11.37 (30.50) |
19.97 (45.55) |
4.79 (7.56) |
4.30 (6.84) |
4.96 (7.84) |
|
|
| |||||||||||||||
| Unstd. Beta (95% CI) | Event Rate Ratio (95% CI) | Event Rate Ratio (95% CI) | Event Rate Ratio (95% CI) | Event Rate Ratio (95% CI) | |||||||||||
|
| |||||||||||||||
| Age | 0.03 (.01:.04)* |
– | – | 1.03 (1.02:1.05)* |
– | – | 1.07 (1.03:1.10)* |
– | – | 1.12 (1.07:1.17)* |
– | – | 1.07 (1.02:1.11)* |
– | – |
| Black | −0.59 (−.73: −.45)* |
−0.54 (−.80: −.29)* |
−0.60 (−.76: −.43)* |
1.19 (1.03:1.37)* |
1.18 (.87:1.58) |
1.19 (1.02:1.40)* |
0.38 (.27:.53)* |
0.22 (.08:.56)* |
0.45 (.31:.65)* |
0.79 (.55:1.13) |
0.34 (.16:.68)* |
1.02 (.69:1.51) |
1.23 (.78:1.94) |
3.11 (1.54:6.27)* |
0.83 (.50:1.36) |
| Hispanic | 0.11 (−.06:.28) |
0.12 (−.17:.42) |
0.12 (−.09:.32) |
0.89 (.76:1.04) |
1.12 (.79:1.60) |
0.83 (.69:.99)* |
0.81 (.57:1.15) |
0.74 (.34:1.62) |
0.81 (.55:1.20) |
0.68 (.46:.99)* |
0.98 (.47:2.01) |
0.65 (.42:.99)* |
0.74 (.47:1.16) |
0.55 (.29:1.03) |
0.70 (.39:1.25) |
| Other Race | 0.00 (−.17:.17) |
−0.13 (−.41:.16) |
0.04 (−.17:.25) |
0.98 (.83:1.16) |
1.20 (.89:1.63) |
0.90 (.74:1.09) |
0.73 (.51:1.05) |
0.85 (.41:1.74) |
0.68 (.45:1.03) |
0.91 (.63:1.33) |
1.19 (.61:2.29) |
0.78 (.50:1.22) |
1.14 (.73:1.78) |
0.95 (.51:1.77) |
0.98 (.53:1.81) |
| Bisexual | 0.06 (−.09:.22) |
0.06 (−.20:.31) |
0.09 (−.10:.28) |
1.18 (1.03:1.35)* |
1.13 (.85:1.50) |
1.23 (1.05:1.43) |
1.84 (1.33:2.53)* |
1.13 (.56:2.26) |
2.10 (1.47:3.00)* |
0.90 (.59:1.38) |
0.88 (.41:1.90) |
1.06 (.60:1.85) |
0.72 (.39:1.34) |
0.51 (.26:.98) |
1.16 (.55:2.46) |
| PFM Scale | −0.08 (−.17:.02) |
−0.12 (−.31:.06) |
−0.08 (−.19:.03) |
0.85 (.77:.94)* |
0.68 (.53:.87)* |
0.89 (.81:0.99)* |
0.67 (.54:.82)* |
0.79 (.44:1.40) |
0.65 (.52:.81)* |
0.73 (.58:.91)* |
0.66 (.41:1.06) |
0.73 (.58:.93)** |
0.85 (.66:1.09) |
0.72 (.53:.96)* |
0.94 (.69:1.30) |
NOTE:
p < .05;
Negative Binomial Model,
Linear Regression; PFM = Poor Family Management.
Table 3.
Multivariate Latent Growth Models for Crew 450 Sample
| Binge Drinking | Marijuana Use | Hard Drugs Used | CAS Acts | # CAS Partners | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (6 Months) | (6 Months) | (6 Months) | (6 Months) | (6 Months) | ||||||
|
| ||||||||||
| Baseline | Slope | Baseline | Slope | Baseline | Slope | Baseline | Slope | Baseline | Slope | |
| Unstandardized Estimate (95% CI) | ||||||||||
|
| ||||||||||
| Intercept | 3.32 (1.41:5.24)*** |
−0.23 (−0.63:0.17) |
1.78 (0.00:3.56) |
0.61 (0.20:1.02)* |
0.85 (0.05:1.65) |
0.12 (−0.06:0.31) |
−0.05 (−9.73:9.63) |
2.90 (−0.56:6.36) |
−0.15 (−1.39:1.09) |
0.19 (−0.15:0.52) |
| Black | −0.62 (−1.75:0.51) |
−0.18 (−0.44:0.13) |
0.97 (−.06:1.99) |
−0.75 (−0.99: −0.52)*** |
−0.16 (−0.58:0.25) |
−0.23 (−0.34: −0.11)** |
4.37 (−1.27:10.02) |
−1.90 (−4.31:0.50) |
0.77 (−0.06:1.59) |
−0.34 (−0.57: −0.11)* |
| Hispanic | −0.37 (−1.59:0.85) |
−0.11 (−0.39:0.18) |
0.66 (−0.42:1.74) |
−0.67 (−0.94: −0.40)*** |
0.20 (−0.36:0.76) |
−0.23 (−0.38: −0.08)* |
3.34 (−3.39:10.07) |
−0.86 (−3.63:1.93) |
0.62 (−0.21:1.45) |
−0.21 (−0.45:0.03) |
| Other Race | 0.00 (−1.74:1.74) |
−0.15 (−0.56:0.25) |
−0.13 (−1.99:1.73) |
−0.49 (−0.91: −0.07)* |
−0.11 (−0.64:0.41) |
−0.22 (−0.35: −0.08)** |
14.71 (3.01:26.41)* |
−4.80 (−7.86:1.74)* |
1.57 (0.42:2.72)* |
−0.54 (−0.85: −0.24)** |
| Bisexual | 0.23 (−0.69:1.15) |
−0.05 (−0.24:0.15) |
0.57 (−0.57:1.71) |
−0.05 (−0.36:0.26) |
0.07 (−0.37:0.50) |
−0.05 (−0.15:0.06) |
−5.83 (−13.06:1.40) |
1.59 (−0.98:4.16) |
−0.56 (−1.18:0.06) |
0.08 (−0.85:0.24) |
| PSQ Knowledge | −0.56 (−0.90: −0.21)** |
0.11 (0.03:0.18)* |
−0.32 (−0.75:0.11) |
0.03 (−0.09:0.15) |
−0.18 (−0.35: −0.01) |
0.16 (−0.01:0.08) |
0.43 (−2.10:2.95) |
−0.29 (−1.16:0.57) |
−0.13 (−0.38:0.13) |
0.00 (−0.08:0.08) |
NOTE:
p < .05,
p < .01,
p < .001
CAS = Condomless Anal Sex. PSQ = Parenting Style Questionnaire.
Outness to Parents, Parental Acceptance, and Parenting Practices
In terms of outness to parents, in the ChiGuys sample 75.4% were out to at least one parent, 74.2% in Crew 450 at baseline, and 82.5% in RADAR. In the ChiGuys sample, being out to parents was unrelated to level of parental knowledge of general activities (Mean Difference = −.03, p = .86). However, ChiGuys participants who were out to at least one parent reported significantly higher levels of parental knowledge of gay-specific activities (Mean Difference = 1.03, p < .001). Parental rejection scores were significantly negatively correlated with general knowledge (r = −.26, p < .01) and gay-specific knowledge (r = −.34, p < .001). In the Crew 450 sample, being out to the mother had a significant positive association with higher levels of general (Mean Difference = .36, p < .05) and gay-specific knowledge (Mean Difference = 1.36, p < .001). Outness to fathers was not associated with general knowledge in Crew 450 (Mean Difference = −17, p = .26), but was significantly and positively associated with gay-specific knowledge (Mean Difference = .73, p < .001). In the RADAR sample there were no associations between outness to parents and parental monitoring (Mean Difference = −.03, p = .70), and parental rejection showed only a small but significant negative association with monitoring (r = −.09, p < .05). No significant differences were found for age.
Effects of Parenting Practices on CAS and Substance Use
Knowledge of general and gay-specific activities had significant and positive correlations in the ChiGuys (r = .35, p < .001) and Crew 450 (r = .44, p < .001) samples. Initially, separate models were run with parental knowledge of gay-specific activities as the primary predictor, but these models were not significant for the ChiGuys or Crew 450 samples on any of the outcomes, so only results for parental knowledge of general activities are presented.
ChiGuys
The effects of parental knowledge on substance use and sexual risk taking behaviors in the ChiGuys sample are shown in Table 2. Controlling for age, race/ethnicity, and bisexual identity, higher parental knowledge was significantly associated with lower rates of binge drinking in the last 30 days and fewer CAS acts in the previous three months. There were no significant associations between parental knowledge and marijuana use, other drug use, and number of CAS partners.
Crew 450
Results for parental knowledge predicting rates of change in substance use and sexual risk taking behaviors from the multivariate latent growth curve model are shown in Table 3. In terms of demographic effects, participants who identified as Black, Hispanic/Latino, or were in the “other” race category all had significantly lower rates of growth in marijuana use and number of other drugs used compared to White participants. Participants who identified as Black had significantly lower growth in number of CAS partners compared to White participants. Participants in the “other” race category also had significantly higher number of baseline CAS acts, lower growth in CAS acts, higher baseline number of CAS partners, and lower growth in number of CAS partners compared to White participants.
Higher parental knowledge was significantly associated with lower baseline binge drinking. Overall the slope for binge drinking was not significantly different than zero, but parental knowledge was significantly associated with the slope of binge drinking over time. A plot of the effect of parental knowledge (see Figure 1) indicated that those higher in parental knowledge at baseline started at lower levels of binge drinking but over time showed increases to become more similar in level of binge drinking as those lower in parental knowledge at baseline. Parental knowledge was not significantly associated with baseline levels or developmental changes in marijuana use, other drugs, number of CAS acts, or number of CAS partners.
Figure 1.
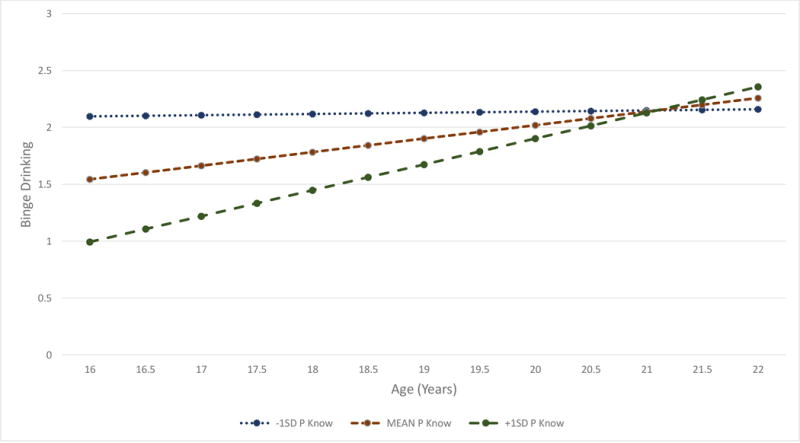
Binge drinking levels across development by levels of parental knowledge in the Crew 450 sample.
NOTE: P Know = Parental Knowledge, SD = standard deviation. For the purpose of illustrating effects levels of binge drinking over time are plotted for baseline levels of parental knowledge 1 SD below the mean, at the mean, and 1 SD above the mean.
RADAR
Results for parental monitoring on substance use and sexual risk behaviors are presented in Table 4. Black participants had significantly lower levels of binge drinking and used significantly fewer hard drugs compared to White participants, but they reported significantly higher levels of marijuana use. Black participants 18 years and under reported a significantly higher number of condomless sex partners compared to White participants. Hispanic/Latino participants reported significantly fewer condomless anal sex acts compared to White participants. Hispanic/Latino participants 19 years and over reported significantly lower marijuana use compared to White participants. Bisexual participants reported significantly higher marijuana use and more hard drugs used compared to participants who reported a different sexual orientation.
Higher parental monitoring was significantly associated with less marijuana use for the whole RADAR sample, for participants 18 years and under, and for participants 19 and over. Higher parental monitoring was significantly associated with a lower number of other drugs used in the full sample and the 19 years and over group. Higher parental monitoring was also significantly associated with lower numbers of CAS acts and fewer CAS partners for the 18 years and under group. There were no significant associations between parental monitoring and binge drinking.
Discussion
The purpose of this study was to examine if two specific dimensions of parenting practice—monitoring of adherence to rules and knowledge of child whereabouts and activities— were predictors of engagement in HIV risk behaviors and substance use among YMSM. In terms of engagement in HIV risk taking behaviors, parental knowledge was significantly associated with CAS in the youngest sample (ChiGuys), but not baseline levels (estimated at age 16) or longitudinal changes in Crew 450. Parental monitoring was significantly associated with CAS in the RADAR sample, but only for participants who were age 18 years and under. In the RADAR sample the effects were significant for both number of CAS acts and number of CAS partners, whereas in the ChiGuys sample effects were only significant for number of CAS acts. As two-thirds of our samples found significant associations between parenting practices and CAS among those 18 and under we suggest this is a promising area for future HIV prevention research with YMSM.
In terms of substance use, parental knowledge was related to rates of binge drinking in both of the samples where it was measured (ChiGuys and Crew 450), but it was not related to use of other substances. The ChiGuys sample was the youngest sample and the longitudinal analysis of the Crew 450 data showed a significant effect on baseline binge drinking as estimated at age 16 years. As such, it appears that parental knowledge has significant protective effects against binge drinking in middle-to-late adolescents. The significant effect on slope in the Crew 450 sample also suggests effects may be limited over time because YMSM with lower levels of parental knowledge had significantly higher rates of binge drinking at age 16, but over time showed similar rates to youth with higher parental knowledge. Parental monitoring was not related to binge drinking in the RADAR sample, but it was associated with rates of marijuana use and use of hard drugs in the older segment of the sample (19 years and over). Taken together, findings suggest general parental knowledge is related to binge drinking, but not other drugs, whereas parental monitoring is related to marijuana use and use of other drug in older youth. It’s important to note that youth who were not living with their parents (primarily older participants) were asked to recall past parental monitoring when they did live at home. This pattern may reflect higher access and use of illicit drugs at older ages (19 years and older), which is also a time when parents tend to reduce their ongoing tracking of their child’s whereabouts and begin to rely on the child’s internalization of rules about drug use. Alcohol is much more available at younger ages than illicit drugs, and binge drinking is more detectable by parents due to obvious intoxication and signals of alcohol consumption, such as smell. As such, parental knowledge may have greater effects at younger ages when YMSM are living at home and alcohol consumption is illegal, whereas for drugs that become more available later when children are less likely to live at home it is the internalization of parental rules that may be more important.
Across both HIV risk behaviors and substance use a general pattern across samples was that we observed larger effects at younger ages. This pattern makes sense in light of the significant negative association between parental knowledge and age we found in the ChiGuys and Crew 450 samples. This age difference likely reflect the developmental process of parents engaging in less solicitation of information about their children’s whereabouts as they grow up and expect greater independence53-55. As these developmental changes occur parental knowledge of activities naturally becomes a less effective strategy for prevention of sexual risk taking and substance use.
One innovative aspect of our study was the inclusion of a measure of knowledge that focused specifically on telling parents about attending gay-specific activities. The mean score on this scale suggested that it was less common for the YMSM participants to tell their parents about attending gay events and about their gay friends. Consistent across samples, scores on this gay-specific measure were significantly lower than the more general knowledge measure. The gay-specific and general parental knowledge measures were moderately correlated, which suggests that youth who tell their parents more about their general whereabouts also tend to tell them more about gay-specific activities. However, that they were only moderately correlated indicates that these are separate dimensions and that general parental knowledge measures only provide a modest amount of information about how much young people are telling them about gay-specific aspects of their lives.
Consistent across samples, being out to parents significantly increased scores on gay-specific parental knowledge, however if YMSM perceived their parents as being rejecting of their sexual orientation then scores were significantly lower. These results are consistent with the only other study to examine these associations, which found that in a sample of 14-19 year old MSM (mean age = 17.37) that participants who were out to their parents reported they were significantly more likely to keep their parents informed of their general whereabouts and activities38. As such these results suggest that reacting in a rejecting manner to a child’s sexual orientation is a barrier to effectively monitoring to protect them from engaging in behaviors that could put them at risk. As such, programs that can increase parental acceptance may have additional benefits on effective parenting practices.
Across all outcomes, our novel measure of gay-specific parental knowledge showed no significant relationships with HIV risk or substance use outcomes. This lack of relationship may reflect the fact that levels of gay-specific parental knowledge were low, and significantly lower among youth who were not out or whose parents were more rejecting. If YMSM are not telling their parents about their whereabouts when attending gay venues or activities it would hinder their parents’ ability to engage in effective supervision of those activities. Research in general adolescent samples has found that adolescents who perceive their parents as disapproving of activities they engage in are more likely to lie to their parents56. Consistent with this interpretation, existing evidence suggests YMSM may not tell their parents about involvement in gay-specific venues or events, particularly when they are not out to their parents, their parents are rejecting, or the family atmosphere discourages discussions of same-sex relationships38,39,57. For example, in interviews with young adult MSM about their coming out experiences with their fathers, Jadwin-Cakmak and colleagues58 described reactions that included explicit prohibitions on discussing same-sex activities (i.e., denial) or that expressed hurt feelings. Such reactions would likely silence YMSM from telling their parents about their activities and relationships in the gay community. In interviews with parents of gay and lesbian children, Saltzburg59 described how emotional anguish associated with grappling with their child’s sexual orientation led some parents to disengage from parenting functions.
Our results have a number of implications for future research and prevention efforts with YMSM. First, low endorsement by YMSM of perceived parental monitoring and knowledge, coupled with some significant associations with substance use and HIV risk behavior, suggest the value of parent- and family-interventions that can help improve parenting practices that can reduce risks of substance use and HIV. Several such programs have been found effective with presumably heterosexual samples29-31, and with adaption to meet the unique needs of YMSM and their parents such prevention programs could be highly impactful60,61. It would also be informative to examine if the YMSM who may have participated in these family-based interventions show similar prevention effects as heterosexual young men. Second, more research is needed to inform the development of YMSM-specific programs. Given some of the inconsistent results across samples in the current study, moderators of effects should be explored in future research, as should greater attention to the specific dimensions of parenting practice being studied. Also needed is research that involves parents as participants in order to understand their needs and perspectives20. Studies of parents of YMSM are nearly non-existent to date, with only some exceptions59,62. Obtaining information only on youths’ perspectives omits critical information needed to understand these bidirectional and dynamic relationships, as demonstrated by research with heterosexual youth that has shown parent and child reports convey unique information63.
Findings from this study must be interpreted in the context of the limitations of the design. First, our study relied on adolescent self-report to measure their perspectives on parental knowledge and monitoring and the study outcomes. Second, two of the studies were cross-sectional and the longitudinal study only measured parenting variables on a single occasion. Longitudinal measurement of parenting practices and outcomes would allow for modeling of the dynamic bi-directional relationship between parenting and adolescent behaviors. Third, data for all three studies came from a single geographic location, and while the samples were racially/ethnically diverse, different results may be found in difference communities. Fourth, some of the participants in the Crew 450 and ChiGuys studies also later participated in the RADAR study. Concerns about how this may have impacted study findings are ameliorated by the fact that RADAR used a different measure of parenting so the same construct was not tested with the same participant more than once. Furthermore, sensitivity analyses were performed with the Crew 450 and ChiGuys participants removed from the RADAR sample and the findings were unchanged. Despite study limitations, our findings support the need for further research on the influences of parents on YMSM health risk behaviors and support the value of developing family- and parent-interventions that could address parents’ roles in supporting healthy same-sex relationships, acceptance of child’s sexual orientation, and more universal parenting practices such as monitoring.
Acknowledgments
We acknowledge the grant funding that supported the studies described in this manuscript: Crew 450 (National Institute on Drug Abuse, R01DA025548), ChiGuys (Centers for Disease Control and Prevention and Chicago Department of Public Health), and RADAR (National Institute on Drug Abuse, U01DA036939). We acknowledge the NIH supported Third Coast Center for AIDS Research for creating a supportive environment for HIV/AIDS research (P30AI117943). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders. Dr. Robert Garofalo was a multiple PI with Dr. Mustanski on Crew 450, and we thank him and his team for their involvement in that project. We thank the participants for sharing their experiences with us.
Funding: This study was funded by the National Institute on Drug Abuse (R01DA025548 & U01DA036939), Centers for Disease Control and Prevention, and Chicago Department of Public Health.
Footnotes
Compliance with Ethical Standards:
Conflict of Interest: The authors have no conflicts of interest to declair.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent: Informed consent was obtained from all individual participants included in the study.
References
- 1.Everett BG, Schnarrs PW, Rosario M, Garofalo R, Mustanski B. Sexual orientation disparities in sexually transmitted infection risk behaviors and risk determinants among sexually active adolescent males: results from a school-based sample. Am J Public Health. 2014;104:1107–1112. doi: 10.2105/AJPH.2013.301759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Newcomb ME, Birkett M, Corliss HL, Mustanski B. Sexual orientation, gender, and racial differences in illicit drug use in a sample of US high school students. Am J Public Health. 2014;104:304–310. doi: 10.2105/AJPH.2013.301702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.CDC. HIV Surveillance - adolescents and young adults through 2014. 2016;6:7–43. http://www.cdc.gov/hiv/pdf/library/slidesets/cdc-hiv-surveillance-adolescents-young-adults-2014.pdf. Accessed 2 February 2016. [Google Scholar]
- 4.CDC. HIV Surveillance - men who have sex with men (MSM) 2016 http://www.cdc.gov/hiv/library/slideSets/index.html. Accessed 4 May 2016.
- 5.Garofalo R, Hotton AL, Kuhns LM, Gratzer B, Mustanski B. Incidence of HIV infection and sexually transmitted infections and related risk factors among very young men who have sex with men. J Acquir Immune Defic Syndr. 2016;72:79–86. doi: 10.1097/QAI.0000000000000933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beck EC, Birkett M, Armbruster B, Mustanski B. A data-driven simulation of HIV spread among young men who have sex with men: role of age and race mixing and STIs. J Acquir Immune Defic Syndr. 2015;70:186–194. doi: 10.1097/QAI.0000000000000733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marshal MP, Friedman MS, Stall R, et al. Sexual orientation and adolescent substance use: a meta-analysis and methodological review. Addiction. 2008;103:546–556. doi: 10.1111/j.1360-0443.2008.02149.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Marshal MP, Friedman MS, Stall R, Thompson AL. Individual trajectories of substance use in lesbian, gay and bisexual youth and heterosexual youth. Addiction. 2009;104:974–981. doi: 10.1111/j.1360-0443.2009.02531.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mustanski B, Newcomb M, Du Bois SN, Garcia SC, Grov C. HIV in young men who have sex with men: a review of epidemiology, risk and protective factors, and interventions. J Sex Res. 2011;48:218–253. doi: 10.1080/00224499.2011.558645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mustanski B, Newcomb ME, Clerkin EM. Relationship characteristics and sexual risk-taking in young men who have sex with men. Health Psychol. 2011;30:597–605. doi: 10.1037/a0023858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Balaji AB, Bowles KE, Le BC, Paz-Bailey G, Oster AM, Group NS High HIV incidence and prevalence and associated factors among young MSM, 2008. AIDS. 2013;27:269–278. doi: 10.1097/QAD.0b013e32835ad489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Newcomb ME, Mustanski B. Developmental change in the relationship between alcohol and drug use before sex and sexual risk behavior in young men who have sex with men. AIDS Behav. 2014;18:1981–1990. doi: 10.1007/s10461-014-0766-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Halkitis PN, Moeller RW, Siconolfi DE, Storholm ED, Solomon TM, Bub KL. Measurement model exploring a syndemic in emerging adult gay and bisexual men. AIDS Behav. 2013;17:662–673. doi: 10.1007/s10461-012-0273-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Celentano DD, Valleroy LA, Sifakis F, et al. Associations between substance use and sexual risk among very young men who have sex with men. J Sex Transm Dis. 2006;33:265–271. doi: 10.1097/01.olq.0000187207.10992.4e. [DOI] [PubMed] [Google Scholar]
- 15.Mustanski B, Garofalo R, Herrick A, Donenberg G. Psychosocial health problems increase risk for HIV among urban young men who have sex with men: preliminary evidence of a syndemic in need of attention. Ann Behav Med. 2007;34:37–45. doi: 10.1080/08836610701495268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Clutterbuck DJ, Gorman D, McMillan A, Lewis R, Macintyre CC. Substance use and unsafe sex amongst homosexual men in Edinburgh. AIDS Care. 2001;13:527–535. doi: 10.1080/09540120120058058. [DOI] [PubMed] [Google Scholar]
- 17.Drumright LN, Little SJ, Strathdee SA, et al. Unprotected anal intercourse and substance use among men who have sex with men with recent HIV infection. J Acquir Immune Defic Syndr. 2006;43:344–350. doi: 10.1097/01.qai.0000230530.02212.86. [DOI] [PubMed] [Google Scholar]
- 18.Hirshfield S, Remien RH, Humberstone M, Walavalkar I, Chiasson MA. Substance use and high-risk sex among men who have sex with men: a national online study in the USA. AIDS Care. 2004;16:1036–1047. doi: 10.1080/09540120412331292525. [DOI] [PubMed] [Google Scholar]
- 19.Vosburgh HW, Mansergh G, Sullivan PS, Purcell DW. A review of the literature on event-level substance use and sexual risk behavior among men who have sex with men. AIDS Behav. 2012;16:1394–1410. doi: 10.1007/s10461-011-0131-8. [DOI] [PubMed] [Google Scholar]
- 20.Mustanski B. Future directions in research on sexual minority adolescent mental, behavioral, and sexual health. J Clin Child Adolesc Psychol. 2015;44:204–219. doi: 10.1080/15374416.2014.982756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bouris A, Guilamo-Ramos V, Pickard A, et al. A systematic review of parental influences on the health and well-being of lesbian, gay, and bisexual youth: time for a new public health research and practice agenda. J Prim Prev. 2010;31:273–309. doi: 10.1007/s10935-010-0229-1. [DOI] [PubMed] [Google Scholar]
- 22.Herrick AL, Stall R, Goldhammer H, Egan JE, Mayer KH. Resilience as a research framework and as a cornerstone of prevention research for gay and bisexual men: theory and evidence. AIDS Behav. 2014;18:1–9. doi: 10.1007/s10461-012-0384-x. [DOI] [PubMed] [Google Scholar]
- 23.Savin-Williams RC. Then and now: recruitment, definition, diversity, and positive attributes of same-sex populations. Dev Psychol. 2008;44:135–138. doi: 10.1037/0012-1649.44.1.135. [DOI] [PubMed] [Google Scholar]
- 24.Bronfenbrenner U. Ecological systems theory. In: Vasta R, editor. Six theories of child development: revised formulations and current issues. Vol. 1992. London: Jessica Kingsley Publishers; pp. 187–250. [Google Scholar]
- 25.Rhodes SD, Wong FY. HIV prevention among diverse young MSM: research needs, priorities, and opportunities. AIDS Educ Prev. 2016;28:191–201. doi: 10.1521/aeap.2016.28.3.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Widman L, Choukas-Bradley S, Noar SM, Nesi J, Garrett K. Parent-adolescent sexual communication and adolescent safer sex behavior: a meta-analysis. JAMA Pediatr. 2016;170:52–61. doi: 10.1001/jamapediatrics.2015.2731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dittus PJ, Michael SL, Becasen JS, Gloppen KM, McCarthy K, Guilamo-Ramos V. Parental monitoring and its associations with adolescent sexual risk behavior: a meta-analysis. Pediatr. 2015;136:e1587–1599. doi: 10.1542/peds.2015-0305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Downing J, Jones L, Bates G, Sumnall H, Bellis MA. A systematic review of parent and family-based intervention effectiveness on sexual outcomes in young people. Health Educ Res. 2011;26:808–833. doi: 10.1093/her/cyr019. [DOI] [PubMed] [Google Scholar]
- 29.Coatsworth JD, Pantin H, Szapocznik J. Familias unidas: a family-centered ecodevelopmental intervention to reduce risk for problem behavior among Hispanic adolescents. Clin Child Fam Psychol Rev. 2002;5:113–132. doi: 10.1023/a:1015420503275. [DOI] [PubMed] [Google Scholar]
- 30.Prado G, Pantin H, Huang S, et al. Effects of a family intervention in reducing HIV risk behaviors among high-risk Hispanic adolescents: a randomized controlled trial. Arch Pediatr Adolesc Med. 2012;166:127–133. doi: 10.1001/archpediatrics.2011.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kogan SM, Yu T, Brody GH, et al. Integrating condom skills into family-centered prevention: efficacy of the strong African American families-teen program. J Adolesc Health. 2012;51:164–170. doi: 10.1016/j.jadohealth.2011.11.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Prado G, Cordova D, Huang S, et al. The efficacy of familias unidas on drug and alcohol outcomes for Hispanic delinquent youth: main effects and interaction effects by parental stress and social support. Drug Alcohol Depend. 2012;125(Suppl 1):S18–25. doi: 10.1016/j.drugalcdep.2012.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Brody GH, Chen YF, Kogan SM, et al. Family-centered program deters substance use, conduct problems, and depressive symptoms in black adolescents. Pediatrics. 2012;129:108–115. doi: 10.1542/peds.2011-0623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ryan SM, Jorm AF, Lubman DI. Parenting factors associated with reduced adolescent alcohol use: a systematic review of longitudinal studies. Aust N Z J Psychiatry. 2010;44:774–783. doi: 10.1080/00048674.2010.501759. [DOI] [PubMed] [Google Scholar]
- 35.Stone AL, Becker LG, Huber AM, Catalano RF. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict Behav. 2012;37:747–775. doi: 10.1016/j.addbeh.2012.02.014. [DOI] [PubMed] [Google Scholar]
- 36.Kuntsche S, Kuntsche E. Parent-based interventions for preventing or reducing adolescent substance use - a systematic literature review. Clin Psychol Rev. 2016;45:89–101. doi: 10.1016/j.cpr.2016.02.004. [DOI] [PubMed] [Google Scholar]
- 37.Van Ryzin MJ, Roseth CJ, Fosco GM, Lee YK, Chen IC. A component-centered meta-analysis of family-based prevention programs for adolescent substance use. Clin Psychol Rev. 2016;45:72–80. doi: 10.1016/j.cpr.2016.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Thoma BC, Huebner DM. Parental monitoring, parent-adolescent communication about sex, and sexual risk among young men who have sex with men. AIDS Behav. 2014;18:1604–1614. doi: 10.1007/s10461-014-0717-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Fisher CB, Arbeit MR, Dumont MS, Macapagal K, Mustanski B. Self-consent for HIV prevention research involving sexual and gender minority youth: reducing barriers through evidence-based ethics. J Empir Res Hum Res Ethics. 2016;11:3–14. doi: 10.1177/1556264616633963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mustanski B, Newcomb M, Garofalo R. Mental health of lesbian, gay, and bisexual youth: a developmental resiliency perspective. Journal of Gay & Lesbian Social Services. 2011;23:204–225. doi: 10.1080/10538720.2011.561474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pearson J, Wilkinson L. Family relationships and adolescent well-being: are families equally protective for same-sex attracted youth? J Youth Adolesc. 2013;42:376–393. doi: 10.1007/s10964-012-9865-5. [DOI] [PubMed] [Google Scholar]
- 42.Mustanski B, Phillips G, 2nd, Ryan DT, Swann G, Kuhns L, Garofalo R. Prospective effects of a syndemic on HIV and STI incidence and risk behaviors in a cohort of young men who have sex with men. AIDS Behav. 2016 doi: 10.1007/s10461-016-1607-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Paz-Bailey G, Raymond HF, Lansky A, Mermin J. Using the National HIV Behavioral Surveillance System to inform HIV prevention efforts in the United States. AIDS Behav. 2014;18(Suppl 3):S233–236. doi: 10.1007/s10461-014-0738-7. [DOI] [PubMed] [Google Scholar]
- 44.Balaji AB. The national HIV behavioral surveillance system for young men who have sex with men (NHBS-YMSM): designing and implementing HIV surveillance for the next generation. National HIV Prevention Conference; Atlanta. 2015. [Google Scholar]
- 45.Mustanski B, Garofalo R, Emerson EM. Mental health disorders, psychological distress, and suicidality in a diverse sample of lesbian, gay, bisexual, and transgender youths. Am J Public Health. 2010;100:2426–2432. doi: 10.2105/AJPH.2009.178319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mustanski B. Ethical and regulatory issues with conducting sexuality research with LGBT adolescents: a call to action for a scientifically informed approach. Arch Sex Behav. 2011;40:673–686. doi: 10.1007/s10508-011-9745-1. [DOI] [PubMed] [Google Scholar]
- 47.Donenberg GR, Wilson HW, Emerson E, Bryant FB. Holding the line with a watchful eye: the impact of perceived parental permissiveness and parental monitoring on risky sexual behavior among adolescents in psychiatric care. AIDS Educ Prev. 2002;14:138–157. doi: 10.1521/aeap.14.2.138.23899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Oregon Social Learning Center. Parental monitoring and supervision constructs (technical reports) Eugene, OR: Oregon Social Learning Center; 1990. [Google Scholar]
- 49.Arthur MW, Hawkins JD, Pollard JA, Catalano RF, Baglioni AJ., Jr Measuring risk and protective factors for substance use, delinquency, and other adolescent problem behaviors: the communities that care youth survey. Eval Rev. 2002;26:575–601. doi: 10.1177/0193841X0202600601. [DOI] [PubMed] [Google Scholar]
- 50.Glaser RR, Van Horn ML, Arthur MW, Hawkins JD, Catalano RF. Measurement properties of the Communities That Care (R) Youth Survey across demographic groups. J Quant Criminol. 2005;21:73–102. [Google Scholar]
- 51.Arthur MW, Briney JS, Hawkins JD, Abbott RD, Brooke-Weiss BL, Catalano RF. Measuring risk and protection in communities using the Communities That Care Youth Survey. Eval Program Plann. 2007;30:197–211. doi: 10.1016/j.evalprogplan.2007.01.009. [DOI] [PubMed] [Google Scholar]
- 52.Mustanski B, Starks T, Newcomb ME. Methods for the design and analysis of relationship and partner effects on sexual health. Arch Sex Behav. 2014;43:21–33. doi: 10.1007/s10508-013-0215-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Keijsers L, Frijns T, Branje SJ, Meeus W. Developmental links of adolescent disclosure, parental solicitation, and control with delinquency: moderation by parental support. Dev Psychol. 2009;45:1314–1327. doi: 10.1037/a0016693. [DOI] [PubMed] [Google Scholar]
- 54.Wang MT, Dishion TJ, Stormshak EA, Willett JB. Trajectories of family management practices and early adolescent behavioral outcomes. Dev Psychol. 2011;47:1324–1341. doi: 10.1037/a0024026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Laird RD, Criss MM, Pettit GS, Bates JE, Dodge KA. Developmental trajectories and antecedents of distal parental supervision. J Early Adolesc. 2009;29:258–284. doi: 10.1177/0272431608320123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Darling N, Cumsille P, Caldwell LL, Dowdy B. Predictors of adolescents' disclosure to parents and perceived parental knowledge: between- and within-person differences. Journal of Youth and Adolescence. 2006;35:667–678. [Google Scholar]
- 57.Heatherington L, Lavner JA. Coming to terms with coming out: review and recommendations for family systems-focused research. J Fam Psychol. 2008;22:329–343. doi: 10.1037/0893-3200.22.3.329. [DOI] [PubMed] [Google Scholar]
- 58.Jadwin-Cakmak LA, Pingel ES, Harper GW, Bauermeister JA. Coming out to dad: young gay and bisexual men’s experiences disclosing same-sex attraction to their fathers. Am J Mens Health. 2015;9:274–288. doi: 10.1177/1557988314539993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Saltzburg S. Learning that an adolescent child is gay or lesbian: the parent experience. Soc Work. 2004;49:109–118. doi: 10.1093/sw/49.1.109. [DOI] [PubMed] [Google Scholar]
- 60.Garofalo R, Mustanski B, Donenberg G. Parents know and parents matter; is it time to develop family-based HIV prevention programs for young men who have sex with men? J Adolesc Health. 2008;43:201–204. doi: 10.1016/j.jadohealth.2008.01.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Mustanski B, Hunter J. Parents as agents of HIV prevention for gay, lesbian, and bisexual youth. In: Pequegnat W, Bell C, editors. Families and HIV/AIDS. Vol. 2009. Washington, D.C.: Springer New York; pp. 249–260. [Google Scholar]
- 62.Newcomb ME, Clifford A, Greene GJ, Mustanski B. Parent perspectives about sexual minority adolescent participation in research and requirements of parental permission. J Adolesc Health. 2016;59:443–449. doi: 10.1016/j.jadohealth.2016.05.014. [DOI] [PubMed] [Google Scholar]
- 63.De Los Reyes A, Kazdin AE. Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull. 2005;13:483–509. doi: 10.1037/0033-2909.131.4.483. [DOI] [PubMed] [Google Scholar]