

ABSTRACT
Introduction: Mycobacterium Nebraskense is a rare nontuberculous mycobacterial infection. The first isolate of the species was from human sputum at University of Nebraska Medical Center. There are only a few cases have been reported and the exact behavior of the disease is not clearly described. Here, we present a case from New York City incidentally found to have a cavitary lung lesion due to M. nebraskense.
Case report: An 82-year-old female with a history of diabetes mellitus, hypertension, and dementia presented with constipation and urinary retention for 1 day. She had no fever, cough, shortness of breath, nausea, vomiting, appetite change, or weight loss. Computed tomography (CT) scan of abdomen and pelvis revealed retained fecal material in the colon, non-obstructing left renal calculus, and bilateral small pleural effusion with right-sided lung infiltrates. Subsequent CT scan of the chest showed 4.5 cm pleural-based opacity in right lung base with a small cavity. Sputum smear for Acid-fast bacilli was positive. Mycobacterial culture reported positive growth of M. nebraskense, while polymerase chain reaction returned negative for Mycobacterium gordonae, Mycobacterium kansasii, Mycobacterium avium complex and Mycobacterium tuberculosis. With the patient asymptomatic and her constipation improved, she was discharged with plans for close follow-up as outpatient.
Conclusion : M. nebraskense is a very rare nontuberculous mycobacterial infection. From only a few cases reported in the USA, the exact presentation of infection, disease progression, and treatment have not been described well. Asymptomatic cavitary lung disease caused by M. nebraskense has not been reported before.
KEYWORDS: Mycobacterium nebraskense, nontuberculous mycobacterium, cavitary lung disease, rare nontuberculous mycobacterium, scotochromogenic mycobacterium
1. Introduction
Nontuberculous mycobacteria (NTM) species are generally free-living organisms and are normally found in soil and water. More than 140 species of NTM have been identified. They continue to emerge as a major cause of opportunistic infection. They can cause a variety of manifestations. The lungs are the most commonly involved sites, and they cause different pulmonary manifestations especially in the elderly with or without underlying lung disease [1,2]. Some of the common NTM to cause lung disease are Mycobacterium avium complex (MAC), Mycobacterium kansasii, Mycobacterium malmoense, and Mycobacterium xenopi [1–3].
Mycobacterium nebraskense is a rare NTM. It is a scotochromogenic mycobacterium and was first isolated from sputum samples of five patients at the University of Nebraska Medical Center. A few other cases of human infection with M. nebraskense have been reported [4]. Here, we present a case from New York City incidentally found to have a cavitary lung lesion due to M. nebraskense.
2. Case description
An 82-year-old African-American female was brought from nursing home after she complained of vague abdominal discomfort for 1 day. She had no nausea, vomiting, shortness of breath, cough, night sweats, fever, appetite change, or weight loss. The review of symptoms was otherwise unremarkable. Her past medical history included dementia, diabetes mellitus, and hypertension. On admission, her blood pressure was 92/63 mm Hg, pulse rate was 83 bpm, temperature was 97° F, respiratory rate was 19/min, and oxygen saturation was 99% on room air. Physical examination revealed reduced air entry with fine crepitation on right lung base, mild abdominal distension, and diffuses tenderness with no guarding, rigidity, or rebound tenderness. Laboratory findings were significant for hemoglobin of 11.2 gm/dl, blood urea nitrogen level of 38 mg/dl, serum creatinine of 1.6 mg/dl, blood glucose of 393 mg/dl, amylase of 115 mg/dl, and serum albumin of 2.8 gm/dl. White blood cell count, serum lipase, ketones, and lactic acid levels were normal. Blood cultures showed no growth. Computed tomography (CT) scan of abdomen and pelvis revealed retained fecal material in the colon, non-obstructing left renal calculus, and bilateral small pleural effusion with right-sided lung infiltrates. The patient was managed for constipation and suspected pneumonia, and was started on ceftriaxone and azithromycin. Subsequent CT scan of the chest (Figure 1) showed 4.5 cm pleural-based opacity in right lung base with a small cavity, patchy ground-glass opacity in right upper and right middle lobe along with bibasilar subsegmental atelectasis. Antibiotics were discontinued after 2 days as clinical suspicion of bacterial pneumonia was low. She was placed on airborne isolation. Subsequently, sputum smear for acid-fast bacilli was positive. Mycobacterial culture reported positive growth of M. nebraskense, while polymerase chain reaction returned negative for Mycobacterium gordonae, M. kansasii, MAC, and Mycobacterium tuberculosis. With the patient asymptomatic and her constipation improved with laxatives, she was discharged with plans for close follow-up as outpatient.
Figure 1.
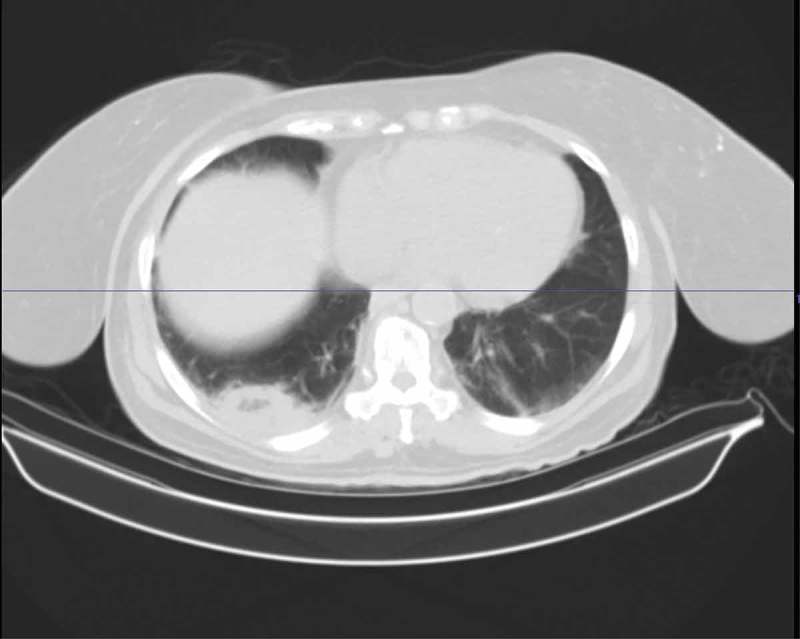
Chest CT scan reveals right lower lobe cavity.
3. Discussion
Nontuberculous mycobacterial infection of the lung usually presents in three forms. The first form is in patients with immunosuppression or underlying structural lung disease, primarily white, middle-aged, or elderly men, often alcoholic or smokers with underlying structural lung disease. The disease resembles typical tuberculosis clinically and radiographically, with cough, weight loss, upper lobe infiltrates, and cavities [5,6]. The second form presents as nodular bronchiectasis in immunocompetent adults without known underlying lung disease, usually nonsmoking slender women who have some skeletal deformities [7,8]. The third form presents as hypersensitivity pneumonitis after use of hot tubs and medicinal baths [9].
NTM infection has been also reported in women without clearly recognized predisposing factors as in our case [10].
Typical radiological findings of NTM infections in immunocompetent patients without underlying lung disease are multiple small parenchymal nodules in a centrilobular pattern, progressive fibrosis which associated with traction bronchiectasis involving more than one lobe [11]; however, our patient did not have any of these lesions on chest CT scan and the only finding was right lower lobe cavitary lesion.
M. nebraskense is a rare NTM and was first isolated from sputum samples in Nebraska. While mostly reported as an opportunistic infection in the immunosuppressed, immunocompetent hosts have been also affected. Prior cases have been reported as nodular lung disease [4]. M. nebraskense had been reported in a patient with underlying emphysema who presented with cough and hemoptysis [12]. However, our patient had no known underlying lung disease or immunosuppression. She had no pulmonary symptoms. However, she was incidentally found to have cavitary lung lesion with the sputum culture growing M. nebraskense. Cavitary lesion with M. nebraskense has not been reported before. As the patient was asymptomatic, it was prudent to follow the patient closely for disease progression in terms of developing clinical symptoms or worsening radiological finding.
Treatment guidelines for M. nebraskense have not been well established. However, one reported case was successfully treated with rifampin and azithromycin [4].
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- [1]. Wolinsky E. Nontuberculous mycobacteria and associated diseases. Am Rev Respir Dis. 1979;119(1):107–159. [DOI] [PubMed] [Google Scholar]
- [2]. Griffith DE, Aksamit T, Brown-Elliott BA, et al., Infectious Disease Society of America . An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416. DOI: 10.1164/rccm.200604-571ST. [DOI] [PubMed] [Google Scholar]
- [3]. Hoefsloot W, Van Ingen J, Andrejak C, et al., Nontuberculous Mycobacteria Network European Trials Group . The geographic diversity of nontuberculous mycobacteria isolated from pulmonary samples: an NTM-NET collaborative study. Eur Respir J. 2013;42(6):1604–1613. DOI: 10.1183/09031936.00149212. [DOI] [PubMed] [Google Scholar]
- [4]. Puthalapattu S, Metersky ML. Mycobacterium nebraskense as a cause of nodular pulmonary disease. Conn Med. 2011;75(9):527–529. [PubMed] [Google Scholar]
- [5]. Ahn CH, McLarty JW, Ahn SS, et al. Diagnostic criteria for pulmonary disease caused by Mycobacterium kansasii and Mycobacterium intracellulare. Am Rev Respir Dis. 1982;125(4):388–391. [DOI] [PubMed] [Google Scholar]
- [6]. Teirstein AS, Damsker B, Kirschner PA, et al. Pulmonary infection with Mycobacterium avium-intracellulare: diagnosis, clinical patterns, treatment. Mt Sinai J Med. 1990;57(4):209–215. [PubMed] [Google Scholar]
- [7]. Prince DS, Peterson DD, Steiner RM, et al. Infection with Mycobacterium avium complex in patients without predisposing conditions. N Engl J Med. 1989;321(13):863–868. [DOI] [PubMed] [Google Scholar]
- [8]. Reich JM, Johnson RE. Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest. 1992;101(6):1605–1609. [DOI] [PubMed] [Google Scholar]
- [9]. Khoor A, Leslie KO, Tazelaar HD, et al. Diffuse pulmonary disease caused by nontuberculous mycobacteria in immunocompetent people (hot tub lung). Am J Clin Pathol. 2001;115(5):755–762. [DOI] [PubMed] [Google Scholar]
- [10]. Griffith DE, Girard WM, Wallace RJ Jr.. Clinical features of pulmonary disease caused by rapidly growing mycobacteria. An analysis of 154 patients. Am Rev Respir Dis. 1993;147(5):1271–1278. [DOI] [PubMed] [Google Scholar]
- [11]. Chung JH, Huitt G, Yagihashi K, et al. Proton magnetic resonance imaging for initial assessment of isolated mycobacterium avium complex pneumonia. Ann Am Thorac Soc. 2016;13(1):49–57. [DOI] [PubMed] [Google Scholar]
- [12]. Iwen PC, Tarantolo SR, Mohamed AM, et al. First report of Mycobacterium nebraskense as a cause of human infection. In Diagn Microbiol Infect Dis. 2006;56(4):451–453. [DOI] [PubMed] [Google Scholar]