

Abstract
Background
Vasopressors are frequently used to increase blood pressure in order to ensure sufficient cerebral perfusion and oxygenation (CPO) during hypotensive periods in anaesthetized patients. Efficacy depends both on the vasopressor and anaesthetic protocol used. Propofol–remifentanil total intravenous anaesthesia (TIVA) is common in human anaesthesia, and dexmedetomidine is increasingly used as adjuvant to facilitate better haemodynamic stability and analgesia. Little is known of its interaction with vasopressors and subsequent effects on CPO. This study investigates the CPO response to infusions of norepinephrine and phenylephrine in piglets during propofol–remifentanil and propofol–remifentanil–dexmedetomidine anaesthesia. Sixteen healthy female piglets (25–34 kg) were randomly allocated into a two-arm parallel group design with either normal blood pressure (NBP) or induced low blood pressure (LBP). Anaesthesia was induced with propofol without premedication and maintained with propofol–remifentanil TIVA, and finally supplemented with continuous infusion of dexmedetomidine. Norepinephrine and phenylephrine were infused in consecutive intervention periods before and after addition of dexmedetomidine. Cerebral perfusion measured by laser speckle contrast imaging was related to cerebral oxygenation as measured by an intracerebral Licox probe (partial pressure of oxygen) and transcranial near infrared spectroscopy technology (NIRS) (cerebral oxygen saturation).
Results
During propofol–remifentanil anaesthesia, increases in blood pressure by norepinephrine and phenylephrine did not change cerebral perfusion significantly, but cerebral partial pressure of oxygen (Licox) increased following vasopressors in both groups and increases following norepinephrine were significant (NBP: P = 0.04, LBP: P = 0.02). In contrast, cerebral oxygen saturation (NIRS) fell significantly in NBP following phenylephrine (P = 0.003), and following both norepinephrine (P = 0.02) and phenylephrine (P = 0.002) in LBP. Blood pressure increase by both norepinephrine and phenylephrine during propofol–remifentanil–dexmedetomidine anaesthesia was not followed by significant changes in cerebral perfusion. Licox measures increased significantly following both vasopressors in both groups, whereas the decreases in NIRS measures were only significant in the NBP group.
Conclusions
Cerebral partial pressure of oxygen measured by Licox increased significantly in concert with the vasopressor induced increases in blood pressure in healthy piglets with both normal and low blood pressure. Cerebral oxygenation assessed by intracerebral Licox and transcranial NIRS showed opposing results to vasopressor infusions.
Electronic supplementary material
The online version of this article (10.1186/s13028-018-0362-z) contains supplementary material, which is available to authorized users.
Keywords: Cerebral oxygenation, Cerebral perfusion, Dexmedetomidine, Laser speckle contrast imaging, Licox, NIRS, Norepinephrine, Phenylephrine, Propofol, Remifentanil, Vasopressor
Main text
Background
Vasopressors are frequently used to increase blood pressure in order to ensure sufficient cerebral perfusion and oxygenation (CPO) during hypotensive periods induced by e.g. anaesthesia or septic shock [1–4]. Two of the most commonly used vasopressors are norepinephrine and phenylephrine [5]. The quality of the response in cerebral blood flow (CBF) to vasopressor treatment has been shown to rely on the type of vasopressor used [3, 6, 7] and on the concurrent anaesthetic protocol [3].
Vasopressors have a well-documented systemic cardiovascular effect [8]. The primary benefit of vasopressors on CPO is believed to be due to the concomitant elevation of cerebral perfusion pressure following elevation of the systemic blood pressure [9]. However, if systemic pressure is kept within the limits of cerebral autoregulation, vasopressor treatment should have little effect on cerebral perfusion, despite an increase in blood pressure [9, 10]. Porcine cerebral arteries and veins have been reported to have dense sympathetic innervation and to be susceptible to vasopressor induced vasoconstriction in vitro [11]. Vasopressor-induced vasoconstriction has also been reported in vivo in healthy humans [12]. The sympathomimetic effect of norepinephrine is mediated by binding to both α-(α1) and β-(β1 and β2) adrenergic-receptors, whereas phenylephrine is a highly selective α1-agonist. The cerebral veins are more sensitive to sympathetic activation than cerebral arteries, and vasoconstriction are more specifically mediated by α2 rather than α1 adrenoceptors [11]. These differences may have contributed to the varying vasopressor effect on cerebral arteries versus veins observed in humans [12]. Despite the presence of α-adrenoceptors in the cerebral arteries, the vasoconstrictive effect of vasopressors on the cerebral arteries has been reported as clinically insignificant, since maximal stimulation has been shown to only reduce CBF by 5–10%, in healthy humans [10, 13].
General anaesthesia with propofol in combination with a potent opioid, such as remifentanil, has become increasingly popular [14] and the preferred total intravenous anaesthesia (TIVA) protocol in neuroanaesthesia and paediatric intensive care units [4, 15]. Propofol alone or in combination with remifentanil has been shown to preserve cerebral autoregulation in anaesthetic doses in both human [16–18] and animal studies [19, 20], and may thus be favourable in experimental studies requiring intact cerebral autoregulation. The α2-agonist, dexmedetomidine, has been receiving increasing attention as anaesthetic adjuvant in human anaesthesia and intensive care because of its abilities to preserve cerebral autoregulation and because of its near-ideal sedation. It has furthermore been recognized for facilitating better haemodynamic stability, analgesia and neuroprotection [15, 21–24]. In veterinary anaesthesia, α2-agonists have been widely used for many years as premedication, sedation and analgesia [25–27]. The hemodynamic effect of dexmedetomidine has shown to be both dose- and species dependent [28]. Dexmedetomidine has been shown to decrease systemic blood pressure in both humans and animals and to cause a generalized decrease in CBF [29–34]. This has not consistently been associated with decreased cerebral metabolic rate of oxygen [30, 31] and concern has been raised that dexmedetomidine may have the potential to cause cerebral vasoconstriction [23, 35].
The potential interactive vasoconstrictive effect of vasopressors and anaesthetics on the cerebral vasculature may be of concern in regard to CBF in hemodynamically compromised or neurocritical patients [36, 37]. The effect of vasopressors on CBF may be influenced by anaesthesia if cerebral autoregulation is preserved (intravenous anaesthesia) or impaired (inhalation anaesthesia) [3, 16–18], the latter making CBF more blood pressure-dependent with high gas concentrations [38], or when used with anaesthetics that might precondition cerebral vasoconstriction (α2-agonists) [39]. The systemic adrenoceptor-mediated properties of norepinephrine and phenylephrine produce different circulatory effects [40, 41]. Norepinephrine has been shown to improve myocardial function whereas phenylephrine decreases ventricular performance. In addition, norepinephrine appears to decrease microcirculatory blood flow to the abdominal organs, whereas phenylephrine does not [5]. Therefore, the choice of anaesthetic protocol in experimental animal studies should include consideration of such interactions to avoid adverse effects on CPO.
The objective of this study was to investigate the CPO response to vasopressor infusion with norepinephrine and phenylephrine during propofol–remifentanil and propofol–remifentanil–dexmedetomidine TIVA, in healthy piglets with normal and lowered blood pressure.
Methods
Study design and animals
Full study details and data regarding the entire study, and results regarding the effect of dexmedetomidine on CPO have been reported elsewhere [42] and are presented in Additional file 1. The same animals were used for the study of vasopressor effect on CPO in this study.
In summary: This study was designed as a non-blinded, randomized, two-arm parallel group, experimental animal trial (Fig. 1). Sixteen female slaughter piglets (Danish Landrace/Yorkshire/Duroc) with a body weight of 25–34 kg were used. In one group, low blood pressure (LBP) was induced using caval block [43, 44], whereas in the other group normal blood pressure (NBP) was maintained. All animals were subjected to the same anaesthetic protocol and did not receive premedication prior to induction on the day of the experiment.
Fig. 1.

Experimental design. The experimental design and flow for the two groups (NBP normal blood pressure group, LBP low blood pressure group). Key time points are marked with arrows and vertical bars. Solid vertical bars show pre- or post-intervention baselines, where the red arrows indicate supplemental blood gas readings. Open vertical bars show vasopressor challenges. Yellow horizontal bar indicates period with propofol–remifentanil TIVA, green horizontal bar indicates period with propofol–remifentanil–dexmedetomidine, and blue horizontal bar indicates period with induced hypotension. PCB pre-caval block, PR-1 baseline during propofol–remifentanil, NE-1 norepinephrine during propofol–remifentanil, PR-intvas after norepinephrine and wash-out period during propofol–remifentanil, PE-1 phenylephrine during propofol–remifentanil, PR-2 after phenylephrine wash-out period/pre-dexmedetomidine during propofol–remifentanil, PRD propofol–remifentanil–dexmedetomidine, NE-2 norepinephrine during propofol–remifentanil, PRD-intvas after norepinephrine and wash-out period during propofol–remifentanil–dexmedetomidine, PE-2 phenylephrine during propofol–remifentanil–dexmedetomidine, PRD-end after phenylephrine and wash-out period during propofol–remifentanil–dexmedetomidine (end of experiment)
Anaesthesia
General anaesthesia was induced while the animals were still in their pen to minimise stress. A dosage of 4–8 mg/kg propofol was given through a catheter placed in an auricular vein the day before the experiment. After endotracheal intubation, the animals were connected to a mechanical ventilator. End tidal CO2 (EtCO2) was maintained between 35 and 50 mmHg. Fraction of inspired oxygen (FiO2) was maintained around 0.8, and was centrally supplied by an in-house generator.
General anaesthesia was maintained using a TIVA protocol with separate syringe pumps (Terumo, Terufusion Syringe Pump TE-331, Belgium) for propofol (12–20 mg/kg/h) and remifentanil (20–45 µg/kg/h) TIVA. Doses were individually regulated to accomplish unresponsiveness to noxious stimuli (dewclaw pinching), with propofol doses adjusted to control anaesthetic depth (assessed as lack of movement) and remifentanil doses adjusted to eliminate responses to noxious stimuli. Once animal preparation was completed, anaesthetic doses were kept unchanged. Dexmedetomidine was supplemented after the first half of the experiment (Fig. 1) with a bolus of 1 µg/kg given over 10 min followed by a fixed dose of 0.7 µg/kg/h iv.
Surgical preparation and instrumentation
All invasive procedures were conducted after infiltration with a mixture of lidocaine and bupivacaine. After surgical cut down, the femoral artery was cannulated for invasive blood pressure monitoring and intermittent blood collection for blood gas analysis. An eight French balloon-tipped catheter was placed in the femoral vein in all animals, with the balloon positioned in the caudal vena cava just below the heart. A urinary catheter with a closed collecting bag was placed to prevent bladder distension. Isotonic glucose solution was administered throughout the experiment at 2.5 mL/kg/h. A multiparametric bedside monitor recorded haemodynamic and respiratory variables every 30 s, and data were transferred to a personal computer using Datex-Ohmeda S/5™ Collect software (GE Healthcare, Helsinki, Finland). The collected variables were pulse rate, and mean arterial blood pressure (MAP), body temperature (oesophageal probe), fractionated inspired oxygen (FiO2), and EtCO2 (Additional file 1). Electrocardiogram and peripheral oxygen saturation by pulse oximetry (SpO2) measured on the tail or the lower lip were monitored for continuous assessment.
Cerebral perfusion and oxygenation (CPO) measures
A circular craniotomy (20–30 mm) was performed over the right parietal lobe with a 5 mm craniotome, and dura was removed. A laser speckle contrast imaging (LSCI) camera (MoorFLPI-2, Moor Instruments, Devon, UK) was used to measure cerebral perfusion semi quantitatively in laser speckle perfusion units (LSPU). The position of the head of the animal remained unchanged throughout the experiment and the focus distance was 25 cm. Cerebral partial pressure of oxygen (PbrO2) was measured by an intracerebral Clark-type probe (Licox, Integra LifeSciences, New Jersey, USA) which was placed 25 mm subdurally into the white matter and secured to the craniotomy edge with bone wax. Non-invasive measurement of cerebral oxygen saturation (SbrO2) was obtained by near infrared spectroscopy (NIRS) (Invos 5100, Covidien/Medtronic, Minneapolis, USA). A sensor was attached to the skin of the forehead on the left side of the animal, on the contralateral side to the Licox probe and the LSCI camera, and isolated from external light.
Experimental protocol
After instrumentation the Licox probe was equilibrated for a period of 2 h or until PbrO2 > 25 mmHg, and followed by baseline data collection (PR-1–NBP and PCB–LBP) for all animals (Fig. 1). The blood pressure was lowered by caval block in the LBP group (by inflation of the balloon catheter in the vena cava) until a stable MAP of 50–60 mmHg was achieved, and an additional baseline was recorded in this group (PR-1–LBP). The caval block was maintained throughout the experiment for the LBP group, and was not subjected to further adjustments.
Vasopressor intervention followed the same sequence (norepinephrine followed by phenylephrine) in both groups and was repeated after initiation of dexmedetomidine infusion. Baseline recordings were obtained before and after each intervention or washout period (Fig. 1). The standard 30 min washout periods were conservatively chosen to allow the blood pressure and the CPO measures to return to baseline values between vasopressor interventions, and were chosen based on the longest reported clinical effect time of 15 min for phenylephrine [45]. Norepinephrine (1 mg/mL Noradrenalin “SAD”, Amgros I/S, Copenhagen, Denmark) was administered by bolus (100 µg) and followed by infusion of (0.6–2.0 µg/kg/min) to a target effect of either MAP 130–140 mmHg or 100% increase in MAP (primarily for the LBP group) from the baseline. Similarly, phenylephrine (1 mg/mL Metaoxedrin “SAD”, Amgros I/S, Copenhagen, Denmark) was administered by bolus (200 µg) and followed by infusion of 5.0–13.5 µg/kg/min to a target effect of either MAP 130–140 mmHg or 100% increase (primarily for the LBP group) in MAP from the baseline. During the experiment, arterial blood samples were collected at PCB, PR-1, PR-2, PRD and PRD-end for blood gas and acid–base evaluation (Fig. 1 and Additional file 1). All animals were euthanized with pentobarbital IV at the end of the experiment.
Statistics
Statistical analysis was performed using SPSS 24.0 software (IBM® SPSS® Statistics for Mac, IBM Corp. ©, Armonk, NY, USA), and Microsoft® Excel® for Mac 2011 version 14.3.9 (2010 Microsoft Corporation). Non-parametric statistical tests were used, since normal distribution of data could not be assumed due to the small sample size. Data were reported as medians and range (min–max), and differences between groups were analysed by the independent-samples median test. Median changes for all outcome variables were reported with 95% confidence intervals (95% CI) using Hodges-Lehmann estimates where appropriate. Primary (Licox, NIRS and LSCI) and secondary (MAP, pulse rate and EtCO2) outcome variables at time points PR-1, NE-1, PR-intvas, PE-1, PRD, NE-2, PRD-intvas and PE-2 were compared using Friedman’s ANOVA with post hoc pairwise comparisons. Significance levels for the four comparisons of interest (before vasopressor and during vasopressor administration) were controlled using Holm–Bonferroni’s correction before reporting. Significance was set at the 5% level.
A sample size of 16 animals, divided into two groups of 8, was calculated using conservative estimates based on earlier studies [46] with expected power of 80% in detecting a minimum of 30% difference in MAP with a two-tailed significance level of 5% after supplementation of dexmedetomidine.
Results
All 16 animals completed the experimental protocol. Data from three (NBP group n = 2, LBP group n = 1) piglets were excluded from analysis. One piglet developed signs of brain oedema with a severe reduction in CPO following craniotomy (LBP group). In the NBP group, one piglet had persistently and unexplainably high pulse rate, EtCO2, PaCO2 and a low pH, which were expected to produce an atypical CPO response. The other piglet was excluded due to technical difficulties.
The remaining 13 piglets reached the target MAP with vasopressor administration of > 130 mmHg or a 100% increase over pre-treatment MAP. The animals of the two groups revealed no significant demographic differences, nor were any significant differences revealed in anaesthesia time, preparation time, anaesthetic doses, baseline PbrO2 or LSPU measurements after equilibration [42]. Additionally, there was found no significant difference between the two groups in SbrO2 measured by NIRS (P = 0.59), which were 65% (range 59–72) in the LBP group and 62% (range 51–70) in the NBP group at PCB and PR-1 respectively. Both groups reached normal PbrO2 and SbrO2 levels [47, 48] after equilibration.
Vasopressor effects under propofol–remifentanil anaesthesia
Norepinephrine administration significantly increased MAP in both groups [LBP: P = 0.002, median increase 61 mmHg (95% CI 47; 71), NBP: P = 0.009, median increase 51 mmHg (95% CI 39; 66)]. Following washout MAP was not significantly different to pre-treatment levels in either group (P = 1) with median differences of 1 mmHg (95% CI − 8; 11) for LBP and 7 mmHg (95% CI − 6; 17) for NBP.
Phenylephrine administration significantly (P = 0.03) increased MAP in the LBP group [median increase 47 mmHg (95% CI 32; 66)] but not in the NBP group [P = 0.13, median increase 33 mmHg (95% CI 14; 55)] (Fig. 2a).
Fig. 2.
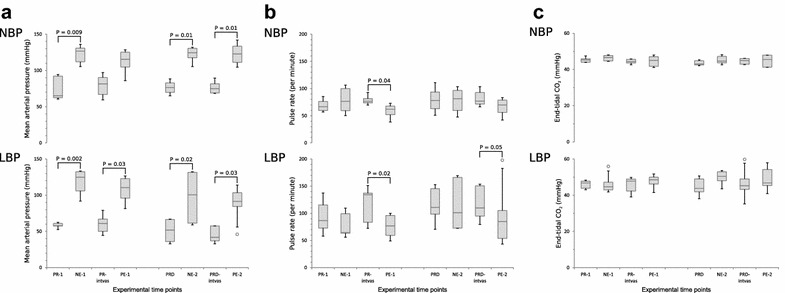
Boxplots of haemodynamic data at baselines and vasopressor interventions. Absolute data presented as boxplots with median and interquartile range. Open circles indicate outliers. All comparisons with significant changes between interventions and the immediate pre-intervention baselines are marked with horizontal solid lines and exact P values are noted. a mean arterial pressure (MAP), b pulse rate, c end-tidal carbon dioxide (EtCO2). For all variables, the results of the normal blood pressure (NBP) are presented on the top chart and results from low blood pressure (LBP) group are presented at the bottom chart. The x-axis represents the experimental time-points, and the y-axis shows the names and units of the individual variables. NE-1/PE-1 norepinephrine/phenylephrine infusion during propofol–remifentanil, NE-2/PE-2 norepinephrine/phenylephrine infusion during propofol–remifentanil–dexmedetomidine, PCB pre-caval block (only LBP), PR-1 baseline before interventions (after caval block in LBP), PR-intvas after NE-1 and 30-min washout, PR-2 after PE-1 and 30-min washout, PRD baseline after infusion start of dexmedetomidine, PRD-intvas after NE-2 and 30-min washout, PRD-end after PE-2 and 30-min washout
Pulse rate decreased significantly in both groups following phenylephrine (LBP: P = 0.02, NBP: P = 0.04) but not norepinephrine (LBP: P = 0.4, NBP: P = 0.6) (Fig. 2b).
Cerebral partial pressure of oxygen (PbrO2) increased significantly following norepinephrine (P = 0.02) but not phenylephrine (P = 0.06) in the LBP group (median increases 14 mmHg (95% CI 6; 26) and 11 mmHg (95% CI 2; 23), respectively). A similar response was observed in the NBP group with a significant increase following norepinephrine [P = 0.04, median increase 17 mmHg (95% CI 5; 33)] but not phenylephrine [P = 0.2, median increase 8 mmHg (95% CI 2; 26)] (Fig. 3a).
Fig. 3.

Boxplots of CPO data at baselines and vasopressor interventions. Absolute data presented as boxplots with median and interquartile range. Open circles indicate outliers. All comparisons with significant changes between interventions and the immediate pre-intervention baselines are marked with horizontal solid lines and exact p-values are noted. a Licox, b near infrared spectroscopy (NIRS), c laser speckle contrast imaging (LSCI). For all variables, the results of the normal blood pressure (NBP) are presented on the top chart and results from low blood pressure (LBP) group are presented at the bottom chart. The x-axis represents the experimental time-points, and the y-axis shows the names and units of the individual variables. NE-1/PE-1 Norepinephrine/phenylephrine infusion during propofol–remifentanil, NE-2/PE-2 Norepinephrine/phenylephrine infusion during propofol–remifentanil–dexmedetomidine, PCB pre-caval block (only LBP), PR-1 baseline before interventions (after caval block in LBP), PR-intvas after NE-1 and 30-min washout, PR-2 after PE-1 and 30-min washout, PRD baseline after infusion start of dexmedetomidine, PRD-intvas after NE-2 and 30-min washout, PRD-end after PE-2 and 30-min washout
In contrast, cerebral oxygen saturation (SbrO2) fell significantly in the LBP group following both norepinephrine and phenylephrine [P = 0.02, median decrease − 11% (95% CI − 20; − 3) and P = 0.002, median decrease − 15% (95% CI − 23; − 7), respectively] and in the NBP group SbrO2 fell significantly following phenylephrine [P = 0.003, median decrease − 24% (95% CI − 31; − 22)] but not norepinephrine [P = 0.2, median decrease − 10% (95% CI − 16; − 6)] (Fig. 3b). LSCI measurements (LSPU) did not exhibit a clear trend to increase or decrease, and no significant changes were observed following vasopressor administration (Fig. 3c).
While EtCO2 readings showed increased variability in the LBP group compared to the NBP group, neither group’s EtCO2 readings responded significantly to vasopressor treatment (Fig. 2c).
Vasopressor effects under propofol–remifentanil–dexmedetomidine anaesthesia
Norepinephrine administration significantly increased MAP in both groups [LBP: P = 0.02, median increase 46 mmHg (95% CI 17; 81), NBP: P = 0.01, median increase 48 mmHg (95% CI 33; 57)]. Following washout MAP was not significantly different to pre-treatment levels in either group (P = 1.0) with median differences of − 6 mmHg (95% CI − 12; 3) for LBP and − 1 mmHg (95% CI − 5; 4) for NBP.
Phenylephrine administration significantly increased MAP in both groups [LBP: P = 0.03, median increase 44 mmHg (95% CI 20; 66), NBP: P = 0.01, median increase 48 mmHg (95% CI 34; 62)] (Fig. 2a).
Pulse rate did not alter significantly in either group with either vasopressor in the NBP group, but fell significantly following phenylephrine in the LBP group [P = 0.05, median decrease − 25 (95% CI − 66; 34)] (Fig. 2b).
Cerebral partial pressure of oxygen (PbrO2) increased significantly in the LBP group following both norepinephrine and phenylephrine [P = 0.001, median increase 18 mmHg (95% CI 11; 28) and P = 0.003, median increase 16 mmHg (95% CI 7; 42)]. In the NBP group, a similar response was seen with significant increases seen following norepinephrine [P = 0.02, median increase 13 mmHg (95% CI 6; 23)] and phenylephrine [P = 0.03, median increase 10 mmHg (95% CI − 2; 16)] (Fig. 3a).
Cerebral oxygen saturation (SbrO2) did not fall significantly in the LBP group following either norepinephrine [P = 0.08, median decrease − 7% (95% CI − 20; 1)] or phenylephrine [P = 0.14, median decrease − 7% (95% CI − 17; − 1)]. In contrast, the NBP group experienced significant decreases following both norepinephrine [P = 0.01, median decrease − 21% (95% CI − 26; − 18)] and phenylephrine [P < 0.001, median decrease − 33% (95% CI − 37; − 30)] (Fig. 3b). As for the NBP group, LSCI did not measure any significant changes in cerebral perfusion (LSPU) following vasopressor administration (Fig. 3c).
The LBP group continued to exhibit increased variability in EtCO2 readings compared to the NBP group, but no significant changes were observed due to vasopressor administration (Fig. 2c).
Discussion
Cerebral partial pressure of oxygen (PbrO2) was found to increase during vasopressor challenges when assessed by Licox, while cerebral oxygen saturation (SbrO2) decreased when assessed by NIRS. Cerebral perfusion (LSPU) was not found to change significantly in concert with the vasopressor induced increases in MAP. This pattern of findings was similar in both groups and during both TIVA protocols (Fig. 3c), suggesting that the cerebral autoregulation did remain intact throughout the experiment. This is consistent with the findings of Bruins et al. [3] indicating preserved cerebral autoregulation during TIVA (midazolam and fentanyl), in contrast to inhalation anaesthesia (isoflurane-based) where autoregulation was impaired.
The increase in PbrO2 during norepinephrine or phenylephrine has been previously reported in pigs with both uninjured brains [49] and traumatic brain injury [7]. In the present study, the significant increase in PbrO2 during vasopressor infusion was not accompanied by a concurrent increase in perfusion, suggesting that changes in PbrO2 do not simply reflect changes in CBF [50]. Decreasing SbrO2 with increasing PbrO2 was observed during vasopressor infusions, in both the propofol–remifentanil and propofol–remifentanil–dexmedetomidine TIVA groups (Fig. 3a, b). These results are consistent with findings in human NIRS studies, where a decrease in SbrO2 in response to blood pressure elevation by norepinephrine [51] or phenylephrine [6, 12, 52, 53] has been reported. Human studies of NIRS have also reported increase in SbrO2 after nitroprusside induced blood pressure decrease and decrease in SbrO2 in response to vasopressor induced increase in blood pressure [54, 55]. Some authors speculated that this response in cerebral oxygen saturation was part of a normal cerebral autoregulatory response [54], while others have questioned the validity of NIRS technology and suggested that it primarily reflects skin perfusion rather than cerebral oxygenation [12, 37, 56–59]. Cerebral oxygen saturation values (SbrO2) and cerebral partial pressure of oxygen values (PbrO2) are not directly comparable in absolute values, since NIRS reflects levels of oxygen-saturated haemoglobin in the venous, capillary and arterial blood [60] and Licox has been described as a measure of “the pool of oxygen” that accumulates in the brain tissue and thus reflects the balance between oxygen delivery, diffusion and consumption [50, 61, 62]. The distribution ratio of arteries versus veins in the cerebral cortex is approximately 30:70, and NIRS therefore predominantly reflects the cerebral venous oxygen reserve [60, 63]. Transcranial assessment of the cerebral oxygen saturation in piglets will furthermore depend on factors like skull thickness and pneumatisation of the frontal sinus, since NIRS has limited penetration. Due to the size and age of the animals used in this study, the pneumatisation of the large frontal sinus, which starts at approximately 3–4 months of age in domestic swine [64], was not expected to affect the results. NIRS purportedly reflects SbrO2 in the grey matter of the cerebral cortex, whereas Licox measures PbrO2 in the less metabolically active white matter of the CNS, areas with different metabolic activity and blood flow [9, 65, 66].
The differences in cerebral oxygenation assessment by Licox and NIRS could indicate that vasopressor treatment affects the cortex and the white matter differently. Whether this is a normal response attributable to a preserved cerebral autoregulation [54] or related to limitations of the methods used remains unanswered. Since cutaneous vessels predominantly have α-adrenergic innervation, treatment with vasopressors having high affinity for α-adrenergic receptors (such as norepinephrine and phenylephrine), results in vasoconstriction [67] and decreases in skin blood flow. Thus, decreases in cerebral oxygen saturation values during vasopressor infusion could therefore be a reflection of extra-cranial rather than cerebral oxygen saturation.
In summary, the CPO response to vasopressor challenge in piglets was found to be qualitatively similar for the two TIVA protocols used, and the concern regarding the potential additive vasoconstrictive effect of dexmedetomidine during vasopressor infusions could not be confirmed in this study.
Strengths and limitations
The current study was strengthened by omission of premedication on the day of experiment, by avoiding a possible vasoactive effect of premedication on CPO, and by using animals of the same sex and with a narrow age span since both age and gender may influences CBF in porcine models [68–70]. The results from this animal study best translates into children with neurodevelopmental maturity of approximately 10 months of age [71, 72] and translation to other age groups should be made with caution [69, 73].
We compared regional with focal CPO measures and at contralateral brain sites in animals undergoing craniotomy, which limits derived conclusions regarding global CPO status and regarding CPO in animals not undergoing craniotomy. Another potential limitation was the possibility that the initial norepinephrine infusion could have affected the physiological and cerebral response to the subsequent phenylephrine infusions. However, the vasopressors were given in the same sequence in all the animals, and any potential preconditioning was therefore expected to be similar in the entire group of animals. The supra clinical target increases in blood pressure and infusion doses of norepinephrine and phenylephrine in this study, were set to ensure an effect on CPO, if present, while retaining the animals within the expected blood pressure range for intact cerebral autoregulation. The doses though, were comparable to doses used in other animal studies [7, 74]. This intensive approach to elevate blood pressure and subsequently CPO, when compared to having used more moderate targets and vasopressor doses, may have increased the risk for type I errors. Furthermore, the design of the study was set up to illustrate haemodynamic influences in the normal as well as in hemodynamically compromised patients without initial brain pathologies. Extrapolation to situations with concurrent brain pathology should be made with caution since neurophysiology and cerebral autoregulation may be different. The animals were subjected to prolonged anaesthesia, which for some animals lasted up to 10–11 h, and a mild to moderate hypercapnia was observed in all animals throughout the experiment [42] (Additional file 1). The resulting respiratory acidosis would make the autoregulatory plateau narrower, and thereby the cerebral perfusion more sensitive to changes in blood pressure. This was however not evident from the results of the current study, since no significant variations in cerebral perfusion could be detected. The increased levels of PaCO2 (represented by EtCO2 in this study) might however have increased the variability of the perfusion data, which would make the non-significant findings expected. In general, PbrO2 showed greater variability and a tendency to increase in the NBP group than in the LBP group, especially after addition of dexmedetomidine. Finally, the supplemented inspiratory oxygen levels were also relatively high in this study, with a FiO2 of 0.8 for all animals (Additional file 1). The FiO2 did not differ throughout the experiment, and is therefore not expected to influence the relative changes in PbrO2 of this study. It cannot be excluded that the CPO response to changes in MAP observed in this study could be different at lower FiO2.
Non-significant P values following Holm-Bonferroni correction were noted for several parameters despite their confidence intervals for the change in medians not including zero. The small sample size and large variability for some parameters (PbrO2, LSPU, pulse rate) increased the risk of type II error. Confidence intervals were therefore reported for both significant and non-significant changes, permitting a more nuanced interpretation.
Conclusions
Cerebral partial pressure of oxygen measured by Licox increased significantly in concert with the vasopressor induced increases in blood pressure in healthy piglets with both normal and low blood pressure. Cerebral oxygenation assessed by intracerebral Licox and transcranial NIRS showed opposing results to vasopressor infusions. The CPO responses, induced by norepinephrine and phenylephrine, were shown to be qualitatively similar during both propofol–remifentanil and propofol–remifentanil–dexmedetomidine TIVA.
Additional file
Additional file 1. Table of experimental data: Cerebral perfusion and oxygenation readings, physiological and haemodynamic data, blood gas data, and anaesthesia time at all time points throughout the experiment. PCB: Pre-Caval block; PR-1: baseline during propofol-remifentanil; NE-1: Norepinephrine during propofol-remifentanil; PR-intvas: after norepinephrine and wash-out period during propofol-remifentanil; PE-1: Phenylephrine during propofol-remifentanil; PR-2: after phenylephrine wash-out period/pre-dexmedetomidine during Propofol-remifentanil; PRD: Propofol-remifentanil-dexmedetomidine; NE-2: Norepinephrine during propofol-remifentanil; PRD-intvas: after norepinephrine and wash-out period during propofol-remifentanil-dexmedetomidine; PE-2: Phenylephrine during propofol-remifentanil-dexmedetomidine; PRD-end: after phenylephrine and wash-out period during propofol-remifentanil-dexmedetomidine (end of experiment); NIRS: Near infra red spectroscopy; LSCI: Laser speckle contrast imaging; MAP: mean arterial pressure; EtCO2: End-tidal carbon dioxide; FiO2: Fraction of inspired oxygen; (T): data corrected for body temperature; PaCO2: Partial pressure of arterial carbon dioxide; PaO2: Partial pressure of arterial oxygen; HCO3: Hydrogen bicarbonate; Hct: Haematocrit; THbc: Total haemoglobin concentration.
Authors’ contributions
MLGM, TE, HHP and FBM conceived the overall objective, study design and experimental protocol for this study. MLGM was the primary license holder and responsible for the ethical approvals and the overall experimental execution. MLGM, TE and RA were present at all experiments. TE performed all surgeries and RA performed all laser speckle contrast imaging. Data analysis and statistical revision was done in collaboration with FBM, JEM and RA. HHP supervised anaesthesia and RR contributed with substantial intellectual guidance and interpretations of data, as well as critical revision of the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was approved by The Danish Animal Experiments Inspectorate (no. 2013-15-2934-00909) and performed in accordance with National legislation and The Council of Europe Convention ETS 123.
Funding
This study was funded by a PhD scholarship granted by the University of Copenhagen.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- CBF
cerebral blood flow
- CPO
cerebral perfusion and oxygenation
- CPP
cerebral perfusion pressure
- EtCO2
end-tidal carbon dioxide
- FiO2
fractionated inspired oxygen
- LBP
low blood pressure group
- LSCI
laser speckle contrast imaging
- LSPU
laser speckle perfusion unit
- Max
maximum
- Min
minimum
- MAP
mean arterial pressure
- NBP
normal blood pressure group
- PaCO2
arterial partial pressure of carbon dioxide
- PaO2
arterial partial pressure of oxygen
- PbrO2
cerebral oxygenation (partial pressure of oxygen in brain tissue)
- PCB
pre-caval block (time point)
- PR-n
propofol/remifentanil TIVA (n: time-point number)
- PRD
propofol/remifentanil TIVA + dexmedetomidine CRI (time point)
- SbrO2
cerebral oxygen saturation
- SpO2
peripheral oxygen saturation by pulse oximetry
- TIVA
total intravenous anaesthesia
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s13028-018-0362-z) contains supplementary material, which is available to authorized users.
Contributor Information
Mai Louise Grandsgaard Mikkelsen, Email: mailo@sund.ku.dk.
Rikard Ambrus, Email: riam@dadlnet.dk.
Rune Rasmussen, Email: rune333@gmail.com.
James Edward Miles, Email: jami@sund.ku.dk.
Helle Harding Poulsen, Email: hhp@sund.ku.dk.
Finn Borgbjerg Moltke, Email: finn.borgbjerg.moltke.01@regionh.dk.
Thomas Eriksen, Email: ter@sund.ku.dk.
References
- 1.Dagal A, Lam AM. General considerations in neuroanaesthesia. In: Matta BF, Menon DK, Smith M, editors. Core topics in neuroanaesthesia and neurointensive care. Cambridge: Cambridge University Press; 2011. pp. 147–161. [Google Scholar]
- 2.Breslow MJ, Miller CF, Parker SD, Walman AT, Traystman RJ. Effect of vasopressors on organ blood flow during endotoxin shock in pigs. Am J Physiol. 1987;252:H291–H300. doi: 10.1152/ajpheart.1987.252.2.H291. [DOI] [PubMed] [Google Scholar]
- 3.Bruins B, Kilbaugh TJ, Margulies SS, Friess SH. The anesthetic effects on vasopressor modulation of cerebral blood flow in an immature swine model. Anesth Analg. 2013;116:838–844. doi: 10.1213/ANE.0b013e3182860fe7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cole CD, Gottfried ON, Gupta DK, Couldwell WT. Total intravenous anesthesia: advantages for intracranial surgery. Neurosurgery. 2007;61:369–378. doi: 10.1227/01.NEU.0000290900.23190.C9. [DOI] [PubMed] [Google Scholar]
- 5.Poterman M, Vos JJ, Vereecke HE, Struys MM, Vanoverschelde H, Scheeren TW, et al. Differential effects of phenylephrine and norepinephrine on peripheral tissue oxygenation during general anaesthesia: a randomised controlled trial. Eur J Anaesthesiol. 2015;32:571–580. doi: 10.1097/EJA.0000000000000247. [DOI] [PubMed] [Google Scholar]
- 6.Nissen P, Brassard P, Jorgensen TB, Secher NH. Phenylephrine but not ephedrine reduces frontal lobe oxygenation following anesthesia-induced hypotension. Neurocrit Care. 2010;12:17–23. doi: 10.1007/s12028-009-9313-x. [DOI] [PubMed] [Google Scholar]
- 7.Friess SH, Bruins B, Kilbaugh TJ, Smith C, Margulies SS. Differing effects when using phenylephrine and norepinephrine to augment cerebral blood flow after traumatic brain injury in the immature brain. J Neurotrauma. 2015;32:237–243. doi: 10.1089/neu.2014.3468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Overgaard CB, Dzavik V. Inotropes and vasopressors: review of physiology and clinical use in cardiovascular disease. Circulation. 2008;118:1047–1056. doi: 10.1161/CIRCULATIONAHA.107.728840. [DOI] [PubMed] [Google Scholar]
- 9.Miller RD. Miller’s anesthesia. 7. Philadelphia: Churchill Livingstone/Elsevier; 2010. [Google Scholar]
- 10.Messick JM, Jr, Newberg LA, Nugent M, Faust RJ. Principles of neuroanesthesia for the nonneurosurgical patient with CNS pathophysiology. Anesth Analg. 1985;64:143–174. doi: 10.1213/00000539-198502000-00008. [DOI] [PubMed] [Google Scholar]
- 11.Asada Y, Lee TJ. Alpha 2-adrenoceptors mediate norepinephrine constriction of porcine pial veins. Am J Physiol. 1992;263:H1907–H1910. doi: 10.1152/ajpheart.1992.263.6.H1907. [DOI] [PubMed] [Google Scholar]
- 12.Ogoh S, Sato K, Fisher JP, Seifert T, Overgaard M, Secher NH. The effect of phenylephrine on arterial and venous cerebral blood flow in healthy subjects. Clin Physiol Funct Imaging. 2011;31:445–451. doi: 10.1111/j.1475-097X.2011.01040.x. [DOI] [PubMed] [Google Scholar]
- 13.Keong NC, Macfarlane R. Anatomical considerations in neuroanaesthesia. In: Matta BF, Menon DK, Smith M, editors. Core topics in neuroanaesthesia and neurointensive care. Cambridge: Cambridge University Press; 2011. pp. 1–16. [Google Scholar]
- 14.Eikaas H, Raeder J. Total intravenous anaesthesia techniques for ambulatory surgery. Curr Opin Anaesthesiol. 2009;22:725–729. doi: 10.1097/ACO.0b013e3283310f6b. [DOI] [PubMed] [Google Scholar]
- 15.Lauder GR. Total intravenous anesthesia will supercede inhalational anesthesia in pediatric anesthetic practice. Paediatr Anaesth. 2015;25:52–64. doi: 10.1111/pan.12553. [DOI] [PubMed] [Google Scholar]
- 16.Strebel S, Lam AM, Matta B, Mayberg TS, Aaslid R, Newell DW. Dynamic and static cerebral autoregulation during isoflurane, desflurane, and propofol anesthesia. Anesthesiology. 1995;83:66–76. doi: 10.1097/00000542-199507000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Conti A, Iacopino DG, Fodale V, Micalizzi S, Penna O, Santamaria LB. Cerebral haemodynamic changes during propofol–remifentanil or sevoflurane anaesthesia: transcranial Doppler study under bispectral index monitoring. Br J Anaesth. 2006;97:333–339. doi: 10.1093/bja/ael169. [DOI] [PubMed] [Google Scholar]
- 18.Dagal A, Lam AM. Cerebral autoregulation and anesthesia. Curr Opin Anaesthesiol. 2009;22:547–552. doi: 10.1097/ACO.0b013e32833020be. [DOI] [PubMed] [Google Scholar]
- 19.Lagerkranser M, Stange K, Sollevi A. Effects of propofol on cerebral blood flow, metabolism, and cerebral autoregulation in the anesthetized pig. J Neurosurg Anesthesiol. 1997;9:188–193. doi: 10.1097/00008506-199704000-00015. [DOI] [PubMed] [Google Scholar]
- 20.Silva A, Venancio C, Ortiz AL, Souza AP, Amorim P, Ferreira DA. The effect of high doses of remifentanil in brain near-infrared spectroscopy and in electroencephalographic parameters in pigs. Vet Anaesth Analg. 2014;41:153–162. doi: 10.1111/vaa.12091. [DOI] [PubMed] [Google Scholar]
- 21.Mahmoud M, Mason KP. Dexmedetomidine: review, update, and future considerations of paediatric perioperative and periprocedural applications and limitations. Br J Anaesth. 2015;115:171–182. doi: 10.1093/bja/aev226. [DOI] [PubMed] [Google Scholar]
- 22.Peng K, Wu S, Liu H, Ji F. Dexmedetomidine as an anesthetic adjuvant for intracranial procedures: meta-analysis of randomized controlled trials. J Clin Neurosci. 2014;21:1951–1958. doi: 10.1016/j.jocn.2014.02.023. [DOI] [PubMed] [Google Scholar]
- 23.Farag E, Argalious M, Sessler DI, Kurz A, Ebrahim ZY, Schubert A. Use of alpha(2)-agonists in neuroanesthesia: an overview. Ochsner J. 2011;11:57–69. [PMC free article] [PubMed] [Google Scholar]
- 24.Bekker A, Sturaitis MK. Dexmedetomidine for neurological surgery. Neurosurgery. 2005;57(suppl_1):1–10. doi: 10.1227/01.neu.0000163476.42034.a1. [DOI] [PubMed] [Google Scholar]
- 25.Flaherty D. Alpha(2)-adrenoceptor agonists in small animal practice 2. Optimising clinical use. Practice. 2013;35:565–573. doi: 10.1136/inp.f6613. [DOI] [Google Scholar]
- 26.Uilenreef JJ, Murrell JC, McKusick BC, Hellebrekers LJ. Dexmedetomidine continuous rate infusion during isoflurane anaesthesia in canine surgical patients. Vet Anaesth Analg. 2008;35:1–12. doi: 10.1111/j.1467-2995.2007.00344.x. [DOI] [PubMed] [Google Scholar]
- 27.Flaherty D. Alpha(2)-adrenoceptor agonists in small animal practice 1. Why they do what they do. Practice. 2013;35:513–517. [Google Scholar]
- 28.Murrell JC, Hellebreckers LJ. Medetomidine and dexmedetomidine: a review of cardiovascular effects and antinocicptive properties in the dog. Vet Anaesth Anal. 2005;32:117–127. doi: 10.1111/j.1467-2995.2005.00233.x. [DOI] [PubMed] [Google Scholar]
- 29.Zornow MH, Maze M, Dyck JB, Shafer SL. Dexmedetomidine decreases cerebral blood flow velocity in humans. J Cereb Blood Flow Metab. 1993;13:350–353. doi: 10.1038/jcbfm.1993.45. [DOI] [PubMed] [Google Scholar]
- 30.Zornow MH, Fleischer JE, Scheller MS, Nakakimura K, Drummond JC. Dexmedetomidine, an alpha 2-adrenergic agonist, decreases cerebral blood flow in the isoflurane-anesthetized dog. Anesth Analg. 1990;70:624–630. doi: 10.1213/00000539-199006000-00008. [DOI] [PubMed] [Google Scholar]
- 31.Karlsson BR, Forsman M, Roald OK, Heier MS, Steen PA. Effect of dexmedetomidine, a selective and potent alpha 2-agonist, on cerebral blood flow and oxygen consumption during halothane anesthesia in dogs. Anesth Analg. 1990;71:125–129. doi: 10.1213/00000539-199008000-00003. [DOI] [PubMed] [Google Scholar]
- 32.Rozet I. Anesthesia for functional neurosurgery: the role of dexmedetomidine. Curr Opin Anaesthesiol. 2008;21:537–543. doi: 10.1097/ACO.0b013e32830edafd. [DOI] [PubMed] [Google Scholar]
- 33.Drummond JC, Dao AV, Roth DM, Cheng CR, Atwater BI, Minokadeh A, et al. Effect of dexmedetomidine on cerebral blood flow velocity, cerebral metabolic rate, and carbon dioxide response in normal humans. Anesthesiology. 2008;108:225–232. doi: 10.1097/01.anes.0000299576.00302.4c. [DOI] [PubMed] [Google Scholar]
- 34.Prielipp RC, Wall MH, Tobin JR, Groban L, Cannon MA, Fahey FH, et al. Dexmedetomidine-induced sedation in volunteers decreases regional and global cerebral blood flow. Anesth Analg. 2002;95:1052–1059. doi: 10.1097/00000539-200210000-00048. [DOI] [PubMed] [Google Scholar]
- 35.Tsaousi GG, Lamperti M, Bilotta F. Role of dexmedetomidine for sedation in neurocritical care patients: a qualitative systematic review and meta-analysis of current evidence. Clin Neuropharmacol. 2016;39:144–151. doi: 10.1097/WNF.0000000000000151. [DOI] [PubMed] [Google Scholar]
- 36.Kroppenstedt SN, Sakowitz OW, Thomale UW, Unterberg AW, Stover JF. Norepinephrine is superior to dopamine in increasing cortical perfusion following controlled cortical impact injury in rats. Acta Neurochir Suppl. 2002;81(225–7):37. doi: 10.1007/978-3-7091-6738-0_58. [DOI] [PubMed] [Google Scholar]
- 37.Hahn GH, Hyttel-Sorensen S, Petersen SM, Pryds O, Greisen G. Cerebral effects of commonly used vasopressor-inotropes: a study in newborn piglets. PLoS ONE. 2013;8(e63069):1–7. doi: 10.1371/journal.pone.0063069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Engelhard K, Werner C. Inhalational or intravenous anesthetics for craniotomies? Pro inhalational. Curr Opin Anaesthesiol. 2006;19:504–508. doi: 10.1097/01.aco.0000245275.76916.87. [DOI] [PubMed] [Google Scholar]
- 39.Asano Y, Koehler RC, Kawaguchi T, McPherson RW. Pial arteriolar constriction to alpha 2-adrenergic agonist dexmedetomidine in the rat. Am J Physiol. 1997;272:H2547–H2556. doi: 10.1152/ajpheart.1997.272.6.H2547. [DOI] [PubMed] [Google Scholar]
- 40.Krejci V, Hiltebrand LB, Sigurdsson GH. Effects of epinephrine, norepinephrine, and phenylephrine on microcirculatory blood flow in the gastrointestinal tract in sepsis. Crit Care Med. 2006;34:1456–1463. doi: 10.1097/01.CCM.0000215834.48023.57. [DOI] [PubMed] [Google Scholar]
- 41.Ducrocq N, Kimmoun A, Furmaniuk A, Hekalo Z, Maskali F, Poussier S, et al. Comparison of equipressor doses of norepinephrine, epinephrine, and phenylephrine on septic myocardial dysfunction. Anesthesiology. 2012;116(1083–91):42. doi: 10.1097/ALN.0b013e31824f9669. [DOI] [PubMed] [Google Scholar]
- 42.Mikkelsen MLG, Ambrus RB, Rasmussen R, Miles JE, Poulsen HH, Moltke FB, et al. The effect of dexmedetomidine on cerebral perfusion and oxygenation in healthy piglets with normal and lowered blood pressure anaesthetized with propofol–remifentanil TIVA. Acta Vet Scand. 2017 doi: 10.1186/s13028-017-0293-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lagerkranser M, Bergstrand G, Gordon E, Irestedt L, Lindquist C, Stange K, et al. Cerebral blood flow and metabolism during adenosine-induced hypotension in patients undergoing cerebral aneurysm surgery. Acta Anaesthesiol Scand. 1989;33:15–20. doi: 10.1111/j.1399-6576.1989.tb02852.x. [DOI] [PubMed] [Google Scholar]
- 44.Lee WA, Martin TD, Gravenstein N. Partial right atrial inflow occlusion for controlled systemic hypotension during thoracic endovascular aortic repair. J Vasc Surg. 2008;48:494–498. doi: 10.1016/j.jvs.2008.03.003. [DOI] [PubMed] [Google Scholar]
- 45.Pro.medicin. Dansk Lægemiddel Information A/S, Copenhagen. 2016. Metaoxedrin “SAD”—Phenylephrin. http://pro.medicin.dk/Medicin/Praeparater/3206. Accessed 16 May 2016.
- 46.Sano H, Dot M, Mimuro S, Yu S, Kurita T, Sato S. Evaluation of the hypnotic and hemodynamic effects of dexmedetomidine on propofol-sedated swine. Exp Anim. 2010;59:199–205. doi: 10.1538/expanim.59.199. [DOI] [PubMed] [Google Scholar]
- 47.Maas AI, Fleckenstein W, de Jong DA, van Santbrink H. Monitoring cerebral oxygenation: experimental studies and preliminary clinical results of continuous monitoring of cerebrospinal fluid and brain tissue oxygen tension. Acta Neurochir Suppl (Wien) 1993;59:50–57. doi: 10.1007/978-3-7091-9302-0_9. [DOI] [PubMed] [Google Scholar]
- 48.Xanthos T, Bassiakou E, Koudouna E, Tsirikos-Karapanos N, Lelovas P, Papadimitriou D, et al. Baseline hemodynamics in anesthetized Landrace-Large White swine: reference values for research in cardiac arrest and cardiopulmonary resuscitation models. J Am Assoc Lab Anim Sci. 2007;46:21–25. [PubMed] [Google Scholar]
- 49.Hemphill JC, 3rd, Knudson MM, Derugin N, Morabito D, Manley GT. Carbon dioxide reactivity and pressure autoregulation of brain tissue oxygen. Neurosurgery. 2001;48:377–383. doi: 10.1097/00006123-200102000-00028. [DOI] [PubMed] [Google Scholar]
- 50.Maloney-Wilensky E, Le Roux P. The physiology behind direct brain oxygen monitors and practical aspects of their use. Child’s Nerv Syst. 2010;26:419–430. doi: 10.1007/s00381-009-1037-x. [DOI] [PubMed] [Google Scholar]
- 51.Brassard P, Seifert T, Secher NH. Is cerebral oxygenation negatively affected by infusion of norepinephrine in healthy subjects? Br J Anaesth. 2009;102:800–805. doi: 10.1093/bja/aep065. [DOI] [PubMed] [Google Scholar]
- 52.Soeding PF, Hoy S, Hoy G, Evans M, Royse CF. Effect of phenylephrine on the haemodynamic state and cerebral oxygen saturation during anaesthesia in the upright position. Br J Anaesth. 2013;111:229–234. doi: 10.1093/bja/aet024. [DOI] [PubMed] [Google Scholar]
- 53.Meng L, Cannesson M, Alexander BS, Yu Z, Kain ZN, Cerussi AE, et al. Effect of phenylephrine and ephedrine bolus treatment on cerebral oxygenation in anaesthetized patients. Br J Anaesth. 2011;107:209–217. doi: 10.1093/bja/aer150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Moerman AT, Vanbiervliet VM, Van Wesemael A, Bouchez SM, Wouters PF, De Hert SG. Assessment of cerebral autoregulation patterns with near-infrared spectroscopy during pharmacological-induced pressure changes. Anesthesiology. 2015;123:327–335. doi: 10.1097/ALN.0000000000000715. [DOI] [PubMed] [Google Scholar]
- 55.Lucas SJ, Tzeng YC, Galvin SD, Thomas KN, Ogoh S, Ainslie PN. Influence of changes in blood pressure on cerebral perfusion and oxygenation. Hypertension. 2010;55:698–705. doi: 10.1161/HYPERTENSIONAHA.109.146290. [DOI] [PubMed] [Google Scholar]
- 56.Ogoh S, Sato K, Okazaki K, Miyamoto T, Secher F, Sorensen H, et al. A decrease in spatially resolved near-infrared spectroscopy-determined frontal lobe tissue oxygenation by phenylephrine reflects reduced skin blood flow. Anesth Analg. 2014;118:823–829. doi: 10.1213/ANE.0000000000000145. [DOI] [PubMed] [Google Scholar]
- 57.Meng L, Gelb AW, Alexander BS, Cerussi AE, Tromberg BJ, Yu Z, et al. Impact of phenylephrine administration on cerebral tissue oxygen saturation and blood volume is modulated by carbon dioxide in anaesthetized patients. Br J Anaesth. 2012;108:815–822. doi: 10.1093/bja/aes023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Davie SN, Grocott HP. Impact of extracranial contamination on regional cerebral oxygen saturation: a comparison of three cerebral oximetry technologies. Anesthesiology. 2012;116:834–840. doi: 10.1097/ALN.0b013e31824c00d7. [DOI] [PubMed] [Google Scholar]
- 59.Sorensen H, Secher NH, Siebenmann C, Nielsen HB, Kohl-Bareis M, Lundby C, et al. Cutaneous vasoconstriction affects near-infrared spectroscopy determined cerebral oxygen saturation during administration of norepinephrine. Anesthesiology. 2012;117:263–270. doi: 10.1097/ALN.0b013e3182605afe. [DOI] [PubMed] [Google Scholar]
- 60.Murkin JM, Arango M. Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br J Anaesth. 2009;103(Suppl 1):i3–i13. doi: 10.1093/bja/aep299. [DOI] [PubMed] [Google Scholar]
- 61.De Georgia MA. Brain tissue oxygen monitoring in neurocritical care. J Intensive Care Med. 2015;30:473–483. doi: 10.1177/0885066614529254. [DOI] [PubMed] [Google Scholar]
- 62.Rohlwink UK, Figaji AA. Methods of monitoring brain oxygenation. Child’s Nerv Syst. 2010;26:453–464. doi: 10.1007/s00381-009-1033-1. [DOI] [PubMed] [Google Scholar]
- 63.Ito H, Kanno I, Fukuda H. Human cerebral circulation: positron emission tomography studies. Ann Nucl Med. 2005;19:65–74. doi: 10.1007/BF03027383. [DOI] [PubMed] [Google Scholar]
- 64.Chang EH, Pezzulo AA, Meyerholz DK, Potash AE, Wallen TJ, Reznikov LR, et al. Sinus hypoplasia precedes sinus infection in a porcine model of cystic fibrosis. Laryngoscope. 2012;122:1898–1905. doi: 10.1002/lary.23392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Nathanson M, Moppett IK, Wiles M. Neuroanaesthesia. Oxford: Oxford University Press; 2011. [Google Scholar]
- 66.Willie CK, Tzeng YC, Fisher JA, Ainslie PN. Integrative regulation of human brain blood flow. J Physiol. 2014;592:841–859. doi: 10.1113/jphysiol.2013.268953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Heistad DD, Abboud FM. Factors that influence blood flow in skeletal muscle and skin. Anesthesiology. 1974;41:139–156. doi: 10.1097/00000542-197408000-00005. [DOI] [PubMed] [Google Scholar]
- 68.Armstead WM. Age-dependent cerebral hemodynamic effects of traumatic brain injury in newborn and juvenile pigs. Microcirculation. 2000;7:225–235. doi: 10.1111/j.1549-8719.2000.tb00123.x. [DOI] [PubMed] [Google Scholar]
- 69.Harada J, Takaku A, Endo S, Kuwayama N, Fukuda O. Differences in critical cerebral blood flow with age in swine. J Neurosurg. 1991;75:103–107. doi: 10.3171/jns.1991.75.1.0103. [DOI] [PubMed] [Google Scholar]
- 70.Armstead WM, Kiessling JW, Kofke WA, Vavilala MS. Impaired cerebral blood flow autoregulation during posttraumatic arterial hypotension after fluid percussion brain injury is prevented by phenylephrine in female but exacerbated in male piglets by extracellular signal-related kinase mitogen-activated protein kinase upregulation. Crit Care Med. 2010;38:1868–1874. doi: 10.1097/CCM.0b013e3181e8ac1a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Conrad MS, Johnson RW. The domestic piglet: an important model for investigating the neurodevelopmental consequences of early life insults. Annu Rev Anim Biosci. 2015;3:245–264. doi: 10.1146/annurev-animal-022114-111049. [DOI] [PubMed] [Google Scholar]
- 72.Conrad MS, Dilger RN, Johnson RW. Brain growth of the domestic pig (Sus scrofa) from 2 to 24 weeks of age: a longitudinal MRI study. Dev Neurosci. 2012;34:291–298. doi: 10.1159/000339311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Prabhakar H, Sandhu K, Bhagat H, Durga P, Chawla R. Current concepts of optimal cerebral perfusion pressure in traumatic brain injury. J Anaesthesiol Clin Pharmacol. 2014;30:318–327. doi: 10.4103/0970-9185.137260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Tranquilli WJ, Thurmon JC, Grimm KA, Lumb WV. Lumb & Jones’ veterinary anesthesia and analgesia. 4. Ames: Blackwell Pub; 2007. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Table of experimental data: Cerebral perfusion and oxygenation readings, physiological and haemodynamic data, blood gas data, and anaesthesia time at all time points throughout the experiment. PCB: Pre-Caval block; PR-1: baseline during propofol-remifentanil; NE-1: Norepinephrine during propofol-remifentanil; PR-intvas: after norepinephrine and wash-out period during propofol-remifentanil; PE-1: Phenylephrine during propofol-remifentanil; PR-2: after phenylephrine wash-out period/pre-dexmedetomidine during Propofol-remifentanil; PRD: Propofol-remifentanil-dexmedetomidine; NE-2: Norepinephrine during propofol-remifentanil; PRD-intvas: after norepinephrine and wash-out period during propofol-remifentanil-dexmedetomidine; PE-2: Phenylephrine during propofol-remifentanil-dexmedetomidine; PRD-end: after phenylephrine and wash-out period during propofol-remifentanil-dexmedetomidine (end of experiment); NIRS: Near infra red spectroscopy; LSCI: Laser speckle contrast imaging; MAP: mean arterial pressure; EtCO2: End-tidal carbon dioxide; FiO2: Fraction of inspired oxygen; (T): data corrected for body temperature; PaCO2: Partial pressure of arterial carbon dioxide; PaO2: Partial pressure of arterial oxygen; HCO3: Hydrogen bicarbonate; Hct: Haematocrit; THbc: Total haemoglobin concentration.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.