

Abstract
The aim of this study is to evaluate the presence of anti-laminin-1 antibodies (aLN-1) in sera and follicular fluid (FF) of infertile women affected by Hashimoto’s thyroiditis (HT) undergoing in vitro fertilization (IVF) and its impact on oocyte maturation and IVF outcome. aLN-1 were measured by a home-made enzyme linked immunosorbent assay (ELISA) in: (1) sera and FF from 44 infertile women affected by HT (HTIW) with tubal factor or male factor as primary cause of infertility; (2) in sera and FF from 28 infertile women without HT, with tubal factor or male factor as cause of infertility (infertile controls-ICTR); and (3) in sera from 50 fertile women (FW). aLN-1 serum levels were significantly higher in HTIW when compared with both fertile women and ICTR (P <0.001and P <0.01, respectively). Assuming as cutoff the 99th percentile of values obtained in sera of FW, 43.2% of HTIW and 3.6% of ICTR were aLN-1 positive (P = 0.0001). Also aLN-1 detected in FF from HTIW were significantly higher in comparison with those found in FF of ICTR (P = 0.006). In HTIW, metaphase II oocyte count showed inverse correlation with both serum and FF aLN-1 levels (r = 0.34, P = 0.02 and r = 0.33, P = 0.03, respectively). Implantation and pregnancy rates were significantly lower in HTIW (7.9% and 9.1%, respectively) when compared with ICTR (23% and 31.1%, respectively) (P = 0.015 and P = 0.03, respectively). Our results demonstrated for the first time the presence of aLN-1 in a relevant percentage of HTIW and suggest that these auto-antibodies may impair IVF outcome.
Keywords: anti-laminin-1 Ab, Hashimoto’s thyroiditis, in vitro fertilization (IVF) outcome
Introduction
Hashimoto’s thyroiditis (HT), characterized by the presence of auto-antibodies (auto-Ab) against thyroglobulin (TG-Ab) and thyroid peroxidase (TPO-Ab), is the most common autoimmune disease, affecting 5–15% of women of reproductive age.
Thyroid auto-Ab are frequently associated with reduced fertility and pregnancy loss.1–4 van den Boogard et al., in an extensive meta-analysis study, reported the association between the presence of TG-Ab and/or TPO-Ab and an increased risk of unexplained infertility, miscarriage, recurrent miscarriage, and preterm birth, even in the absence of overt clinical thyroid dysfunction.5
In the current literature, different results are available regarding the effect of thyroid autoimmunity (TAI) on in vitro fertilization (IVF) outcome.6–11 In the aforementioned meta-analysis study, it was reported that thyroid auto-Ab did not affect pregnancy rate after IVF.5 By contrast, Monteleone et al. demonstrated that in infertile women with TAI undergoing IVF, TPO-Ab, and/or TG-Ab were detectable in follicular fluid (FF), positively correlated with serum auto-Ab levels, and were associated with reduced oocyte fertilization, grade A embryos, and pregnancy rate.10 A close result has been reported in a retrospective study by Zhong et al., who found a reduced fertilization, implantation, and pregnancy rate, as well as an increased abortion rate in infertile women positive for anti-thyroid antibodies undergoing IVF.11
It is well known that autoimmunity plays an important role in reproductive failure and some auto-Ab, in particular antiphospholipid antibodies (APL), are significantly associated with infertility.12–14
More recently other auto-Ab, namely antibodies against laminin-1 (LN-1), have been associated with reproductive failure.15 Since LN-1 is an important component of the extracellular matrix involved in oocyte maturation, embryogenesis, implantation, and placentation,16,17 it has been suggested that anti-LN-1 antibodies (aLN-1) may affect early reproductive processes leading to autoimmune infertility.18
In humans, raised levels of aLN-1 are detectable in women with recurrent miscarriages and their prevalence is significantly higher in women with endometriosis.18,19
Recently, we analyzed aLN-1 presence in the serum and FF of infertile women with endometriosis undergoing IVF.20 Our data confirmed that aLN-1 levels were significantly higher in women with endometriosis when compared with infertile women without endometriosis. Interestingly, in the same study, we demonstrated a negative correlation between aLN-1 levels detected in FF and the number of metaphase II (MII) oocytes, suggesting that aLN-1 could affect oocyte maturation.
Besides disease-specific auto-Ab, auto-Ab with different specificities, including APL and other non-organ specific auto-Ab, are frequently detectable in patients with TAI when compared with healthy subjects.21–23
Although patients with TAI seem more prone to produce several auto-Ab, the presence of aLN-1 was not yet investigated in infertile women with HT.
Therefore, aim of our study is to evaluate: (1) the presence of aLN-1 in serum and FF of infertile women affected by HT undergoing IVF; and (2) the impact of aLN-1 on oocyte maturation and IVF outcome.
Materials and methods
Patients
The study was previously approved by the Institutional Review Board of Bari University Hospital and written informed consent was obtained from each patient.
Forty-four consecutive infertile women affected by HT (HT infertile women [HTIW]; mean age 35.3 ± 4.99 years; age range, 22–40 years), undergoing ovarian stimulation and IVF at the Centre of Reproductive Medicine of Bari, University Hospital, entered the study. The diagnosis of HT was based on standard clinical and laboratory criteria, including quantification of TG-Ab and TPO-Ab. Eligibility criteria were: (1) a normal menstrual cycle (range, 26–32 days); (2) baseline follicle stimulating hormone (FSH) levels <12 IU/mL; (3) body mass index (BMI) in the range of 18–30 kg/m2; (4) no oral contraceptive pills taken in the last year; (5) tubal factor or male factor as primary cause of infertility; and (6) normal blood free triiodothyronine (FT3) and free thyroxine (FT4) concentrations irrespective of treatment with levothyroxine. Exclusion criteria were: (1) other autoimmune disease, including anti-phospholipid syndrome (APS); (2) treatment with corticosteroids, immune-suppressive drugs, or immune-modulators; or (3) other cause of infertility.
As controls, sera and FF were obtained on the day of oocyte retrieval by 28 age-matched infertile women without HT (infertile controls [ICTR]) with male factor or tubal factor infertility undergoing IVF. They were included in the study according to the following criteria: (1) baseline FSH levels <12 IU/mL; (2) BMI in the range of 18–30 kg/m2; (3) no oral contraceptive pill taken in the last year; (4) absence of autoimmune disease and/or treatments affecting immune response; and (5) tubal factor or male factor as cause of infertility.
Sera were also obtained in the luteal phase of the menstrual cycle by 50 age-matched, fertile women (FW) (last pregnancy >2 years before study entry).
Ovarian hyperstimulation and IVF procedure
Pituitary desensitization was achieved using GnRH antagonists (Cetrotide, Merck Serono, Geneva, Switzerland) administered daily starting on day 6 of ovarian stimulation or GnRH agonists (Decapeptyl 0.1 mg/mL, Ipsen SpA, Assago (MI), Italy) started in the mid-luteal phase of the previous menstrual cycle. Both GnrH agonist and antagonist were continued until the hCG day administration.
Follicular growth was achieved with 150–225 IU/daily of recombinant FSH (Puregon, MSD Organon, Oss, The Netherlands or Gonal-F, Merck-Serono, Geneva, Switzerland) starting from day 2 or 3 of the cycle.24 The dosage of FSH was individualized based on the age and the ovarian reserve (basal FSH and antral follicles count).
A dose of 250 µg (6500 IU) of recombinant hCG (Ovitrelle, Merk-Serono, Geneva, Switzerland) was given for ovulation induction when two or more follicles ⩾18 mm in diameter were present and E2 concentrations dropped to 150–200 pg/mL for each leading follicle.
The response to stimulation was monitored with serial ultrasound scans and plasma estrogen levels. Transvaginal oocyte retrieval was performed 36 h after rhCG injection. Mature oocytes were inseminated with or without intra-cytoplasmic sperm injection (ICSI). Denuded oocytes were assessed for nuclear status by evaluating the polar body extrusion immediately before ICSI, alternatively on the day after oocytes retrieval in the IVF procedure. The embryos were transferred 48–72 h after insemination.
The implantation rate was calculated as the percentage of implanted embryos compared to the total number of transferred embryos. Clinical pregnancy was judged by observation of the gestational sac on vaginal ultrasonography after 6–7 weeks of gestation.
Sampling of sera and follicular fluids
Patient sera and FF were obtained on the day of oocyte retrieval. FF from large follicles (diameter, >16 mm) were collected in separate tubes and examined separately to pinpoint differences between immature and mature oocytes. Samples contaminated by blood cells were excluded. After centrifugation at 2000 × g, FF were stored at −80°C until assay. All samples were coded and the investigators performing aLN-1 assay were unaware of either the cause of infertility or IVF/ET outcome.
Biochemistry analyses
All biochemistry analyses were carried out in the same laboratory. Serum LH, progesterone, E2, TPO-Ab, and TG-Ab were measured by means of chemiluminescence. The dosing systems were ADVIA Centaur and ADVIA Centaur XP. Levels of THS, FT3, and FT4 were measured by Luminescent Oxygen Channeling Immunoassay (LOCI) technology.
ELISA for aLN-1 determination
Laminin from Engelbreth-Holm-Swarm murine sarcoma basement membrane, affinity purified anti- laminin antibodies produced in rabbit, bovine serum albumin (BSA), o-phenylenediamine (OPD), Tween-20, and 30% H2O2, were purchased from Sigma-Aldrich, Milan, Italy. Peroxidase (HRP)-conjugated affinity purified goat antibodies to human IgG and to rabbit IgG were obtained from Jackson Immunoresearch, Avondale, PA, USA.
In the ELISA described in this study, phosphate buffered saline (PBS) containing 0.05% (v/v) Tween-20, PBS/3% (w/v) BSA, and PBS/1% BSA/0.05/Tween 20 were used as washing, blocking, and diluent buffer, respectively. Each step, except the coating of the plates, was performed at 25°C.
Half of the wells (alternate rows) of 96-well ELISA plates (Nunc MaxiSorp, Roskilde, Denmark) were coated with 500 ng/100 µL/well of LN-1 in 0.05 M carbonate/bicarbonate buffer, pH 9.6 (coating buffer), while the other half with 100 µL of coating buffer alone and left overnight at 4°C. Wells were washed four times (250 µL/well of washing buffer) and non-specific site on the plates were blocked by incubating wells for 2 h with 125 µL of blocking buffer. After washes, 100 µL/well of serum or FF specimens (diluted 1:100 and 1:20, respectively) were added in duplicate in antigen-coated wells as well as in non-coated wells, the latter to assess the non-specific binding. In preliminary experiments we found that such different dilutions gave optimal specific/non-specific antibody binding ratio. Rabbit aLN-1 antibody was incubated in two wells of each plate at a concentration of 16.5 ng/100 µL/well in order to confirm antigen binding and as positive control. The assay blank value was obtained by using 100 µL/well of diluent buffer in place of serum. After a 30 min incubation, the plates were washed four times and 100 µL/well of HRP-conjugated anti human IgG or anti-rabbit IgG, diluted 1:8000 were applied for 30 min. After washing, 100 µL/well of freshly prepared solution of OPD (0.4 mg/mL) and hydrogen peroxide 30% (0.4 µL/mL) in citrate buffer (pH 5) were dispensed. The color reaction was stopped by addition of 50 µL/well of 2 M H2SO4 after a 10 min incubation in the dark. Optical densities (OD) were measured at 492 nm using an ELISA reader (Bio-Rad, Hercules, CA, USA).
The mean OD of the sample duplicates in the absence of antigen was subtracted from the mean OD achieved in the presence of antigen to obtain the net OD reading. aLN-1 values were expressed as percent of the positive control. The intra- and inter-assay coefficients of variation, the latter evaluated with a pool of sera or FF, were <10%.
Where FF samples were obtained from more than one follicle, the mean value of aLN-1 was utilized for statistical analysis.
Statistical analysis
Statistical analysis was performed with version 4 of GraphPad prism software (GraphPad, San Diego, CA, USA). According to the Gaussian or non-Gaussian distribution, continuous variables are reported as mean ± SD or median and 25th–75th percentiles, respectively, while numbers are presented as counts (percentage) for dichotomous data. Continuous data were compared with Student’s t-test or Mann–Whitney U test, for unpaired two group analyses; unpaired three group analysis was performed using Kruskal–Wallis ANOVA (Dunn’s post hoc test).
Spearman rank correlation coefficient analysis was used to examine the correlation between serum and FF aL-1 and between aL-1 levels and oocyte count. Frequency data were compared with Chi-square test or Fisher’s exact test. P values <0.05 were taken as statistically significant.
Results
In HTIW, male factor was present as primary cause of infertility in 23 of 44 women evaluated (52%), tubal factor in 17 women (39%), and both in four women (9%), while in ICTR male factor was present in 50%, tubal factor in 36%, and both in 14%.
Selected characteristics of participants at study entry are reported in Table 1.
Table 1.
Selected clinical and laboratory parameters of 44 infertile women with Hashimoto’s thyroiditis (HTIW) and 28 infertile controls (ICTR) at study enter.
| HTIW | ICTR | P value | |
|---|---|---|---|
| Age, years (mean ± SD) | 35.3 ± 4.99 | 33.79 ± 4.89 | 0.21* |
| BMI (mean ± SD) | 22.86 ± 2.8 | 22.1 ± 2.4 | 0.22* |
| FSH, IU/mL (mean ± SD) | 7.66 ± 2.34 | 7.37 ± 2.09 | 0.6* |
| TSH†, µIU/mL (median (25th–75th percentile)) | 2.22 (1.34–3.1) | 1.55 (1.23–2.25) | 0.048‡ |
| FT3§, pg/mL (median (25th–75th percentile)) | 2.95 (2.68–3.25) | 3.2 (2.9–3.43) | 0.02‡ |
| FT4**, ng/dL (median (25th–75th percentile)) | 1.14 (0.99–1.21) | 1.15 (1.06–1.29) | 0.22‡ |
| TG-Ab††, U/mL (median (25th–75th percentile)) | 147 (63–293) | 6 (2.5–17) | <0.0001‡ |
| TPO-Ab††, U/mL (median (25th–75th percentile)) | 92 (74–268) | 4.5 (1.5–17) | <0.0001‡ |
Unpaired Student’s t-test.
Normal range, 0.5–5.5.
Mann-Whitney U test.
Normal range, 2.3–4.2.
Normal range 0.7–1.8.
Normal values <60.
No significant differences were found regarding women’s age, BMI, and basal FSH. All HTIW showed normal blood FT3 and FT4 concentrations. Subclinical hypothyroidism (normal serum concentrations of FT3 and FT4, and TSH >5.5 µIU/mL) was present in three of 44 HTW.
Highly significant differences were found between HTIW and ICTR regarding both TG-Ab and TPO-Ab serum concentrations.
aLN-1 levels detected in sera of HTIW (median 30% of the positive control; 25th–75th percentiles 18.5–42.5) were significantly higher in comparison with those found both in FW (14; 6–20; P <0.001) and in ICTR (18.5; 8–27; P <0.01). The difference between FW and ICTR was not significant (Figure 1).
Figure 1.
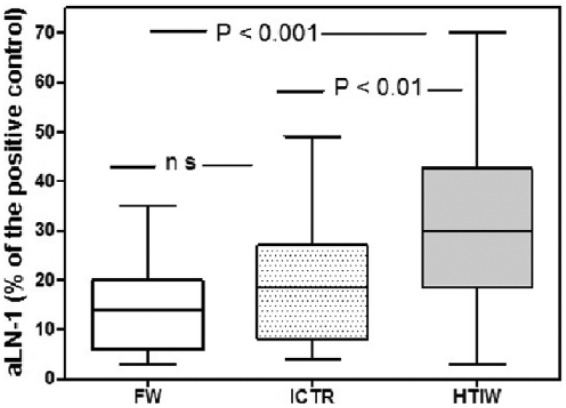
IgG-aLN-1 levels detected by ELISA in sera from 50 fertile women (FW), 44 infertile women with Hashimoto’s thyroiditis (HTIW), and 28 infertile controls (ICTR). The data are depicted as box-plot diagrams, with the box encompassing the range of values from the 25th percentile (lower bar) to the 75th percentile (upper bar). The horizontal line within the box represents the median, and the vertical lines represent maximum and minimum values.
Assuming as cutoff the 99th percentile of serum aLN-1 values obtained in FW (i.e. 33.04% of the positive control), the prevalence of serum aLN-1 in HTIW (19/44; 43.2%) was significantly higher in comparison with that found in ICTR (1/28; 3.6%) (P = 0.0001).
A total number of 315 and 227 FF were collected from HTIW and ICTR and of them, 58 (18%) and 46 (20%), respectively, were excluded due to blood contamination. However, FF from all HTIW and ICTR were analyzed.
aLN-1 detected in FF of HTIW (median 35% of positive control; 25th–75th percentiles 24.5–55.5) were significantly higher in comparison with ICTR (22; 14.5–36; P = 0.0063) (Figure 2).
Figure 2.
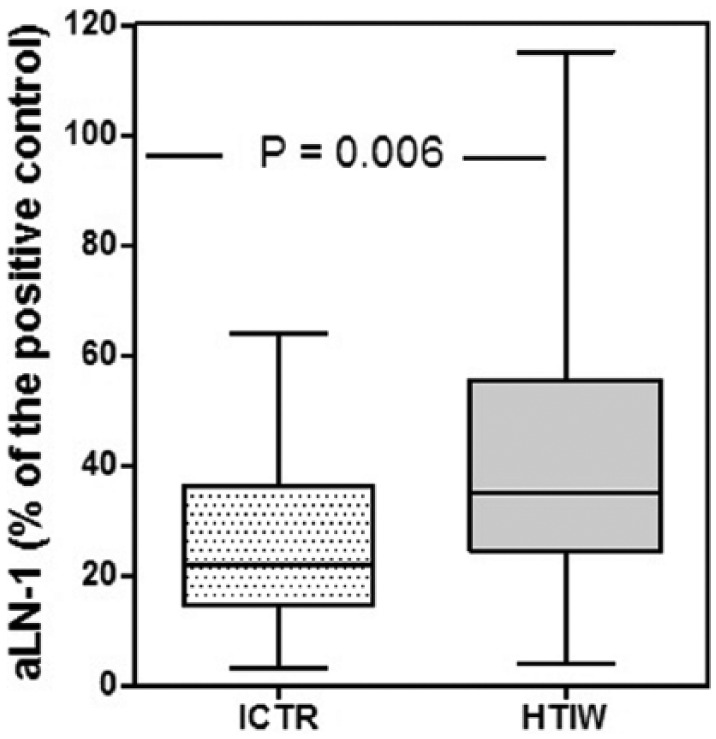
IgG-aLN-1 levels detected by ELISA in follicular fluids from 44 infertile women with Hashimoto’s thyroiditis (HTIW) and 28 infertile controls (ICTR). The data are depicted as box-plot diagrams, with the box encompassing the range of values from the 25th percentile (lower bar) to the 75th percentile (upper bar). The horizontal line within the box represents the median, and the vertical lines represent maximum and minimum values.
Serum-aLN-1 showed a highly significant correlation with FF and aLN-1, both in HTIW (r = 0.79, P <0.0001) and in ICTR (r = 0.76, P <0.0001) (Figure 3a and 3b).
Figure 3.

(a) Positive correlation detected between serum IgG-aLN-1 levels and FF IgG-aLN-1 levels in 44 infertile women with Hashimoto’s thyroiditis (HTIW). (b) Positive correlation detected between serum IgG-aLN-1 levels and FF IgG-aLN-1 levels in 28 infertile controls (ICTR).
In HTIW, there was no correlation between serum aLN-1 levels and TG-Ab (r = 0.03, P = 0.85) or TPO-Ab (r = 0.05, P = 0.75).
In HTIW a significant inverse correlation was found between MII oocyte counts and serum or FF aLN-1 (r = −0.34, P = 0.024, and r = −0.33, P = 0.03, respectively) (Figure 4a and 4b). All other correlations, i.e. between total oocytes and serum and FF-aLN-1 in HTIW, total and MII oocytes and serum and FF-aLN-1 in ICTR were not significant. In addition, no correlation was found between MII oocytes count and both TPO-Ab and TG-Ab (r = 0.05, P = 0.77, and r = 0.22, P = 0.16, respectively) (data not shown).
Figure 4.

(a) Inverse correlation between IgG-aLN-1 levels detected in sera from 44 infertile women with Hashimoto’s thyroiditis (HTIW) and MII oocyte count. (b) Inverse correlation between IgG-aLN-1 levels detected in follicular fluids from 44 HTIW and MII oocyte count.
As reported in Table 2, no significant differences were observed between HTIW and ICTR in estrogen levels on the day of hCG administration, total number of retrieved oocytes, MII oocyte count, number of transferred embryos, or in fertilization rate.
Table 2.
IVF outcome in 44 infertile women with Hashimoto’s thyroiditis (HTIW) and 28 infertile controls (ICTR).
| HTIW | ICTR | P value | |
|---|---|---|---|
| E2 on day of hCG (pg/mL) (median (25th–75th percentile)) | 1843 (1151–2700) | 1836 (859–2536) | 0.76* |
| Number of retrieved oocytes (median (25th–75th percentile)) | 6 (4–9) | 7 (5–12) | 0.34* |
| MII oocytes (median (25th–75th percentile)) | 5 (4–6.5) | 5.5 (5–8) | 0.28* |
| Number of embryos transferred (median (25th–75th percentile)) | 1.5 (1.5–2) | 2 (2–2) | 0.59* |
| Fertilization rate (%) | 67.4% (128/190) | 73.4% (91/124) | 0.26† |
| Implantation rate (%) | 7.9% (6/76) | 23% (12/52) | 0.015† |
| Pregnancy rate (%) | 9.1% (4/41) | 31.1% (9/28) | 0.03‡ |
Mann–Whitney U test.
Chi-square test.
Fisher’s exact test.
Both implantation and clinical pregnancy rate were significantly lower in HTIW when compared with ICTR. In fact, implantation rate was 7.9% in HTIW (6/76) and 23% in ICTR (12/52) (odds ratio [OR], 0.26; 95% confidence interval [CI], 0.099–0.0.82; P = 0.015), while pregnancy rate was 9.1% in HTIW (4/41) and 32.1% in ICTR (9/28) (OR, 4.86; 95% CI, 1.3–17.8; P = 0.03) (Table 2).
Discussion
In this study we demonstrated, for the first time, increased levels of aLN-1 in serum and FF of HTIW in comparison with both FW and ICTR. In addition, we found an inverse correlation between serum and FF-aLN1 levels and MII oocyte count, along with a significantly reduced implantation rate and pregnancy rate.
Among extracellular matrix components, LN-1 and fibronectin promote follicle maturation and increase the rate of oocyte polar body formation.26 Therefore, it is possible that aLN-1 may reduce MII oocyte count interfering with LN-1 functions.
Among its physiologic functions, LN-1 is involved in implantation and placentation as finely demonstrated by Klaffy et al.,27 who highlighted the importance of laminin-trophoblast cell interaction for implantation and placentation in a mouse model.
Additionally, the effects of aLN-1, as well as antibodies to laminin binding protein, have been investigated in animal models.28–30 Results clearly indicate that such auto-Ab may be responsible for reproductive failure and suggest their detrimental role on IVF outcome by affecting several steps of reproductive process. In this respect, it should be pointed out that in all four pregnant HTWI, serum aLN-1 levels fell into the normal range (i.e. below the 99th percentile of values obtained in FW), whereas TPO-Ab were positive in all and TG-Ab in three of them. Of course, due to the low number of HTIW who became pregnant following IVF, caution should be paid in interpreting this finding, which requires validation in a larger number of subjects.
In conclusion, our data show that HTIW have a reduced chance of successful IVF. Moreover, we demonstrated for the first time in a relevant percentage of HTIW the presence of aLN-1, namely different auto-Ab that, in addition to the effects of anti-thyroid antibodies, could increase the risk of poor IVF outcome.
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: This research was supported by MIUR “Programma Operativo Nazionale (PON) Bioscienze & Salute (B&H)”.
References
- 1. Poppe K, Glinoer D. (2003) Thyroid autoimmunity and hypothyroidism before and during pregnancy. Human Reproduction Update 9: 149–161. [DOI] [PubMed] [Google Scholar]
- 2. Tartakover-Matalon S, Blank M, Ornoy A, et al. (2001) The association between anti-thyroid antibodies and pregnancy loss. American Journal of Reproductive Immunology 45: 72–77. [DOI] [PubMed] [Google Scholar]
- 3. Stagnaro-Green A, Glinoer D. (2004) Thyroid autoimmunity and the risk of miscarriage. Best Practice & Research Clinical Endocrinology & Metabolism 18: 167–181. [DOI] [PubMed] [Google Scholar]
- 4. Poppe K, Velkeniers B, Glinoer D. (2008) The role of thyroid autoimmunity in infertility and pregnancy. Nature Clinical Practice Endocrinology & Metabolism 4: 394–405. [DOI] [PubMed] [Google Scholar]
- 5. Van den Boogaard E, Vissenberg R, Land JA, et al. (2011) Significance of (sub) clinical thyroid dysfunction and thyroid autoimmunity before conception and in early pregnancy: A systematic review. Human Reproduction Update 17: 605–619. [DOI] [PubMed] [Google Scholar]
- 6. Geva E, Vardinon N, Lessing JB, et al. (1996) Organ-specific autoantibodies are possible markers for reproductive failure: A prospective study in an in-vitro fertilization-embryo transfer program. Human Reproduction 11: 1627–1631. [DOI] [PubMed] [Google Scholar]
- 7. Kim C-H, Chae H-D, Kang B-M, et al. (1998) Influence of antithyroid antibodies in euthyroid women on in vitro fertilization-embryo transfer outcome. American Journal of Reproductive Immunology 40: 2–8. [DOI] [PubMed] [Google Scholar]
- 8. Muller AF, Verhoeff A, Mantel MJ, et al. (1999) Thyroid autoimmunity and abortion: A prospective study in women undergoing in vitro fertilization. Fertility and Sterility 71: 30–34. [DOI] [PubMed] [Google Scholar]
- 9. Kutteh WH, Schoolcraft WB, Scott RT. (1999) Antithyroid antibodies do not affect pregnancy outcome in women undergoing assisted reproduction. Human Reproduction 14: 2886–2890. [DOI] [PubMed] [Google Scholar]
- 10. Monteleone P, Parrini D, Faviana P, et al. (2011) Female infertility related to thyroid autoimmunity: The ovarian follicle hypothesis. American Journal of Reproductive Immunology 66: 108–114. [DOI] [PubMed] [Google Scholar]
- 11. Zhong YP, Ying Y, Wu HT, et al. (2012) Relationship between antithyroid antibody and pregnancy outcome following in vitro fertilization and embryo transfer. International Journal of Medical Sciences 9: 121–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Geva E, Amit A, Lerner-Geva L, et al. (1997) Autoimmunity and reproduction. Fertility and Sterility 67: 599–611. [DOI] [PubMed] [Google Scholar]
- 13. Reimand K, Talja I, Metskula K, et al. (2001) Autoantibodies studies of female patients with reproductive failure. Journal of Reproductive Immunology 51: 167–176. [DOI] [PubMed] [Google Scholar]
- 14. Sherer Y, Tartakover-Matalon S, Blank M, et al. (2003) Multiple autoantibodies associated with autoimmune reproductive failure. Journal of Assisted Reproduction and Genetics 20: 53–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Inagaki J, Kondo A, Lopez LR, et al. (2005) Pregnancy loss and endometriosis: Pathogenic role of anti-laminin-1 autoantibodies. Annals of the New York Academy of Sciences 1051: 174–184. [DOI] [PubMed] [Google Scholar]
- 16. Colognato H, Yurchenco PD. (2000) Form and function: The laminin family of heterotrimers. Developmental Dynamics 218: 213–234. [DOI] [PubMed] [Google Scholar]
- 17. Smyth N, Vatansever HS, Murray P, et al. (1999) Absence of basement membranes after targeting the LAMC1 gene results in embryonic lethality due to failure of endoderm differentiation. Journal of Cell Biology 144: 151–160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Inagaki J, Sugiura-Ogasawara M, Nomizu M, et al. (2003) An association of IgG anti-laminin-1 autoantibodies with endometriosis in infertile patients. Human Reproduction 18: 544–549. [DOI] [PubMed] [Google Scholar]
- 19. Inagaki J, Matsuura E, Nomizu M, et al. (2001) IgG anti-laminin-1 autoantibody and recurrent miscarriages. American Journal of Reproductive Immunology 45: 232–238. [DOI] [PubMed] [Google Scholar]
- 20. Caccavo D, Pellegrino NM, Totaro I, et al. (2011) Anti-laminin-1 antibodies in sera and follicular fluid of women with endometriosis undergoing in vitro fertilization. International Journal of Immunopathology and Pharmacology 24: 481–488. [DOI] [PubMed] [Google Scholar]
- 21. Paggi A, Caccavo D, Ferri GM, et al. (1994) Anti-cardiolipin antibodies in autoimmune thyroid diseases. Clinical Endocrinology 40: 329–333. [DOI] [PubMed] [Google Scholar]
- 22. Nabriski D, Ellis M, Ness-Abramof R, et al. (2000) Autoimmune thyroid disease and antiphospholipid antibodies. American Journal of Hematology 64: 73–75. [DOI] [PubMed] [Google Scholar]
- 23. Tektonidou MG, Anapliotou M, Vlachoyiannopoulos P, et al. (2004) Presence of systemic autoimmune disorders in patients with autoimmune thyroid diseases. Annals of the Rheumatic Diseases 63: 1159–1161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Depalo R, Jayakrishan K, Garruti G, et al. (2012) GnRH agonist versus GnRH antagonist. Reproductive Biology and Endocrinology 10: 26–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Glinoer D. (1997) The regulation of thyroid function in pregnancy: Pathways of endocrine adaptation from physiology to pathology. Endocrine Reviews 18: 404–433. [DOI] [PubMed] [Google Scholar]
- 26. Kreeger PK, Deck JW, Woodruff TK, et al. (2006) The in vitro regulation of ovarian follicle development using alginate-extracellular matrix gels. Biomaterials 27: 714–723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Klaffky E, Williams R, Yao CC, et al. (2001) Trophoblast-specific expression and function of the integrin α7 subunit in the peri-implantation mouse embryo. Developmental Biology 239: 161–175. [DOI] [PubMed] [Google Scholar]
- 28. Foidart JM, Yaar M, Figueroa A, et al. (1983) Abortion in mice induced by intravenous injection of antibodies to type IV collagen or laminin. American Journal of Pathology 110: 346–357. [PMC free article] [PubMed] [Google Scholar]
- 29. Tartakover Matalon S, Blank M, Matsuura E, et al. (2003) Immunization of naïve mice with mouse laminin-1 affected pregnancy outcome in a mouse model. American Journal of Reproductive Immunology 50: 159–165. [DOI] [PubMed] [Google Scholar]
- 30. Zhang C, Duan E, Cao Y, et al. (2000) Effect of 32/67 laminin-binding protein antibody on mouse embryo implantation. Journal of Reproduction and Fertility 119: 137–142. [DOI] [PubMed] [Google Scholar]