

Abstract
The concept of using natural orifices to reduce the complications of surgery, Natural Orifices Transluminal Endoscopic Surgery, has also been applied to therapeutic endoscopy. Endoscopic submucosal surgery (ESS) provides more treatment options for various gastrointestinal diseases than traditional therapeutic endoscopy by using the submucosal layer as a working space. ESS has been performed in various fields ranging from transluminal peritoneoscopy to peroral endoscopic myotomy. With further advances in technology, ESS will be increasingly useful for diagnosis and treatment of gastrointestinal diseases.
Keywords: Endoscopic submucosal surgery, Natural orifices transluminal endoscopic surgery, Peroral endoscopic myotomy, Endoscopic pyloromyotomy, Endoscopic submucosal tunnel dissection
INTRODUCTION
Advances in therapeutic endoscopy and laparoscopic surgery have caused a shift in focus from maximal to minimal access surgery. Natural Orifices Transluminal Endoscopic Surgery (NOTES) represents an approach to the peritoneal cavity through the wall of the gastrointestinal tract without the need for a skin incision [1]. This approach can appeal to patients as it leaves them free of a surgical scar. With many advantages over conventional surgery, NOTES aims to eliminate the complications related to incisions, and may provide unique benefits with the avoidance of wound infections, fewer adhesions, decreased incidence of ileus, more rapid recovery, less postoperative pain, and no abdominal wall hernias. Endoscopic submucosal surgery (ESS) is derived from the concept of NOTES. Therapeutic endoscopy has advanced at a rapid pace since endoscopic resection was first used for excision of early mucosal cancer in the late 20th century. Therapeutic endoscopy has introduced the concept of NOTES to enable surgery beyond the mucosa. Experimental transgastric peritoneoscopy was first described in 2004 by Kalloo et al. using a porcine model [2]. After upper endoscopy, the peritoneal cavity was accessed by needle-knife puncture of the gastric wall. The peritoneal cavity was examined and a liver biopsy specimen was obtained. The gastric wall incision was closed with clips. Herein, the outlines of the procedure and human applications of ESS will be described.
OUTLINE OF ENDOSCOPIC SUBMUCOSAL SURGERY
Submucosal endoscopy with a mucosal flap safety valve (SEMF) technique is based on the concept of using the submucosa as a practical working space for endoscopic interventions. This technique provides a protective submucosal tunnel to prevent peritoneal contamination and a mucosal entry point that can be closed with clips alone. The SEMF technique was proposed by Sumiyama et al. [3] and modified by Yoshizumi et al. [4].
PREPARATION FOR ENDOSCOPIC SUBMUCOSAL SURGERY
Because of the submucosal tunneling, air leakage usually occurs in the abdominal cavity and general anesthesia with controlled ventilation should be used to prevent complications such as pneumothorax and pneumoperitoneum. Prophylactic antibiotics are given 30 minutes before surgery because of the high risk of infection due to use of endoscopic knives and other surgical tools. Patient positioning varies depending on the lesion, but it is usually better to place the patient supine and expose part of the thorax and abdomen. Air is the main source of carbon dioxide in the rapid absorption of air that has leaked into the abdominal or thoracic cavity after surgery.
HUMAN APPLICATIONS OF ENDOSCOPIC SUBMUCOSAL SURGERY
Peroral endoscopic myotomy
Peroral endoscopic myotomy (POEM) utilizes a submucosal tunnel (Fig. 1). After injection, an incision is made approximately 12 cm proximal to the esophagogastric junction. Submucosal dissection is usually performed up to the cardia. The submucosal tunnel creates a stable working space for myotomy and helps to prevent infection by creating a safety check valve. After selective myotomy, closure of the entry site is achieved with endoclips. Human applications of POEM were first described by Inoue et al. in 2010 [5]. Now, POEM is accepted as a safe and effective procedure for achalasia [6]. POEM can be used to treat achalasia, different types of spastic motility disorders, and various comorbid conditions, even in children and the elderly. POEM provides excellent relief of dysphagia and chest pain for patients with esophageal spastic disorders with acceptable procedural morbidity. POEM also offers a logical therapeutic modality for patients with severe symptomatic esophageal ring [7].
Fig. 1.

Schematic process of peroral endoscopic myotomy. (A) After injection, an incision is made. (B) Submucosal dissection is usually performed up to the cardia of the stomach. (C) Selective myotomy is performed with an endoscopic knife. (D) After selective myotomy, closure of the entry site is achieved with endoclips.
Endoscopic pyloromyotomy
POEM can be used in patients with gastroparesis refractory to medical therapy. Human applications of gastric POEM were first described by Khashab et al. [8]. The order of endoscopic pyloromyotomy is similar to that of POEM (Fig. 2). First, the incision is placed 5 cm proximal to the pylorus. Submucosal injection, mucosal incision, and creation of the submucosal tunnel are then performed. The pylorus is dissected until deeper layers appear. The thickness of the pyloric ring is about 7 mm. Complete pyloromyotomy is performed with full separation of the pyloric ring. Lastly, complete closure of the mucosal entry is performed using standard hemoclips. In light of literature reports and the authors’ experience, POEM seems to be a relatively safe and effective procedure [9,10]. Long-term follow-up should be performed to confirm the efficacy and indications for this technique, and a comparative study with previous methods is also needed.
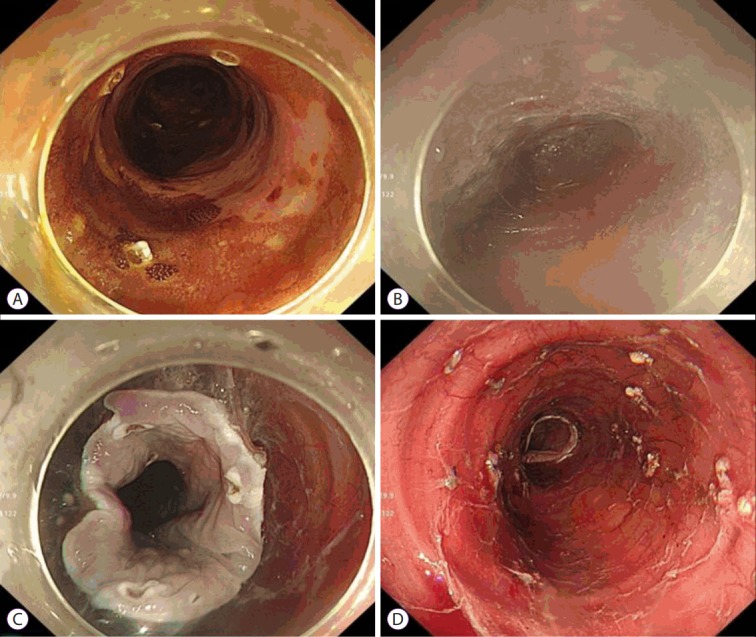
Fig. 2.

Endoscopic pyloromyotomy. (A) Submucosal injection 5 cm proximal to the pylorus. (B) After mucosal incision, submucosal dissection is usually performed up to the pylorus. (C) The pylorus is dissected until deeper layers are apparent. (D) Closure of the mucosal entry using standard hemoclips.
Endoscopic submucosal tunnel dissection
We can also remove a subepithelial tumor (SET) using the combination of submucosal tunnel technique and endoscopic resection. Because endoscopic submucosal dissection of a tumor originating from the intrinsic epithelium is rarely attempted due to the risk of perforation, surgery has been the main treatment modality. However, a number of preliminary studies have been reported on endoscopic submucosal tunnel dissection (ESTD) for resection of a SET [11-13]. We made an incision 5 cm proximal to the lesion, and a submucosal tunnel was created with a tip-knife. The exposed tumor was completely resected and collected using an insulation-tipped knife. Finally, the tumor was removed and the mucosal entry point was sutured. This technique is also used to remove large early esophageal cancers (Fig. 3). ESTD is relatively safe and allows en bloc resection of large esophageal neoplastic lesions without aggressive esophageal resection [14]. However, since the number of studies is small and the long-term treatment results are not known, more clinical experience will be needed.
Fig. 3.
Endoscopic submucosal tunnel dissection for superficial esophageal cancer. (A) Marking the proximal and distal ends of the tumor. (B) Submucosal tunnel reached the distal end. (C, D) Circumferential submucosal dissection was completed. (E, F) The final specimen removed with endoscopic submucosal tunnel dissection.
CONCLUSIONS
NOTES represents a new era in interventional endoscopy. With the development of many tools, the human NOTES experience will continue to broaden. Endoscopists have developed new applications for ESS, but their limitations include the need for peritoneal access and closure, infection, development of anastomotic devices, insufflation, spatial orientation, platform development, and so on. With more experience, ESS is expected to become an important NOTES method and will improve the quality of life.
Footnotes
Conflicts of Interest:The authors have no financial conflicts of interest.
REFERENCES
- 1.Swain P. A justification for NOTES--natural orifice translumenal endosurgery. Gastrointest Endosc. 2007;65:514–516. doi: 10.1016/j.gie.2006.11.034. [DOI] [PubMed] [Google Scholar]
- 2.Kalloo AN, Singh VK, Jagannath SB, et al. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc. 2004;60:114–117. doi: 10.1016/s0016-5107(04)01309-4. [DOI] [PubMed] [Google Scholar]
- 3.Sumiyama K, Tajiri H, Gostout CJ. Submucosal endoscopy with mucosal flap safety valve (SEMF) technique: a safe access method into the peritoneal cavity and mediastinum. Minim Invasive Ther Allied Technol. 2008;17:365–369. doi: 10.1080/13645700802528512. [DOI] [PubMed] [Google Scholar]
- 4.Yoshizumi F, Yasuda K, Kawaguchi K, Suzuki K, Shiraishi N, Kitano S. Submucosal tunneling using endoscopic submucosal dissection for peritoneal access and closure in natural orifice transluminal endoscopic surgery: a porcine survival study. Endoscopy. 2009;41:707–711. doi: 10.1055/s-0029-1214959. [DOI] [PubMed] [Google Scholar]
- 5.Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010;42:265–271. doi: 10.1055/s-0029-1244080. [DOI] [PubMed] [Google Scholar]
- 6.Stavropoulos SN, Desilets DJ, Fuchs KH, et al. Per-oral endoscopic myotomy white paper summary. Surg Endosc. 2014;28:2005–2019. doi: 10.1007/s00464-014-3630-7. [DOI] [PubMed] [Google Scholar]
- 7.Song GW, Ko WJ, Kim WH, Hahm KB, Hong SP, Cho JY. Peroral endoscopic myotomy for esophageal muscular ring. Endoscopy. 2015;47 Suppl 1 UCTN:E387–E388. doi: 10.1055/s-0034-1392596. [DOI] [PubMed] [Google Scholar]
- 8.Khashab MA, Stein E, Clarke JO, et al. Gastric peroral endoscopic myotomy for refractory gastroparesis: first human endoscopic pyloromyotomy (with video) Gastrointest Endosc. 2013;78:764–768. doi: 10.1016/j.gie.2013.07.019. [DOI] [PubMed] [Google Scholar]
- 9.Chung H. Endoscopic pyloromyotomy: overview and early experience. In: International Digestive Endoscopy Network 2015 (IDEN 2015); 2015 Sep 12-13; Seoul, Korea. Seoul. 2015. pp. 143–146. [Google Scholar]
- 10.Kawai M, Peretta S, Burckhardt O, Dallemagne B, Marescaux J, Tanigawa N. Endoscopic pyloromyotomy: a new concept of minimally invasive surgery for pyloric stenosis. Endoscopy. 2012;44:169–173. doi: 10.1055/s-0031-1291475. [DOI] [PubMed] [Google Scholar]
- 11.Inoue H, Ikeda H, Hosoya T, et al. Submucosal endoscopic tumor resection for subepithelial tumors in the esophagus and cardia. Endoscopy. 2012;44:225–230. doi: 10.1055/s-0031-1291659. [DOI] [PubMed] [Google Scholar]
- 12.Gong W, Xiong Y, Zhi F, Liu S, Wang A, Jiang B. Preliminary experience of endoscopic submucosal tunnel dissection for upper gastrointestinal submucosal tumors. Endoscopy. 2012;44:231–235. doi: 10.1055/s-0031-1291720. [DOI] [PubMed] [Google Scholar]
- 13.Lu J, Zheng M, Jiao T, Wang Y, Lu X. Transcardiac tunneling technique for endoscopic submucosal dissection of gastric fundus tumors arising from the muscularis propria. Endoscopy. 2014;46:888–892. doi: 10.1055/s-0034-1377442. [DOI] [PubMed] [Google Scholar]
- 14.Gan T, Yang JL, Zhu LL, Wang YP, Yang L, Wu JC. Endoscopic submucosal multi-tunnel dissection for circumferential superficial esophageal neoplastic lesions (with videos) Gastrointest Endosc. 2016;84:143–146. doi: 10.1016/j.gie.2016.01.049. [DOI] [PubMed] [Google Scholar]