

Abstract
Objective
To determine if family food and mealtime practices experienced in adolescence are carried forward into parenthood.
Design
Baseline (EAT-I) and 15-year follow-up (EAT-IV) survey data from a population-based cohort study (Project EAT).
Participants
Cohort members identified as parents at follow-up (n=727). To gain additional data about the practices of both parents in the household, significant others completed surveys at EAT-IV (n=380).
Main Outcome Measure
Frequency of family meals, healthfulness of foods at home, frequency of meals in front of the TV, and expectations of being home for dinner.
Analysis
Linear regression models tested associations between parent food and mealtime practices reported at baseline and follow-up controlling for demographics.
Results
Healthy and unhealthy home food availability, expectations to be home for dinner, and eating in front of the television in adolescence predicted similar outcomes 15 years later among female parents (effect sizes range: β=0.2–0.3; p<.001), and to a lesser extent among males. Families ate more frequent family meals when either 1 or both parents reported frequent family meals as an adolescent compared to when neither parent reported frequent family meals as an adolescent.
Conclusions and Implications
Parenting interventions that target healthful family food and mealtime practices are important to invest in because of their potential long-term impact on their own children’s parenting practices.
Keywords: parent feeding practices, family mealtime, longitudinal dietary research, adolescents
INTRODUCTION
The family and home food environment is an important public health target for promoting healthy eating patterns in children and reducing chronic disease risk.1–3 The rules, structures, and routines that families practice around food and mealtimes help to shape children’s current and future eating habits.1,2 For example, a large body of evidence now shows that practices such as making available and serving healthy foods, having frequent family meals, and creating expectations for mealtimes are related to a variety of positive dietary outcomes in children and adolescents. For example, studies have found that more frequent family meals are associated with higher diet quality,4,5 lower rates of disordered eating,6 better weight status,7 lower risk for depression and substance abuse,8,9 and improved well-being.9 Previous studies have also identified associations between healthy food and beverage consumption and family practices such as healthy home food availability and rules like having to eat dinner with the family and not eating in front of the TV.10
There is also evidence to suggest that the benefits of family food and mealtime practices within the home carry forward from childhood to adulthood to positively influence health across the lifespan. For example, regular family meals during adolescence are associated with healthier dietary patterns in adolescence and predict healthier eating patterns in young adulthood.11,12 Further, the availability of unhealthy foods in the home during childhood is associated with less healthful eating in early adolescence.13 To understand the full potential of healthful family food and mealtime practices, it is of interest to know if the family food and mealtime practices an individual experiences during adolescence are carried forward and implemented with their own family during adulthood, as this would have health implications for the next generation of children. Only a small number of qualitative and cross-sectional studies have assessed past experiences with family meals retrospectively and they provide some evidence to suggest that parents who have regular family meals recall having had regular family meals as a child.14–16
To build on this previous literature, there is a need to examine relationships between current and past experiences with a variety of family food and mealtime practices prospectively, in longitudinal samples that span adolescence and parenthood. In addition, studies are needed to explore gender differences in the adoption of family food and mealtime practices given that the roles of males and females differ in many families, particularly with regard to food provision and household responsibilities,17. Finally, it will be important to examine the combined experiences of both parents within a household, as the past experiences of both parents are relevant to current family meal experiences.
To address current gaps in the literature, this study utilized baseline and 15-year follow-up data from the Project EAT (Eating and Activity in Teens and Young Adults) cohort and had 3 study aims. The first aim was to examine, among longitudinal cohort participants, whether the use of 4 family food and mealtime practices experienced in adolescence, specifically: 1) family meal frequency; 2) home food availability; 3) meals eaten in front of the TV; and 4) expectations to be home for dinner (referred to as family food and mealtime practices from this point on) were carried forward into adulthood as a parent. It was hypothesized that family food and mealtime practices would be associated longitudinally, indicating that practices reported in adolescence inform practices that an individual uses later on in life with their own family. The second aim was to determine, among longitudinal cohort participants, if family food and mealtime practices reported during adolescence were carried forward differently by males and females. It was hypothesized that associations would be stronger for females than for males. Finally, the third aim of this study was to explore, in a subset of families where data were available from both parents, how the frequency of family meals in adolescence of each parent contributed to current family meal frequency. For example, it was of interest to compare families where both parents had regular family meals as adolescents to families where only 1 parent had regular family meals as an adolescent. It was hypothesized that associations would be stronger when both parents report having experienced concordant practices in adolescence.
METHODS
Study Design
Data were drawn from the 1st and 4th waves of Project EAT, a 15-year longitudinal study that examined dietary intake, physical activity, weight control behaviors, weight status, and factors associated with these outcomes among young adults.18,19 Data from EAT-I (baseline) and EAT-IV (15-year follow-up) were used because they captured the 2 periods of interest (i.e., adolescence and adulthood/early parenthood) and thus contained corresponding survey questions about family food and mealtime practices. In contrast, at EAT-II and EAT-III, when participants were in emerging adulthood, survey questions were tailored to that particular developmental period and focused on social eating with friends as well as the college/university eating environments.
Participants and Recruitment
Given that the focus of this study was on family practices, the analytic sample was restricted to the 727 young adults who participated in both waves of the study and who were a parent to 1 or more children (≥ 1 years old) living in their home at least 50% of the time in EAT-IV. Participants were asked specifically about their own children, including stepchildren or adopted children. In EAT-I, middle school and high school students at 31 public schools in Minneapolis-St. Paul completed surveys and anthropometric measures during the 1998–1999 academic year. EAT-IV was designed to follow up on the original participants in 2015–2016 as they were progressing through young adulthood at a time of life when many of the participants would be parents.
At follow-up, all participants in the original sample who had responded to at least 1 previous follow-up survey were invited to complete the EAT-IV survey online, by mail, or by phone. Surveys were completed by 66% of those who could be contacted and 95% completed the survey online. When respondents indicated they had been living in the same household as their current significant other for at least 6 months, significant others were also invited to complete their own survey online or by mail. Significant other surveys were returned by 60% of the sample with an eligible spouse/partner. All study protocols were approved by the University of Minnesota’s Institutional Review Board Human Subjects Committee.
Instruments
To allow for longitudinal comparisons, key items from earlier study waves were retained on the EAT-IV survey.19 Additions to the survey were also made to reflect the study’s life course perspective and focus on learning about significant other and intergenerational influences on weight-related outcomes. Scale psychometric properties were examined in the full EAT-IV sample and test-retest reliability or percent agreement was assessed in a diverse adolescent sample (n=161) at EAT-I and in a sample of 103 young adults at EAT-IV. The psychometric properties of survey measures are reported below for follow-up unless the measure was included only at baseline.
Measures
Family meal frequency
In EAT-I participants were asked, “During the past seven days, how many times did all, or most, of your family living in your house eat a meal together?” (Test-retest r=0.70). At EAT-IV participants were asked, “During the past seven days, how many times did all, or most, of the people living in your household eat a meal together?” (Test-retest r=0.64). Response options were: never, 1–2 times, 3–4 times, 5–6 times, 7 times, more than 7 times. Additionally, at EAT-IV, significant others were asked: “When you were a teenager, how many times per week did your family eat a meal together? Response options were: less than weekly, 1–2 times, 3–4 times, 5–6 times, 7 times, more than 7 times. For all 3 items, a continuous variable was created whereby responses were given numerical values representing times per week: never/less than weekly=0; 1–2 times=1.5; 3–4 times=3.5; 5–6 times=5.5; 7 times=7; more than 7 times=10.
Healthy home food availability
3 items assessed healthy foods available in the home at both time points. Participants were asked, “How often are the following true? a) Fruits and vegetables are available in my home (Test-retest r=0.74); b) Vegetables are served at dinner in my home (Test-retest r=0.76); c) Milk is served at meals in my home (Test-retest r=0.82). Response options were: Never, Sometimes, Usually, Always. Items were summed to produce an index with a higher score indicating more healthful items available or served more often (range=3–12).
Unhealthy home food availability
3 items assessed unhealthy foods or drinks available in the home at both time points. Participants were asked, “How often are the following true?: a) Potato chips or other salty snack foods are available in my home (Test-retest r=0.70); b) Chocolate or other candy is available in my home (Test-retest r=0.66); c) Soda pop is available in my home (Test-retest r=0.72)” Response options were: Never, Sometimes, Usually, Always. Items were summed to produce an index with a higher score indicating more unhealthy items available more often (range=3–12).
Eating dinner while watching TV
At both time points, participants were asked, “How strongly do you agree with the following statements about mealtimes in your family?: In my family, we often watch TV while eating dinner” (Test-retest r=0.86). Response options were: strongly disagree, somewhat disagree, somewhat agree, strongly agree.
Expectation to be home for dinner
At both time points, participants were asked, “How strongly do you agree with the following statements about mealtimes in your family?: In my family, we are expected to be home for dinner” (Test-retest r=0.60). Response options were: strongly disagree, somewhat disagree, somewhat agree, strongly agree.
Socio-demographics
Age in years was calculated by subtracting the participant’s self-reported birthdate from the date on which the survey was completed (percent agreement=99%). Sex was self-reported as male or female (percent agreement=99%). Socioeconomic status (SES) at baseline was calculated primarily from the highest educational attainment of the participants’ parents with penalties for reporting being on public assistance or being unemployed. The participant reported their own highest level of education achieved, which was treated as a continuous variable ranging from 1=middle school or junior high to 7=graduate or professional degree (percent agreement=97%). Participants reported their relationship status (casually dating/committed dating relationship vs. engaged/married/domestic partner; percent agreement=95%), and reported if they currently live with their significant other (yes/no; percent agreement=100%). Participants reported age in years for each of the children living more than 50% of the time in their household and a mean age of the children living in the household was calculated from these reported ages.
Data Analysis
Descriptive statistics were used to present the mean and standard deviation of family food and mealtime practices at baseline (EAT-I) and follow-up (EAT-IV). Significant differences across time were examined with a paired t-test. Graphical examination of each variable confirmed that variables were normally distributed, or deviated only modestly from normality, and tests performed were robust to modest deviations from normality.
Separate linear regression models were run to examine associations between family food and mealtime practices at baseline and follow-up adjusted for the participants’ age, sex, and educational attainment, and the SES of their parents in adolescence (primarily based on parent education). Interaction effects were tested by sex and further examined in stratified models if any effects had a p-value<0.05. Results are presented as standardized beta coefficients and standard errors. To account for multiple testing (n=22), a bonferoni adjusted p-value of <0.002 was considered statistically significant.
In the sample of participants whose significant other completed the baseline survey (n=380), linear regression models were run to test the association between family meal frequency in adolescence reported retrospectively by the significant other and current family meal frequency. To determine if associations with current family meal frequency were more positive when both partners had frequent family meals in adolescence, past family meal frequency variables were dichotomized and 4 groups were created to compare each possible combination among couples: both partners reported family meals <5 times/week (low-low); both partners reported family meals ≥5 times per week (high-high); partners reported discordant family meals (EAT-I participant only reported family meals ≥5 times per week [high-low] or significant other only reported family meals ≥5 times per week [low-high]). The adjusted mean number of family meals at follow-up was examined for each of the 4 concordant/discordant groups using linear regression followed by the margins command to obtain adjusted means and p-values determined using the delta method.
Study variables had a varying amount of missing data, with none greater than 3%; therefore, all analyses were conducted with complete cases. All analyses were conducted using Stata (Stata Statistical Software, version 13, statacorp., College Station, TX, 2013).
RESULTS
Sample Characteristics
The mean age (SD) of parents in the cohort sample (n=727) was 31 years (1.5), 63% were female, 96% were living with a significant other, 81% were married or had a domestic partner, and 63% had 2 or more children living in their household with a mean age of 4.6 years (3.3). The significant other sample (n=380) had a mean age (SD) of 32 years (3.3), 46% were female, and retrospective report of family meal frequency in adolescence was as follows: less than weekly (6.6%); 1–2 times per week (14.7%); 3–4 times per week (22.9%); 5–6 times per week (26.1%); 7 times per week (11.8%); more than 7 times per week (17.9%).
Frequency of family food and mealtime practices reported as adolescents and as parents
Family food and mealtime practices reported as a parent (EAT-IV) were more favorable (i.e., more healthful) than what they reported in their homes as adolescents (EAT-I) (Table 1). For example, participants reported having an average of 4.1 family meals per week as adolescents and 6.8 family meals per week as parents. Similarly, participants reported having more healthy foods available, fewer unhealthy foods available, eating dinner in front of the TV less frequently, and higher expectations for the family to be home for dinner as parents than they did as adolescents.
Table 1.
Family Food and Mealtime Practices Reported as an Adolescent (EAT-I) and as a Parent (EAT-IV)
| Females (n=458) | Males (n=267) | |||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| EAT I |
EAT IV |
EAT I |
EAT IV |
|||
| Mean (SD) | Mean (SD) | p-value | Mean (SD) | Mean (SD) | p-value | |
|
|
|
|
|
|||
| Family meal frequency, 0–10 times/wk (n=717) | 4.0 (3.2) | 6.9 (3.1) | <.001 | 4.1 (3.0) | 6.7 (3.1) | <.001 |
| Healthy home food availability, 3–12 (n=706) | 9.5 (2.0) | 9.9 (1.7) | <.001 | 9.9 (1.7) | 9.7 (1.6) | 0.09 |
| Unhealthy home food availability, 3–12 (n=712) | 8.2 (2.1) | 7.3 (1.9) | <.001 | 9.0 (2.1) | 7.7 (2.0) | <.001 |
| Eating dinner with TV, 1–4 (n= 698) | 2.4 (1.0) | 2.1 (1.0) | <.001 | 2.4 (1.0) | 2.1 (1.1) | <.001 |
| Expected to be home for dinner, 1–4 (n=695) | 2.3 (1.0) | 3.1 (0.9) | <.001 | 2.6 (0.9) | 3.1 (0.9) | <.001 |
Data come from surveys collected in 1999 (EAT-I) and 2016 (EAT-IV) from participants of Project EAT, a longitudinal cohort of adolescents from Minneapolis-St. Paul, MN, who identified as parents at EAT-IV.
Paired t-tests were used to determine differences between EAT-I an EAT-IV family food and mealtime practices.
Longitudinal adjusted associations between family food and mealtime practices in adolescence and as parents
Adjusted for demographic characteristics, associations between family food and mealtime practices reported in adolescence and those practiced as parents were examined with interaction effects by sex. Interactions were found for unhealthy home food availability (p=.02), and eating dinner with the TV (p=.002), therefore, associations are presented separately for males and females (Table 2).
Table 2.
Associations Between Family Food and Mealtime Practices Reported as an Adolescent (EAT-I) and as a Parent (EAT-IV)
| EAT-IV |
||||
|---|---|---|---|---|
| Females |
Males |
|||
| EAT-I | β | p-value | β | p-value |
|
|
|
|||
| Family Meal Frequency | 0.07 | .16 | 0.03 | .61 |
| Healthy Home Food Availability | 0.31 | <.001 | 0.29 | <.001 |
| Unhealthy Home Food Availability | 0.18 | <.001 | 0.09 | .16 |
| Eating dinner with TV | 0.24 | <.001 | 0.08 | .22 |
| Expected to be home for dinner | 0.20 | <.001 | 0.12 | .05 |
Data come from surveys collected in 1999 (EAT-I) and 2016 (EAT-IV) from participants of Project EAT, a longitudinal cohort of adolescents from Minneapolis-St. Paul, MN, who identified as parents at wave 4.
Five separate linear regression models run for each practice at EAT-IV (outcome) and at EAT-I (predictor). Standardized regression coefficients (β) and p-values are presented. All models control for participants’ age, sex, and educational attainment, and their socioeconomic status as an adolescent (based primarily on parent education)
Positive associations between each family food and mealtime practice in adolescence and the same practice at follow-up were found among females, with fewer associations found among males. For females, higher reporting of each family food and mealtime practice in adolescence was associated with greater use of that same practice as a parent, with the exception of family meal frequency, where no association was found. The magnitudes of the associations were moderate and ranged from 0.24 to 0.34. For males, a single association was found. Males who had healthier home food availability as adolescents also reported healthier foods in their homes as a parent (β=0.29, p<.001).
Associations with significant others’ retrospective account of family meal frequency in adolescence
For a subset of participants whose significant other completed a survey (n=380), a positive association between current family meal frequency and significant others’ retrospective report about when they were an adolescent was found (β=0.28, p<.001). Patterns in concordance/discordance were also examined: 24.1% of couples reported having frequent family meals as adolescents (≥5 times/week; high-high); 27.6% of couples reported having infrequent family meals as adolescents (<5 times/week; low-low); and the remaining 51.7% reported discordant family meal frequencies as adolescents (high-low or low-high). As shown in Figure 1, current mean number of weekly family meals (adjusted for covariates) was higher when at least 1 partner had frequent family meals as an adolescent as compared to when both partners had infrequent family meals as an adolescent; no additional benefit was observed when both parents (as compared to only 1) reported frequent family meals as an adolescent.
Figure 1. Mean number of family meals per week among families (N=380) by concordance and discordance in parents’ family meal frequency as an adolescent.
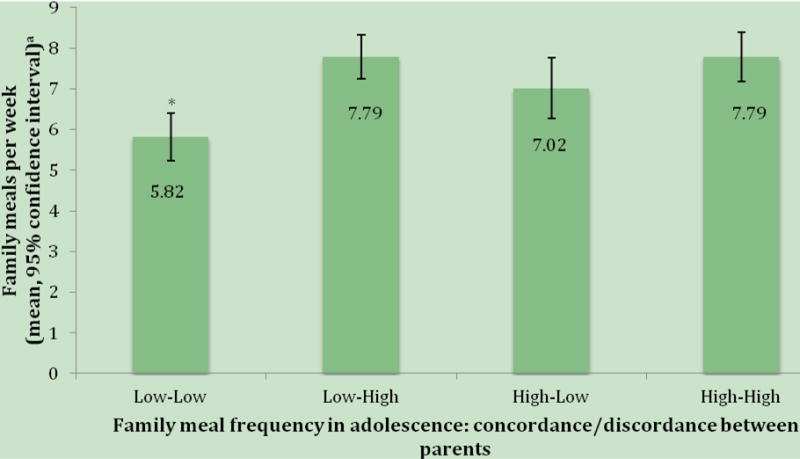
Data come from surveys collected in 1999 (EAT-I) and 2016 (EAT-IV) from participants of Project EAT, a longitudinal cohort of adolescents from Minneapolis-St. Paul, MN, who identified as parents and from the significant other of cohort participants at EAT-IV.
aMeans adjusted for participants’ age, gender, and educational attainment, and their socioeconomic status as an adolescent (primarily based on parent education)
*Significantly different from other groups (Bonferroni adjusted p<.002)
Low-low (n=104) represents the longitudinal cohort participant and their significant other reporting < 5 family meals per week as an adolescent
High-high (n=91) represents the longitudinal cohort participant and their significant other reporting ≥5 family meals per week as an adolescent
High-low (n=62; EAT-I participant only reported ≥5 family meals per week as an adolescent) and low-high (n=120; significant other only reported ≥5 family meals per week as an adolescent) represent couples who were in different family meal frequency categories as adolescents.
Family meal frequency was collected as an adolescent (EAT-I) among the longitudinal cohort participants and was collected as a retrospectively at EAT-IV among significant others of the longitudinal cohort participants.
DISCUSSION
This study sought to determine if family food and mealtime practices experienced in adolescence are carried forward into parenthood. Results from this longitudinal study of adolescents followed over 15 years, encompassing important developmental stages of the life course and including the potential influence of their significant other, suggest that family food and mealtime practices, such as the healthfulness of food available/offered, expectations to be home for dinner, and eating in front of the television, are carried forward to the next generation by females, but to a lesser extent by males. These findings highlight that the family food and mealtime environment of adolescents may shape what is practiced later in adulthood and thus has implications for interventions.
As hypothesized, the healthfulness of food available/offered in the home, expectations to be home for dinner, and eating in front of the television during adolescence predicted use of these practices as parents, and relationships were stronger for females. However, contrary to our hypothesis, family meal frequency as reported by the original cohort member for a given week in adolescence was not prospectively related to family meal frequency as a parent. On the other hand, data collected from the cohort member’s significant other revealed that retrospective report of average family meal frequency in adolescence was associated with more family meals as a parent. Other studies exploring family meals have found this relationship when examined retrospectively among parents.14–16 Differences observed between males and females should be further understood but may have to do with the continued role of females in American society as the primary purveyors of home and domestic responsibilities.17,20
The benefits of family meals for health and well-being have been well documented in the literature and communicated with the public,3,21 and indeed, family meals were much more frequently endorsed in the sample of parents at follow-up than at baseline. Results show that in families of young children, discordance between parents’ family meal frequency as an adolescent did not reduce the likelihood of having regular family meals as long as 1 parent had regular family meals as an adolescent. Discordance between parents for other family food and mealtime practices were not examined in this study, and very little research has explored congruence in parent food practices.22–24 In cross-sectional studies, discordance in food parenting practices attenuated associations with children’s snacking behavior24 and was associated with greater adolescent unhealthy weight control behaviors and fast food consumption,23 although findings were inconsistent across practices and outcomes. It is also important to consider that what is practiced among families with young children may be different than with adolescent children; therefore, families in Project EAT should continue to be followed to determine if patterns persist further into parenthood.
An important strength of this study is the longitudinal design that collected data both in adolescence and young adulthood. This design is important in order to reduce recall bias and control for sociodemographic characteristics in adolescence and young adulthood. However, recall bias may have biased significant others’ retrospective recollections of their adolescent experiences. This study also has limitations including, the self-reported nature of the data, differences in family meal frequency assessment for cohort members versus their significant other in analyses of concordance/discordance, and social-desirability bias, which may impact the responses of adolescents and adults differently.25 Responses may also be biased due to attrition of the original study sample. In addition, surveys administered to significant others only asked about adolescent experiences of family meal frequency; therefore, discordance/concordance between partners’ history of other family food and mealtime practices could not be examined. Future research should explore how each parent’s past experiences interact to determine how a variety of family food and mealtime practices are utilized in families. Finally, only a select number of family food and mealtime practices were examined (for example, TV as a distraction during mealtimes did not include other devices such as cell phones or computers) and relationships between these additional practices may differ from those in the present study.
Implications for Research and Practice
The preliminary findings from this study suggest that what parents practice with their adolescent children may influence what these adolescent children go on to practice with their own families as adults. This means that targeting food-related parenting practices within families of adolescents through interventions and public policy could have a multigenerational effect and thus a wide-reaching public health impact. However, given associations identified in this study were moderate and it is unclear to what extent traits of the individual (and not the parent or home environment) influence associations in family food and mealtime practices over time: a) there are likely opportunities to change or improve family food and mealtime practices at various times across the life course beyond adolescence; and b) parenting interventions likely need to be complemented by other individual, social, economic and physical supports guided by public health policy. Making parents aware of the potential long-term impacts of healthful parenting practices may add motivation for their use, however, there remains a need to better understand how to successfully help parents modify their food and mealtime practices. Interventions that promote healthful practices in the home warrant continued development and rigorous testing in different population groups to determine their short- and long-term impacts and to better understand for whom these interventions are most effective.
Acknowledgments
Research is supported by grant number R01HL116892 from the National Heart, Lung, and Blood Institute (PI: Neumark-Sztainer). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung and Blood Institute, the National Institute of Child Health and Human Development or the National Institutes of Health. AW received salary support from the Canadian Institutes of Health Research.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Birch LL, Davison KK. Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatr Clin North Am. 2001;48:893–907. doi: 10.1016/s0031-3955(05)70347-3. [DOI] [PubMed] [Google Scholar]
- 2.Patrick H, Nicklas TA. A review of family and social determinants of children’s eating patterns and diet quality. J Am Coll Nutr. 2005;24:83–92. doi: 10.1080/07315724.2005.10719448. [DOI] [PubMed] [Google Scholar]
- 3.Fulkerson JA, Larson N, Horning M, Neumark-Sztainer D. A review of associations between family or shared meal frequency and dietary and weight status outcomes across the lifespan. J Nutr Educ Behav. 2014;46:2–19. doi: 10.1016/j.jneb.2013.07.012. [DOI] [PubMed] [Google Scholar]
- 4.Hammons AJ, Fiese BH. Is frequency of shared family meals related to the nutritional health of children and adolescents? Pediatrics. 2011;127:e1565–74. doi: 10.1542/peds.2010-1440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Utter J, Scragg R, Schaaf D, Mhurchu CN. Relationships between frequency of family meals, BMI and nutritional aspects of the home food environment among New Zealand adolescents. Int J Behav Nutr Phys Act. 2008;5:50. doi: 10.1186/1479-5868-5-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Loth K, Wall M, Choi C-W, Bucchianeri M, Quick V, Larson N, et al. Family meals and disordered eating in adolescents: are the benefits the same for everyone? Int J Eat Disord. 2015;48:100–10. doi: 10.1002/eat.22339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berge JM, Wall M, Hsueh T-F, Fulkerson JA, Larson N, Neumark-Sztainer D. The protective role of family meals for youth obesity: 10-year longitudinal associations. J Pediatr. 2015;166:296–301. doi: 10.1016/j.jpeds.2014.08.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eisenberg ME, Olson RE, Neumark-Sztainer D, Story M, Bearinger LH. Correlations between family meals and psychosocial well-being among adolescents. Arch Pediatr Adolesc Med. 2004;158:792–6. doi: 10.1001/archpedi.158.8.792. [DOI] [PubMed] [Google Scholar]
- 9.Utter J, Denny S, Robinson E, Fleming T, Ameratunga S, Grant S. Family meals and the well-being of adolescents. J Paediatr Child Health. 2013;49:906–11. doi: 10.1111/jpc.12428. [DOI] [PubMed] [Google Scholar]
- 10.Couch SC, Glanz K, Zhou C, Sallis JF, Saelens BE. Home food environment in relation to children’s diet quality and weight status. J Acad Nutr Diet. 2014;114:1569–1579 e1. doi: 10.1016/j.jand.2014.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Larson NI, Neumark-Sztainer D, Hannan PJ, Story M. Family meals during adolescence are associated with higher diet quality and healthful meal patterns during young adulthood. J Am Diet Assoc. 2007;107:1502–10. doi: 10.1016/j.jada.2007.06.012. [DOI] [PubMed] [Google Scholar]
- 12.Neumark-Sztainer D, Hannan PJ, Story M, Croll J, Perry C. Family meal patterns: associations with sociodemographic characteristics and improved dietary intake among adolescents. J Am Diet Assoc. 2003;103:317–22. doi: 10.1053/jada.2003.50048. [DOI] [PubMed] [Google Scholar]
- 13.Vereecken C, Haerens L, Bourdeaudhuij ID, Maes L. The relationship between children’s home food environment and dietary patterns in childhood and adolescence. Public Health Nutr. 2010;13:1729–35. doi: 10.1017/S1368980010002296. [DOI] [PubMed] [Google Scholar]
- 14.Friend S, Fulkerson JA, Neumark-Sztainer D, Garwick A, Flattum CF, Draxten M. Comparing childhood meal frequency to current meal frequency, routines, and expectations among parents. J Fam Psychol. 2015;29:136–40. doi: 10.1037/fam0000046. 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.De Backer CJS. Family meal traditions. Comparing reported childhood food habits to current food habits among university students. Appetite. 2013;69:64–70. doi: 10.1016/j.appet.2013.05.013. [DOI] [PubMed] [Google Scholar]
- 16.Malhotra K, Herman AN, Wright G, Bruton Y, Fisher JO, Whitaker RC. Perceived benefits and challenges for low-income mothers of having family meals with preschool-aged children: childhood memories matter. J Acad Nutr Diet. 2013;113:1484–93. doi: 10.1016/j.jand.2013.07.028. [DOI] [PubMed] [Google Scholar]
- 17.Beagan B, Chapman GE, D’Sylva A, Bassett BR. ‘It’s just easier for me to do it’: rationalizing the family division of foodwork. Sociology. 2008;42:653–71. [Google Scholar]
- 18.Berge J, Miller J, Watts AW, Larson NI, Loth KA, Neumark-Sztainer D. Family meals from adolescence to young adulthood: Associations with young parents’ dietary, weight-related and psychosocial outcomes. Public Health Nutr. doi: 10.1017/S1368980017002270. (In Press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Larson N, Neumark-Sztainer D, Story M, van den Berg P, Hannan PJ. Identifying correlates of young adults’ weight behavior: survey development. Am J Health Behav. 2011;35:712–25. [PMC free article] [PubMed] [Google Scholar]
- 20.Flagg LA, Sen B, Kilgore M, Locher JL. The influence of gender, age, education and household size on meal preparation and food shopping responsibilities. Public Health Nutr. 2014;17:2061–70. doi: 10.1017/S1368980013002267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Harrison ME, Norris ML, Obeid N, Fu M, Weinstangel H, Sampson M. Systematic review of the effects of family meal frequency on psychosocial outcomes in youth. Can Fam Physician. 2015;61:e96–106. [PMC free article] [PubMed] [Google Scholar]
- 22.Larsen JK, Hermans RCJ, Sleddens EFC, Engels RCME, Fisher JO, Kremers SPJ. How parental dietary behavior and food parenting practices affect children’s dietary behavior. Interacting sources of influence? Appetite. 2015;89:246–57. doi: 10.1016/j.appet.2015.02.012. [DOI] [PubMed] [Google Scholar]
- 23.Berge JM, MacLehose RF, Meyer C, Didericksen K, Loth KA, Neumark-Sztainer D. He said, she said: examining parental concordance on home environment factors and adolescent health behaviors and weight status. J Acad Nutr Diet. 2016;116:46–60. doi: 10.1016/j.jand.2015.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gevers DWM, van Assema P, Sleddens EFC, de Vries NK, Kremers SPJ. Associations between general parenting, restrictive snacking rules, and adolescent’s snack intake. The roles of fathers and mothers and interparental congruence. Appetite. 2015;87:184–91. doi: 10.1016/j.appet.2014.12.220. [DOI] [PubMed] [Google Scholar]
- 25.Fulkerson JA, Neumark-Sztainer D, Story M. Adolescent and parent views of family meals. J Am Diet Assoc. 2006;106:526–32. doi: 10.1016/j.jada.2006.01.006. [DOI] [PubMed] [Google Scholar]