

Abstract
Background
People who inject drugs (PWID) constitute 60% of the approximately 5 million people in the U.S. infected with hepatitis C virus (HCV). Treatment of PWID is complex due to addiction, mental illness, poverty, homelessness, lack of positive social support, poor adherence-related skills, low motivation and knowledge, and poor access to and trust in the health care system. New direct-acting antiviral medications are available for HCV with high cure rates and few side effects. The life expectancy and economic benefits of new HCV treatments will not be realized unless we determine optimal models of care for the majority of HCV-infected patients. The purpose of this study is to evaluate the effectiveness of directly observed therapy and group treatment compared with self-administered individual treatment in a large, urban opioid agonist therapy clinic setting in the Bronx, New York.
Methods/design
In this randomized controlled trial 150 PWID with chronic HCV were recruited from opioid agonist treatment (OAT) clinics and randomized to one of three models of onsite HCV treatment in OAT: 1) modified directly observed therapy; 2) group treatment; or 3) control – self-administered individual treatment. Participants were age 18 or older, HCV genotype 1, English or Spanish speaking, treatment naïve (or treatment experienced after 12/3/14), willing to receive HCV treatment onsite, receiving methadone or buprenorphine at the medication window at least once per week, and able to provide informed consent. Outcomes of interest include adherence (as measured by self-report and electronic blister packs), HCV treatment completion, sustained virologic response, drug resistance, and cost-effectiveness.
Discussion
This paper describes the design and rationale of a randomized controlled trial comparing three models of care for HCV therapy delivered in an opioid agonist treatment program. Our trial will be critical to rigorously identify models of care that result in high adherence and cure rates. Use of blister pack technology will help us determine the role of adherence in successful cure of HCV. Moreover, the trial methodology outlined here can serve as a template for the development of future programs and studies among HCV-infected drug users receiving opioid agonist therapy, as well as the cost-effectiveness of such programs.
Trial registration
This trial was registered with ClinicalTrials.gov (NCT01857245). Trial registration was obtained prospectively on May 20th, 2013.
Keywords: Hepatitis C virus, Injection drug use, People who inject drugs, Directly observed therapy, Group treatment, Models of care
Background
Hepatitis C virus (HCV) is the leading cause of cirrhosis, hepatocellular carcinoma, and liver transplantation in the United States. Successful HCV treatment leading to sustained virologic response (SVR) is associated with decreased progression of liver disease and increased survival [1]. Without active treatment, mortality and health care costs due to HCV are expected to increase over the next two decades [2].
People who inject drugs (PWID) constitute 60% of the approximately 5 million people in the U.S. infected with HCV [3]. Although a large proportion of PWID with HCV are willing to undergo treatment [4–6], few are offered HCV treatment due to concerns about suboptimal adherence rates [7, 8]. PWID face many challenges in adhering to therapy including addiction, mental illness, poverty, homelessness, lack of positive social support, poor adherence-related skills, low motivation and knowledge, and poor access to and trust in the health care system [9, 10]. New direct-acting antiviral (DAA) regimens are promising for treatment on this population. However, optimal cost-effective models of care that promote adherence and SVR have not been elucidated.
To maximize HCV treatment outcomes, we have developed a multidisciplinary model of HCV care that integrates substance abuse treatment, on-site primary care, and HCV-related care within opioid agonist treatment (OAT) clinics. Adherence support is particularly important for active drug users, because active drug use has been associated with non-adherence in the setting of HIV antiretroviral therapy (ART) [11–14]. Although treatment for addiction and access to multidisciplinary teams likely play important roles in successfully treating HCV-infected PWID, it is unknown which specific psychosocial and/or structural interventions are needed.
We have piloted two models of intensive care: modified directly observed therapy (mDOT), and group treatment (GT). The proposed mDOT and GT interventions are guided by Fisher’s Information-Motivation-Behavior Skills (IMB) model [15–17]. The IMB model asserts that information, motivation, and behavioral skills are fundamental determinants of adherence [15]. According to the IMB model, information and motivation work through behavioral skills to affect adherence. Behavioral skills are a critical prerequisite of adherence, and determine whether even well-informed and motivated individuals are able to adhere. The IMB model further specifies that personal and situational characteristics, such as poor psychologic health, substance abuse, unstable housing, or inadequate access to medical care, may moderate these relationships and impact adherence [15]. In extreme cases, strong negative effects on adherence are expected, and interventions aimed at improving information and motivation may not be effective without support.
In our mDOT model, adherence to HCV treatment is linked to an established behavioral skill, specifically clinic attendance addresses adherence skills: acquisition and administration of HCV medications; incorporation of HCV treatment into daily routines; coping with side effects (through side effect assessment and management); and acquisition of social support. While primarily operating on behavioral skills, the mDOT intervention also enhances both information and motivation (through support from nurses and other clinic staff).
In our GT model, patient groups initiate and complete HCV treatment in a weekly treatment group, which provides powerful social support to mitigate fears of side effects, promote efficient education, and deliver medications. GT addresses information (through education by providers), motivation (through peer and provider support), and behavioral skills (by dispensing medications during group). While mDOT and GT have been associated with good pilot outcomes [18], we do not know whether either model is more efficacious or cost-effective than the standard care.
The primary objective of this study is to determine the effectiveness of three models of care for HCV treatment in PWID. The aims of this study are 1) to determine whether mDOT or GT is more efficacious than a control group of self-administered individual treatment (SIT) for enhancing adherence and virological outcomes, and decreasing drug resistance; 2) to determine the incidence and factors associated with the development of drug resistance in PWID initiating HCV treatment; 3) to perform cost and cost-effectiveness analyses of each model of intensive on-site HCV care; 4) to determine whether adherence to HIV ART, HIV viral load (VL), and CD4 count are affected by initiating HCV therapy.
We hypothesize that 1) rates of adherence, treatment completion, and SVR will be significantly higher in the intensive intervention arms compared to the control arm, and that rates of resistance will be lower. We further hypothesize that the proportion of subjects in the intensive models of care arms who achieve an SVR will be equivalent to that observed in large registration trials. 2) We hypothesize that only a minority (~ 20%) of PWID will develop resistance, and that the relationship between adherence and resistance will be quadratic. 3) We hypothesize that the total cost of delivering the GT intervention will be lower than delivering the mDOT intervention, and that the incremental cost-effectiveness ratios for CGT compared with SIT and mDOT compared with SIT will each be less than $100,000/QALY. 4) We hypothesize that adherence to ART, HIV VLs, and CD4 counts will not be affected by initiating HCV therapy.
The trial entitled Intensive Models of HCV Care for Injection Drug Users (ClinicalTrials.gov NCT01857245) has completed enrollment as of 5/9/16, treatment as of 9/5/16, and follow up is ongoing. In this manuscript, we provide a detailed description of the trial design and the methodological approach to analysis, which will complement the reporting of the study findings.
Methods/design
Study setting
This study is a randomized controlled trial in which 150 PWID with chronic HCV (genotype 1) were recruited from three Division of Substance Abuse (DoSA) clinics. DoSA is a network of nine methadone maintenance clinics administered by the Albert Einstein College of Medicine in the Bronx, New York. DoSA clinics provide comprehensive substance abuse treatment including pharmacotherapy and supportive services to approximately 4200 adults (≥ 18 years) with current substance use disorders (typically heroin). The primary focus is treatment of opioid dependence with methadone, and the average methadone pick-up schedule is 5 times per week. Three of DoSA’s clinics were the sites for study recruitment and delivery of the SIT, mDOT and group interventions.
Multidisciplinary staff comprised of substance abuse counselors, nurses, a part-time social worker, and a medical team consisting of a physician and at least one physician assistant delivers substance abuse treatment at each DoSA clinic. The medical team provides comprehensive primary medical care, including HCV and HIV care.
On-site HCV treatment program
HCV-infected patients with appropriate insurance (including Medicaid) are offered on-site HCV evaluation and treatment by primary care providers, and are free to choose whether to receive HCV and other medical care at the methadone clinic or elsewhere. Primary care providers receive ongoing HCV-related training from an internist with expertise in providing HCV treatment to drug users and follow standardized HCV treatment protocols [19].
This trial began when the standard of care was pegylated interferon (IFN) alfa-2a injections (180 mcg weekly), self-administered twice-daily ribavirin, and telaprevir or boceprevir. The trial was adapted to reflect the standard of care with the release of DAAs. Trial participants were initiated on HCV regimens from 10/29/13 to 5/23/16 according to AASLD guidelines current at the time of treatment initiation: telaprevir/pegylated interferon/ribavirin (TVR/IFN/RBV) as of 10/29/13, sofosbuvir/pegylated interferon/ribavirin (SOF/IFN/RBV) and sofosbuvir/ribavirin (SOF/RBV) as of 12/10/13, sofosbuvir/simeprevir (SOF/SMV) as of 8/11/14, and sofosbuvir/ledipasvir (SOF/LDV) as of 11/11/14.
Trial inclusion and exclusion criteria
Potential trial subjects were eligible for inclusion if infected with HCV genotype 1, > 18 years of age, English or Spanish speaking, treatment naïve (or treatment experienced after 12/3/14), willing to receive HCV treatment onsite, and receiving methadone or buprenorphine at the medication window at least three times per week (or at least once per week after 6/26/15). Participants were excluded if they had known hypersensitivity to any study medication or were decompensated cirrhotic, unable or unwilling to provide informed consent, psychiatrically unstable, or pregnant or breast-feeding.
Approvals and data safety and monitoring
The trial was approved by the Committee on Clinical Investigations of the Albert Einstein College of Medicine and the Institutional Review Board of Montefiore Medical Center. All participants provided written informed consent. We were testing a low-risk behavioral intervention that is highly integrated with usual clinical care; for this reason, we did not create an independent data safety and monitoring board. Instead we established a data safety and monitoring plan, which required interim analyses after every 50 patients enrolled to determine whether there were sufficient risks or benefits, or whether significant differences in virologic outcomes between study arms developed to warrant trial cessation.
Recruitment
Medical providers were asked to invite all patients initiating on-site HCV treatment to consider enrolling in the trial. Subjects also self-referred after seeing flyers posted in clinics, or were referred by other subjects or through HCV support groups. The initial steps in subject recruitment included a brief screening survey, informed consent, and in depth verification of eligibility using medical records and discussion with providers.
Randomization
We recruited 150 patients who were randomized to mDOT, GT, or in a 1:1:1 ratio in variable block sizes of 3–6 via central, computer-generated randomization (see Fig. 1). Two special randomization strategies (stratification and blocking) were used to avert imbalances in prognostic factors, and to ensure comparison groups of approximately equal size. We stratified randomization by IL28B genotype, HIV status, and stage of liver disease (cirrhosis vs. no cirrhosis) because of the importance of these factors in determining virologic outcomes [20–22]. To determine presence of cirrhosis, our algorithm included prioritizing a liver biopsy performed within the last 2 years (Ishak Stage 1–4 vs. 5/6) or any liver biopsy that demonstrated cirrhosis. As non-invasive testing became standard of care, we used fibrosure (< 0.75 vs ≥ 0.75), which was performed on all participants at baseline, and fibroscan (< 12.5 kPa vs ≥ 12.5 kPa) beginning 8/14/15 to determine the presence of cirrhosis [23, 24]. In cases where fibroscans and liver biopsies were not available and fibrosure testing was indeterminate, we used an AST to Platelet Ratio Index (APRI) score of ≥ 2.
Fig. 1.
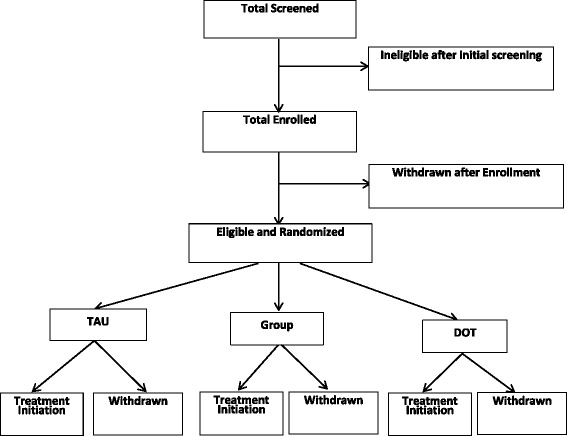
Flow chart of study recruitment and enrollment
Models of care
All 3 models of care included co-located onsite care including HCV care, primary care, and OAT. Table 1 summarizes similarities and differences between the 3 models.
Table 1.
Characteristics of three models of care
| Element | SIT | mDOT | GT |
|---|---|---|---|
| Co-located care | X | X | X |
| Enhanced Social Support by providers | Nurse – individual | Medical provider – group | |
| mDOT | 1–6 doses/week | ||
| Enhanced social support by patients | Peers – group | ||
| Enhanced education | Weekly educational session | ||
| Enhanced side effect management | Nurse – individual | Weekly group treatment |
Self-administered individual treatment (SIT)
Subjects randomized to SIT received all medications at the clinic from the clinic nurse, packaged in 7-day blister packs (oral medications). Medication were dispensed either weekly, biweekly, or monthly based on provider preference. In this arm, all medications are self-administered at home. For the subjects who received IFN early in the trial (10/29/13 – last date subject receiving IFN/SOF/RBV completed treatment), they were instructed on proper administration. The provider administered the first injection, and the subject administered the second injection under provider observation. The remainders of the doses were provided in a box containing a month’s supply of IFN.
Modified DOT intervention arm (mDOT)
Subjects randomized to the mDOT arm received DOT during methadone visits. Since DOT of HCV medications was linked to methadone visits, the number of directly observed oral doses varied based on the number of days the patient attended the clinic to receive directly observed methadone (pick-up schedule). Depending on methadone pick-up schedule and dosing frequency, certain doses could not be observed (i.e., weekend doses, evening doses, and doses to be taken on a non-clinic day). In these instances, participants were given blister packs that include “take home doses,” for each unobserved dose, and were asked to return the blister pack at the next study visit, whether or not they took the pills. This intervention was considered modified DOT (mDOT) since initially only 3 to 6 out of 14 weekly TVR, 14 weekly RBV, and 7 weekly SOF, SMV, or LDV doses were observed. As subjects moved to once daily medications, subjects on more reduced pick-up schedules (once or twice weekly) were included within the trial as the frequency of reduced doses remained similar (14% - 29% observed doses for subjects on 1–2× weekly PUS for once daily regimens versus 21% observed doses for subjects on 3× PUS for twice daily regimens). Methadone clinic nurses notified clinicians when doses were declined, assessed for side effects, and referred subjects to onsite clinicians as necessary.
Group treatment (GT)
We developed this model by adapting models linking HCV support with treatment [25–27] and models of group medical visits across many chronic conditions [28–30]. Subjects had orientation meetings, which were the first opportunity for subjects to meet as a group and interact with each other and the treatment team (physician and physician assistant). Subjects introduced themselves and shared concerns about HCV. The treatment team presented an overview of the HCV epidemic and its impact on drug users, natural history of HCV, and risks, benefits, and efficacy of HCV treatment. The group treatment protocol and schedule was discussed, and time was allowed for questions and discussion. Weekly CGT meetings had 6 components: 1) brief physical exams; 2) psychosocial support from peers and providers; 3) education; 4) side effect management; and 5) closing meditation on positive health. Six to 12 patients attended the groups, and entry in the groups occurred in a rolling fashion.
Adherence measures
We used self-report and Med-ic® blister pack technology for RBV and DAA adherence in all three arms. Self-reported adherence was measured using a modified AIDS Clinical Trials questionnaire adapted for IFN, RBV and DAAs, as well as a single-item visual analogue scale (VAS) which has been shown to correlate well with both pill counts and virological outcomes in HIV-infected patients taking ART [31, 32]. Med-ic® is an innovative stick-on paper label for medication blisters that provides a disposable method to measure adherence [33]. Adherence is calculated by dose openings divided by total number of prescribed doses over thr different time intervals: 1) weekly adherence: patient receive credit if dose/s taken during the specified week; 2) daily: patient receives credit if dose/s taken during the specified day; 3) daily window adherence: patient receives credit if dose/s taken within the window period based on 25% of the dosing interval. For example a patient who is prescribed twice daily ribavirin 10 AM and 10 PM would get credit if morning dose were taken between 7 AM and 3 PM and evening dose was taken betweem 7 PM and 1 AM. A patient who is scheduled to take once daily medication at 10 AM would receive credit if dose taken between 4 AM and 4 PM. Treatment completion was defined as those who completed at least 80% of the duration of treatment.
Virologic assessments
We obtained data on HCV VL tests performed at 4 weeks, 12 or 24 weeks (end of treatment response) through medical chart review. SVR was determined with a VL test 12 weeks after HCV treatment completion or discontinuation [19]. A VL test was also conducted at 24 weeks following treatment completion, which was the standard for assessing SVR prior to the introduction of DAAs [34]. Quantitative HCV VLs were performed using the Roche COBAS Ampliprep/Taqman assay, which quantifies HCV VL 43 IU/mL to 100 million IU/mL. After 10/9/14, we used COBAS Ampliprep/Taqman assay v2.0, which quantifies HCV VL 15 IU/mL to 100 million IU/mL. DoSA conducts annual HIV testing for all patients (unless they opt out) who are not already known to be HIV-positive. In addition, patients initiating on-site HCV treatment undergo HIV tests as part of our standard treatment protocol. For subjects without HCV VL tests in the chart, study sample was sent to the same laboratory for HCV VL testing.
Psychosocial measures
Psychosocial domains and instruments are listed in Table 2. The full Audio Computer-Assisted Self-Interview (ACASI) takes between two and four hours to complete, and is administered at baseline. An abbreviated ACASI is administered at all other research visits.
Table 2.
Schedule of research visits
| Data Sources | Pre-Baseline | Baseline | Wk0 | Wk4 | Wk8 | Wk12 | Wk24 | Final Tx Wk | FU Wk4 |
FU Wk12 |
FU Wk24 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Blood Tests | |||||||||||
| HCV Viral Load | X | X | X | X | X | X | X | X | X | ||
| Resistance Tests (NS3/4A, NS5A, NS5B Assays) |
X | X | X | X | X | X | |||||
| Other Clinical Measures | |||||||||||
| Urine Toxicology (amphetamine, benzos, cocaine, methadone, opiates, oxycodone) | X | X | X | X | X | X | X | X | X | ||
| Methadone dose | X | X | X | X | X | X | |||||
| Chart Abstraction | X | X | |||||||||
| Blister Pack | X | X | X | X | X | ||||||
| Questionnaires (ACASI) | |||||||||||
| Demographics | X | ||||||||||
| Adherence [32, 66, 67] | X | X | X | X | X | ||||||
| ACTG for Interferon if used [31] | X | X | X | X | X | ||||||
| Awareness of Viral Load questions | X | X | X | X | X | X | X | ||||
| Quality of Life: EQ-5D-3 L [38, 68], HCV QoL [69, 70] | X | X | X | X | X | X | X | X | |||
| Depression: BDI-II [71, 72] | X | X | X | X | X | X | X | X | |||
| Healthcare Service Utilization (NMOS) [73] | X | X | X | X | X | X | X | X | |||
| Alcohol: AUDIT [74] | X | X | X | X | X | X | X | X | |||
| Drug and Alochol Use: ASI-Lite [75, 76] | X | X | X | X | X | X | X | X | |||
| Tobacco Questionnaire [77] | X | X | |||||||||
| Social Support: Norbeck Social Support Questionnaire [78], MOS [79] | X | X | X | X | X | X | |||||
| IMB Questions [80, 81] | X | X | |||||||||
| HCV Beliefs | X | X | |||||||||
| Common Sense Model Questions [82] | X | X | |||||||||
| Psychiatric comorbidities: MINI [83] | X | ||||||||||
| Trust in physician [84] | X | ||||||||||
| Distrust in Health Care System [85] | X | ||||||||||
| Trust in Health Care Provider [86] | X | ||||||||||
| Subjective Opiate Withdrawal Scale [87] | X | X | X | X | X | X | X | X | |||
| Side Effects Survey | X | X | X | X | X | X | |||||
Cost
Costs of HCV treatment were collected by conducting chart reviews and assigning unit costs to all provider visits, lab tests, and medications based on Medicare fee schedules. The cost of the mDOT intervention was determined by conducting brief interviews with medical providers to estimate additional provider and patient time required for mDOT, using prevailing national wage rates to determine the cost of the time, and applying this cost to each DOT interaction. Patient time costs were valued based on the minimum wage, because most patients are likely to be unemployed. The cost of the GT intervention was similarly determined through activity logs that document the number of patients attending each session and the provider time per patient, as well as expense logs that were maintained for transportation and other incidental costs. Provider time spent on research activities, such as conducting research visit assessments, was excluded. We also examined the cost of health care services received outside of the study (emergency department visits, hospitalizations, substance abuse treatment) based on participant self-reports in the ACASI.
Planned statistical analyses
The success of randomization will be checked by comparing key baseline covariates among the mDOT, GT, and SIT groups. If unbalanced covariates are identified, they will be adjusted for in the statistical analysis. We will apply Chi-square or Fisher’s exact tests to compare the proportion of subjects who achieve high overall adherence rate (≥ 80%), complete treatment, achieve SVR, and develop resistance in the 3 arms. If the omnibus equality test of adherence across the 3 groups is rejected, we will conduct the following 2 specific post-hoc pairwise tests with a Bonferroni adjusted 2-sided alpha = 0.025: mDOT vs. control, and GT vs. control. This strategy will be applied to multivariable logistic regressions to adjusted for the potential confounding variables not equally distributed between the study arms at baseline.
For the analysis of repeatedly measured adherence (using 6 post-baseline time points and adherence as a continuous measure), we will apply mixed effects linear model to test if the 3 groups are significantly different. The model will also include potential confounding variables. Again, if the omnibus equality test is rejected, we will conduct the 2 post-hoc pairwise tests described above. Likewise, we will apply mixed effects logistic regression to test the significance of mDOT and GT on repeatedly-measured undetectable HCV VL throughout the intervention period, adjusting for substance use. Changes in illicit drug use will be analyzed using urine toxicology data from each visit, counting the “person-month” as a unit of analysis, and analyzing the proportion of person-months that are positive for use of illicit drugs using a chi-square analysis.
As secondary analyses, we will examine if mDOT and GT effects, vs. SIT, will be mediated by IMB components. We will assess IMB model mediators of adherence at baseline, and during the intervention, and will analyze changes in those variables from the baseline to the intervention period. The indirect effects of IMB mediators will be tested by assessing changes in coefficients of the intervention effect (mDOT or GT) with and without IMB component(s) in mixed effects models. Confidence intervals of the mediated effects will be calculated by bootstrapping, and mediation assumed if confidence intervals do not include zero.
The proportion of participants who develop resistance will be determined with 95% confidence interval (CIs) calculated using exact binomial methods. The proportion of participants with resistance will then be determined within each of 4 groups determined by quartiles of adherence measured at the final time point in the study. We will apply multivariable exact logistic regression models to estimate odds ratios for resistance with the first quartile group as the referent.. To examine whether the relationship between adherence and resistance is linear, we will test a linearity of trends in odds ratios. If this linear trend is not significant, we will identify a quartile group that is associated with the highest odds of resistance.
Cost and cost-effectiveness analyses
To project future HCV costs and life expectancy, we will adapt the Hepatitis C Cost-Effectiveness model (HEP-CE), a Monte Carlo simulation model of HCV disease progression and treatment [35, 36]. The model simulates chronic HCV with fibrosis progression through each of the Metavir stages of liver fibrosis and decompensated cirrhosis. At all stages, HCV infection is associated with increased resource utilization and decreased quality of life (QOL) [37–39]. When HCV infection reaches the stage of cirrhosis (metavir F4), individuals begin to experience increased mortality attributable to liver disease [40]. With successful HCV therapy, disease progression halts, and mortality, resource utilization, and quality of life returns to that of HCV un-infected individuals [41]. HCV-related QOL is stratified by fibrosis stage, and costs of chronic HCV care (such as hospitalizations, ED visits, and clinic visits) are identified separately for patients with and without cirrhosis and stratified by age and sex.
We will populate the model with data collected by PREVAIL including cohort characteristics (demographics and fibrosis stage at baseline), treatment outcomes (rates of treatment toxicity and default, and proportion achieving SVR) and costs. We will explore the potential impact of resistance mutations by varying the efficacy of subsequent HCV retreatment for patients with resistance who choose to be retreated.
We will estimate the cost-effectiveness. of the 3 interventions: SIT, mDOT, and GT, assuming a lifetime horizon, health sector budgetary perspective, and 3% annual discounting to both costs and benefits [42]. We will interpret incremental cost-effectiveness ratios (ICER) assuming a $100,000/QALY willingness to pay threshold [43, 44]. To explore uncertainties in our results, we will perform one and 2-way sensitivity analyses on key input variables and probabilistic sensitivity analyses (PSAs) using second order Monte Carlo simulation on multiple variables [45].
Discussion
This is the first RCT comparing two innovative HCV treatment strategies with self-administered individual treatment in an OAT program. This study will provide valuable information on optimal models of care to promote adherence and reduce viral resistance among PWID from effectiveness and cost perspectives. Understanding these factors will be crucial to addressing the HCV epidemic in this high-risk population.
There have been several operational challenges over the course of the trial due to rapid advances in HCV therapies from IFN-containing to IFN-free DAA regimens, as well as diagnostic modalities. These advances had several important implications for our study design and analysis. Since a heterogeneous study population would decrease our power to detect differences in SVR between treatment arms, we incorporated HIV positivity as a criterion for stratification in our randomization process. As efficacy became comparable with SOF-based regimens among HIV-infected and uninfected patients [46], HIV-positivity remained a criterion for stratification, which we will control for in our analysis.
Similarly, the IL28B genotype affected responses to HCV therapy in the IFN-era. Therefore, we also used IL28B (C/C vs. C/T or T/T) as a criterion for stratification. Since IL28B explained much of the variability in response between African Americans and non-African Americans [20, 47], and rates of SVR with triple therapy were shown to be equivalent in Latinos and non-Latino Whites [21], we did not stratify by race or ethnicity. We continue to stratify by IL28B; however, since the emergence of SOF-based regimens it is no longer a significant predictors of SVR. Thus, we do not anticipate this will be a factor influencing response to therapy within or between treatment arms.
Fibroscan technology became more widely available while the trial was being conducted. Fibroscan yields greater sensitivity and specificity to assess for severe fibrosis. We began using fibroscan technology to stratify our study participants on 8/14/15. We do not anticipate this will result in difference in stratification since fibroscans are widely comparable to liver biopsy and other non-invasive testing [48, 49].
Another advance that was introduced in this trial was electronic blister pack technology to monitor DAA adherence. In the IFN-era, strict adherence to IFN and RBV therapy was necessary to optimize SVR rates. Studies demonstrated that patients who adhere to at least 80% of the intended treatment schedule (taking at least 80% of the total dose of both IFN and ribavirin for at least 80% of the intended duration) were more likely to achieve an SVR [50–52]. Some studies suggested that ribavirin exposure was particularly important in determining response to HCV treatment; supporting the concept that adherence to daily oral medications required unique interventions [53, 54].
The study was originally powered (> 80%) to detect differences using SVR rates in the IFN era (with TVR or BOC). At that time, we anticipated that SVR rates in the mDOT and GT arms would be ≥70%, and ≤40% in the SIT arm [25, 55, 56]. With SOF-based regimens, which are taken orally daily, the effect-sizes are smaller; however, the latter are not currently known.
In the DAA era, due to the risk of viral resistance, adherence remains a critical issue [57]. Yet, there are currently no data describing associations between DAA adherence and virologic outcomes. Therefore, optimal adherence to DAA regimens is currently not known. Accurate measurement of adherence will be a critical issue to understand the direct effect of adherence on treatment failure. Previous RCTs have focused on DOT pegylated-IFN injections and RBV, but these trials have utilized diaries and pill counts for all medications [55, 58, 59]. We utilized electronic blister packs in our trial. This innovative technology will build on this literature by investigating adherence as measured by electronic monitors that have been shown to better predict virologic outcomes in HIV-infected population [60–62]. These results will be of particular relevance since two recent trials examined adherence to DAAs (as measured by diaries) among individuals who were on vs. not on OAT without active substance use [59], as well as active drug users on OAT [63]. While these studies demonstrated adherence rates were similar in these groups, the direct effect of adherence on virologic failure was not addressed.
This trial will also provide valuable information on the cost and cost-effectiveness of treating HCV in PWID. HCV treatment in PWID has been demonstrated to be cost-effective in various geographic settings [64, 65]. However, there is a paucity of data about the cost-effectiveness of various intensive models of care among PWID that could be used to inform implementation of these models. Given the high cost of DAAs and the importance of PWID as a driver of the HCV epidemic, the impact of findings about the cost-effectiveness of intensive models of care may yield information to guide policy recommendations for this critical population.
Acknowledgements
The authors gratefully acknowledge support received from Gilead Sciences for this study.
Funding
National Institute on Drug Abuse (US), R01DA034086 and P30DA0500.
Availability of data and materials
This trial is ongoing so data are not yet available.
Abbreviations
- ACASI
Audio Computer-Assisted Self-Interview
- APRI
AST to Platelet Ratio Index
- BOC
Boceprevir
- DAA
Direct Acting Antiviral
- GT
Group treatment
- HCV
Hepatitis C
- IFN
Interferon
- IMB
Information-Motivation-Behavior
- MDOT
Modified Directly Observed Therapy
- OAT
Opiate Agonist Therapy
- PWID
People who inject drugs
- RBV
Ribavirin
- SIT
Self-administered Individual Treatment
- SOF
Sofosbuvir
- SVR
Sustained virologic response
- TVR
Telaprevir
Authors’ contributions
AHL, BRS, and BPL conceptualized and designed the study. MJA drafted the manuscript. MJA, LA, JHA, MH, BLN, BRS, BPL, AHL provided critical revision and final approval of the version to be published.
Ethics approval and consent to participate
The trial was approved by the Committee on Clinical Investigations of the Albert Einstein College of Medicine and the Institutional Review Board of Montefiore Medical Center (IRB# 2011–555). All participants provided written informed consent.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Matthew J. Akiyama, Email: makiyama@montefiore.org
Linda Agyemang, Email: lagyeman@montefiore.org.
Julia H. Arnsten, Email: jarnsten@montefiore.org
Moonseong Heo, Email: mheo@montefiore.org.
Brianna L. Norton, Email: bnorton@montefiore.org
Bruce R. Schackman, Email: brs2006@med.cornell.edu
Benjamin P. Linas, Email: benjamin.linas@bmc.org
Alain H. Litwin, Email: alitwin@ghs.org
References
- 1.Pearlman BL, Traub N. Sustained virologic response to antiviral therapy for chronic hepatitis C virus infection: a cure and so much more. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2011;52(7):889–900. doi: 10.1093/cid/cir076. [DOI] [PubMed] [Google Scholar]
- 2.Razavi H, Elkhoury AC, Elbasha E, Estes C, Pasini K, Poynard T, Kumar R. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology (Baltimore, Md) 2013;57(6):2164–2170. doi: 10.1002/hep.26218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alter MJ, Kruszon-Moran D, Nainan OV, GM MQ, Gao F, Moyer LA, Kaslow RA, Margolis HS. The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N Engl J Med. 1999;341(8):556–562. doi: 10.1056/NEJM199908193410802. [DOI] [PubMed] [Google Scholar]
- 4.Strathdee SA, Latka M, Campbell J, O’Driscoll PT, Golub ET, Kapadia F, Pollini RA, Garfein RS, Thomas DL, Hagan H, Study to Reduce Intravenous Exposures P Factors associated with interest in initiating treatment for hepatitis C virus (HCV) infection among young HCV-infected injection drug users. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2005;40(Suppl 5):S304–S312. doi: 10.1086/427445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Stein MD, Maksad J, Clarke J. Hepatitis C disease among injection drug users: knowledge, perceived risk and willingness to receive treatment. Drug Alcohol Depend. 2001;61(3):211–215. doi: 10.1016/S0376-8716(00)00144-7. [DOI] [PubMed] [Google Scholar]
- 6.Walley AY, White MC, Kushel MB, Song YS, Tulsky JP. Knowledge of and interest in hepatitis C treatment at a methadone clinic. J Subst Abus Treat. 2005;28(2):181–187. doi: 10.1016/j.jsat.2004.12.004. [DOI] [PubMed] [Google Scholar]
- 7.Mehta SH, Genberg BL, Astemborski J, Kavasery R, Kirk GD, Vlahov D, Strathdee SA, Thomas DL. Limited uptake of hepatitis C treatment among injection drug users. J Community Health. 2008;33(3):126–133. doi: 10.1007/s10900-007-9083-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Grebely J, Raffa JD, Lai C, Krajden M, Kerr T, Fischer B, Tyndall MW. Low uptake of treatment for hepatitis C virus infection in a large community-based study of inner city residents. J Viral Hepat. 2009;16(5):352–358. doi: 10.1111/j.1365-2893.2009.01080.x. [DOI] [PubMed] [Google Scholar]
- 9.Gebo KA, Keruly J, Moore RD. Association of social stress, illicit drug use, and health beliefs with nonadherence to antiretroviral therapy. J Gen Intern Med. 2003;18(2):104–111. doi: 10.1046/j.1525-1497.2003.10801.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tucker JS, Burnam MA, Sherbourne CD, Kung FY, Gifford AL. Substance use and mental health correlates of nonadherence to antiretroviral medications in a sample of patients with human immunodeficiency virus infection. Am J Med. 2003;114(7):573–580. doi: 10.1016/S0002-9343(03)00093-7. [DOI] [PubMed] [Google Scholar]
- 11.Wagner JH, Justice AC, Chesney M, Sinclair G, Weissman S, Rodriguez-Barradas M, Team VP Patient- and provider-reported adherence: toward a clinically useful approach to measuring antiretroviral adherence. J Clin Epidemiol. 2001;54(Suppl 1):S91–S98. doi: 10.1016/S0895-4356(01)00450-4. [DOI] [PubMed] [Google Scholar]
- 12.Lucas GM, Cheever LW, Chaisson RE, Moore RD. Detrimental effects of continued illicit drug use on the treatment of HIV-1 infection. J Acquir Immune Defic Syndr. 2001;27(3):251–259. doi: 10.1097/00042560-200107010-00006. [DOI] [PubMed] [Google Scholar]
- 13.Howard AA, Arnsten JH, Lo Y, Vlahov D, Rich JD, Schuman P, Stone VE, Smith DK, Schoenbaum EE, Group HERS. A prospective study of adherence and viral load in a large multi-center cohort of HIV-infected women. AIDS 2002;16(16):2175-2182. PubMed PMID: 12409739. [DOI] [PubMed]
- 14.Golin CE, Liu H, Hays RD, Miller LG, Beck CK, Ickovics J, Kaplan AH, Wenger NS. A prospective study of predictors of adherence to combination antiretroviral medication. J Gen Intern Med. 2002;17(10):756–765. doi: 10.1046/j.1525-1497.2002.11214.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fisher JD, Fisher WA, Amico KR, Harman JJ. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006;25(4):462–473. doi: 10.1037/0278-6133.25.4.462. [DOI] [PubMed] [Google Scholar]
- 16.Amico KR, Toro-Alfonso J, Fisher JD. An empirical test of the information, motivation and behavioral skills model of antiretroviral therapy adherence. AIDS Care. 2005;17(6):661–673. doi: 10.1080/09540120500038058. [DOI] [PubMed] [Google Scholar]
- 17.Starace F, Massa A, Amico KR, Fisher JD. Adherence to antiretroviral therapy: an empirical test of the information-motivation-behavioral skills model. Health Psychol. 2006;25(2):153–162. doi: 10.1037/0278-6133.25.2.153. [DOI] [PubMed] [Google Scholar]
- 18.Stein MR, Soloway IJ, Jefferson KS, Roose RJ, Arnsten JH, Litwin AH. Concurrent group treatment for hepatitis C: implementation and outcomes in a methadone maintenance treatment program. J Subst Abus Treat. 2012;43(4):424–432. doi: 10.1016/j.jsat.2012.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.American Association for the Study of Liver Diseases, Infectious Diseases Society of America . Recommendations for testing, managing, and treating hepatitis C. 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, Heinzen EL, Qiu P, Bertelsen AH, Muir AJ, Sulkowski M, McHutchison JG, Goldstein DB. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461(7262):399–401. doi: 10.1038/nature08309. [DOI] [PubMed] [Google Scholar]
- 21.Jacobson IM, McHutchison JG, Dusheiko G, Di Bisceglie AM, Reddy KR, Bzowej NH, Marcellin P, Muir AJ, Ferenci P, Flisiak R, George J, Rizzetto M, Shouval D, Sola R, Terg RA, Yoshida EM, Adda N, Bengtsson L, Sankoh AJ, Kieffer TL, George S, Kauffman RS, Zeuzem S, Team AS. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med 2011;364(25):2405-2416. doi: 10.1056/NEJMoa1012912. PubMed PMID: 21696307. [DOI] [PubMed]
- 22.Terrault NA, Zeuzem S, Di Bisceglie AM, Lim JK, Pockros PJ, Frazier LM, Kuo A, Lok AS, Shiffman ML, Ben Ari Z, Akushevich L, Vainorius M, Sulkowski MS, Fried MW, Nelson DR, Group H-TS Effectiveness of Ledipasvir-Sofosbuvir combination in patients with hepatitis C virus infection and factors associated with sustained Virologic response. Gastroenterology. 2016;151(6):1131–40 e5. doi: 10.1053/j.gastro.2016.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, Lok AS. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology (Baltimore, Md) 2003;38(2):518–526. doi: 10.1053/jhep.2003.50346. [DOI] [PubMed] [Google Scholar]
- 24.Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y, Poynard T, Group M Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: a prospective study. Lancet (London, England). 2001;357(9262):1069–1075. doi: 10.1016/S0140-6736(00)04258-6. [DOI] [PubMed] [Google Scholar]
- 25.Sylvestre DL, Litwin AH, Clements BJ, Gourevitch MN. The impact of barriers to hepatitis C virus treatment in recovering heroin users maintained on methadone. J Subst Abus Treat. 2005;29(3):159–165. doi: 10.1016/j.jsat.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 26.Grebely J, Genoway K, Khara M, Duncan F, Viljoen M, Elliott D, Raffa JD, DeVlaming S, Conway B. Treatment uptake and outcomes among current and former injection drug users receiving directly observed therapy within a multidisciplinary group model for the treatment of hepatitis C virus infection. Int J Drug Policy. 2007;18(5):437–443. doi: 10.1016/j.drugpo.2007.01.009. [DOI] [PubMed] [Google Scholar]
- 27.Litwin AH, Soloway I, Gourevitch MN. Integrating services for injection drug users infected with hepatitis C virus with methadone maintenance treatment: challenges and opportunities. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2005;40(Suppl 5):S339–S345. doi: 10.1086/427450. [DOI] [PubMed] [Google Scholar]
- 28.Bronson DL, Maxwell RA. Shared medical appointments: increasing patient access without increasing physician hours. Cleve Clin J Med. 2004;71(5):369–370. doi: 10.3949/ccjm.71.5.369. [DOI] [PubMed] [Google Scholar]
- 29.Jaber R, Braksmajer A, Trilling JS. Group visits: a qualitative review of current research. J Am Board Fam Med. 2006;19(3):276–290. doi: 10.3122/jabfm.19.3.276. [DOI] [PubMed] [Google Scholar]
- 30.Meehan KR, Hill JM, Root L, Kimtis E, Patchett L, Noffsinger EB. Group medical appointments: organization and implementation in the bone marrow transplantation clinic. Support Cancer Ther. 2006;3(2):84–90. doi: 10.3816/SCT.2006.n.003. [DOI] [PubMed] [Google Scholar]
- 31.Chesney MA, Ickovics JR, Chambers DB, Gifford AL, Neidig J, Zwickl B, Wu AW. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: the AACTG adherence instruments. Patient Care Committee & Adherence Working Group of the outcomes Committee of the Adult AIDS Clinical Trials Group (AACTG) AIDS Care. 2000;12(3):255–266. doi: 10.1080/09540120050042891. [DOI] [PubMed] [Google Scholar]
- 32.Kalichman SC, Amaral CM, Swetzes C, Jones M, Macy R, Kalichman MO, Cherry C. A simple single-item rating scale to measure medication adherence: further evidence for convergent validity. J Int Assoc Physicians AIDS Care (Chic) 2009;8(6):367–374. doi: 10.1177/1545109709352884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Information Mediary Corp. [December 1st, 2016]. Available from: http://www.informationmediary.com/med-ic.
- 34.McHutchison JG, Poynard T, Esteban-Mur R, Davis GL, Goodman ZD, Harvey J, Ling MH, Garaud JJ, Albrecht JK, Patel K, Dienstag JL, Morgan T, International hepatitis interventional therapy G. Hepatic HCV RNA before and after treatment with interferon alone or combined with ribavirin. Hepatology (Baltimore, Md). 2002;35(3):688-693. 10.1053/jhep.2002.31870. PubMed PMID: 11870385. [DOI] [PubMed]
- 35.Poynard T, Bedossa P, Opolon P. Natural history of liver fibrosis progression in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet (London, England) 1997;349(9055):825–832. doi: 10.1016/S0140-6736(96)07642-8. [DOI] [PubMed] [Google Scholar]
- 36.Salomon JA, Weinstein MC, Hammitt JK, Goldie SJ. Cost-effectiveness of treatment for chronic hepatitis C infection in an evolving patient population. JAMA. 2003;290(2):228–237. doi: 10.1001/jama.290.2.228. [DOI] [PubMed] [Google Scholar]
- 37.Linas BP, Wang B, Smurzynski M, Losina E, Bosch RJ, Schackman BR, Rong J, Sax PE, Walensky RP, Schouten J, Freedberg KA. The impact of HIV/HCV co-infection on health care utilization and disability: results of the ACTG longitudinal linked randomized trials (ALLRT) cohort. J Viral Hepat. 2011;18(7):506–512. doi: 10.1111/j.1365-2893.2010.01325.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chong CA, Gulamhussein A, Heathcote EJ, Lilly L, Sherman M, Naglie G, Krahn M. Health-state utilities and quality of life in hepatitis C patients. Am J Gastroenterol 2003;98(3):630-638. PubMed PMID: 12650799. [DOI] [PubMed]
- 39.Grieve R, Roberts J, Wright M, Sweeting M, De Angelis D, Rosenberg W, Bassendine M, Main J, Thomas H. Cost effectiveness of interferon alpha or peginterferon alpha with ribavirin for histologically mild chronic hepatitis C. Gut. 2006;55(9):1332–1338. doi: 10.1136/gut.2005.064774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pineda JA, Aguilar-Guisado M, Rivero A, Giron-Gonzalez JA, Ruiz-Morales J, Merino D, Rios-Villegas MJ, Macias J, Lopez-Cortes LF, Camacho A, Merchante N, Del Valle J, Grupo para el Estudio de las Hepatitis Viricas de la Sociedad Andaluza de Enfermedades I Natural history of compensated hepatitis C virus-related cirrhosis in HIV-infected patients. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2009;49(8):1274–1282. doi: 10.1086/605676. [DOI] [PubMed] [Google Scholar]
- 41.Berenguer J, Alvarez-Pellicer J, Martin PM, Lopez-Aldeguer J, Von-Wichmann MA, Quereda C, Mallolas J, Sanz J, Tural C, Bellon JM, Gonzalez-Garcia J, Group GS Sustained virological response to interferon plus ribavirin reduces liver-related complications and mortality in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology (Baltimore, Md) 2009;50(2):407–413. doi: 10.1002/hep.23020. [DOI] [PubMed] [Google Scholar]
- 42.Neumann PJ, Sanders GD. Cost-effectiveness analysis 2.0. N Engl J Med. 2017;376(3):203–205. doi: 10.1056/NEJMp1612619. [DOI] [PubMed] [Google Scholar]
- 43.Neumann PJ, Cohen JT, Weinstein MC. Updating cost-effectiveness--the curious resilience of the $50,000-per-QALY threshold. N Engl J Med. 2014;371(9):796–797. doi: 10.1056/NEJMp1405158. [DOI] [PubMed] [Google Scholar]
- 44.Braithwaite RS, Meltzer DO, King JT, Jr, Leslie D, Roberts MS. What does the value of modern medicine say about the $50,000 per quality-adjusted life-year decision rule? Med Care. 2008;46(4):349–356. doi: 10.1097/MLR.0b013e31815c31a7. [DOI] [PubMed] [Google Scholar]
- 45.Briggs A. Probabilistic analysis of cost-effectiveness models: statistical representation of parameter uncertainty. Value Health. 2005;8(1):1–2. doi: 10.1111/j.1524-4733.2005.08101.x. [DOI] [PubMed] [Google Scholar]
- 46.Chastain CA, Naggie S. Treatment of genotype 1 HCV infection in the HIV coinfected patient in 2014. Curr HIV/AIDS Rep. 2013;10(4):408–419. doi: 10.1007/s11904-013-0182-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Thompson AJ, Muir AJ, Sulkowski MS, Ge D, Fellay J, Shianna KV, Urban T, Afdhal NH, Jacobson IM, Esteban R, Poordad F, Lawitz EJ, Mc Cone J, Shiffman ML, Galler GW, Lee WM, Reindollar R, King JW, Kwo PY, Ghalib RH, Freilich B, Nyberg LM, Zeuzem S, Poynard T, Vock DM, Pieper KS, Patel K, Tillmann HL, Noviello S, Koury K, Pedicone LD, Brass CA, Albrecht JK, Goldstein DB, JG MH. Interleukin-28B polymorphism improves viral kinetics and is the strongest pretreatment predictor of sustained virologic response in genotype 1 hepatitis C virus. Gastroenterology. 2010;139(1):120–9 e18. doi: 10.1053/j.gastro.2010.04.013. [DOI] [PubMed] [Google Scholar]
- 48.Ferraioli G, Tinelli C, Dal Bello B, Zicchetti M, Lissandrin R, Filice G, Filice C, Above E, Barbarini G, Brunetti E, Calderon W, Di Gregorio M, Gulminetti R, Lanzarini P, Ludovisi S, Maiocchi L, Malfitano A, Michelone G, Minoli L, Mondelli M, Novati S, Patruno SF, Perretti A, Poma G, Sacchi P, Zanaboni D, Zaramella M. Performance of liver stiffness measurements by transient elastography in chronic hepatitis. World J Gastroenterol. 2013;19(1):49–56. doi: 10.3748/wjg.v19.i1.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lurie Y, Webb M, Cytter-Kuint R, Shteingart S, Lederkremer GZ. Non-invasive diagnosis of liver fibrosis and cirrhosis. World J Gastroenterol. 2015;21(41):11567–11583. doi: 10.3748/wjg.v21.i41.11567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Mc Hutchison JG, Manns M, Patel K, Poynard T, Lindsay KL, Trepo C, Dienstag J, Lee WM, Mak C, Garaud JJ, Albrecht JK, International Hepatitis Interventional Therapy G Adherence to combination therapy enhances sustained response in genotype-1-infected patients with chronic hepatitis C. Gastroenterology. 2002;123(4):1061–1069. doi: 10.1053/gast.2002.35950. [DOI] [PubMed] [Google Scholar]
- 51.Raptopoulou M, Tsantoulas D, Vafiadi I, Ketikoglou I, Paraskevas E, Vassiliadis T, Kanatakis S, Hatzis G, Sidiropoulos L, Akriviadis E. The effect of adherence to therapy on sustained response in daily or three times a week interferon alpha-2b plus ribavirin treatment of naive and nonresponder chronic hepatitis C patients. J Viral Hepat. 2005;12(1):91–95. doi: 10.1111/j.1365-2893.2005.00549.x. [DOI] [PubMed] [Google Scholar]
- 52.Lo TN, Boyle MD. Relationship between the intracellular cyclic adenosine 3′:5′-monophosphate level of tumor cells and their sensitivity to killing by antibody and complement. Cancer Res. 1979;39(8):3156–3162. [PubMed] [Google Scholar]
- 53.Davis GL, Wong JB, McHutchison JG, Manns MP, Harvey J, Albrecht J. Early virologic response to treatment with peginterferon alfa-2b plus ribavirin in patients with chronic hepatitis C. Hepatology (Baltimore, Md) 2003;38(3):645–652. doi: 10.1053/jhep.2003.50364. [DOI] [PubMed] [Google Scholar]
- 54.Shiffman ML, Suter F, Bacon BR, Nelson D, Harley H, Sola R, Shafran SD, Barange K, Lin A, Soman A, Zeuzem S, Investigators A. Peginterferon alfa-2a and ribavirin for 16 or 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2007;357(2):124–134. doi: 10.1056/NEJMoa066403. [DOI] [PubMed] [Google Scholar]
- 55.Bonkovsky HL, Tice AD, Yapp RG, Bodenheimer HC, Jr., Monto A, Rossi SJ, Sulkowski MS. Efficacy and safety of peginterferon alfa-2a/ribavirin in methadone maintenance patients: randomized comparison of direct observed therapy and self-administration. Am J Gastroenterol 2008;103(11):2757-2765. doi: 10.1111/j.1572-0241.2008.02065.x. PubMed PMID: 18684176. [DOI] [PubMed]
- 56.Feuerstadt P, Bunim AL, Garcia H, Karlitz JJ, Massoumi H, Thosani AJ, Pellecchia A, Wolkoff AW, Gaglio PJ, Reinus JF. Effectiveness of hepatitis C treatment with pegylated interferon and ribavirin in urban minority patients. Hepatology (Baltimore, Md) 2010;51(4):1137–1143. doi: 10.1002/hep.23429. [DOI] [PubMed] [Google Scholar]
- 57.Benitez-Gutierrez L, Barreiro P, Labarga P, de Mendoza C, Fernandez-Montero JV, Arias A, Pena JM, Soriano V. Prevention and management of treatment failure to new oral hepatitis C drugs. Expert Opin Pharmacother. 2016;17(9):1215–1223. doi: 10.1080/14656566.2016.1182156. [DOI] [PubMed] [Google Scholar]
- 58.Litwin AH, Berg KM, Li X, Hidalgo J, Arnsten JH. Rationale and design of a randomized controlled trial of directly observed hepatitis C treatment delivered in methadone clinics. BMC Infect Dis. 2011;11:315. doi: 10.1186/1471-2334-11-315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Grebely J, Mauss S, Brown A, Bronowicki JP, Puoti M, Wyles D, Natha M, Zhu Y, Yang J, Kreter B, Brainard DM, Yun C, Carr V, Dore GJ. Efficacy and safety of Ledipasvir/Sofosbuvir with and without Ribavirin in patients with chronic HCV genotype 1 infection receiving Opioid substitution therapy: analysis of phase 3 ION trials. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016;63(11):1405–11. doi: 10.1093/cid/ciw580. [DOI] [PubMed] [Google Scholar]
- 60.Petersen ML, Wang Y, van der Laan MJ, Guzman D, Riley E, Bangsberg DR. Pillbox organizers are associated with improved adherence to HIV antiretroviral therapy and viral suppression: a marginal structural model analysis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2007;45(7):908–915. doi: 10.1086/521250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Schneider PJ, Murphy JE, Pedersen CA. Impact of medication packaging on adherence and treatment outcomes in older ambulatory patients. J Am Pharm Assoc (2003) 2008;48(1):58–63. doi: 10.1331/JAPhA.2008.07040. [DOI] [PubMed] [Google Scholar]
- 62.Zedler BK, Kakad P, Colilla S, Murrelle L, Shah NR. Does packaging with a calendar feature improve adherence to self-administered medication for long-term use? A systematic review. Clin Ther. 2011;33(1):62–73. doi: 10.1016/j.clinthera.2011.02.003. [DOI] [PubMed] [Google Scholar]
- 63.Dore GJ, Altice F, Litwin AH, Dalgard O, Gane EJ, Shibolet O, Luetkemeyer A, Nahass R, Peng CY, Conway B, Grebely J, Howe AY, Gendrano IN, Chen E, Huang HC, Dutko FJ, Nickle DC, Nguyen BY, Wahl J, Barr E, Robertson MN, Platt HL, Group CEC-SS. Elbasvir-Grazoprevir to treat hepatitis C virus infection in persons receiving Opioid agonist therapy: a randomized trial. Ann Intern Med. 2016; 10.7326/M16-0816. PubMed PMID: 27537841 [DOI] [PubMed]
- 64.Martin NK, Vickerman P, Dore GJ, Grebely J, Miners A, Cairns J, Foster GR, Hutchinson SJ, Goldberg DJ, Martin TC, Ramsay M, Consortium S-H, Hickman M. Prioritization of HCV treatment in the direct-acting antiviral era: an economic evaluation. J Hepatol. 2016;65(1):17–25. doi: 10.1016/j.jhep.2016.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Scott N, Iser DM, Thompson AJ, Doyle JS, Hellard ME. Cost-effectiveness of treating chronic hepatitis C virus with direct-acting antivirals in people who inject drugs in Australia. J Gastroenterol Hepatol. 2016;31(4):872–882. doi: 10.1111/jgh.13223. [DOI] [PubMed] [Google Scholar]
- 66.Restrictions on Medicaid abortions blocked temporarily, but situation could change soon. Fam Plann Popul Rep. 1978;7(5):73–5. PubMed PMID: 11663989 [PubMed]
- 67.Genberg BL, Lee Y, Rogers WH, Willey C, Wilson IB. Stages of change for adherence to antiretroviral medications. AIDS Patient Care STDs. 2013;27(10):567–572. doi: 10.1089/apc.2013.0126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann Med 2001;33(5):337-343. PubMed PMID: 11491192. [DOI] [PubMed]
- 69.Ware JE, Jr, Bayliss MS, Mannocchia M, Davis GL. Health-related quality of life in chronic hepatitis C: impact of disease and treatment response. The interventional therapy group. Hepatology (Baltimore, Md) 1999;30(2):550–555. doi: 10.1002/hep.510300203. [DOI] [PubMed] [Google Scholar]
- 70.Foster GR. Quality of life considerations for patients with chronic hepatitis C. J Viral Hepat. 2009;16(9):605–611. doi: 10.1111/j.1365-2893.2009.01154.x. [DOI] [PubMed] [Google Scholar]
- 71.Dozois D, Dobson K, Ahnberg J. A psychometric evaluation of the Beck depression inventory–II. Psychol Assess. 1998;10(2):83–89. doi: 10.1037/1040-3590.10.2.83. [DOI] [Google Scholar]
- 72.Johnson ME, Neal DB, Brems C, Fisher DG. Depression as measured by the Beck depression inventory-II among injecting drug users. Assessment. 2006;13(2):168–177. doi: 10.1177/1073191106286951. [DOI] [PubMed] [Google Scholar]
- 73.Chandler RK, Kahana SY, Fletcher B, Jones D, Finger MS, Aklin WM, Hamill K, Webb C. Data collection and harmonization in HIV research: the seek, test, treat, and retain initiative at the National Institute on Drug Abuse. Am J Public Health. 2015;105(12):2416–2422. doi: 10.2105/AJPH.2015.302788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption--II. Addiction. 1993;88(6):791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- 75.Cacciola JS, Alterman AI, McLellan AT, Lin YT, Lynch KG. Initial evidence for the reliability and validity of a “Lite” version of the addiction severity index. Drug Alcohol Depend. 2007;87(2–3):297–302. doi: 10.1016/j.drugalcdep.2006.09.002. [DOI] [PubMed] [Google Scholar]
- 76.McGahan P, Griffith J, Parente R, McLellan A. Addiction severity index composite scores manual. 1986. [Google Scholar]
- 77.Centers for Disease Control. 2013. Available from: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_questions.htm.
- 78.Norbeck JS, Lindsey AM, Carrieri VL. Further development of the Norbeck social support questionnaire: normative data and validity testing. Nurs Res. 1983;32(1):4–9. doi: 10.1097/00006199-198301000-00002. [DOI] [PubMed] [Google Scholar]
- 79.Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32(6):705–714. doi: 10.1016/0277-9536(91)90150-B. [DOI] [PubMed] [Google Scholar]
- 80.Canfield KM, Smyth E, Batki SL. Methadone maintenance patients’ knowledge, attitudes, beliefs, and experiences concerning treatment for hepatitis C virus infection. Subst Use Misuse. 2010;45(4):496–514. doi: 10.3109/10826080903452538. [DOI] [PubMed] [Google Scholar]
- 81.Strauss SM, Astone-Twerell J, Munoz-Plaza CE, Des Jarlais DC, Gwadz M, Hagan H, Osborne A, Rosenblum A. Drug treatment program patients’ hepatitis C virus (HCV) education needs and their use of available HCV education services. BMC Health Serv Res. 2007;7:39. doi: 10.1186/1472-6963-7-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Krauskopf K, McGinn TG, Federman AD, Halm EA, Leventhal H, McGinn LK, Gardenier D, Oster A, Kronish IM. HIV and HCV health beliefs in an inner-city community. J Viral Hepat. 2011;18(11):785–791. doi: 10.1111/j.1365-2893.2010.01383.x. [DOI] [PubMed] [Google Scholar]
- 83.Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC. The Mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33. [PubMed] [Google Scholar]
- 84.Anderson LA, Dedrick RF. Development of the Trust in Physician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol Rep. 1990;67(3 Pt 2):1091–1100. doi: 10.2466/pr0.1990.67.3f.1091. [DOI] [PubMed] [Google Scholar]
- 85.Altice FL, Mostashari F, Friedland GH. Trust and the acceptance of and adherence to antiretroviral therapy. J Acquir Immune Defic Syndr. 2001;28(1):47–58. doi: 10.1097/00042560-200109010-00008. [DOI] [PubMed] [Google Scholar]
- 86.Safran DG, Taira DA, Rogers WH, Kosinski M, Ware JE, Tarlov AR. Linking primary care performance to outcomes of care. J Fam Pract. 1998;47(3):213–220. [PubMed] [Google Scholar]
- 87.Handelsman L, Cochrane KJ, Aronson MJ, Ness R, Rubinstein KJ, Kanof PD. Two new rating scales for opiate withdrawal. Am J Drug Alcohol Abuse. 1987;13(3):293–308. doi: 10.3109/00952998709001515. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This trial is ongoing so data are not yet available.