

Abstract
Background:
Body-powered prostheses require cable operation forces between 33 and 131 N. The accepted upper limit for fatigue-free long-duration operation is 20% of a users’ maximum cable operation force. However, no information is available on users’ maximum force.
Objectives:
To quantify users’ maximum cable operation force and to relate this to the fatigue-free force range for the use of body-powered prostheses.
Study design:
Experimental trial.
Methods:
In total, 23 subjects with trans-radial deficiencies used a bypass prosthesis to exert maximum cable force three times during 3 s and reported discomfort or pain on a body map. Additionally, subjects’ anthropometric measures were taken to relate to maximum force.
Results:
Subjects generated forces ranging from 87 to 538 N. Of the 23 subjects, 12 generated insufficient maximum cable force to operate 8 of the 10 body-powered prostheses fatigue free. Discomfort or pain did not correlate with the magnitude of maximum force achieved by the subjects. Nine subjects indicated discomfort or pain. No relationships between anthropometry and maximal forces were found except for maximum cable forces and the affected upper-arm circumference for females.
Conclusion:
For a majority of subjects, the maximal cable force was lower than acceptable for fatigue-free prosthesis use. Discomfort or pain occurred in ~40% of the subjects, suggesting a suboptimal force transmission mechanism.
Clinical relevance
The physical strength of users determines whether a body-powered prosthesis is suitable for comfortable, fatigue-free long-duration use on a daily basis. High cable operation forces can provoke discomfort and pain for some users, mainly in the armpit. Prediction of the users’ strength by anthropometric measures might assist the choice of a suitable prosthesis.
Keywords: Upper-limb prosthetics, body-powered prosthesis, cable operation force
Background
Body-powered prostheses are rejected by 26%–45% of the users.1 One of the reasons for rejection is the high operating force required for prosthesis activation,2,3 leading to pain or fatigue or, in the worst case, nerve and vessel damage.1,4 Required operating forces to pinch 15 N with a voluntary closing prosthesis vary between 33 and 131 N.2 For a 50-mm opening of voluntary opening prostheses, which are able to pinch at least 15 N, cable forces between 50 and 94 N are required.3 Using a prosthesis on a daily basis implies that the user should not feel tired after a number of manipulations and should also not experience any pain (e.g. sore muscles and pinching) during or after use. Humans can conduct isometric contractions without fatigue effects at a critical force level of 15%–20% of their maximum voluntary contraction.5 Hence, taking the conservative value and maintaining 20% of users’ maximum cable operation force as an upper boundary for daily use will enable users to operate their body-powered prosthesis fatigue free.
However, the user’s maximum cable forces (MCFs) have never been quantified. Current research is based on measurements on 50 “normal” subjects by Taylor6 in 1954, who measured cable forces of 280 (24) N (mean (standard deviation)) for arm flexion, 270 (106) N for shrug, and 251 (29) N for arm extension. Unfortunately, the measurement procedure and the subject characteristics were not described. Moreover, the study reported forces and displacements from isolated movements instead of combinations of movements typically used for body-powered prosthesis operation. A recent unpublished pilot experiment on 10 male controls (28 (2) years old; mean (standard deviation)) revealed average values of 475 N and a peak value of 970 N for one subject, which are significantly higher than the reported values of Taylor.6
Prosthesis user strength will probably show a large variety, resulting in a challenge for the clinical team to find the best individual suitable prosthesis. Predicting maximum cable operation forces by anthropometric measures might facilitate the prosthesis fitting procedure and prevent the need for costly measurement equipment. Furthermore, although discomfort has been reported for body-powered prosthesis operation,1,4 extent and locations of discomfort have never been related to the exerted cable forces.
This study aims to quantify users’ maximum cable operation forces and to relate these to a fatigue-free force range for the use of body-powered prostheses. In addition, we aim to identify extent and locations of discomfort provoked by the exertion of cable forces and to explore the predictability of maximum cable operation forces by the anthropometric measures of users.
Methods
This study was approved by the medical ethical committee of University Medical Center Groningen (UMCG). The subjects were recruited from UMCG, Erasmus Medical Center, Rotterdam, and the rehabilitation institute De Hoogstraat, Utrecht.
Subjects
In total, 23 adults (11 males, age: 49 (13) years) with a unilateral trans-radial deficiency participated (Table 1). All participants were free of neurological, muscle, joint, or motor control problems concerning the upper extremity or the torso (exclusion criteria). In total, 9 participants had a right deficiency, 14 had a congenital defect, and 11 had experience with body-powered prostheses.
Table 1.
Overview of the subject characteristics.
| Subject no. | Gender | Age | Acquired/congenital defect | Affected side | Dominant side | Currently used prosthesis | Experience in body-powered prosthesis use | Frequency of prosthesis use |
|---|---|---|---|---|---|---|---|---|
| 9 | Female | 54 | Acquired | Left | Right | Myo | No | Daily use |
| 11 | 60 | Right | Right | Myo | No | Daily use | ||
| 14 | 69 | Left | Right | Myo and body-powered | Yes | Daily use | ||
| 2 | 20 | Congenital | Left | Right | None | No | Never | |
| 4 | 43 | Left | Left | Cosmetic | Yes | Use for specific tasks | ||
| 8 | 46 | Left | Right | Myo | No | Use for specific tasks | ||
| 12 | 52 | Right | Right | Cosmetic | No | Use for specific tasks | ||
| 17 | 43 | Right | Left | Cosmetic | Yes | Use for specific tasks | ||
| 18 | 34 | Left | Left | None, only fork on socket | Yes | Use for specific tasks | ||
| 19 | 58 | Left | Right | None | No | Got one, but never wore it | ||
| 7 | 49 | Left | Right | Body-powered | Yes | Daily use | ||
| 10 | 54 | Right | Left | Myo | Yes | Daily use | ||
| 1 | Male | 57 | Acquired | Left | Right | Myo | No | Daily use |
| 3 | 68 | Right | Right | Myo and cosmetic | No | Daily use | ||
| 6 | 35 | Left | Right | Myo | No | Daily use | ||
| 16 | 50 | Left | Left | Myo | No | Daily use | ||
| 20 | 68 | Right | Right | Myo | Yes | Daily use | ||
| 23 | 49 | Left | Right | Myo and body-powered | Yes | Daily use | ||
| 13 | 47 | Congenital | Right | Right | None | No | Got one, but never wore it | |
| 5 | 63 | Left | Right | Myo | No | Daily use | ||
| 15 | 25 | Right | Right | Myo | Yes | Daily use | ||
| 21 | 37 | Right | Right | Myo | Yes | Daily use | ||
| 22 | 55 | Left | Left | Myo | Yes | Daily use |
Subjects are sorted by gender and the cause of their arm defect.
Materials
Maximum force measurements
A custom-made prosthesis simulator (Figure 1) was connected by the experimenter to the participant’s prosthesis. For two participants who did not own a prosthesis, the prosthesis simulator was placed on a temporary WILMER Open Socket.7 For two other participants, the bypass prosthesis was attached to the remnant arm since its length was sufficient for a firm connection. The prosthesis simulator consisted of an adjustable “figure-of-nine” harness linked to a standard 1/16″ (0.159 cm) diameter stainless steel cable (C100; Hosmer Dorrance Corporation, Chattanooga, TN). Cable excursions were disabled in this setup. The Bowden cable was interrupted by a force sensor (S-Beam load cell ZFA 100 kg; Scaime, Juvigny, France). The measured forces were amplified (CPJ; Scaime), sampled at 1 kHz (NI USB-6008; National Instruments, Austin, TX), and finally stored using a custom LabVIEW program (LabVIEW 2012; National Instruments).
Figure 1.
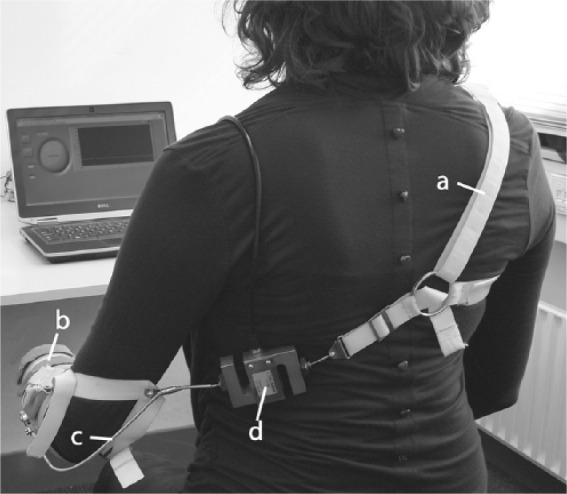
Measurement setup for maximum force measurements: (a) the “figure-of-nine” harness and (b) thermoplastic shell are connected through a (c) Bowden cable, which is interrupted by a (d) force sensor. In this setup, cable excursions are disabled.
Anthropometric data
The subject’s shoulder width, upper-arm length, and remaining lower-arm length were measured by the experimenter with an anthropometer (Model 101; GPM, Zurich, Switzerland). The upper-arm circumference was measured with a sewing tape.
Procedure
After signing an informed consent form, the anthropometric data were taken following the instructions of the NASA Reference Publication 1024:8 103, biacromial breadth; 751, shoulder–elbow length: 113, biceps circumference, relaxed; 381, forearm–hand length (the fingertips are represented by the far end of the subjects’ stump). Then, a prosthetic simulator was connected to the subjects’ prosthesis. The subject was instructed to use their preferred combination of shoulder protraction of the sound side, humeral abduction, and forward flexion on the affected side to create cable forces. Before starting the measurements, the subjects were allowed trial movements until they felt familiar with exerting forces on the control cable. Subjects were asked to deliver their maximal cable forces within 3 s. This was repeated three times. The 3-s time interval was chosen based on trial measurements, testing how much time is required to achieve the maximum force. The trial measurements were done with able-bodied subjects. Finally, subjects were requested to report locations of pain or discomfort on a body map (Figure 2) after completing the experiment.
Figure 2.
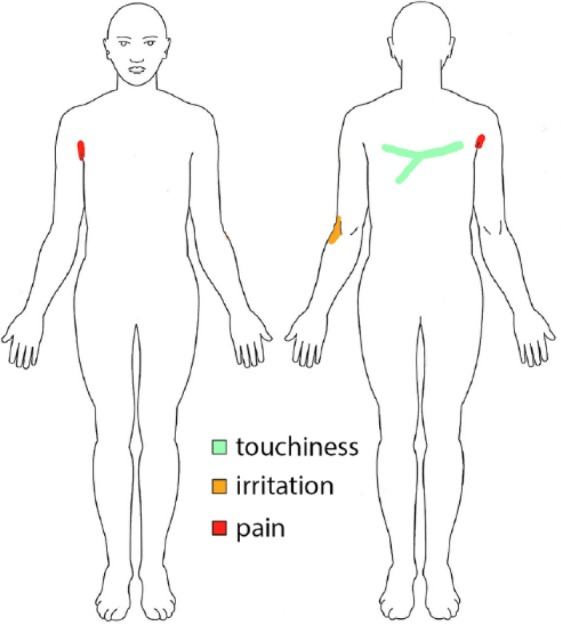
Body map colored by one subject indicating pain in the right armpit, irritation at the back of the left elbow, and touchiness on a stripe of his back.
Data analysis
Maximum force measurements
The highest values of the three maximum force measurements were determined. Only trials where the maximum force was attained within the predetermined 3 s were included (56 of 69 trials).
The subjects’ MCFs and fatigue limits were compared to the required forces to (1) create a 15-N pinch force with a voluntary closing prostheses2 and (2) achieve a 50-mm prehensor opening with voluntary opening prostheses, which is capable to pinch at least 15 N3 (Table 2).
Table 2.
Required cable forces to operate voluntary closing and opening prostheses.
| Voluntary closing prostheses | Required cable force (N) to create a 15-N pinch force2 | Voluntary opening prostheses | Required cable force (N) to achieve a 50-mm prehensor opening3 |
|---|---|---|---|
| TRS Hook, Grip 2S | 33 | Hosmer Hook 5XA, 2 bands | 50 |
| Hosmer APRL Hand, 52541 | 61 | Hosmer Sierra Hand, ungloved | 70 |
| Hosmer APRL Hook, 52601 | 62 | Hosmer Hook 5XA, 3 bands | 71 |
| Otto Bock Hand, 8K24 | 98 | Hosmer Sierra Hook, setting 2 | 82 |
| Hosmer Soft Hand, 61794 | 131 | Otto Bock Hook, setting 2 | 94 |
Body maps
The body maps were inspected visually and were summarized in the highest discomfort intensity and its affected body part by the experimenter. The analysis procedure and results for different subjects were discussed with the other authors.
Statistics and prediction of maximum forces
For statistical analysis, SPSS version 20 was used, and a significance level of α = 0.05 was maintained. Gender effects for the force magnitude were analyzed with a paired sample t-test. A linear multiple regression analysis was conducted to predict the maximum forces body-powered prosthesis users can create on the control cable from (1) shoulder width, arm circumferences, upper-arm length of the affected arm, and remnant length as well as (2) gender, experience in body-powered prosthesis use, and cause of defect.
Results
The maximum cable operation force averaged over all subjects was 257 (124) N. The individual maxima ranged from 87 to 360 N (188 (87) N) for female subjects and from 199 to 538 N (332 (117) N) for males (Figure 3), which is a significant difference (t(22) = 9.89, p < 0.001).
Figure 3.
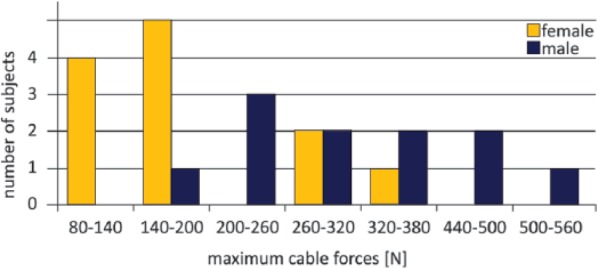
Male subjects attained significantly higher forces than female subjects (t(22) = 9.89, p < 0.001). Subjects created cable forces of 257 (124) N (mean (standard deviation)). The maximum attained forces range from 87 to 360 N (188 (87) N) and 199 to 538 N (332 (117) N) for female and male subjects, respectively.
Assuming fatigue-free operation at 20% of the users’ MCFs,5 females can operate a body-powered prostheses fatigue free up to 38 (17) N, whereas males can handle forces up to 66 (23) N.
The subjects’ MCFs and fatigue limits were compared to the required operation forces of (1) voluntary closing prostheses creating a 15-N pinch force2 (Figure 4) and (2) voluntary opening prostheses achieving a 50-mm prehensor opening with prostheses which can at least pinch 15 N3 (Figure 5). The results indicate that 3 of 10 evaluated prostheses cannot be operated by all subjects even when exerting their MCFs. More than 50% of the subjects will not operate 8 of the 10 evaluated prostheses in daily life fatigue free. One prosthesis included into the study, the Hosmer Soft Hand, cannot even be operated by a single user without exhaustion.
Figure 4.
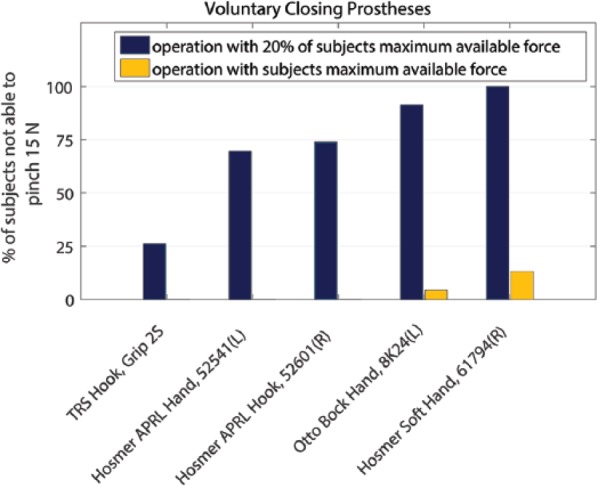
Pinching 15 N repetitively with five voluntary closing prostheses fatigue free is impossible for 26%–100% of prosthesis users. Fatigue-free operation is considered at 20% of users’ maximum cable force5 and is desired for ADL. Cable forces required to pinch 15 N with five voluntary closing prostheses vary between 33 and 131 N.2 The maximum strength of 13% of prosthesis users is insufficient to pinch 15 N with the Hosmer Soft Hand.
Figure 5.
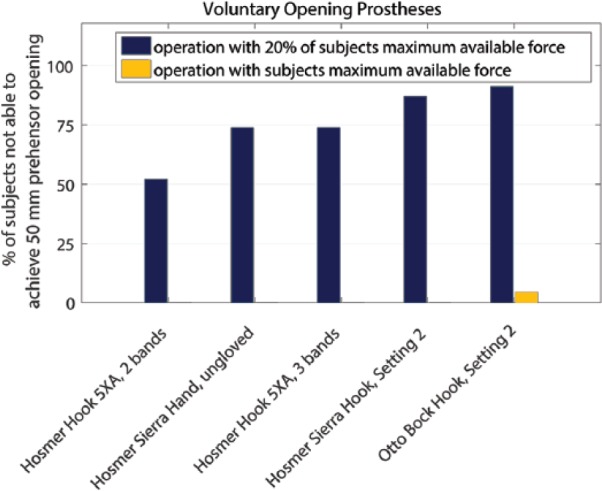
Achieving a 50-mm prehensor opening repetitively with five voluntary opening prostheses fatigue free is impossible for 52%–91% of prosthesis users. Fatigue-free operation is considered at 20% of users’ maximum cable force5 and is desired for ADL. Voluntary opening prostheses, which are able to pinch at least 15 N, require between 50 and 94 N cable force to achieve a 50-mm prehensor opening.3 The maximum strength of 4% of prosthesis users is insufficient to open the Otto Bock Hook.
Reported sensations after exerting the MCFs are summarized in Table 3. Sensations were mostly reported in armpit, neck/shoulders, and upper back. Of the 23 subjects, 9 reported pain or discomfort, of which 6 reported the armpit as the affected body part. Detailed information on extent and locations of reported sensations can be found in Appendix 1.
Table 3.
Reported sensations in the body maps were independent of the subjects’ maximum cable forces.
| Subject no. | Maximum cable force (N) | Fatigue-free operation force (N) | Sufficient force to operate Hosmer Hook 5XA fatigue free | Body maps |
|---|---|---|---|---|
| 18 | 86.6 | 17.3 | No | Irritation |
| 19 | 100.4 | 20.1 | No | None |
| 11 | 117.9 | 23.6 | No | Pain |
| 14 | 134.1 | 26.8 | No | Mild sensation |
| 16 | 147.9 | 29.6 | No | Pain |
| 12 | 164.1 | 32.8 | No | None |
| 4 | 165.4 | 33.1 | No | Mild sensation |
| 8 | 181.6 | 36.3 | No | Pain |
| 3 | 197.9 | 39.6 | No | Irritation |
| 22 | 199.1 | 39.8 | No | Pain |
| 9 | 212.9 | 42.6 | No | None |
| 23 | 229.2 | 45.8 | No | Mild sensation |
| 21 | 259.2 | 51.8 | No | Mild sensation |
| 5 | 272.9 | 54.6 | No | Mild sensation |
| 1 | 277.9 | 55.6 | No | Mild sensation |
| 15 | 290.4 | 58.1 | No | Mild sensation |
| 17 | 307.9 | 61.6 | No | Mild sensation |
| 2 | 360.4 | 72.1 | Yes | None |
| 13 | 360.4 | 72.1 | Yes | Mild sensation |
| 7 | 369.2 | 73.8 | Yes | Mild sensation |
| 6 | 441.7 | 88.3 | Yes | Irritation |
| 10 | 490.4 | 98.1 | Yes | Irritation |
| 20 | 537.9 | 107.6 | Yes | Irritation |
The Hosmer Hook 5XA with three bands requires 71 N cable operation force, the average operation forces over all prostheses. The individual maximum cable forces indicate that all users are capable to operate the hook, but only 6 of the 23 subjects could operate the hook fatigue free on a daily basis (printed in bold).
Reported sensations appear to vary randomly between the subjects and are independent of the maximum force they could generate (as can been seen in Table 3). The Hosmer Hook 5XA with three bands requires a cable operation force of 71 N, which is the average operation force of all tested prostheses. With its individual maximum and fatigue-free cable operation forces, Table 3 indicates that all users can operate the hook, but only 6 of 23 subjects would be able to operate the prosthesis fatigue free on a daily basis.
The MCF can be predicted for the females by the following model
The affected upper-arm circumference shows a Pearson correlation with an MCF of 0.646 for female subjects (n = 12, p = 0.023). Other predictors and correlations were not significant. Anthropometric measures and subject characteristics are summarized in Appendix 2.
Discussion
This study aimed to quantify users’ maximum cable operation forces and to relate these to a fatigue-free force range for the use of body-powered prostheses. In addition, we aimed to identify extent and locations of discomfort provoked by the exertion of cable forces and to explore the predictability of maximum cable operation forces by the anthropometric measures of users. Subjects created MCFs of 257 (124) N. The majority of subjects cannot use most body-powered prostheses fatigue free on a daily basis. Nine subjects reported discomfort or pain after exerting MCFs, of which six reported the armpit as the affected body part. Pain and discomfort do not correlate with the maximum force a subject could generate. The affected upper-arm circumference can predict the MCF exerted by females.
The attained MCFs are comparable to the reported cable forces of Taylor,6 although isolated movements of controls were measured. The results show that the required cable forces of available prostheses are, generally speaking, not befitted to the user’s strength when corrected for fatigue-free operation. Accordingly, more than half of all users cannot operate 8 of the 10 prostheses that were evaluated, which might explain the high rejection rates of body-powered prostheses.1 Thus, the development of low-operation force prehensors, especially of more efficient hand prostheses, is greatly desired. Current body-powered hand prostheses show inferior mechanical behavior compared to hook prostheses2,3 but might be preferred by users for cosmetic reasons. As a design recommendation for body-powered prostheses, the fatigue-free operation force for the average female of 38 (17) N and for the average male of 66 (23) N should be considered. An alternative way to derive a design criterion could be to determine the cable force level that can be exerted, fatigue free, by 90% of the users. Based on the results of this experiment, this would result in even lower allowed forces (<23 N), which is considered quite challenging for prosthesis design. In both cases, the design recommendation is based on the fatigue limit of 20% of the user’s maximum force.5 The strength–duration curve of Monod shows that when incidentally a higher pinch force is required, the fatigue-free boundary can be exceeded without further consequences. This means that for most daily activities with a voluntary closing prosthesis, higher operation forces are acceptable as long as they are limited in frequency and duration. The higher the required force, the shorter it can be produced without fatigue effects. However, the indicated fatigue-free boundary should not be exceeded for repetitive daily tasks. Unfortunately, the information on daily usage patterns, for instance, the required amount of prosthesis activations, the duration of object manipulation, and the required pinch force for daily activities with available prostheses, is limited. The required pinch force to conduct a daily activity might be higher or lower than the estimate of 15 N, depending on the task and the used prostheses. The distribution of forces exerted on an object might differ between a hook and a hand prehensor, and consequentially, the required normal force to grasp and hold an object will be different as well. A multi-articulating hand might require an even lower pinch force since the hand can adapt to the shape of the object and the object’s mass can rest, for instance, on a finger. The quantification of daily usage patterns is an important aspect in prosthesis development, and more research attention is greatly desired. This knowledge would allow an optimized transmission system design, matching user capacities (cable operation forces or “input”) with demands (pinch forces or “output”) for body-powered prosthesis. Also, it would quantify technical specifications to allow minimization of motors and battery packs in myo-electric prostheses and, therefore, reduce the prosthesis’ weight.
The results indicate that a number of subjects may only be able to operate a very limited range of prehensors, and some users might not be able to operate a body-powered prosthesis at all. The alternative functional prosthesis, a myo-electric prosthesis, is not widely available in various countries due to its high costs. Additionally, a myo-electric prosthesis does not offer the user proprioceptive feedback of prehensor activation like a body-powered prosthesis. Strength training as part of rehabilitation might help to mitigate the effects of limited availability of low-operation force body-powered prehensors currently on the market. The user’s strength could, for instance, routinely be measured by clinicians as part of terminal device selection and rehabilitation planning. The strength of females (but not males) could be predicted by the upper-arm circumference. An alternative solution in clinical practice might be to use a simple spring balance system instead.
Discomfort and pain are reasons for prosthesis rejection1,4,9 and occasional nonuse in frequent wearers.10 In body-powered prostheses use, the harness system can cause skin irritations and upper body pain.4 Supplementary to the literature, the results of this study show that the exertion of maximum forces provokes discomfort and pain with approximately 40% of the users. Reported locations of discomfort and pain are mainly the armpit, neck/shoulders, and upper back, which is caused by the harness system. However, it is noted that daily activities may not require the user to exert maximum forces. On one hand, operation forces required to conduct daily activities are lower and might not result in the extent of discomfort that the maximum forces provoke. On the other hand, in this study, the force is only exerted for a short period of time (3 s), whereas perceived discomfort seemed to be also dependent on the duration and frequency of force production.11 In other words, perception of discomfort during or after daily activities is likely to be dependent on duration and frequency of object manipulation next to the magnitude of exerted forces. Therefore, the results can only serve as an indication of discomfort perceived during daily body-powered prosthesis operation and point out areas for improvement by quantifying extent and locations of discomfort provoked by the exertion of cable forces.
It was expected that anthropometric measures could predict user strength in terms of MCFs. This might help clinicians to make a quick estimate whether a body-powered prosthesis is suitable for a patient. However, this study showed predictability of maximum forces only by the affected upper-arm circumference of females. Unfortunately, the strength of males is not predictable by anthropometric measures since the predictions were not significant for this subject population.
Study limitations
The magnitude of maximum cable operation forces partly depends on the eagerness and motivation of subjects. The encouragement of the experimenter may contribute but may not be sufficient to reach the maximum strength.
The results show a wide variability in achieved maximum forces over the subjects. Data of more participants might have allowed more (gender specific) predictions of MCFs by anthropometric data. However, the subject population was a representative group of (potential) prosthesis users with trans-radial defects since the group covered a wide variety of characteristics as indicated in Table 1 and Appendix 2.
The group’s wide variety of characteristics might have led to the wide variability in achieved maximum forces over the subjects. After many years of active use of body-powered prosthesis, frequent users may increase muscle strength and be able to produce higher forces than those not trained. By contrast, myo-electric prosthesis users may suffer from muscle atrophy over time, and their muscle force may be greatest immediately after amputation.
We concluded that pain and discomfort do not correlate with the magnitude of the maximum force achieved by the subjects. In other words, subjects who were able to attain higher forces were not experiencing more discomfort or pain than subjects who created significant lower maximum forces. This study did not investigate the subjects’ individual discomfort thresholds of exerted cable forces. Also, conclusions on the severity of the pain cannot be drawn by the subjective data of the body maps. Furthermore, depending on his physical strength and desired daily activities, a user may not need the maximum force to operate his prosthesis. The recorded pain or discomfort associated with maximum forces, therefore, may or may not be experienced in daily life.
Conclusion
In conclusion, in many cases, the user’s strength is insufficient to operate body-powered prostheses fatigue free on a daily basis. Exerting MCFs provokes discomfort and pain, especially in the armpit. The fatigue-free operation forces for the average female of up to 38 N and for the average male user of up to 66 N should be considered as input design target of body-powered prostheses to conduct most daily activities. This implies that a significant number of users may not be able to achieve this group average in consideration of their personal fatigue limit. The choice of a body-powered prosthesis should be based on the user’s strength, which can be predicted, for females only, by the affected upper-arm circumference.
Appendix
Appendix 1.
Extent and locations of sensations provoked by the exertion of cable forces.
| Subject no. | Touchiness (=green) | Irritation (=orange) | Pain (=red) |
|---|---|---|---|
| 1 | – | – | – |
| 5 | – | – | – |
| 8 | – | – | – |
| 12 | – | – | – |
| 3 | Left and right armpit | – | – |
| 17 | Left and right neck and upper and lower back | – | – |
| 10 | Left armpit | – | – |
| 21 | Left armpit and back (sensor) and stump | – | – |
| 2 | Left neck | – | – |
| 18 | Left neck | – | – |
| 9 | Right shoulder | – | – |
| 13 | Right upper arm | – | – |
| 23 | Upper back | – | – |
| 15 | Upper back (sensor) and left armpit | – | – |
| 20 | Back (harness) | Left armpit | – |
| 6 | – | Left elbow and right armpit | – |
| 14 | – | Right armpit | – |
| 16 | – | Right armpit | – |
| 11 | Left shoulder and neck | Right stump | – |
| 19 | – | – | Back (harness) |
| 22 | Right armpit | – | Left armpit |
| 7 | Right shoulder | Left upper back | Left neck |
| 4 | Upper back (harness) | Left elbow | Right armpit |
Appendix 2.
Subject characteristics and anthropometric measures.
| Subject no. | Gender | Age | Acquired/congenital defect | Affected side | Dominant side | Maximum cable force (N) | Body mapsa | Shoulder widthb | Affected upper-arm lengthc | Sound upper-arm circumferenced | Affected upper-arm circumferenced | Remnant lengthe | Weight (kg) | Height (cm) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 11 | F | 60 | Acquired | R | R | 87 | 2 | 39.7 | 31.7 | 25.0 | 23.6 | 20.9 | 57 | 164 |
| 9 | F | 54 | Acquired | L | R | 134 | 1 | 35.1 | 33.9 | 27.3 | 26.0 | 24.1 | 58 | 172 |
| 14 | F | 69 | Acquired | L | R | 198 | 2 | 40.3 | 33.3 | 36.8 | 34.3 | 15.4 | 93 | 168 |
| 12 | F | 52 | Congenital | R | R | 100 | 0 | 36.8 | 33.2 | 26.7 | 22.5 | 9.1 | 60 | 169 |
| 7 | F | 49 | Congenital | L | R | 118 | 3 | 38.2 | 36.5 | 31.5 | 29.0 | 10.0 | 70 | 177 |
| 19 | F | 58 | Congenital | L | R | 148 | 3 | 39.3 | 31.4 | 28.3 | 27.2 | 14.7 | 64 | 161 |
| 8 | F | 46 | Congenital | L | R | 164 | 0 | 35.7 | 33.3 | 26.5 | 24.5 | 16.7 | 57 | 161 |
| 2 | F | 20 | Congenital | L | R | 165 | 1 | 36.4 | 35.5 | 26.0 | 23.2 | 10.5 | 64 | 168 |
| 4 | F | 43 | Congenital | L | L | 182 | 3 | 40.0 | 35.4 | 33.4 | 27.2 | 9.7 | 94 | 173 |
| 18 | F | 34 | Congenital | L | L | 290 | 1 | 41.0 | 33.0 | 33.0 | 31.0 | 18.0 | 89 | 168 |
| 10 | F | 54 | Congenital | R | L | 308 | 1 | 37.5 | 33.5 | 32.0 | 26.8 | 10.5 | 68 | 168 |
| 17 | F | 43 | Congenital | R | L | 360 | 1 | 39.4 | 28.4 | 23.8 | 34.0 | 14.9 | 91 | 170 |
| 23 | M | 49 | Acquired | L | R | 229 | 1 | 48.0 | 35.4 | 45.5 | 46.5 | 23.5 | – | 186 |
| 1 | M | 57 | Acquired | L | R | 360 | 0 | 42.0 | 37.5 | 34.0 | 30.5 | 17.0 | 103 | 187 |
| 3 | M | 68 | Acquired | R | R | 369 | 1 | 42.3 | 35.4 | 34.5 | 32.0 | 18.4 | 81 | 170 |
| 16 | M | 50 | Acquired | L | L | 442 | 2 | 45.0 | 35.0 | 32.0 | 28.0 | 29.0 | 98 | 184 |
| 6 | M | 35 | Acquired | L | R | 490 | 2 | 41.2 | 35.0 | 27.8 | 27.5 | 31.9 | 68 | 178 |
| 20 | M | 68 | Acquired | R | R | 538 | 2 | 44.2 | 34.7 | 31.0 | 26.0 | 20.0 | 85 | 179 |
| 22 | M | 55 | Congenital | L | L | 199 | 3 | 41.5 | 34.5 | 28.3 | 24.9 | 23.2 | 62 | 176 |
| 5 | M | 63 | Congenital | L | R | 213 | 0 | 41.0 | 32.0 | 31.5 | 25.5 | 10.7 | 74 | 172 |
| 21 | M | 37 | Congenital | R | R | 259 | 1 | 45.5 | 35.1 | 31.0 | 30.0 | 12.9 | 82 | 185 |
| 15 | M | 25 | Congenital | R | R | 273 | 1 | 40.9 | 34.0 | 32.0 | 28.5 | 12.3 | 76 | 178 |
| 13 | M | 47 | Congenital | R | R | 278 | 1 | 45.0 | 37.5 | 31.2 | 24.3 | 8.9 | 82 | 186 |
M: male; F: female; R: right; L: left.
Subjects are sorted by gender and the cause of their arm defect (indicated by the horizontal lines).
Body maps: 0 = none, 1 = mild sensation, 2 = irritation, and 3 = pain.
Anthropometric data (cm) were taken following the instructions of the NASA Reference Publication 1024: b103: biacromial breadth; c751: shoulder–elbow length; d113: biceps circumference, relaxed; and e381: forearm–hand length (the fingertips are represented by the far end of the subjects’ stump).
Footnotes
Author contribution: All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fonds NutsOhra (Grant/Award Number1101-049).
References
- 1. Biddiss EA, Chau TT. Upper limb prosthesis use and abandonment: a survey of the last 25 years. Prosthet Orthot Int 2007; 31(3): 236–257. [DOI] [PubMed] [Google Scholar]
- 2. Smit G, Plettenburg DH. Efficiency of voluntary closing hand and hook prostheses. Prosthet Orthot Int 2010; 34(4): 411–427. [DOI] [PubMed] [Google Scholar]
- 3. Smit G, Bongers RM, Van der Sluis CK, et al. Efficiency of voluntary opening hand and hook prosthetic devices: 24 years of development? J Rehabil Res Dev 2012; 49(4): 523–534. [DOI] [PubMed] [Google Scholar]
- 4. Biddiss E, Beaton D, Chau T. Consumer design priorities for upper limb prosthetics. Disabil Rehabil Assist Technol 2007; 2(6): 346–357. [DOI] [PubMed] [Google Scholar]
- 5. Monod H. Contractility of muscle during prolonged static and repetitive dynamic activity. Ergonomics 1985; 28(1): 81–89. [DOI] [PubMed] [Google Scholar]
- 6. Taylor CL. The biomechanics of the normal and of the amputated upper extremity. In: Klopsteg P, Wilson P. (eds) Human limbs and their substitutes. New York: McGraw-Hill, 1954, pp. 169–221. [Google Scholar]
- 7. Delft Prosthetics BV: the WILMER open fitting, http://www.delftprosthetics.nl/nl/producten/open-fitting (accessed 20 June 2016).
- 8. Churchill E, Churchill T, Downing K, et al. Anthropometric source book volume II—a handbook of anthropometric data (ed Staff of Anthropology Research Project, Webb Associates and Yellow Springs, Ohio, NASA Reference Publication 1024). Washington, DC: NASA, 1978. [Google Scholar]
- 9. Kejlaa GH. Consumer concerns and the functional value of prostheses to upper limb amputees. Prosthet Orthot Int 1993; 17(3): 157–163. [DOI] [PubMed] [Google Scholar]
- 10. Biddiss E, Chau T. Upper-limb prosthetics: critical factors in device abandonment. Am J Phys Med Rehabil 2007; 86(12): 977–987. [DOI] [PubMed] [Google Scholar]
- 11. Hichert M, Abbink DA, Vardy AN, et al. Perception and control of low cable operation forces in voluntary closing body-powered upper-limb prostheses, submitted to IEEE Transactions on Human-Machine Systems. [DOI] [PMC free article] [PubMed] [Google Scholar]