

Abstract
Objectives
We hypothesized that tonsillectomy modifies the risk of Parkinson’s disease (PD) and tested the hypothesis in a nationwide population-based cohort study.
Methods
We used Danish medical registries to construct a cohort of all patients in Denmark with an operation code of tonsillectomy 1980–2010 (n= 195,169) and a matched age and sex general population comparison cohort (n= 975,845). Patients were followed until PD diagnosis, death, censoring, or end of follow-up Nov 30th 2013. Using Cox regression, we computed hazard ratios (HRs) for PD and corresponding 95% confidence intervals (CIs), adjusting for age and sex by study design, and potential confounders.
Results
We identified 100 and 568 patients diagnosed with PD amongst the tonsillectomy and general population comparison cohort, respectively, finding similar risks of PD [adjusted (a) HR = 0.95 (95% CI: 0.76–1.19); for > 20 years follow-up (aHR= 0.96 (95% CI: 0.64–1.41)].
Conclusion
Tonsillectomy is not associated with risk of PD, especially early onset PD.
Keywords: Tonsils, Tonsillectomy, prion, Parkinson’s disease, risk factor, epidemiology, cohort study
Introduction
Parkinson’s Disease (PD) may be a prion-like disorder with inter-neuronal propagation of aggregated α-synuclein.1 In the transmissible prion disease, variant Creutzfeld Jakob disease (vCJD), prions may initially infect the Peyer’s patches in the gut and tonsils.2 In fact, tonsil biopsies are used to diagnose vCJD.3 From these lymphoid tissues, prions spread via autonomic nerves to the dorsal motor nucleus of the vagus, sympathetic ganglia, and the intermediolateral cell column in the spinal cord.4 Thus, the spread of prions is reminiscent of the spreading pattern hypothesized to occur in PD,5, 6 which can affect similar neural populations 7.
If lymphoid tissues of the tonsils may play a part in establishing or facilitating the pathological conditions in PD including initial misfolding of α-synuclein, tonsillectomy would potentially protect against PD. This possibility has not previously been studied. In Danish patients, 90% with a hospital diagnosis of chronic tonsillitis had subsequent tonsillectomy.8 The close relation between the immune system and the microbiome, which may influence PD risk,9 provides further justification for this study. We hypothesized that tonsillectomy modifies the risk of PD and tested the hypothesis in a nationwide population-based cohort study.
Methods
Denmark has universal tax-supported health care, including free access to hospital-based care. All residents are assigned a unique personal identification number, registered in the Danish Civil Registration System at birth or upon immigration, permitting unambiguous linkage across registries. 10
We assembled a population-based Danish cohort of all patients with a surgical code for tonsillectomy (see appendix) between January 1, 1980 and December 31, 2010. Patients were identified from the Danish National Patient Registry (DNPR), 11 which has registered all diagnoses (the International Classification of Diseases (ICD), Eight revision from 1977 to 1993, and Tenth Revision since 1994.12, 13 ) and procedures associated with inpatient hospitalizations in Denmark since 1977 and all hospital outpatient clinic visits since 1995.
Using the Danish Civil Registration System, we assembled a matched general population comparison cohort of individuals with no history of tonsillectomy prior to the tonsillectomy date of the corresponding patient (the index date). 10 We randomly selected up to five persons from the general population for each patient without replacement, matched on year of birth, sex, and year of index date.
PD was identified based on first-time inpatient diagnoses (from 1980 on) or outpatient hospital clinic diagnoses (from 1995 on) in the DNPR. We excluded patients with a PD diagnosis prior to the index date, excluding all prevalent cases.
Little is known about risk factors for tonsillitis or tonsillectomy, except age and sex.8, 14 We therefore chose known risk factors for PD, and used these for adjustment. In addition to age and sex, these risk factors were previous head trauma, diabetes, smoking (using the correlate chronic pulmonary disease), and cardiovascular diseases.15 As there is an association between tonsillectomy and increased risk of Crohn’s disease, 16 we also controlled for this, despite a lack of a clear association with PD.17
We followed each cohort from the index date until emigration, death, November 30, 2013, or PD diagnosis, whichever came first.
Statistical methods
We characterized the tonsillectomy and general population comparison cohorts according to sex, age group at index (0–14, 15–24, 25–34, 35+ years), year of index date, and potential confounders.
We calculated incidence rates of PD per 10,000 person-years in the two cohorts. We used Cox proportional hazards models to compute hazard ratios (HRs) and associated 95% confidence intervals (CIs) for PD, comparing the tonsillectomy cohort and the general population comparison cohort, adjusting for age and sex by study design, and then potential confounders.
We stratified all analyses by sex. Time of follow-up was additionally stratified into 11–15 years, 16–20 years, and >20 years since tonsillectomy/index date.
We conducted three sensitivity analyses. In the first, we restricted case ascertainment of after 1995, the time when outpatient data were first available. In the second, we restricted the analysis to persons born after 1967, to ensure close to complete assessment of the exposure, and followed to early onset PD. In the third, we restricted the analyses to persons over 35 years at tonsillectomy. To assess possible misclassification due to left truncation of data, we calculated the lifetime risk of tonsillectomy in all Danes born between 1977–1982 from birth to 2012, giving the proportion with tonsillectomy prior to age 35 years. We then ran 5 iterations, randomly excluding this proportion in the comparison cohort. In both, we examined the association > 10 years after the index date (>10 years follow-up).
We assessed potential unmeasured confounding of smoking by external adjustment. 18 We assumed that the relative risk of PD in smokers is 0.53, 19 and that the proportion of smokers was respectively 0.50 and 0.55 in the unexposed cohort and tonsillectomy cohort. 20
The study was approved by the Danish Data Protection Agency (Record Nr. 1-16-02-1-08). As this registry-based study did not involve patient contact, no separate permission from the Danish Scientific Ethics Committee was required, according to Danish legislation.
Results
Between 1980 and 2010, 195,169 individuals were registered in the DNPR with an operation code for tonsillectomy (Table 1). On the index date, in the two cohorts, the median age was 17 years, 11% of were older than 35 years, and 56% were female, and the variables considered as potential confounders did not differ in prevalence (Table 1).
Table 1.
Characteristics of 195,169 patients with tonsillectomy, and 975,845 general population comparison cohort members, Denmark 1980–2010
| Tonsillectomy cohort | Matched comparison cohort | |||
|---|---|---|---|---|
| N | % | N | % | |
| Sex | ||||
| Female | 109,525 | 56 | 547,625 | 56 |
| Male | 85,644 | 44 | 428,220 | 44 |
| Age | ||||
| 0–14 years | 77,657 | 40 | 389,390 | 40 |
| 15–24 years | 67,783 | 35 | 337,948 | 35 |
| 25–34 years | 29,121 | 15 | 145,417 | 15 |
| 35+ years | 20,608 | 11 | 103,090 | 11 |
| Index date | ||||
| 1980–1989 | 67,693 | 35 | 338,465 | 35 |
| 1990–1999 | 68,222 | 35 | 341,110 | 35 |
| 2000–2010 | 59,254 | 30 | 296,270 | 30 |
| Diabetes | ||||
| No | 194,437 | 99 | 971,830 | 99 |
| Yes | 732 | 0.4 | 4,015 | 0.4 |
| Chronic pulmonary disease | ||||
| No | 189,820 | 97 | 956,721 | 98 |
| Yes | 5,349 | 3 | 19,124 | 2 |
| Any previous cardiovascular disease | ||||
| No | 194,101 | 99 | 970,871 | 99 |
| Yes | 1,068 | 1 | 4,974 | 1 |
| Head trauma | ||||
| No | 186,857 | 96 | 943,606 | 97 |
| Yes | 8,312 | 4 | 32,239 | 3 |
| Crohn’s disease | ||||
| No | 195,015 | 100 | 975,111 | 100 |
| Yes | 154 | 0.1 | 734 | 0.1 |
| Ulcerative colitis | ||||
| No | 194,903 | 100 | 974,562 | 100 |
| Yes | 266 | 0.1 | 1,283 | 0.1 |
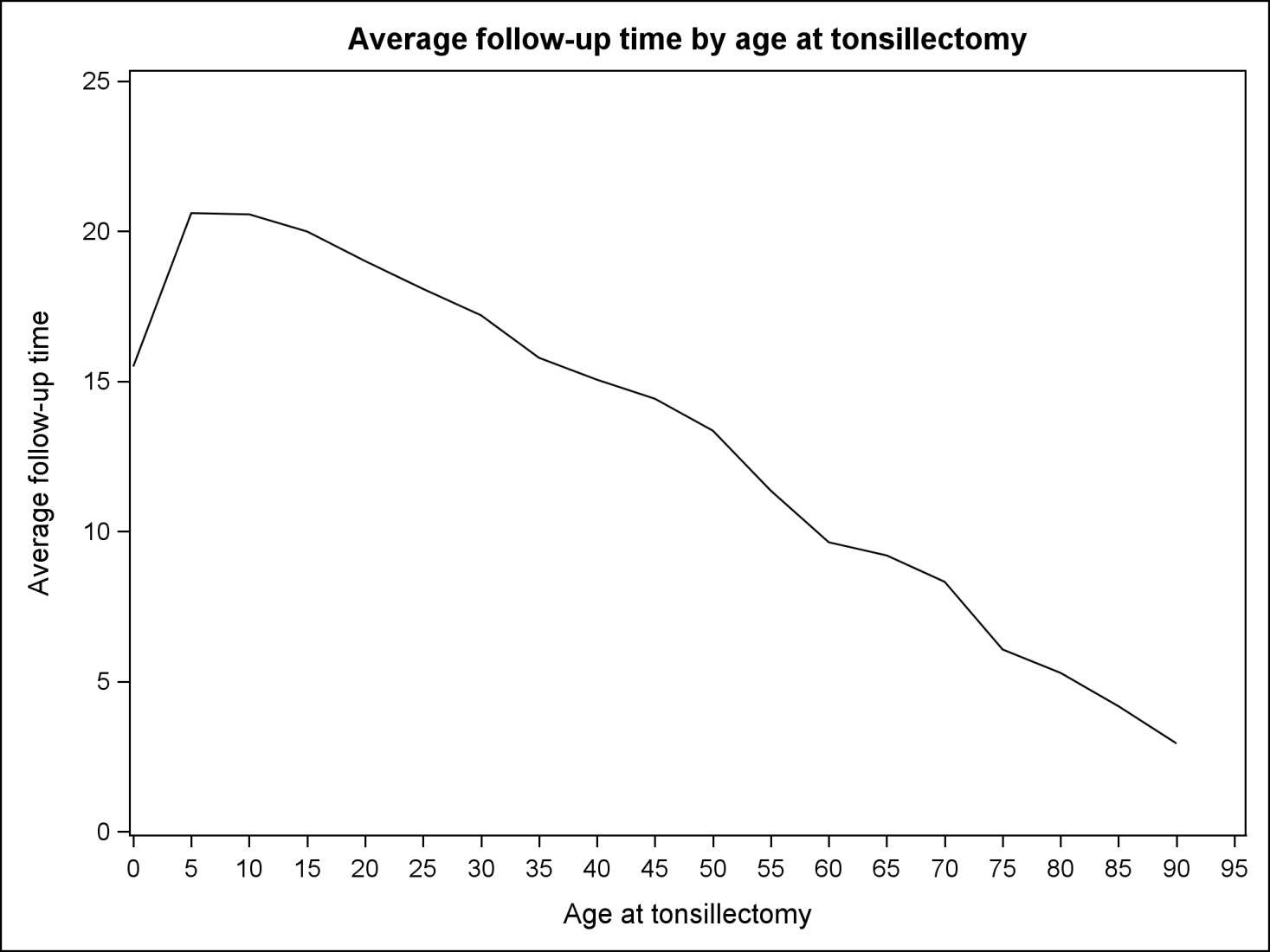
Overall, we identified 100 persons with PD among the patients with tonsillectomy (incidence rate 0.27 per 10,000 person years at risk), and 568 persons with PD among matched members of the general population comparison cohort (incidence rate: 0.31 per 10,000 person-years at risk). This corresponded to a similar risk of PD [adjusted (a) HR = 0.95 (95% CI: 0.76–1.19)]. None of the adjustments for potential confounders accounted for the observed associations (Table 2); the HR remained virtually unchanged. The median age of PD diagnosis was 64 (IQR 53–73) years in the tonsillectomy cohort and 67 (IQR 55–76) years in the general population cohort (p=0.09). The initial PD diagnosis was made in an inpatient setting for 44% of the tonsillectomy cohort and 36% for the comparison cohort. The median age at censoring for those not diagnosed with PD during follow-up was 37 years (IQR 27–46 years)(see supplemental figure).
Table 2.
Incidence rates, hazard ratios (HRs), and associated 95% confidence intervals (CIs) for Parkinson’s disease, comparing patients who underwent tonsillectomy with persons from a matched general population comparison cohort, overall and stratified by sex and follow-up time.
| Follow-up time | PD diagnoses (n) | Incidence rate per 10,000 pyr (95% CI) | Unadjusted HR a (95% CI) | Adjusted HR b (95% CI) | |
|---|---|---|---|---|---|
| Overall (0–34) | Comparison cohort | 568 | 0.31 (0.29–0.34) | 1.00 | 1.00 |
| Tonsillectomy cohort | 100 | 0.27 (0.22–0.33) | 0.95 (0.76–1.18) | 0.95 (0.76–1.19) | |
| 11–15 years | Comparison cohort | 103 | 0.30 (0.24–0.35) | 1.00 | 1.00 |
| Tonsillectomy cohort | 17 | 0.24 (0.13–0.36) | 0.94 (0.54–1.64) | 0.95 (0.55–1.67) | |
| 16–20 years | Comparison cohort | 90 | 0.33 (0.26–0.40) | 1.00 | 1.00 |
| Tonsillectomy cohort | 20 | 0.36 (0.20–0.52) | 1.15 (0.69–1.90) | 1.17 (0.70–1.95) | |
| 20–34 years | Comparison cohort | 167 | 0.55 (0.47–0.64) | 1.00 | 1.00 |
| Tonsillectomy cohort | 31 | 0.51 (0.33–0.69) | 0.95 (0.64–1.41) | 0.96 (0.65–1.42) |
Abbreviation: pyr – person-years.
Adjusted for age and sex.
Adjusted for age, sex, diabetes, chronic pulmonary disease, cardiovascular disease, head trauma and Crohn’s disease.
The results were similar when restricting on follow-up time exceeding 20 years [aHR= 0.96 (95% CI: 0.64–1.41]. No sex differences were observed (men [aHR=0.93 (95% CI: 0.69–1.24)], women [aHR=1.00 (95% CI: 0.72–1.41)].
The first sensitivity analysis showed consistent results with the overall analysis.
In the second sensitivity analysis, restricting to patients born after 1967, there were 9 PD diagnoses in the tonsillectomy cohort (incidence rate 0.03 per 10 000 person-years at risk), and 43 PD diagnosis in the comparison cohort (incidence rate 0.03 per 10 000 person years at risk), yielding a crude HR of 1.07 (95%CI 0.52–2.12) (no further adjustment possible).
In the third sensitivity analyses, restricting on tonsillectomy >35 years of age, there were 71 PD diagnoses in tonsillectomy cohort (median age of diagnosis 70 (IQR 62–77)), and 422 PD diagnosis in the comparison cohort (median age of diagnosis 72 (IQR 65–79)) (median age, p=0.08). This yielded an aHR = 0.94 (95% CI 0.72–1.22); follow-up > 10 years: aHR=1.03 (95% CI: 0.73–1.47). 9% of all persons under age 35 had a tonsillectomy. Running 5 iterations, excluding a random 9% of the comparison cohort yielded aHR overall ranging from 0.92–0.97 ; >10 years follow-up ranging from 0.99–1.11.
The RR externally adjusted for unmeasured confounding by smoking was 0.91.
Discussion
Tonsillectomy was not associated with risk of PD in this nationwide prospective cohort study. Results were consistent in stratified analyses and in the sensitivity analyses. Of note, we did we did follow over 20 000 persons who had undergone tonsillectomy over the age of 35, and their corresponding 103 000 matched comparison subjects for a median 15 years. Findings thus fail to support the hypothesis that tonsillectomy reduces risk of PD, especially early onset PD.
The study has several limitations. Although the study included up to 34 years of follow-up, the study population was relatively young, and many have not reached the age of full susceptibility for PD. Another concern is incomplete ascertainment of tonsillectomies, particularly for persons aged over 45 years, who might have undergone tonsillectomy prior to establishment of the DNPR in 1977. We estimated that 9% of the population had a tonsillectomy before age 35 years. We assumed that this was constant over time, and ran several iterations randomly excluding 9% of the comparison cohort. This did not noteworthy change the estimates. The validity of registry diagnoses for tonsillectomy is not known, but surgical procedure codes in general have high validity.21 Finally, confounding by measured comorbid disease was minimized, but we cannot exclude the possibility of residual confounding by unmeasured factors. We aimed to assess unmeasured confounding of smoking by external adjustment, and the estimates were consistent. Of note the assumptions of external adjustment are based on qualified estimates at best.
Study strengths include its large sample size and nationwide population-based design, conducted in a setting in which comprehensive long-term follow-up reduce the potential for selection bias. Even though the validity of the PD diagnosis in registries is high (positive predictive value of 82%, comparing the DNPR with medical records)22 this study may have missed some PD patients with early disease, as initial treatment may not be provided in a hospital-setting. Such potential misclassification would tend to bias associations toward the null, as it would apply equally to the tonsillectomy and general population cohorts.
The absence of a protective effect of tonsillectomy in this study does not rule out that the tonsils may be involved in PD pathogenesis. Further studies on this association are warranted, including epidemiological studies with more complete ascertainment of the tonsillectomy exposure. Recently, it was hypothesized that lymphoid tissue of the appendix could be an initiation point of α-synuclein aggregation23, but appendectomy was associated with a slightly increased risk of subsequent PD rather than decreased risk. 24, 25 It is possible that the preceding inflammation predisposes to α-synuclein aggregation in the mucosa, followed by a secondary prion-like spreading of pathology, irrespective of subsequent appendectomy. The putative importance of lymphoid tissue in PD pathogenesis — be it in the tonsils, Peyer’s patches or appendix — could be explored in tissue specimens obtained from diagnosed or prodromal PD patients.
Supplementary Material
{kind=link}
Acknowledgments
Funding: We received funding from the Program for Clinical Research Infrastructure established by the Lundbeck and Novo Nordisk Foundations and from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No 116020 (“ROADMAP”). This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA. VWH received support from National Institutes of Health grant P50AG047366.
Prior presentation: Part of the results were presented as poster number 23 (Epidemiology) at the 21st International Congress of Parkinson’s disease and Movement Disorders, Vancouver, B.C, June 2017
Footnotes
Author contributions: PB, ES, MGS, TEK, VWH, and HTS conceived the idea for the study and developed the study concept and design, and SS performed the statistical analysis. All authors contributed to the drafting and revision of the manuscript, approved its final version, and agreed to be accountable for all aspects of the work.
Potential conflict of interests: We declare no competing interests.
Reference List
- 1.Olanow CW, Brundin P. Parkinson’s disease and alpha synuclein: is Parkinson’s disease a prion-like disorder? Mov Disord. 2013;28(1):31–40. doi: 10.1002/mds.25373. [DOI] [PubMed] [Google Scholar]
- 2.Geschwind MD. Prion Diseases. Continuum (Minneap Minn ) 2015;21:1612–1638. doi: 10.1212/CON.0000000000000251. (6 Neuroinfectious Disease) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ugnon-Cafe S, Dorey A, Bilheude JM, et al. Rapid screening and confirmatory methods for biochemical diagnosis of human prion disease. J Virol Methods. 2011;175(2):216–223. doi: 10.1016/j.jviromet.2011.05.016. [DOI] [PubMed] [Google Scholar]
- 4.van Keulen LJ, Vromans ME, Dolstra CH, Bossers A, van Zijderveld FG. Pathogenesis of bovine spongiform encephalopathy in sheep. Arch Virol. 2008;153(3):445–453. doi: 10.1007/s00705-007-0007-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hawkes CH, Del TK, Braak H. Parkinson’s disease: the dual hit theory revisited. Ann N Y Acad Sci. 2009;1170:615–22. doi: 10.1111/j.1749-6632.2009.04365.x.:615-622. [DOI] [PubMed] [Google Scholar]
- 6.Borghammer P. How does parkinson’s disease begin? Perspectives on neuroanatomical pathways, prions, and histology. Mov Disord. 2017 doi: 10.1002/mds.27138. [DOI] [PubMed] [Google Scholar]
- 7.Del TK, Braak H. Review: Sporadic Parkinson’s disease: development and distribution of alpha-synuclein pathology. Neuropathol Appl Neurobiol. 2016;42(1):33–50. doi: 10.1111/nan.12298. [DOI] [PubMed] [Google Scholar]
- 8.Vestergaard H, Wohlfahrt J, Westergaard T, Pipper C, Rasmussen N, Melbye M. Incidence of tonsillectomy in Denmark, 1980 to 2001. Pediatr Infect Dis J. 2007;26(12):1117–1121. doi: 10.1097/INF.0b013e31814536ba. [DOI] [PubMed] [Google Scholar]
- 9.Sampson TR, Debelius JW, Thron T, et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell. 2016;167(6):1469–1480. doi: 10.1016/j.cell.2016.11.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi: 10.1007/s10654-014-9930-3. [DOI] [PubMed] [Google Scholar]
- 11.Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi: 10.1177/1403494811401482. [DOI] [PubMed] [Google Scholar]
- 12.World Health Organization. International Statistical Classidicationof Diseases and Related Health Problems. 8. Geneva: World Health Organization; 1965. [Google Scholar]
- 13.World Health Organization. International statistical classification of Diseases and related health problems. Geneva, Switzerland: World Health Organization; 1993. Tenth revision. [Google Scholar]
- 14.Mattila PS, Tahkokallio O, Tarkkanen J, Pitkaniemi J, Karvonen M, Tuomilehto J. Causes of tonsillar disease and frequency of tonsillectomy operations. Arch Otolaryngol Head Neck Surg. 2001;127(1):37–44. doi: 10.1001/archotol.127.1.37. [DOI] [PubMed] [Google Scholar]
- 15.Wirdefeldt K, Adami HO, Cole P, Trichopoulos D, Mandel J. Epidemiology and etiology of Parkinson’s disease: a review of the evidence. Eur J Epidemiol. 2011;26(Suppl 1):S1–58. doi: 10.1007/s10654-011-9581-6. [DOI] [PubMed] [Google Scholar]
- 16.Sun W, Han X, Wu S, Yang C. Tonsillectomy and the risk of inflammatory bowel disease: A systematic review and meta-analysis. J Gastroenterol Hepatol. 2016;31(6):1085–1094. doi: 10.1111/jgh.13273. [DOI] [PubMed] [Google Scholar]
- 17.Rugbjerg K, Friis S, Ritz B, Schernhammer ES, Korbo L, Olsen JH. Autoimmune disease and risk for Parkinson disease: a population-based case-control study. Neurology. 2009;73(18):1462–1468. doi: 10.1212/WNL.0b013e3181c06635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lash TL, Fow MP, Fink AK. Sensitivity analyses for unnmeasured confouding. In: Lash Rl, Fox MP, Fink AK., editors. Applying quantative bias analysis to epidemiological data. Oxford, UK: Springer Verlag; 2009. [Google Scholar]
- 19.Powers KM, Kay DM, Factor SA, et al. Combined effects of smoking, coffee, and NSAIDs on Parkinson’s disease risk. Mov Disord. 2008;23:88–95. doi: 10.1002/mds.21782. [DOI] [PubMed] [Google Scholar]
- 20.Cinamon U, Goldfarb A, Marom T. The Impact of Tobacco Smoking Upon Chronic/Recurrent Tonsillitis and Post Tonsillectomy Bleeding. Int Arch Otorhinolaryngol. 2017 Apr;21(2):165–170. doi: 10.1055/s-0036-1593835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sorensen HT. Regional administrative health registries as a resource in clinical epidemiology:A study of options, strengths, limitations and data quality provided with examples of use. Int J Risk Saf Med. 1997;10(1):1–22. doi: 10.3233/JRS-1997-10101. [DOI] [PubMed] [Google Scholar]
- 22.Wermuth L, Lassen CF, Himmerslev L, Olsen J, Ritz B. Validation of hospital register-based diagnosis of Parkinson’s disease. Dan Med J. 2012;59(3):A4391. [PMC free article] [PubMed] [Google Scholar]
- 23.Gray MT, Munoz DG, Gray DA, Schlossmacher MG, Woulfe JM. Alpha-synuclein in the appendiceal mucosa of neurologically intact subjects. Mov Disord. 2014;29(8):991–998. doi: 10.1002/mds.25779. [DOI] [PubMed] [Google Scholar]
- 24.Marras C, Lang AE, Austin PC, Lau C, Urbach DR. Appendectomy in mid and later life and risk of Parkinson’s disease: A population-based study. Mov Disord. 2016;31(8):1243–1247. doi: 10.1002/mds.26670. [DOI] [PubMed] [Google Scholar]
- 25.Svensson E, Horvath-Puho E, Stokholm MG, Sorensen HT, Henderson VW, Borghammer P. Appendectomy and risk of Parkinson’s disease: A nationwide cohort study with more than 10 years of follow-up. Mov Disord. 2016;31(12):1918–1922. doi: 10.1002/mds.26761. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.