

Abstract
Background
It has been suggested that mild hypothermia treatment of hypoxia-ischemic encephalopathy (HIE) should start within 6 h after HIE, but many children are admitted to the hospital > 6 h, particularly in developing areas. We aimed to determine whether hypothermia treatment could remain effective within 12 h after birth.
Methods
According to their admission, 152 newborns were enrolled in the < 6 h and 6–12 h after HIE groups. All newborns received conventional treatment combined with mild head hypothermia therapy, according to our routine clinical practice. Some newborns only received conventional treatment (lacking informed consent). All newborns received amplitude-integrated electroencephalography (aEEG) monitoring for 4 h and neuron-specific enolase (NSE) measurement before and after 3 days of therapy.
Results
Compared to the conventional treatment, hypothermia significantly improved the aEEG scores and NSE values in all newborns of the < 6-h group. In the 6–12-h group, the aEEG scores (F = 5.67, P < 0.05) and NSE values (F = 4.98, P < 0.05) were only improved in newborns with moderate HIE. Hypothermia treatment seems to have no effect in newborns with severe HIE after 6 h (P > 0.05). Hypothermia improved the rates of neonatal death and 18-month disability (all P < 0.01).
Conclusions
In newborns with moderate HIE, starting hypothermia therapy < 6 h and 6–12 h after HIE showed curative effects. In those with severe HIE, only starting hypothermia therapy within 6 h showed curative effects.
Keywords: Hypoxic ischemic encephalopathy, Mild hypothermia, Time window
Background
Neonatal hypoxic-ischemic encephalopathy (HIE) remains a devastating cause of death in the perinatal period as well as of future neurodevelopmental abnormalities [1, 2]. Hypothermia is a proven effective treatment of HIE and can improve survival and long-term prognosis of children [3, 4]. It has been suggested that hypothermia treatment of HIE should start within 6 h after hypoxia ischemia [5], but many newborns are admitted to the hospital > 6 h after HIE, particularly those living in rural areas. In addition, a number of factors can lead to delays in treatment initiation; parents are sometimes unsure of symptoms and may take some time before going to the hospital, or the hypothermia devices may be broken or unavailable. In patients admitted > 6 h after HIE, hypothermia can still be carried out and provide some benefits.
The protocols actually being used are mainly based on animal data. Indeed, the 6-h limit for hypothermia initiation comes from data suggesting that the effectiveness of hypothermia diminishes as time increases from the hypoxic ischemic event, with the closing of the therapeutic window occurring 5.5–8 h after the event [6]. Nevertheless, the exact timing of the therapeutic window after HIE is mostly unknown in human newborns and needs to be further investigated [7].
Amplitude-integrated electroencephalography (aEEG) reveals the changes of brain physiology and identifies subclinical seizures in the early stage of brain hypoxic-ischemia. Indeed, aEEG has high sensitivity, specificity, and prognostic value in brain function monitoring. Neuron specific enolase (NSE) is an early biochemical index for neonatal brain damage, and can also help determine the degree of neuronal damage and evaluate prognosis.
This study aimed to assess newborns with HIE by observing aEEG changes and NSE levels before and after hypothermia treatment, in order to explore the clinical curative effect of different initiating times for mild hypothermia treatment of HIE.
Methods
Patients and grouping
Newborns with HIE were enrolled between August 2013 and August 2014 at the Neonate Department of our hospital [8]. The inclusion criteria were: 1) gestational age ≥ 36 weeks; 2) birth weight ≥ 2500 g; and 3) admission within 12 h of birth. The exclusion criteria were: 1) major congenital abnormalities; 2) known or suspected chromosomal abnormalities; 3) major brain malformations; or 4) aEEG abnormalities from causes other than HIE.
The diagnostic criteria for HIE were: 1) evidence of moderate or severe clinical encephalopathy in the first 12 h of life; and 2) evidence of fetal distress, with at least one of the following: a) Apgar score ≤ 5 at 5 min; b) continued need for ventilation initiated at birth and for at least 10 min; and/or c) pH ≤ 7.00 in arterial cord blood or other sample in the first hour of life [3, 4]. Encephalopathy was classified as mild, moderate or severe according to a previously reported scale that focuses on the level of alertness [9, 10].
The study was approved by the institutional ethics committee. Informed consent was obtained from the legal guardians.
The patients were divided into the mild hypothermia and control groups according to the decision of the parents. According to the treatment starting time, they were further divided into the < 6 h and 6–12 h groups. According to HIE severity, they were divided into the moderate and severe groups.
Therapies
The study enrolled all newborns with HIE undergoing the neonatal HIE treatment plan defined by the “Five-year Research Project HIE Cooperative Group” [11]. The control group included the newborns who received conventional treatment. The mild hypothermia group included the newborns who received conventional treatment combined with mild head hypothermia therapy after admission. For mild hypothermia, the Olympic Cool-Cap 004204 ice Cap system was used. The aim of hypothermia was to achieve rectal temperature of 34–35 °C, anterior fontanelle temperature of 20–25 °C, and skin temperature of 33–34.5 °C. The instrument entered the rewarming process automatically after 72 h of treatment. Table temperature was adjusted according to the anal temperature + 0.5 °C, based on computer interface prompts [12].
aEEG monitoring
aEEG was performed using the NicoletOne 32-lead brain function monitoring instrument (Olympic company, USA) and according to the international 10/20 standard electrode placement system, with C3-C4 and P3-P4 in bilateral central and parietal regions, respectively, as lead signal patch; F3-F4 was used as the reference electrode [13]. Particular care was taken to place the electrodes and to be sure that they made contact with the skin. All newborns were immediately placed in a natural quiet environment upon admission. aEEG monitoring was carried out for 4 h and repeated after 3 days of treatment.
aEEG interpretation
A synthetic marking system established by Burdjalov was used to analyze the graphs for continuity, periodicity, continuous voltage, lower boundary values, and narrow-band widths of aEEG [14]. The specific criteria are shown in Table 1.
Table 1.
Scoring system of amplitude integrated electroencephalography (aEEG)
| Score | Curve variability | SWC | Lower boundary values | Narrow-band width and lower boundary voltage |
|---|---|---|---|---|
| 0 | No variation curve | None | Seriously inhibited (< 3 μV) | Amplitude suppression: low amplitude (≤15 μV) and low voltage (5 μV) |
| 1 | Some curve, no sinusoidal ariation | Starting occurrence period | Some inhibition (3~ 5 μV) | Immaturity amplitude: high amplitude (> 20 μV) or medium amplitude (15~ 20 μV) and low voltage (5 μV) |
| 2 | Sinusoidal ariation | No clear | No inhibition (> 5 μV) | Immaturity amplitude: high amplitude (> 20 μV) and high voltage (> 5 μV) |
| 3 | Clear period, but suspension | Gradually mature amplitude: medium amplitude (15~ 20 μV) and high voltage (> 5 μV) | ||
| 4 | Clear period, no suspension | Mature amplitude: low amplitude (< 15 μV) and high voltage (> 5 μV) | ||
| 5 | Rule and mature period |
NSE measurements
Venous blood (1 ml) was collected upon admission and after three days of treatment. Serum was prepared routinely. A commercial enzyme-linked immunoassay (ELISA) was used to measure NSE (North Institute of Biotechnology Products, Beijing, China), according to the manufacturer’s instructions. The serum samples were tested as soon as possible after preparation.
Follow-up
Magnetic resonance imaging (MRI) was performed 2 weeks after HIE. The results were recorded as normal vs. abnormal. The rates of severe disability and death at 18 months were calculated.
Statistical analysis
SAS 9.1 (SAS Institute, Cary, NY, USA) was used for all analyses. Categorical data were assessed using the Chi-square test. Continuous variables were analyzed using one way analysis of variance and the Tukey’s post hoc test. P < 0.05 was considered statistically significant.
Results
Baseline characteristics of the patients
A total of 2988 newborns were treated at our Neonatology Department during the study period. Among them, 513 had HIE, and 152 cases were enrolled based on the eligibility criteria. The mild hypothermia group included 63 newborns (< 6 h subgroup, 35 cases; 6–12 h subgroup, 28 cases). There were 89 newborns in the control group (< 6 h subgroup, 48 cases; 6–12 h group, 41 cases). The characteristics of the newborns are shown in Table 2. There were no significant differences among the subgroups for gestational age, birth weight, gender, delivery mode, 5-min Apgar score, HIE stage, and aEEG score. Due to changes of NSE levels with time after hypoxia, the values in different time windows within a given group changed; nevertheless, in both groups, similar NSE values were obtained for the same initiating window.
Table 2.
General characteristics of the patients
| Control | Hypothermia | P | |||
|---|---|---|---|---|---|
| < 6 h | ≧6 h | < 6 h | ≧6 h | ||
| n | 48 | 41 | 35 | 28 | |
| Gestational age | 38.5 ± 1.4 | 40 ± 0.8 | 38.4 ± 1.47 | 38.1 ± 0.9 | 0.16 |
| Birth weight (kg) | 3.44 ± 0.68 | 3.13 ± 0.34 | 3.17 ± 0.42 | 3.27 ± 0.34 | 0.15 |
| Gender (male) | 30 (62%) | 26 (63%) | 20 (57%) | 23 (82%) | 0.19 |
| Cesarean section | 18 (37%) | 15 (36%) | 15 (42%) | 8 (28%) | 0.71 |
| 5-min Apgar grade < 7 | 34 (50%) | 30 (53%) | 16 (46%) | 13 (46%) | 0.35 |
| HIE | |||||
| Mild | 15 (31%) | 17 (41%) | 18 (51%) | 14 (50%) | |
| Moderate | 18 (38%) | 12 (29%) | 11 (31%) | 9 (32%) | 0.49 |
| Severe | 15 (31%) | 12 (29%) | 6 (17%) | 5 (18%) | |
| aEEG marking | 3.6 ± 3.1 | 3.8 ± 3.0 | 4.6 ± 2.5 | 4.5 ± 3.1 | 0.45 |
| NSE value | 25.6 ± 10.9 | 38.1 ± 24.6 | 29.5 ± 27 | 41 ± 25.6 | < 0.01 |
HIE Hypoxia ischemic encephalopathy, aEEG Amplitude integrated electroencephalography, NSE Neuron-specific enolase
aEEG values and NSE levels in the hypothermia and control groups
There were no significant differences in aEEG values and NSE levels between the hypothermia and control groups, both for the < 6 h and 6–12 h subgroups, in newborns with mild HIE after 3 days of treatment (P > 0.05) (Fig. 1). The hypothermia and control groups with treatment starting time < 6 h in patients with moderate and severe HIE showed statistically significant differences in aEEG scores (Table 3) and NSE levels (Table 4) after 3 days of treatment (P < 0.05). When treatment started at 6–12 h, aEEG scores and NSE levels were significantly different after 3 days only in patients with moderate HIE (P < 0.05). Newborns with severe HIE showed no significant difference between the two groups after treatment (P > 0.05) (Tables 3 and 4).
Fig. 1.
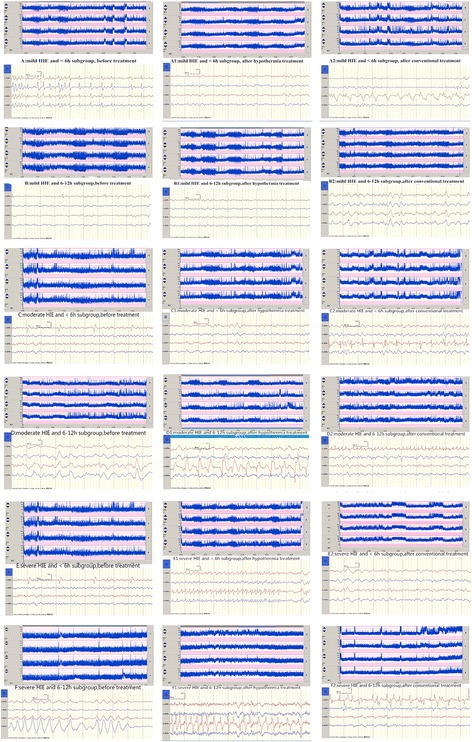
aEEG image comparison at all levels in different time windows of hypothermia treatment
Table 3.
Changes in aEEG scores after 3 days of treatment in children with HIE
| ∆aEEG | |||||||
|---|---|---|---|---|---|---|---|
| Group | Time window | Mild | Moderate | Severe | |||
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | ||
| Control group | < 6 h | 13 | 3.6 ± 2.2 | 15 | 4.7 ± 1.7b1 | 13 | 3.0 ± 2.1c1 |
| ≥ 6 h | 13 | 3.7 ± 2.2 | 10 | 3.7 ± 3.4b2 | 11 | 2.1 ± 1.4c2 | |
| Hypothermia group | < 6 h | 14 | 4.5 ± 2.3 | 9 | 1.8 ± 0.7b1 | 5 | 0.2 ± 0.4c1 |
| ≥ 6 h | 11 | 4.1 ± 2.7 | 8 | 2.1 ± 1.0b2 | 5 | 1.0 ± 0.7c2 | |
| P | 0.76a | < 0.005b | < 0.05c | ||||
∆ Before and after treatment; ano statistically significant difference between mild HIE groups (P > 0.05), bmoderate HIE groups showed statistically significant differences (P < 0.01): b1moderate HIE and < 6 h subgroup (P < 0.05), b2 moderate HIE and 6-12 h subgroup (P < 0.05); c severe HIE patients showed statistically significant differences between the subgroups (P < 0.05): c1severe HIE and < 6 h subgroup (P < 0.05) c2severe HIE and 6-12 h subgroup (P > 0.05); two initiation time windows in the hypothermia group showed no difference in moderate HIE patients (b1b2 HIE; P > 0.05) but in severe HIE patients (c1c2 P < 0.05)
Table 4.
Changes in NSE levels after 3 days of treatment in children with HIE
| ∆NSE | |||||||
|---|---|---|---|---|---|---|---|
| Group | Time window | Mild | Moderate | Severe | |||
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | ||
| Control group | < 6 h | 14 | 4.0 ± 0.6 | 14 | 19.1 ± 2.4b1 | 13 | 12.1 ± 0.3c1 |
| ≥ 6 h | 13 | 5.2 ± 1.5 | 9 | 21.4 ± 3.6b2 | 9 | 16.8 ± 5.2c2 | |
| Hypothermia group | < 6 h | 15 | 2.0 ± 0.8 | 10 | 13.7 ± 1.8b1 | 6 | 14.3 ± 3.9c1 |
| ≥ 6 h | 9 | 3.9 ± 2.8 | 7 | 15.3 ± 5.1b2 | 5 | 19.8 ± 1.9c2 | |
| P | 0.35a | < 0.01b | < 0.05c | ||||
∆ Before and after treatment; ano statistically significant difference between mild HIE groups (P > 0.05), bmoderate HIE groups showed statistically significant differences (P < 0.01): b1moderate HIE and < 6 h subgroup (P < 0.05), b2 moderate HIE and 6-12 h subgroup (P < 0.05); csevere HIE patients showed statistically significant differences between the subgroups (P < 0.05): c1severe HIE and < 6 h subgroup (P < 0.05) c2severe HIE and 6-12 h subgroup (P > 0.05); two initiation time windows in the hypothermia group showed no difference in moderate HIE patients (b1b2 HIE; P > 0.05) but in severe HIE patients (c1c2 P < 0.05)
Mid- and long-term outcomes
Table 5 presents the results of the 2-week MRI, as well as the 18-month outcomes. The rate of normal MRI was higher in the hypothermia group compared with the control group (P < 0.01). In the hypothermia group, the rate of normal MRI results was higher in the < 6 h subgroup (P < 0.01). The 18-month rate of severe disability and the rate of neonatal death were lower in the hypothermia group compared with the control group (both P < 0.01). There were no differences between the < 6 h and 6–12 h groups.
Table 5.
Results of 2-week MRI, 18-month disability rate, and neonatal death
| Controls | Hypothermia | P | |||
|---|---|---|---|---|---|
| < 6 h | 6–12 h | < 6 h | 6–12 h | ||
| n | 48 | 41 | 35 | 28 | |
| MRI during the second week | |||||
| Normal | 26 (54.2%) | 23 (56.1%) | 30 (85.7%) | 20 (71.4%) | < 0.01 |
| Abnormal | 22 (45.8%) | 18 (43.9%) | 15 (14.3%) | 8 (29.6%) | < 0.01 |
| Severe disability | 19 (39.6%) | 16 (39.0%) | 9 (25.7%) | 7 (28.6%) | < 0.01 |
| Neonatal death | 4 (8.3%) | 3 (7.3%) | 1 (2.9%) | 1 (3.6%) | < 0.01 |
Discussion
It has been suggested that mild hypothermia treatment of HIE should occur at < 6 h after HIE, but many newborns are admitted to the hospital > 6 h, particularly in developing areas. Therefore, this study aimed to determine whether hypothermia treatment could remain effective within 12 h after birth. The results showed that in newborns with moderate HIE, both < 6 h and 6–12 h hypothermia therapy starting times showed curative effects. In those with severe HIE, only starting hypothermia therapy within 6 h showed curative effects.
The etiology of neonatal HIE is complex [15]. It begins with cerebral flow reperfusion at 6–24 h after several hours or days of hypoxia ischemia, leading to mitochondrial oxidative damage and neuronal energy failure. Excess free radicals, intracellular Ca2+ overload, and large amounts of excitatory amino acids, combined with the action of inflammatory cells and inflammatory cytokines, will lead to cell death. More important hypoxia severity and duration will lead to greater pathological changes. The key link is secondary energy failure, which activates a series of biochemical reactions, finally causing or aggravating neuronal death. Secondary energy failure after 6–12 h offers a time window for disease development. Multicenter studies [16–18] also indicated that hypothermia treatment can significantly improve the prognosis of newborns with moderately severe HIE, as well as the time window of treatment < 6 h after birth. Nevertheless, some authors proposed that delaying treatment to within 10 h after hypoxia ischemia results in similar effectiveness [19], but studies reporting a treatment delay of 10 or even 12 h are scarce. Meanwhile, quite a few newborns are admitted to the hospital more than 6 h after hypoxic ischemia. Specifically, Western China has a relatively underdeveloped medical and transportation systems. The patients could benefit from hypothermia if treatment start could be delayed to > 6 h after birth. Therefore, this study included newborns with hypoxic ischemic brain damage admitted 6–12 h after birth.
Few studies have assessed hypothermia in the treatment of mild HIE. Zhou et al. [20] suggested that newborns with mild HIE have less neurological sequelae, and that the curative effect of hypothermia in such patients is not significant. Some studies found that newborns with mild HIE exhibit poor cognitive function in childhood [21], with lower memory score compared with the normal group [22]. In the present study, hypothermia improved the rates of neonatal death and 18-month disability. The time window of < 6 h led to better rates of 18-month disability, but without difference on death. Therefore, newborns with HIE could benefit from hypothermia treatment, but further studies with larger sample size are needed. In particular, it is difficult to evaluate the severity of HIE according to objective indexes early after birth, and only treating newborns with moderately severe HIE with hypothermia may be leaving out newborns that could be helped. In this study, newborns with mild HIE underwent hypothermia treatment for 72 h after informed consent was provided by their legal guardians. The findings suggest that delayed hypothermia therapy for newborns with HIE is effective, although further clinical studies are needed for confirmation. If hypothermia treatment is delayed by more than 6 h after birth, the best treatment window of HIE patients might be missed.
aEEG can sensitively reflect the change of brain physiology at the early stage of brain ischemic hypoxia. This is the only way to detect subclinical seizures and reversible changes of brain function [23, 24]. Some authors [25] indicated that aEEG can confirm encephalopathy within 6 h after HIE. Indeed, aEEG could predict abnormal neurological development with 82% specificity, 85% positive rate, and 100% negative rate. In the present study, aEEG was an effective method of monitoring the newborns since some improvements were seen in patients receiving hypothermia.
NSE is a soluble protein and exists in central nerve cells and peripheral nerve tissues, more specifically in neuroendocrine cells. It is very rare in normal body fluids (including blood and the cerebrospinal fluid). In case of neuronal injury and necrosis, the blood brain barrier is damaged [26]. Celtik et al. [27] demonstrated that NSE can be used as a quantitative marker of brain damage. This study revealed that NSE levels in newborns with moderately severe HIE were higher than in those with mild HIE before treatment. In addition, NSE levels were positively associated with the degree of brain damage. In HIE newborns and within 48 h, plasma NSE levels are significantly higher than control values, and even more significantly elevated in severe HIE, indicating that hypoxic ischemia and reperfusion injury is an important mechanism of HIE [28]. NSE levels are associated with disease course and with serious brain edema. It has been shown that NSE levels peak at 24 h after hypoxic brain damage [29]. Therefore, the time of specific peak in the disease course may still need to be assessed in studies with a large sample size.
Mild-to-moderate brain edema is reversible; therefore, patients with mild HIE, whose brain damage is still mostly at the state of brain edema, can be fully restored a week or so, even with routine treatment. As shown above, no difference in the curative effect of hypothermia treatment was found in newborns with mild HIE between the < 6 h and 6–12 h groups. In addition, these patients showed no differences compared with the control group, suggesting a good prognosis in newborns with mild HIE, even without hypothermia treatment. Nevertheless, long-term prognosis assessment and long-term follow-up are needed to investigate whether newborns with mild HIE would show long-term developmental issues such as cognitive dysfunction. This would determine whether such patients need hypothermia treatment at all.
A remarkable curative effect was obtained in newborns with moderate HIE for both time windows (< 6 h and 6–12 h) of hypothermia treatment, in disagreement with some reports [30]. In these patients, the series of biochemical reaction leading to serious hypoxic brain damage might not have started. Even after a long period of time, deterioration can still be prevented to a certain degree through effective treatment.
Severe brain edema entering the stage of neuron necrosis is irreversible. The cerebral blood flow decreases significantly within 12 h after severe asphyxia, and gradually increases by 24–120 h. By then, the brain is in a state of multiple perfusion, and has launched a series of biochemical reactions, with subsequent nerve cell necrosis and apoptosis. For severe hypoxic brain damage, even if the corresponding hypothermia treatment takes place and reduces the cerebral metabolic process beyond a certain time window, important neurons have already been involved in irreversible necrosis or even infarction. This explains the poor curative effect. Our findings corroborate numerous studies showing that hypothermia treatment of newborns with severe HIE at < 6 h after birth is useless [31].
This study is not without limitations. The sample size was small and from a single center. In addition, due to the principles of informed consent by family members regarding hypothermia treatment and because of the economic status and education background of the families, randomization was impossible. Finally, no follow-up was performed to examine the impact of treatment on long-term cognitive functions.
Conclusions
In newborns with moderate HIE, both time windows (< 6 h and 6–12 h) for starting hypothermia treatment showed curative effects. The treatment effects were better when the treatment was started early. Meanwhile, newborns with severe HIE only showed a therapeutic effect for hypothermia treatment beginning within 6 h. Good prognosis was obtained in newborns with mild HIE, even without hypothermia treatment. Whether newborns with mild HIE would show long-term developmental issues (such as cognitive dysfunction) needs to be assessed in long-term follow-up.
Acknowledgments
None
Funding
None
Availability of data and materials
The datasets analyzed during the current study will not be publicly available to protect patient confidentiality.
Author’s contributions
WJ carried out the studies, participated in collecting data, and drafted the manuscript. XL performed the statistical analysis, participated in its design and critically revised the manuscript. WD critically revised the manuscript. QL designed the study and critically revised the manuscript. All authors approved the final manuscript.
Abbreviations
- aEEG
Amplitude integrated electroencephalography
- ELISA
Enzyme-linked immunoassay
- HIE
Neonatal hypoxic-ischemic encephalopathy
- NSE
Neuron specific enolase
Ethics approval and consent to participate
This study was approved by the Ethics Committee of The Hospital Affiliated of Southwest Medical University. Written informed consent was obtained from the legal guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Wen Jia, Email: 512186895@qq.com.
Xiaoping Lei, Email: leixiaopingde@126.com.
Wenbin Dong, Email: dongwenbin2000@163.com.
Qingping Li, Phone: +86-15283084262, Email: lzlqp@126.com.
References
- 1.Jacobs SE, Morley CJ, Inder TE, Stewart MJ, Smith KR, McNamara PJ, Wright IM, Kirpalani HM, Darlow BA, Doyle LW, Infant Cooling Evaluation C. Whole-body hypothermia for term and near-term newborns with hypoxic-ischemic encephalopathy: a randomized controlled trial. Arch Pediatr Adolesc Med. 2011;165:692–700. doi: 10.1001/archpediatrics.2011.43. [DOI] [PubMed] [Google Scholar]
- 2.Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, Kapellou O, Levene M, Marlow N, Porter E, et al. Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med. 2009;361:1349–1358. doi: 10.1056/NEJMoa0900854. [DOI] [PubMed] [Google Scholar]
- 3.Edwards AD, Brocklehurst P, Gunn AJ, Halliday H, Juszczak E, Levene M, Strohm B, Thoresen M, Whitelaw A, Azzopardi D. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data. BMJ. 2010;340:c363. doi: 10.1136/bmj.c363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang LS, Cheng GQ, Zhou WH, Sun JQ, Cao Y, Shao XM. Meta-analysis of mild hypothermia for gestational age over 35-week newborns with hypoxic-ischemic encephalopathy. Zhonghua Yi Xue Za Zhi. 2012;92:1400–1404. [PubMed] [Google Scholar]
- 5.Kattwinkel J, Perlman JM, Aziz K, Colby C, Fairchild K, Gallagher J, Hazinski MF, Halamek LP, Kumar P, Little G, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:S909–S919. doi: 10.1161/CIRCULATIONAHA.110.971119. [DOI] [PubMed] [Google Scholar]
- 6.Gunn AJ, Gunn TR. The 'pharmacology' of neuronal rescue with cerebral hypothermia. Early Hum Dev. 1998;53:19–35. doi: 10.1016/S0378-3782(98)00033-4. [DOI] [PubMed] [Google Scholar]
- 7.Higgins RD, Raju T, Edwards AD, Azzopardi DV, Bose CL, Clark RH, Ferriero DM, Guillet R, Gunn AJ, Hagberg H, et al. Hypothermia and other treatment options for neonatal encephalopathy: an executive summary of the Eunice Kennedy Shriver NICHD workshop. J Pediatr. 2011;159:851–858. doi: 10.1016/j.jpeds.2011.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Diagnostic criteria for neonatal hypoxic-ischemic encephalopathy. Zhong guo Dang Dai Er Ke Za Zhi 2005, 7:97–98. [PubMed]
- 9.Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol. 1976;33:696–705. doi: 10.1001/archneur.1976.00500100030012. [DOI] [PubMed] [Google Scholar]
- 10.Shalak LF, Laptook AR, Velaphi SC, Perlman JM. Amplitude-integrated electroencephalography coupled with an early neurologic examination enhances prediction of term infants at risk for persistent encephalopathy. Pediatrics. 2003;111:351–357. doi: 10.1542/peds.111.2.351. [DOI] [PubMed] [Google Scholar]
- 11.Group NFPoHTC Treatment of neonatal hypoxic ischemic encephalopathy (draft) Chin J Pract Pediatr. 2000;15:381–382. [Google Scholar]
- 12.Shao X. Programme of mild hypothermia treatment for hypoxic-ischemic encephalopathy in neonates. Chin J Evid Based Pediatr. 2011;6:337–339. [Google Scholar]
- 13.Shah NA, Wusthoff CJ. How to use: amplitude-integrated EEG (aEEG) Arch Dis Child Educ Pract Ed. 2015;100:75–81. doi: 10.1136/archdischild-2013-305676. [DOI] [PubMed] [Google Scholar]
- 14.Burdjalov VF, Baumgart S, Spitzer AR. Cerebral function monitoring: a new scoring system for the evaluation of brain maturation in neonates. Pediatrics. 2003;112:855–861. doi: 10.1542/peds.112.4.855. [DOI] [PubMed] [Google Scholar]
- 15.Vasiljevic B, Maglajlic-Djukic S, Gojnic M, Stankovic S, Ignjatovic S, Lutovac D. New insights into the pathogenesis of perinatal hypoxic-ischemic brain injury. Pediatr Int. 2011;53:454–462. doi: 10.1111/j.1442-200X.2010.03290.x. [DOI] [PubMed] [Google Scholar]
- 16.Arca G, Garcia-Alix A, Arnaez J, Blanco D. Sedation in term or near-term newborns with hypoxic-ischemic encephalopathy who require therapeutic hypothermia. An Pediatr (Barc) 2015;82:52–53. doi: 10.1016/j.anpedi.2014.04.030. [DOI] [PubMed] [Google Scholar]
- 17.Arnaez J, Vega C, Garcia-Alix A, Gutierrez EP, Caserio S, Jimenez MP, Castanon L, Esteban I, Hortelano M, Hernandez N, et al. Multicenter program for the integrated care of newborns with perinatal hypoxic-ischemic insult (ARAHIP) An Pediatr (Barc) 2015;82:172–182. doi: 10.1016/j.anpedi.2014.05.006. [DOI] [PubMed] [Google Scholar]
- 18.Merchant N, Azzopardi D. Early predictors of outcome in infants treated with hypothermia for hypoxic-ischaemic encephalopathy. Dev Med Child Neurol. 2015;57 Suppl 3:8–16. doi: 10.1111/dmcn.12726. [DOI] [PubMed] [Google Scholar]
- 19.Li T, Xu F, Cheng X, Guo X, Ji L, Zhang Z, Wang X, Blomgren K, Simbruner G, Zhu C. Systemic hypothermia induced within 10 hours after birth improved neurological outcome in newborns with hypoxic-ischemic encephalopathy. Hosp Pract (1995) 2009;37:147–152. doi: 10.3810/hp.2009.12.269. [DOI] [PubMed] [Google Scholar]
- 20.Zhou WH, Cheng GQ, Shao XM, Liu XZ, Shan RB, Zhuang DY, Zhou CL, Du LZ, Cao Y, Yang Q, Wang LS: Selective head cooling with mild systemic hypothermia after neonatal hypoxic-ischemic encephalopathy: a multicenter randomized controlled trial in China. J Pediatr 2010, 157:367–372, 372.e361–363. [DOI] [PubMed]
- 21.van Handel M, Swaab H, de Vries LS, Jongmans MJ. Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal asphyxia: a review. Eur J Pediatr. 2007;166:645–654. doi: 10.1007/s00431-007-0437-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.de Vries LS, Jongmans MJ. Long-term outcome after neonatal hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed. 2010;95:F220–F224. doi: 10.1136/adc.2008.148205. [DOI] [PubMed] [Google Scholar]
- 23.Padden B, Scheer I, Brotschi B, Wohlrab G, Latal B, Bernet V. Does amplitude-integrated electroencephalogram background pattern correlate with cerebral injury in neonates with hypoxic-ischaemic encephalopathy? J Paediatr Child Health. 2015;51:180–185. doi: 10.1111/jpc.12697. [DOI] [PubMed] [Google Scholar]
- 24.Werther T, Olischar M, Giordano V, Czaba C, Waldhoer T, Berger A, Pollak A, Deindl P. Bispectral index and lower margin amplitude of the amplitude-integrated electroencephalogram in neonates. Neonatology. 2015;107:34–41. doi: 10.1159/000365277. [DOI] [PubMed] [Google Scholar]
- 25.Jiang CM, Yang YH, Chen LQ, Shuai XH, Lu H, Xiang JH, Liu ZL, Zhu YX, Xu RY, Zhu DR, Huang XM. Early amplitude-integrated EEG monitoring 6 h after birth predicts long-term neurodevelopment of asphyxiated late preterm infants. Eur J Pediatr. 2015;174:1043–1052. doi: 10.1007/s00431-015-2490-z. [DOI] [PubMed] [Google Scholar]
- 26.Lv H, Wang Q, Wu S, Yang L, Ren P, Yang Y, Gao J, Li L. Neonatal hypoxic ischemic encephalopathy-related biomarkers in serum and cerebrospinal fluid. Clin Chim Acta. 2015;450:282–297. doi: 10.1016/j.cca.2015.08.021. [DOI] [PubMed] [Google Scholar]
- 27.al Naqeeb N, Edwards AD, Cowan FM, Azzopardi D. Assessment of neonatal encephalopathy by amplitude-integrated electroencephalography. Pediatrics. 1999;103:1263–1271. doi: 10.1542/peds.103.6.1263. [DOI] [PubMed] [Google Scholar]
- 28.Sun J, Li J, Cheng G, Sha B, Zhou W. Effects of hypothermia on NSE and S-100 protein levels in CSF in neonates following hypoxic/ischaemic brain damage. Acta Paediatr. 2012;101:e316–e320. doi: 10.1111/j.1651-2227.2012.02679.x. [DOI] [PubMed] [Google Scholar]
- 29.Celik Y, Atici A, Gulasi S, Makharoblidze K, Eskandari G, Sungur MA, Akbayir S. The effects of selective head cooling versus whole-body cooling on some neural and inflammatory biomarkers: a randomized controlled pilot study. Ital J Pediatr. 2015;41:79. doi: 10.1186/s13052-015-0188-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tagin MA, Woolcott CG, Vincer MJ, Whyte RK, Stinson DA. Hypothermia for neonatal hypoxic ischemic encephalopathy: an updated systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2012;166:558–566. doi: 10.1001/archpediatrics.2011.1772. [DOI] [PubMed] [Google Scholar]
- 31.Thoresen M, Whitelaw A. Therapeutic hypothermia for hypoxic-ischaemic encephalopathy in the newborn infant. Curr Opin Neurol. 2005;18:111–116. doi: 10.1097/01.wco.0000162850.44897.c6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study will not be publicly available to protect patient confidentiality.