

Abstract
Objectives
Developing compassion towards oneself has been linked to improvement in many areas of psychological well‐being, including psychosis. Furthermore, developing a non‐judgemental, accepting way of relating to voices is associated with lower levels of distress for people who hear voices. These factors have also been associated with secure attachment. This study explores associations between the constructs of mindfulness of voices, self‐compassion, and distress from hearing voices and how secure attachment style related to each of these variables.
Design
Cross‐sectional online.
Method
One hundred and twenty‐eight people (73% female; M age = 37.5; 87.5% Caucasian) who currently hear voices completed the Self‐Compassion Scale, Southampton Mindfulness of Voices Questionnaire, Relationships Questionnaire, and Hamilton Programme for Schizophrenia Voices Questionnaire.
Results
Results showed that mindfulness of voices mediated the relationship between self‐compassion and severity of voices, and self‐compassion mediated the relationship between mindfulness of voices and severity of voices. Self‐compassion and mindfulness of voices were significantly positively correlated with each other and negatively correlated with distress and severity of voices.
Conclusion
Mindful relation to voices and self‐compassion are associated with reduced distress and severity of voices, which supports the proposed potential benefits of mindful relating to voices and self‐compassion as therapeutic skills for people experiencing distress by voice hearing.
Practitioner points
Greater self‐compassion and mindfulness of voices were significantly associated with less distress from voices. These findings support theory underlining compassionate mind training.
Mindfulness of voices mediated the relationship between self‐compassion and distress from voices, indicating a synergistic relationship between the constructs.
Although the current findings do not give a direction of causation, consideration is given to the potential impact of mindful and compassionate approaches to voices.
Keywords: hearing voices, auditory hallucinations, psychosis, compassion, mindfulness, attachment, mediation
Background
Hearing voices others do not hear is a relatively common experience with prevalence ranging between 0.6% and 84% in the general population (Beavan, Read, & Cartwright, 2011) though frequently associated with psychosis (McCarthy‐Jones, 2012). The psychological impact varies between individuals: for some, voices can be positive and comforting; for others, dominant and distressing (McCarthy‐Jones, 2012). Understanding the reasons why some people experience voices as distressing and others as positive is important to providing support that will reduce distress. Distress, which is characterized by ‘threat emotions’ such as fear, anxiety, shame, and anger (Freeman & Garety, 2003), can increase the intensity and hostility of voices (Romme, Honig, Noorthorn, & Escher, 1992). Influencing factors include negative content (Beavan & Read, 2010), intrusiveness (Sorrell, Hayward, & Meddings, 2010), beliefs about voices (Birchwood & Chadwick, 1997), and active resistance or confrontation with voices (Singh, Sharan, & Kulhara, 2003; Vaughan & Fowler, 2004). These findings suggest the process by which an individual relates and applies meaning to their voices has a significant role in mediating distress, in line with early theoretical work that posits acceptance of voices is essential to coping (Romme & Escher, 1989).
Relating and responding mindfully to voices is proposed as a way of alleviating distress experienced (Chadwick, Barnbrook, & Newman‐Taylor, 2007). Mindfully relating to voices involves accepting and ‘decentring’ from the experience, that is, experiencing thoughts and emotions as transient mental events rather than as truths, maintaining a non‐judgemental stance and allowing it to pass (Hargus, Crane, Barnhofer, & Williams, 2010). This is in contrast with reacting to unpleasant voices with confrontation, judgement, rumination, or avoidance, which appears to increase distress (Chadwick, Birchwood, & Trower, 1996; Chadwick, Newman‐Taylor, & Abba, 2005). Low meta‐awareness is characterized by an inability to distinguish the self from the content of negative thoughts and emotions, such that the self is defined by or is synonymous with negative mental phenomenon (Segal, Williams, & Teasdale 2002). Mindfulness practices create the opportunity for individuals to perceive distance between themselves and their thoughts, emotions, and experiences. In this way, one's thoughts are viewed as ‘events in the mind rather than necessarily being reflections of reality or accurate self‐view’ (Feldman, Greeson, & Seville, 2010, p. 1002). When separated from events (internal or otherwise), negative events may be decoupled from the self and become less threatening (Glomb, Duffy, Bono, & Yang, 2011). This adoption of a mindful approach to voices involves changing the relationship an individual has with their voices and increasing meta‐awareness, rather than preventing the voices from occurring.
Recent developments in mindfulness‐based research (Khoury et al., 2013a; Radford et al., 2014) distinguish between two levels of the construct: ‘trait’ level, an individual's natural disposition to be mindful, and ‘state’ level, a person's ability to be mindful following experiential mindfulness meditation practice. It is has been shown that those who regularly practice mindfulness meditation show shifts in state mindfulness post‐meditation, and increased levels of trait mindfulness over time, which is in turn protective against distress (Khoury et al., 2013a; Kiken, Garland, Bluth, Palsson, & Gaylord, 2015). Cross‐sectional surveys examining the associations between trait mindfulness in populations without meditation experience and outcomes of interest are based on the premise that all humans have the capacity to be mindful and that there is individual difference in the extent to which people can be described as mindful (Brown & Ryan, 2003; Kabat‐Zinn, 2003). Commonality between state and trait mindfulness is argued to rest in the premise that practicing state mindfulness leads to increased trait mindfulness (Chiesa, 2013). In relation to experiencing distress from hearing voices, increased trait mindfulness of voices has been found to be negatively correlated with distress (Chadwick et al., 2007; Newman‐Taylor, Harper, & Chadwick, 2009; Strauss, Thomas, & Hayward, 2015; Úbeda‐Gómez et al., 2015). In a grounded theory study, participants described being mindful of voices as something that provided freedom from distress (Abba, Chadwick, & Stevenson, 2008).
Distress from voices has also been linked to mechanisms underlying threat regulation. Gilbert (2009) suggests self‐compassion plays a role in activating the ‘soothing system’, a neural system associated with the regulation of threat emotions. Self‐compassion is conceptualized as the ability to relate to distressing feelings with kindness, common humanity, and mindful awareness (Depue & Morrone‐Strupinsky, 2005; Neff, 2003). Self‐compassion has been shown to be negatively correlated with distress from voices (Mayhew & Gilbert, 2008), and the presence of voices and unusual beliefs (Eicher, Davis, & Lysaker, 2013). These findings are supported in a case study in which development of self‐compassion was described as useful in management of distress from critical voices (Kennedy & Ellerby, 2016)
Birchwood et al. (2004) suggest that the way individuals relate interpersonally also influences the way they relate to their voices. Interpersonal relating is theorized to stem from attachment experiences with primary caregivers (Bowlby, 1973). Although definitions of attachment are inconsistent in the literature, it is generally accepted that there is a difference between ‘secure’ and ‘insecure’ attachment. Bartholomew and Horowitz (1991) propose a four‐category model of attachment style in adulthood. First, secure attachment refers to those with a positive relationship with self and others. Second, fearful‐avoidant refers to those who have a negative view of self and fear rejection from others. Third, dismissing‐avoidant refers people who are self‐reliant and avoid intimacy with others, and finally, preoccupied individuals are reliant on others to bolster their low self‐esteem. Studies have shown insecure attachment styles to be related to increased distress from voices (Berry, Wearden, Barrowclough, Oakland, & Bradley, 2011); fearful attachment has also been associated with severity of voices specifically (Ponizovsky, Vitenberg, Baumgarten‐Katz, & Grinshpoon, 2013). In contrast, secure attachment has been associated with an increased capacity for mindfulness (Shaver, Lavy, Saron, & Mikulincer, 2007) and self‐compassion (Gilbert & Procter, 2006; Wei, Liao, Ku, & Shaffer, 2011). Based on these findings, secure attachment is also considered a potential mediator in the relationships between mindfulness and self‐compassion and psychological difficulties, such as voice hearing and/or associated distress. Moreover, secure attachment appears to be highly correlated with self‐compassion, though appears to remain a distinct construct. Secure attachment is thought to be formed through experience of compassion from caregivers, therefore may be causally linked to the development of self‐compassion as an internal mechanism (Gillath, Shaver, & Mikulincer, 2005).
Self‐compassion has been identified as important or relevant in studies that have shown mindfulness helps with depression (Kuyken et al., 2010), perceived stress (Shapiro, Astin, Bishop, & Cordova, 2005), and well‐being (Hollis‐Walker & Colosimo, 2011). Furthermore, several studies have demonstrated that self‐compassion moderates the clinical effect size of mindfulness for psychosis outcomes (Khoury, Lecomte, Gaudiano, & Paquin, 2013b). Mindfulness has also been found to mediate positive clinical outcome in interventions for depression (Kuyken et al., 2010). These findings show that there is a clear link between mindfulness and self‐compassion and outcomes in psychosis although the directionality and interrelation between these constructs have not been closely examined, with both being potential mediators. Furthermore, to date no known studies have investigated self‐compassion and mindfulness of voices together in relation to distressing voices.
The primary aim of this study was to explore associations between factors hypothesized to relate to the alleviation of distress associated with hearing voices, in order to provide further insight and evidence for therapeutic approaches. This study investigates the following hypotheses:
Mindfulness of voices and self‐compassion will be negatively correlated with severity of voices.
Secure attachment will be correlated positively with mindfulness of voices and self‐compassion, and negatively with severity of voices.
Self‐compassion will mediate the relationship between mindfulness of voices and severity of voices.
Secure attachment will mediate the relationship between mindfulness of voices and severity of voices.
Mindfulness of voices will mediate the relationship between self‐compassion and severity of voices.
Method
Participants
One hundred and twenty‐eight people who currently hear voices and aged 18 years and over completed an online survey. Data from participants not completing the survey were not included in the analysis, see Figure 1 for full details. See Table 1 for demographic details of the sample.
Figure 1.
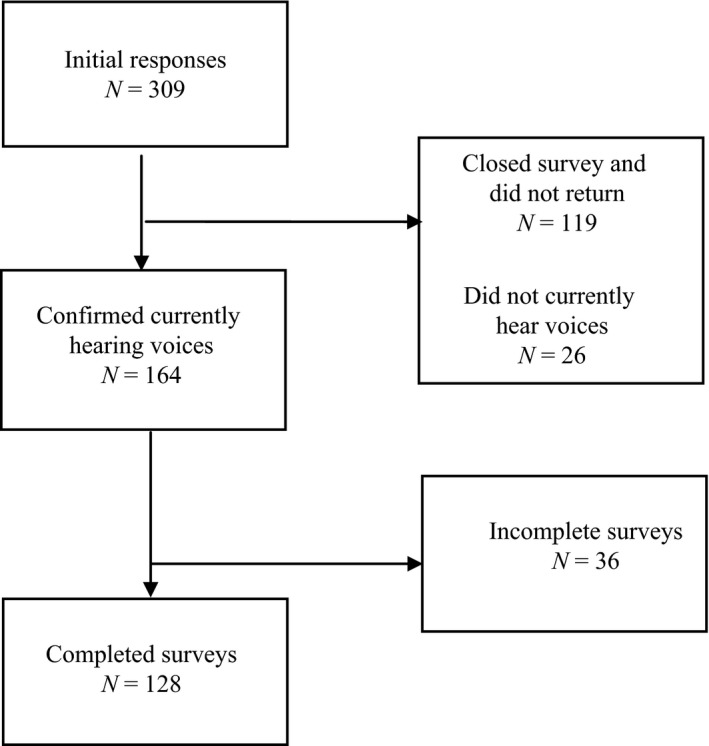
Flow chart of participants study completion.
Table 1.
Participant demographic data
| N | % | ||
|---|---|---|---|
| Age (years) | |||
| Mean | 37.6 | – | – |
| Range | 18–74 | – | – |
| Gender | |||
| Male | 14 | 27 | |
| Female | 94 | 73 | |
| Ethnicity | |||
| Caucasian | 112 | 87.5 | |
| Latin/Hispanic | 3 | 2.3 | |
| Middle Eastern | 1 | 0.8 | |
| African | 1 | 0.8 | |
| South Asian | 1 | 0.8 | |
| East Asian | 1 | 0.8 | |
| Mixed | 4 | 3.1 | |
| Other | 4 | 3.1 | |
| Employment | |||
| Full‐time | 27 | 21 | |
| Part‐time | 11 | 8.6 | |
| Self‐employed | 6 | 4.7 | |
| Student | 21 | 16.4 | |
| Unable to work | 38 | 29.7 | |
| Out of work and looking | 6 | 4.7 | |
| Out of work not looking | 4 | 3.1 | |
| Voluntary | 5 | 3.9 | |
| Retired | 5 | 3.9 | |
| Salary | |||
| <£10,000 | 64 | 50 | |
| £10,000–£19,999 | 32 | 25 | |
| £20,000–£29,000 | 13 | 10.2 | |
| >£29,000 | 17 | 13.3 | |
| Diagnosis | |||
| Yes | 107 | 84 | |
| Proportion ICD‐10 F20‐F29 | 56 | 52 | |
| No | 21 | 16.4 | |
| Accessing mental health services | |||
| Currently | 81 | 63 | |
| Past | 116 | 91 | |
| Never | 12 | 9.4 | |
| Medication | |||
| Current use | 81 | 63 | |
| Proportion antipsychotics | 63 | 77 | |
| Past use | 34 | 27 | |
| Never | 13 | 10 | |
| Mindfulness‐based therapy intervention | |||
| Accessed | 45 | 35 | |
| Not accessed | 83 | 65 | |
| Mindfulness course | |||
| Accessed | 51 | 40 | |
| Structured group weekly format | 31 | 24 | |
| Short course | 10 | 8 | |
| Online course | 12 | 9 | |
| Taster day | 8 | 6 | |
| Mobile app | 6 | 5 | |
| Self‐help book | 23 | 18 | |
| Not accessed | 77 | 60 | |
| Mindfulness practice | |||
| Daily | 22 | 17 | |
| Weekly | 18 | 14 | |
| Monthly | 6 | 5 | |
| Past | 34 | 27 | |
| Never | 48 | 38 | |
Note. ICD‐10 Codes refer to International Classification of Diseases 10th Revision (World Health Organization, 1992) diagnostic categories: F20‐F29 schizophrenia, schizotypal and delusional, and other non‐mood psychotic disorders.
Measures
Self‐Compassion Scale (SCS; Neff, 2003)
The SCS is a 26‐item questionnaire with a five‐point Likert scale, rated almost never (1) to almost always (5) giving a maximum total score of 130. Six constructs of self‐compassion are measured: self‐kindness, self‐judgement, common humanity, mindfulness, isolation, and over‐identification. Negative constructs are reverse coded, and the total score indicates overall level of self‐compassion. The scale has been shown to have good test–retest reliability (r = .93) and internal consistency (Cronbach's α = .92; Neff, 2003), also maintained in this study (Cronbach's α = .94). Total scores were included in the study.
Southampton Mindfulness of Voices Questionnaire (SMVQ; Chadwick et al., 2007)
The SMVQ is a 16‐item questionnaire with a seven‐point Likert scale rated from ‘disagree totally’ (0) to agree totally (6), giving a maximum total score of 96. The SMVQ measures how mindfully an individual responds to their voices across four constructs: (1) clarity of awareness of the present moment versus being unaware and lost to the voice; (2) allowing attention to maintain with unpleasant sensations versus experiential avoidance; (3) accepting difficult situations and of oneself versus judgement of the situation and self; and (4) letting go versus struggle and rumination. The SMVQ has been found to be a reliable and valid measure (Cronbach's α = 0.84; Chadwick et al., 2007) and yielded high internal consistency in this study (Cronbach's α = .89). Total scores were used in the study.
The Hamilton Program for Schizophrenia Voices Questionnaire (HPSVQ; Van Lieshout & Goldberg, 2007)
The HPSVQ is a nine‐item questionnaire with a five‐point Likert scale rated from 0 to 4, measuring severity of voices. The items measure frequency, negative content, loudness, distress, impact on self‐appraisal, clarity, and compliance with commands. The scale has been found to have excellent test–retest reliability (r = .84) and internal consistency (Cronbach's α = .94; Kim et al., 2010), replicated with good internal consistency in this study (Cronbach's α = .88). The scale yields a total score for severity of scores, this was included in the study alongside an examination of the distress from voices item specifically.
The Relationship Questionnaire (RQ; Bartholomew & Horowitz, 1991)
The RQ is a measure of adult attachment comprising of four statements describing different attachment styles: secure, dismissing, preoccupied, and fearful. This is followed by four questions measuring how closely the participant identifies with each statement, providing four continuous measures of attachment style on a seven‐point Likert scale rated from disagree strongly (1), neutral/mixed (4) to agree strongly (7). Participants are also asked to select the paragraph which best describes their experience, providing a categorical measure. Internal reliability could not be analysed as each construct contains one item, although past research has found the measure to be reliable and stable over time and when compared to other attachment measures (Scharfe & Bartholomew, 1994). All subscales were used in the study, although the secure attachment scale was of primary interest.
Design, sample size and ethics
The study was a Web‐based survey with a cross‐sectional design. Apriori power analysis using G*Power 3 (Faul, Erdfelder, Buchner, & Lang, 2009) indicated a sample of at least 127 participants would be required to reach .80 power, based on 12 predictors, with a medium effect size (f 2 = 0.15) in line with Cohen's (1977) guidelines for behavioural sciences. Prior to submission for ethical review, the study design and materials were considered with a hearing voices group and a service user and carer research evaluation group. Changes were made to advertising material, and a research blog was created based on recommendations. The study received ethical approval from the University of Liverpool Non‐Invasive Subcommittee (RETH000825, 01/05/15) and followed the British Psychological Society (BPS) code of human research ethics (BPS, 2010) and ethics guidelines for Internet‐mediated research (BPS, 2013).
Procedure
An online survey was created using Qualtrics (2016) software and distributed online across social media, forums, university announcements, and a research blog. The survey was also advertised via the Hearing Voices Network and Intervoice websites and approved non‐NHS UK locations using posters and leaflets. Participants volunteered to take part by responding to the advertisements and were required to read an information sheet and indicate informed consent before completing the study measures. Participants could withdraw by closing the survey at any time. Participants were then debriefed and offered the opportunity to enter into a prize draw, of which six participants won a £25 voucher. Signposting information to national and international support charities was presented as part of the debriefing sheet.
Data analysis procedure
All analysis was completed using SPSS v23 (IBM, 2015). Data were prepared by removing incomplete data sets, computing reverse‐scored measures, subscales, and total scores. String variables and groups were coded appropriately for analysis. Normality assumptions were tested using visual assessment of histograms and Q–Q plots, Kolmogorov–Smirnov, and Levene's tests. HPSVQ total was not normally distributed. Total scores for HPSVQ, SMVQ, and SCS were square‐root transformed to be used together in parametric analysis and met assumptions for parametric testing (Field, 2009). All attachment variables and all subscales except SMVQ ‘mindful observation’ and ‘letting go’ violated normality assumptions. As transformation and standardizing z‐scores did not substantially change distribution, nonparametric tests were used for correlational analyses including these measures.
Correlational analysis was used to test hypotheses one and two. Bonferroni correction was applied to adjust for multiple testing, yielding p < .003. Mediation analyses were undertaken to test hypotheses three, four, and five. Mediation analysis followed the Hayes (2013) method (model four from the PROCESS macro for SPSS). Bias‐corrected and accelerated bootstrap percentile confidence intervals (5,000 resamples) are presented for total and indirect effects. 95% confidence intervals that do not contain zero between upper and lower bounds indicated significant mediation. Regression diagnostics were all within acceptable ranges.
Results
Means, standard deviations, and correlational results are reported in Table 2.
Table 2.
Means, standard deviations, and correlational data for all measures and subscales
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Secure attachment | 1 | |||||||
| 2 | Fearful attachment | −.45* | 1 | ||||||
| 3 | Preoccupied attachment | −.14 | .14 | 1 | |||||
| 4 | Dismissing attachment | −.08 | −.15 | −.13 | 1 | ||||
| 5 | Self‐compassion total | .38* | −.42* | −.26 | .13 | 1 | |||
| 6 | Mindfulness of voices total | .30* | −.27* | −.06 | .09 | .58 * | 1 | ||
| 7 | Severity of voices total | −.21 | .21 | .03 | −.10 | −.51 * | −.73 * | 1 | |
| 8 | Distress from voices item | −.19 | .24 | .06 | −.18 | −.45* | −.79* | .83* | 1 |
| Mean | 3.4 | 4.87 | 3.24 | 4.32 | 2.59 | 44.86 | 21.63 | 2.41 | |
| SD | 2.1 | 1.98 | 1.87 | 0.23 | 0.75 | 17.91 | 8.34 | 1.42 |
Note. N = 128.
*p < .003 (alpha adjusted by Bonferroni correction); Italics = Pearson's r, none‐italics = Spearman's rho.
Correlational analysis
Results supported hypotheses one and two, namely that severity of and distress from voices were negatively associated with mindfulness of voices and self‐compassion (see Table 2). Hypothesis two was also supported, with secure attachment positively associated with mindfulness of voices and self‐compassion. Partial support was indicated for secure attachment as a negative association with severity of voices, although not significant when applying Bonferroni correction (r = −.21, p = .02). In contrast, fearful attachment was correlated with mindfulness of voices (r = −.27, p = .002), self‐compassion (r = −.42, p < .001), and severity of voices (r = .21, p = .02), again the latter was no longer significant when applying Bonferroni correction (p < .003). In addition to the hypothesized correlations, significant associations were found between secure attachment and self‐compassion (r = .38, p < .003) and fearful attachment and self‐compassion (r = −.42, p = <.003).
Mediation analysis
Mediation analysis results are presented in Table 3. Model 1 tests the hypothesis that self‐compassion mediates the relationship between mindfulness of voices and severity of voices (see Figure 2). The total and direct effects of mindfulness of voices and severity of voices were significant (with confidence intervals of LLCI = −.64, ULCI = −.46 and LLCI = −.59, ULCI = −.37, respectively). The hypothesis is supported in that self‐compassion mediates the relationship between mindfulness of voices and severity of voices, as the zero is not within the interval of confidence, only at one end (rather that in the centre of the interval of confidence; LLCI = −.14, ULCI = .00). Furthermore, paths a and b are significant, which also shows the significance of the indirect effect (see Figure 2). Model 2 tests the hypothesis that secure attachment will mediate the relationship between mindfulness of voices and severity of voices (see Figure 3). Again the total and direct effects of mindfulness on severity of voices were significant (with confidence intervals of LLCI = −.64, ULCI = −.46 and LLCI = −.65, ULCI = −.45, respectively). However, the hypothesis was not supported as secure attachment did not significantly mediate the relationship between mindfulness of voices and severity of voices (LLCI = −.02, ULCI = .05). Finally, Model 3 tests the hypothesis that the relationship between self‐compassion and severity of voices would be mediated by mindfulness of voices (see Figure 4). The total and direct effects were significant (with confidence intervals of LLCI = −2.95, ULCI = −1.61 and LLCI = −1.32, ULCI = −.02, respectively). This mediation hypothesis was supported as mindfulness of voices significantly mediated the relationship between self‐compassion and severity of voices (LLCI = −2.19, ULCI = −1.10).
Table 3.
Mediation analysis results
| Path a | Path b | Path c | Path c’ | Sobel test | Mediation effect interval of confidence (95%) | |||
|---|---|---|---|---|---|---|---|---|
| (X→M) | (M→Y) | (X→Y) | Direct effect | Effect (boot SE) | LLCI to ULCI | K 2 | ||
| Model 1: X = mindfulness of voices; M = self‐compassion; Y = severity of voices | ||||||||
| b(SE) | 0.10 (0.01) | −0.67 (0.33) | −0.55 (0.46) | −0.48 (0.56) | Z = −1.97 | −0.06 (0.04) | −0.14 to 0.00 | 0.11 |
| p‐values | <.001** | .04* | <.001** | <.001** | .049* | |||
| Model 2: X = mindfulness of voices; M = secure attachment; Y = severity of voices | ||||||||
| b(SE) | 0.47 (0.13) | 0.02 (0.03) | 0.04 (0.34) | −0.56 (0.05) | Z = −3.24 | 0.01 (0.02) | −0.02 to 0.05 | −0.02 |
| p‐values | <.001** | .56 | <.001** | <.001** | <.001** | |||
| Model 3: X = self‐compassion; M = mindfulness of voices; Y = severity of voices | ||||||||
| b(SE) | 3.33 (0.43) | −0.48 (0.06) | −2.28 (0.34) | −0.67 (0.33) | Z = −5.74 | −1.61 (0.27) | −2.19 to −1.13 | 0.09 |
| p‐values | <.001** | <.001** | <.001** | .04* | <.001** | |||
Note. X = predictor variable; Y = outcome variable; M = mediator variable.
**p < .001; *p < .05.
Figure 2.
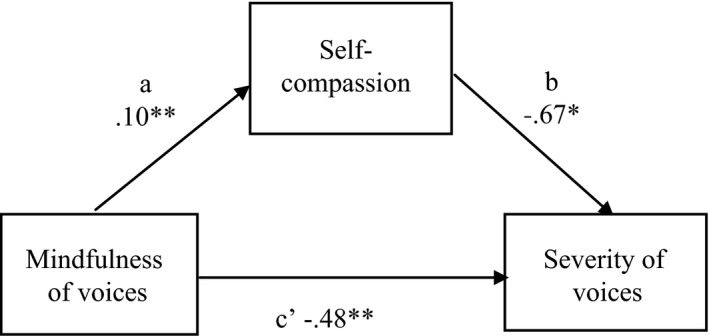
Regression coefficients for the relationship between mindfulness of voices and severity of voices as mediated by self‐compassion. *p < .05, **p < .001.
Figure 3.
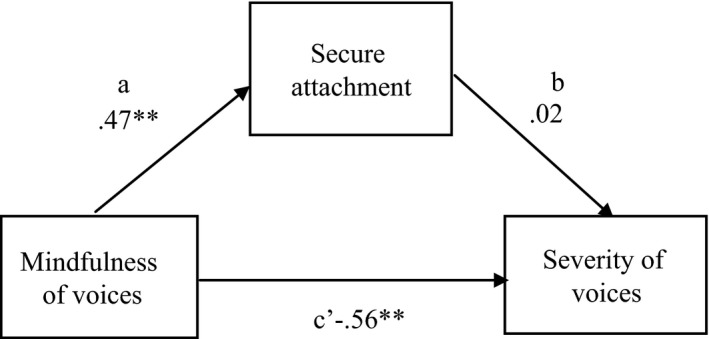
Regression coefficients for the relationship between mindfulness of voices and severity of voices as mediated by secure attachment. **p < .001.
Figure 4.
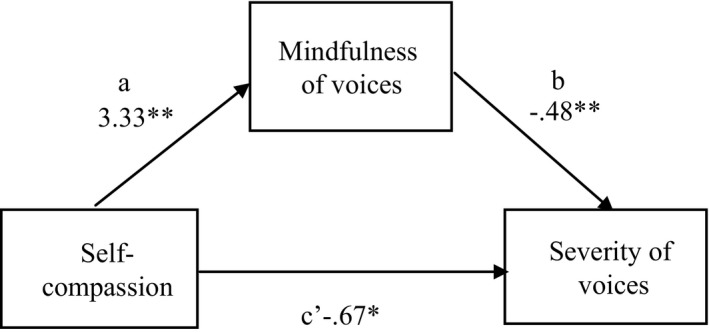
Regression coefficients for the relationship between self‐compassion and severity of voices as mediated by mindfulness of voices. *p < .05, **p < .001.
Discussion
This study demonstrated that mindfulness of voices, self‐compassion, and secure attachment were positively associated with each other and negatively associated with distress/severity of voices. Self‐compassion emerged as significantly correlated with lower distress and severity of voices, supporting the limited range of past findings related to hearing voices (Eicher et al., 2013; Mayhew & Gilbert, 2008), and the suggestion that self‐compassion may play a part in self‐soothing and regulation of feelings of threat (Gilbert, 2009). However, the findings may also imply that those who are highly distressed by their voices are not as able to access feelings of self‐compassion. This interpretation is aligned with the theoretical underpinnings of compassion as a psychological construct that suggest people in a state of threat or who feel unsafe are unlikely to access the ‘soothing system’ as it is of evolutionary disadvantage leaving people feeling vulnerable to attack and less likely to report feelings of self‐compassion (Gilbert, 2009).
Mindfulness of voices was shown to be most strongly associated with lower distress and severity of voices, replicating past research (Chadwick et al., 2007; Úbeda‐Gómez et al., 2015). These results suggest that trait mindfulness may have a role in reduced distress from voices as noted in a recent systematic review (Strauss et al., 2015). Furthermore, the findings support the notion that trait mindfulness may be a protective factor against distressing cognitions or experiences (Khoury et al., 2013a; Radford et al., 2014). However, the findings may also mean that those with highly intrusive and distressing voices have difficulties focusing on the present moment and maintaining a non‐judgemental stance towards their experiences. Future studies would benefit from further investigating direction of causality.
Self‐compassion mediated the relationship between mindfulness of voices and distress/severity of voices, in line with past findings investigating other areas of mental health (Hollis‐Walker & Colosimo, 2011; Shapiro et al., 2005). Moreover, mindfulness of voices significantly mediated the relationship between self‐compassion and distress/severity of voices, supporting our hypothesis and past findings indicating mindfulness as a mediator of positive clinical outcomes (Kuyken et al., 2010; Strauss, 2014).
Higher secure attachment scores correlated with increased self‐compassion and mindfulness of voices and reduced with severity and distress from voices, although the latter finding became non‐significant following Bonferroni correction. These findings support past literature suggesting those with secure attachment have more capacity for self‐compassion (Gilbert & Procter, 2006; Wei et al., 2011) and mindfulness (Shaver et al., 2007). However, hypothesis four was not supported as secure attachment did not mediate the relationship between mindfulness and severity/distress from voices. In addition to the hypothesized findings, it was found that fearful attachment was the only insecure attachment style significantly associated with lower self‐compassion. Gilbert, McEwan, Matos, and Rivis (2011) suggest that ‘fears of compassion’ are crucial to resolve in order to experience self‐compassion and that those from ‘low affection or abusive backgrounds’ are more likely to have fears of self‐compassion. Given those with fearful attachment styles are likely to have experienced highly aversive or abusive attachment relationships, it may be that they are more predisposed to be more fearful of compassion, including self‐compassion. No significant association was found between insecure attachment styles and severity/distress from voices, and the reasons for this are unclear and warrant further research.
Finally, the authors consciously decided against setting diagnosis of a schizophrenia or psychosis‐related disorder as an inclusion criterion in the present study; only 52% of participants self‐reported having received a diagnosis of schizophrenia or other psychosis‐related diagnoses. This trend in our participant sample supports prevalence studies reporting hearing voices as a relatively common experience (Beavan, et al., 2011), and we suggest future research on voice hearing may improve generalizability of findings by including those who do not have a psychosis‐related diagnosis.
Limitations
Several limitations should be noted: firstly, the inability to infer the direction of causation due to the cross‐sectional design, and secondly, the small number of measures completed, which, although intended to reduce participant burden, limited the number of potential confounds measured. Furthermore, although the attachment measure chosen is widely used in research, it is not as comprehensive as interview‐based measures. It should also be noted that the sample was also biased towards female Caucasians with access to the Internet, which may hinder generalizability. Future research may benefit from recruiting participants from a broader range of ethnic backgrounds to explore potential differences, particularly between Eastern and Western cultures. Furthermore, collecting data on participant nationality may aid in distinguishing cultural difference. Of interest, demographics showed large proportions of people with experience of practising mindfulness, which may indicate that people have access, or are aware of mindfulness as a therapeutic tool for mental health difficulties. Finally, it is important to consider that as no self‐report measures of distress from voices currently exist (Thomas, 2014), total severity score from the HPSVQ (Van Lieshout & Goldberg, 2007) was used as analogous to distress from voices in regression and mediation analysis. Although distress was highly correlated with severity, there may be differences between the constructs that impact on interpretation of the findings in this study. Longitudinal research would be useful to assess whether the relationships observed here are maintained over time. Moreover, development of a validated self‐report measure specific to distress from voices would provide a more consistent construct.
Clinical implications
Although the study design was cross‐sectional, the findings provide support for the emerging evidence base of mindfulness‐based and compassion‐focused therapies for people who are distressed by their voices (Chadwick, Hughes, Russell, Russell, & Dagnan, 2009; Chadwick et al., 2016; Eicher et al., 2013; Mayhew & Gilbert, 2008) as well as some insight into the mechanisms involved. The findings support theory underpinning compassionate mind training (CMT; Gilbert & Procter, 2006). Secure attachment is associated with positive experiences with primary caregivers, fostering development of the mammalian caregiving system and feelings of security, safety, warmth, and soothing, attributes which tend to continue into adulthood (Gillath et al., 2005). Those with this attachment style are therefore likely to have higher pre‐existing levels of trait self‐compassion (Gilbert & Procter, 2006). CMT assumes that these attributes can be developed by practising skills such as mindful attention and self‐compassion (Gilbert, 2009), regardless of early experiences. Interventions may be made more effective by helping clients develop the ability to switch their attention from the distressing voice to present moment awareness, in conjunction with responding to themselves and/or their voices with compassion. From our mediation findings, it appears that developing these skills simultaneously would potentiate the overall outcome. These are core tenets of compassion‐focused therapy (CFT; Gilbert, 2009) and person‐based cognitive therapy (Chadwick et al., 2005, 2016); therefore, these approaches may be particularly useful for people distressed by voices.
The implications of the present study may also support the emerging ‘compassion for voices’ approach. Kennedy and Ellerby (2016) discuss integration of CFT with the voice dialogue approach utilized by the hearing voices movement (Corstens, Escher, & Romme, 2008). Given self‐compassion (in particular an absence of aversion) significantly predicted lower distress/severity of voices, accepting and engaging with voices in a compassionate manner may be a useful direction for future research and therapeutic practice to explore.
Conclusion
The findings of the present study demonstrate strong associations between self‐compassion, mindfulness of voices, secure attachment and lower levels of distress and voices severity, as well as mediating relationships, highlighting synergy between mindfulness and self‐compassion. Results suggest that developing self‐compassion and mindful relating to voices may be a useful therapeutic method for people distressed by their voices.
References
- Abba, N. , Chadwick, P. , & Stevenson, C. (2008). Responding mindfully to distressing psychosis: A grounded theory analysis. Psychotherapy Research, 18(1), 77–87. https://doi.org/10.1080/10503300701367992 [DOI] [PubMed] [Google Scholar]
- Bartholomew, K. , & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four‐category model. Journal of Personality and Social Psychology, 61, 226–244. https://doi.org/10.1037/0022-3514.61.2.226 [DOI] [PubMed] [Google Scholar]
- Beavan, V. , & Read, J. (2010). Hearing voices and listening to what they say: The importance of voice content in understanding and working with distressing voices. The Journal of Nervous and Mental Disease, 198, 201–205. https://doi.org/10.1097/nmd.0b013e3181d14612 [DOI] [PubMed] [Google Scholar]
- Beavan, V. , Read, J. , & Cartwright, C. (2011). The prevalence of voice‐hearers in the general population: A literature review. Journal of Mental Health, 20, 281–292. https://doi.org/10.3109/09638237.2011.562262 [DOI] [PubMed] [Google Scholar]
- Berry, K. , Wearden, A. , Barrowclough, C. , Oakland, L. , & Bradley, J. (2011). An investigation of adult attachment and the nature of relationships with voices. British Journal of Clinical Psychology, 51, 280–291. https://doi.org/10.1111/j.2044-8260.2011.02027.x [DOI] [PubMed] [Google Scholar]
- Birchwood, M. , & Chadwick, P. (1997). The omnipotence of voices: Testing the validity of a cognitive model. Psychological Medicine, 27, 1345–1353. https://doi.org/10.1017/s0033291797005552 [DOI] [PubMed] [Google Scholar]
- Birchwood, M. , Gilbert, P. , Gilbert, J. , Trower, P. , Meaden, A. , Hay, J. , … Miles, J. N. (2004). Interpersonal and role‐related schema influence the relationship with the dominant ‘voice’ in schizophrenia: A comparison of three models. Psychological Medicine, 34, 1571–1580. https://doi.org/10.1017/s0033291704002636 [DOI] [PubMed] [Google Scholar]
- Bowlby, J. (1973). Attachment and loss: Separation (Vol. 2). New York, NY: Basic Books. [Google Scholar]
- British Psychological Society (2010). Code of human research ethics. INF180/04.2011. Leicester, UK: Author. [Google Scholar]
- British Psychological Society (2013). Ethics guidelines for internet‐mediated research. INF206/1.2013. Leicester, UK: Author. [Google Scholar]
- Brown, K. W. , & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well‐being. Journal of Personality and Social Psychology, 84, 822 https://doi.org/10.1037/0022-3514.84.4.822 [DOI] [PubMed] [Google Scholar]
- Chadwick, P. , Barnbrook, E. , & Newman‐Taylor, K. (2007). Responding mindfully to distressing voices: Links with meaning, affect and relationship with voice. Journal of the Norwegian Psychological Association, 44, 581–587. https://doi.org/10.1080/10503300701367992 [Google Scholar]
- Chadwick, P. , Birchwood, M. J. , & Trower, P. (1996). Cognitive therapy for delusions, voices and paranoia. Chichester, UK: Wiley. [Google Scholar]
- Chadwick, P. , Hughes, S. , Russell, D. , Russell, I. , & Dagnan, D. (2009). Mindfulness groups for distressing voices and paranoia: A replication and randomized feasibility trial. Behavioural and Cognitive Psychotherapy, 37, 403–412. https://doi.org/10.1017/s1352465809990166 [DOI] [PubMed] [Google Scholar]
- Chadwick, P. , Newman‐Taylor, K. , & Abba, N. (2005). Mindfulness groups for people with psychosis. Behavioural and Cognitive Psychotherapy, 33, 351–359. https://doi.org/10.1017/s1352465805002158 [Google Scholar]
- Chadwick, P. , Strauss, C. , Jones, A. , Kingdon, D. , Ellett, L. , Dannahy, L. , & Hayward, M. (2016). Group mindfulness‐based intervention for distressing voices: A pragmatic randomised controlled trial. Schizophrenia Research, 175, 168–173. https://doi.org/10.1016/j.schres.2016.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiesa, A. (2013). The difficulty of defining mindfulness: current thought and critical issues. Mindfulness, 4, 255–268. https://doi.org/10.1007/s12671-012-0123-4 [Google Scholar]
- Cohen, J. (1977). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence; https://doi.org/10.1016/b978-0-12-179060-8.50016-5 [Google Scholar]
- Corstens, D. , Escher, S. , & Romme, M. (2008). Accepting and working with voices: The Maastricht approach In Moskowitz A., Schafer I. & Dorahy M. J. (Eds.), Psychosis, trauma and dissociation: Emerging perspectives on severe psychopathology (pp. 319–331). Oxford, UK: Wiley‐Blackwell. [Google Scholar]
- Depue, R. A. , & Morrone‐Strupinsky, J. V. (2005). A neurobehavioral model of affiliative bonding. Behavioral and Brain Sciences, 28, 313–395. https://doi.org/10.1017/s0140525x05000063 [DOI] [PubMed] [Google Scholar]
- Eicher, A. C. , Davis, L. W. , & Lysaker, P. H. (2013). Self compassion: A novel link with symptoms in schizophrenia? Journal of Nervous and Mental Disorders, 201, 389–393. https://doi.org/10.1097/nmd.0b013e31828e10fa [DOI] [PubMed] [Google Scholar]
- Faul, F. , Erdfelder, E. , Buchner, A. , & Lang, A. G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41, 1149–1160. https://doi.org/10.3758/brm.41.4.1149 [DOI] [PubMed] [Google Scholar]
- Feldman, G. , Greeson, J. , & Seville, J. (2010). Differential effects of mindful breathing, progressive muscle relaxation and loving kindness meditation on decentering and negative reactions to repetitive thoughts. Behaviour Research and Therapy, 48, 1002–1011. https://doi.org/10.1016/j.brat.2010.06.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London, UK: SAGE; https://doi.org/10.1111/j.1365-2648.2007.04270_1.x [Google Scholar]
- Freeman, D. , & Garety, P. A. (2003). Connecting neurosis and psychosis: The direct influence of emotion on delusions and hallucinations. Behaviour Research and Therapy, 41, 923–947. https://doi.org/10.1016/s0005-7967(02)00104-3 [DOI] [PubMed] [Google Scholar]
- Gilbert, P. (2009). Introducing compassion‐focused therapy. Advances in Psychiatric Treatment, 15, 199–208. https://doi.org/0.1192/apt.bp.107.005264 [Google Scholar]
- Gilbert, P. , McEwan, K. , Matos, M. , & Rivis, A. (2011). Fears of compassion: Development of three self‐report measures. Psychology and Psychotherapy: Theory, Research and Practice, 84, 239–255. https://doi.org/10.1348/147608310X526511 [DOI] [PubMed] [Google Scholar]
- Gilbert, P. , & Procter, S. (2006). Compassionate mind training for people with high shame and self‐criticism: Overview and pilot study of a group therapy approach. Clinical Psychology and Psychotherapy, 13, 353–379. https://doi.org/10.1002/cpp.507 [Google Scholar]
- Gillath, O. , Shaver, P. , & Mikulincer, M. (2005). An attachment‐theoretical approach to compassion and altruism In Gilbert P. (Ed.), Compassion: Conceptualisations, research and use in psychotherapy (pp. 121–147). London, UK: Routledge. [Google Scholar]
- Glomb, T. M. , Duffy, M. K. , Bono, J. E. , & Yang, T. (2011). Mindfulness at work In Joshi A., Liao H. & Martocchio J. J. (Ed.), Research in personnel and human resources management (Research in personnel and human resources management, volume 30) (pp. 115–157). Bingley: Emerald Group Publishing Limited. [Google Scholar]
- Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. New York, NY: Guilford Press. [Google Scholar]
- Hargus, E. , Crane, C. , Barnhofer, T. , & Williams, J. M. G. (2010). Effects of mindfulness on meta‐awareness and specificity of describing prodromal symptoms in suicidal depression. Emotion, 10, 34 https://doi.org/10.1037/a0016825 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollis‐Walker, L. , & Colosimo, K. (2011). Mindfulness, self‐compassion, and happiness in non‐meditators: A theoretical and empirical examination. Personality and Individual Differences, 50, 222–227. https://doi.org/10.1016/j.paid.2010.09.033 [Google Scholar]
- IBM (2015). IBM SPSS statistics for windows, version 23.0. Armonk, NY: Author. [Google Scholar]
- Kabat‐Zinn, J. (2003). Mindfulness‐based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10, 144–156. https://doi.org/10.1093/clipsy/bpg016 [Google Scholar]
- Kennedy, A. , & Ellerby, M. (2016). A compassion‐focused approach to working with someone diagnosed with schizophrenia. Journal of Clinical Psychology, 72, 123–131. https://doi.org/10.1002/jclp.22251 [DOI] [PubMed] [Google Scholar]
- Khoury, B. , Lecomte, T. , Fortin, G. , Masse, M. , Therien, P. , Bouchard, V. , … Hofmann, S. G. (2013a). Mindfulness‐based therapy: A comprehensive meta‐analysis. Clinical Psychology Review, 33, 763–771. https://doi.org/10.1016/j.cpr.2013.05.005 [DOI] [PubMed] [Google Scholar]
- Khoury, B. , Lecomte, T. , Gaudiano, B. A. , & Paquin, K. (2013b). Mindfulness interventions for psychosis: A meta‐analysis. Schizophrenia Research, 150, 176–184. https://doi.org/10.1016/j.schres.2013.07.055 [DOI] [PubMed] [Google Scholar]
- Kiken, L. G. , Garland, E. L. , Bluth, K. , Palsson, O. S. , & Gaylord, S. A. (2015). From a state to a trait: Trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Personality and Individual Differences, 81, 41–46. https://doi.org/10.1016/j.paid.2014.12.044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, S. H. , Jung, H. Y. , Hwang, S. S. , Chang, J. S. , Kim, Y. , Ahn, Y. M. , & Kim, Y. S. (2010). The usefulness of a self‐report questionnaire measuring auditory verbal hallucinations. Progress in Neuro‐Psychopharmacology & Biological Psychiatry, 34, 968–973. https://doi.org/10.1016/j.pnpbp.2010.05.005 [DOI] [PubMed] [Google Scholar]
- Kuyken, W. , Watkins, E. , Holden, E. , White, K. , Taylor, R. S. , Byford, S. , … Dalgleish, T. (2010). How does mindfulness‐based cognitive therapy work? Behaviour Research and Therapy, 48, 1105–1112. https://doi.org/10.1016/j.brat.2010.08.003 [DOI] [PubMed] [Google Scholar]
- Mayhew, S. L. , & Gilbert, P. (2008). Compassionate mind training with people who hear malevolent voices: A case series report. Clinical Psychology & Psychotherapy, 15, 113–138. https://doi.org/10.1016/s0920-9964(06)70180-3 [DOI] [PubMed] [Google Scholar]
- McCarthy‐Jones, S. (2012). Hearing voices: The history, causes and meanings of auditory verbal hallucinations. Cambridge, UK: Cambridge University Press; https://doi.org/10.1017/cbo9781139017534.001 [Google Scholar]
- Neff, K. D. (2003). The development of a scale to measure self‐compassion. Self and Identity, 2, 223–250. https://doi.org/10.1080/15298860309027 [Google Scholar]
- Newman‐Taylor, K. , Harper, S. , & Chadwick, P. (2009). Impact of cognition and affect in voice hearing: Evidence from two case studies. Behavioural and Cognitive Psychotherapy, 37, 397–402. https://doi.org/10.1017/s135246580999018x [DOI] [PubMed] [Google Scholar]
- Ponizovsky, A. M. , Vitenberg, E. , Baumgarten‐Katz, I. , & Grinshpoon, A. (2013). Attachment styles and affect regulation among outpatients with schizophrenia: Relationships to symptomatology and emotional distress. Psychology and Psychotherapy: Theory, Research and Practice, 86, 164–182. https://doi.org/10.1111/j.2044-8341.2011.02054.x [DOI] [PubMed] [Google Scholar]
- Qualtrics . (2016). Qualtrics survey software [computer software]. Provo, UT: Qualtrics. [Google Scholar]
- Radford, S. , Eames, C. , Brennan, K. , Lambert, G. , Crane, C. , Williams, J. M. G. , … Barnhofer, T. (2014). Trait mindfulness as a limiting factor for residual depressive symptoms: An explorative study using quantile regression. PLoS One, 9, e100022 https://doi.org/10.1371/journal.pone.0100022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romme, M. A. J. , & Escher, A. (1989). Hearing voices. Schizophrenia Bulletin, 15, 209–216. https://doi.org/10.1093/schbul/15.2.209 [DOI] [PubMed] [Google Scholar]
- Romme, M. A. J. , Honig, A. , Noorthorn, E. O. , & Escher, A. D. (1992). Coping with hearing voices: An emancipatory approach. British Journal of Psychiatry, 161, 99–103. https://doi.org/10.1192/bjp.161.1.99 [DOI] [PubMed] [Google Scholar]
- Segal, Z. V. , Williams, J. M. G. , & Teasdale, J. D. (2002). Mindfulness based cognitive therapy for depression – a new approach to preventing relapse. New York, NY: Guilford Press. [Google Scholar]
- Scharfe, E. , & Bartholomew, K. (1994). Reliability and stability of adult attachment patterns. Personal Relationships, 1, 23–43. https://doi.org/10.1111/j.1475-6811.1994.tb00053.x [Google Scholar]
- Shapiro, S. L. , Astin, J. A. , Bishop, S. R. , & Cordova, M. (2005). Mindfulness‐based stress reduction for health care professionals: Results from a randomized controlled trial. International Journal of Stress Management, 12, 164–176. https://doi.org/10.1037/1072-5245.12.2.164 [Google Scholar]
- Shaver, P. R. , Lavy, S. , Saron, C. D. , & Mikulincer, M. (2007). Social foundations of the capacity for mindfulness: An attachment perspective. Psychological Inquiry: An International Journal for the Advancement of Psychological Theory, 18, 264–271. https://doi.org/10.1080/10478400701598389 [Google Scholar]
- Singh, G. , Sharan, P. , & Kulhara, P. (2003). Role of coping strategies and attitudes in mediating distress due to hallucinations in schizophrenia. Psychiatry and Clinical Neurosciences, 57, 517–522. https://doi.org/10.1046/j.1440-1819.2003.01157.x [DOI] [PubMed] [Google Scholar]
- Sorrell, E. , Hayward, M. , & Meddings, S. (2010). Interpersonal process and hearing voices: A study of the association between relating to voices and distress in clinical and non‐clinical hearers. Behavioural and Cognitive Psychotherapy, 38, 127 https://doi.org/10.1017/s1352465809990506 [DOI] [PubMed] [Google Scholar]
- Strauss, C. (2014). What have we learnt about mindfulness‐based interventions and acceptance and commitment therapy for distressing voices? In Hayward M., Strauss C. & McCarthy‐Jones S. (Eds.), Psychological approaches to understanding and treating auditory hallucinations: From theory to therapy (pp. 151–169). London, UK: Routledge. [Google Scholar]
- Strauss, C. , Thomas, N. , & Hayward, M. (2015). Can we respond mindfully to distressing voices? A systematic review of evidence for engagement, acceptability, effectiveness and mechanisms of change for mindfulness‐based interventions for people distressed by hearing voices. Frontiers in Psychology, 6, 1144 https://doi.org/10.3389/fpsyg.2015.01154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas, N. (2014). What have we learnt about how to capture and measure the outcomes of psychological therapies for voices? In Hayward M., Strauss C. & McCarthy‐Jones S. (Eds.), Psychological approaches to understanding and treating auditory hallucinations: From theory to therapy (pp. 100–128). London, UK: Routledge. [Google Scholar]
- Úbeda‐Gómez, J. , León‐Palacios, M. G. , Escudero‐Pérez, S. , Barros‐Albarrán, M. D. , López‐Jiménez, A. M. , & Perona‐Garcelán, S. (2015). Relationship between self‐focused attention, mindfulness and distress in individuals with auditory verbal hallucinations. Cognitive Neuropsychiatry, 20, 482–488. https://doi.org/10.1080/13546805.2015.1089225 [DOI] [PubMed] [Google Scholar]
- Van Lieshout, R. J. , & Goldberg, J. O. (2007). Quantifying self‐reports of auditory verbal hallucinations in persons with psychosis. Canadian Journal of Behavioural Science, 39(1), 73–77. https://doi.org/10.1037/cjbs2007006 [Google Scholar]
- Vaughan, S. , & Fowler, D. (2004). The distress experienced by voice hearers is associated with the perceived relationship between the voice hearer and the voice. British Journal of Clinical Psychology, 43, 143–153. https://doi.org/10.1348/014466504323088024 [DOI] [PubMed] [Google Scholar]
- Wei, M. , Liao, K. Y. , Ku, T. , & Shaffer, P. A. (2011). Attachment, self‐compassion, empathy, and subjective well‐being among college students and community adults. Journal of Personality, 79(1), 191–219. https://doi.org/10.1111/j.1467-6494.2010.00677.x [DOI] [PubMed] [Google Scholar]
- World Health Organization (1992). The ICD‐10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. Geneva, Switzerland: Author. [Google Scholar]