

Abstract
Background:
The medical prescription is a valid and legal document. Prescriptions can also be used as a measure of the quality of medical education, observance of the laws and regulations, and sociocultural beliefs.
Aims:
To assess the quality of prescription written by dental and medical students and practitioners.
Settings and Design:
A cross-sectional study was conducted in three dental and two medical colleges in Kerala covering 345 participants (dental - 235 and medical - 110).
Materials and Methods:
Simulation exercise was conducted for drafting a model prescription based on a given clinical condition. The variables were identified based on the model prescription format by the Medical Council of India and were classified into four domains. Points were assigned for each variable.
Statistical Analysis Used:
Analysis was performed using descriptive statistics and Mann–Whitney U-test.
Results and Conclusion:
The total scores were found to be higher among dental fraternity (10.93 ± 2.88) to medical (10.81 ± 2.55). The medical house surgeons and postgraduates fared better in the doctor identification domain. Among the dental professionals, there was a significant difference among the undergraduates (mean score = 1.91) and postgraduates (mean score = 1.60) in the doctor identification domain. However, among the medical professionals, in the patient identification domain, house surgeons had a significantly higher score compared to postgraduates. There were no significant differences in quality of prescription writing among medical and dental professionals.
Keywords: Dentistry, drugs, medicine, prescription
INTRODUCTION
The medical prescription is a valid, legal document. The prescription order is an important transaction between the physician and the patient.[1] Prescription writing is both an art and science, which needs to be mastered by the medical professional.[2] The word “prescription,” derives from “pre” (before) and “script” (writing, written), which denotes that it is an order that must be written down before or for the preparation and administration of a drug. A prescription is defined as a health-care program implemented by a physician in the form of instructions that govern the plan of care for an individual patient.[3] Prescriptions can be used as a measure of the quality of medical education and observance of the laws and regulations.[4] The essence of a good prescription writing is to ensure that the prescriber should know exactly which drug formulation and dosage to dispense, and the patient has explicit written instructions for self-administration of the prescribed drug.[5] Prescribing is also used to describe certain activities which include delivery of medicines and devices. It is used to describe written information provided for patients or any advice.[6]
Errors in prescription can occur due to variety of reasons; however, most common errors are human errors which occur in prescription writing.[7,8] Some of the common errors observed during prescription writing can be attributed to wrong format, lack of clarity in comprehending the prescription, or aberration in spelling. This results in pharmacist misreading/misinterpreting the prescription, dispensing the wrong drug/dose, or providing insufficient/ambiguous information to the patient.[5,6,7,9,10,11]
According to the World Health Organization's (WHO) recommendations, prescriptions should identify the professional, the patient, the mode of administration, as well as the medicine's pharmaceutical form, dosage, frequency of use, duration of treatment along with patient guidance and information.[12] In the context of the present study, “quality of prescriptions” meant the amount of errors committed in reference to a standard prescription format.
The prevalence of errors in prescriptions among dental and medical practitioners in teaching institutions and clinical practice was found to be high, and most prescriptions did not follow the WHO prescription guidelines (India, UK, and Brazil).[13,14,15,16,17,18] Data on irrational drug use show an increasing trend worldwide often leading to adverse health consequences.[19] The WHO in 2010 reported that more than 50% of drugs were not correctly prescribed, dispensed, or sold. This was much worse in developing countries where the majority of patients are not treated as per the clinical guidelines.[19,20] Some of the factors underlying the irrational use of drugs were drug misinformation, misleading beliefs, patient demands/expectations, and prescribers – lack of education and training, inappropriate role models, lack of objective drug information, etc.[20,21]
A review of studies conducted in this regard reflected some commonly encountered prescribing errors. Abbreviations, illegible letters, lack of information on mode of administration, total quantity of drug prescribed, dosage/posology, duration and/or guidance about drug allergies and proposed treatment were a few of those.[1,4,22,23] Failure to identify prescriber and patients were common errors noted among students.[24] The use of brand names instead of generic names is a common practice worldwide and has garnered much attention.[1]
These errors can lead to serious repercussions resulting in undesirable consequences such as worsening of treatment, increased cost of treatment, and other serious adverse events.[18] Most of these errors could be attributed to the lack of training in practical prescribing and failure to link theory and practice.[18]
The frequency of errors committed during prescribing drugs can be reduced to a great extent by adequate and proper training beginning right from the formative years of a medical/dental student.[15,25] Systematic reviews support the use WHO guide to good prescribing as the gold standard for training medical students and doctors for proper prescription writing.[26,27]. In addition, use of electronic prescriptions can reduce the chances of inadvertent and careless error.[2,18]
There has been a paucity of studies comparing the quality of prescription writing among medical and dental students though it has been studied in isolation. Knowledge of good prescribing practices is of prime importance to any medical professional irrespective of their qualification. The objectives were to assess the quality of prescription written by dental and medical students and practitioners.
MATERIALS AND METHODS
Study design
This was a cross-sectional study.
Study setting
Three dental and two medical colleges in Kerala, India.
Study participants
Students and practitioners of dental and medical colleges were included in the study. The study participants included third and final year undergraduate students, house surgeons, postgraduate students, and faculty/practitioners. The undergraduate medical students were excluded as they did not write prescriptions independently. The study participants were selected from three dental and two medical colleges in Kerala.
Sample size
Since it was exploratory study, a convenience sampling method was employed. Twenty-five students from all categories were selected from each dental and medical college making a total of 345. A subsample of 10 practitioners was selected from these colleges [Figure 1].
Figure 1.

Flowchart for data collection
Variables
The variables were identified based on the prescription format by the Medical Council of India (MCI). These variables were classified into four domains, namely, patient identification, doctors identification, drug information, and legibility of prescription. Legibility of prescriptions was assessed by the investigator based on an ease of reading index. One point was assigned to each variable in the model prescription format. Thus,
The patient identification: Maximum score = 4 (1 each for patient name, age, gender, and date of prescription)
Doctor's identification: Maximum score = 5 (1 each for doctor's name, qualification, registration number, full address, and doctors signature)
Drug information: Maximum score = 7 (1 each for treatment, form, name of medicine, strength, dosage instructions, duration, and total quantity)
-
Legibility of prescription was assessed by a single investigator using an index which was graded on a 4-point scale.
- Score 1: More than one aspect not clear
- Score 2: One aspect not clear (patient name/drug name)
- Score 3: Clear but requires effort to read
- Score 4: Prescription details are clear and legible.
Informed consent
A voluntary informed consent was obtained from the study participants.
Data sources/collection
A simulation exercise was conducted which involved a template which gave the details of the prescribing doctor and the condition (medical/dental) for which drug prescription was sought. The participants were assumed to take up the role of the dental/medical practitioner given in the template and were instructed to draft a prescription for the same using the all the required elements for a model prescription.
Quantitative variables
The prescriptions were analyzed as per the scoring format. The mean scores for different domains and the total score for the prescription were calculated.
Ethical approval
The study was approved by the Institutional Review Committee of Amrita Institute of Medical Sciences (Ref/030/TPRC/2016).
Statistical analysis
The obtained scores for each variable were entered, and other data were coded. Descriptive analysis was done for assessing the mean scores of each domain and the total score. Comparison of scores of medical and dental colleges and among each category in medical and dental colleges were done using Mann–Whitney U-test and Kruskal–Wallis ANOVA.SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0 (Chicago: SPSS Inc) was used for statistical analysis.
RESULTS
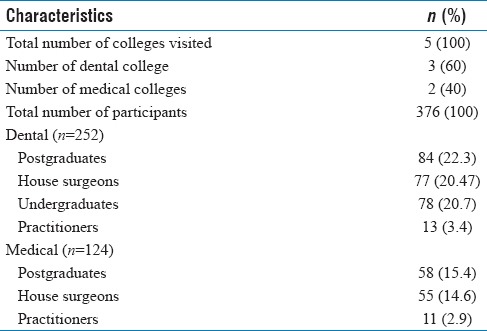
Out of the five colleges surveyed, there were two medical and three dental colleges. The total numbers of participants were 376. The demographic details are given in Table 1.
Table 1.
Demographic details of study participants
Among the dental undergraduates, the mean scores for patient identification, doctor identification, drug information, and legibility of prescription were 2.50, 2.24, 5.46, and 0.79, respectively, and the total score was 11. The box-and-whisker plot represents the total scores obtained by various groups in dental and medical colleges [Figures 2 and 3].
Figure 2.
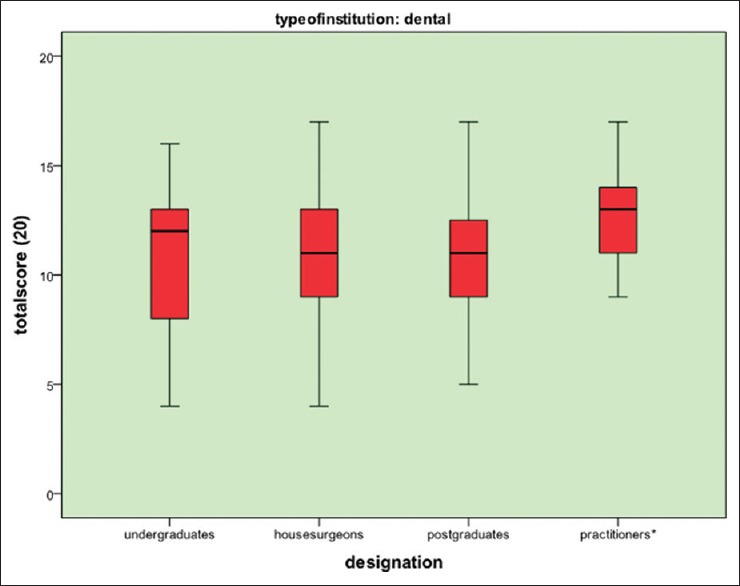
Total score obtained by various groups in dental colleges
Figure 3.
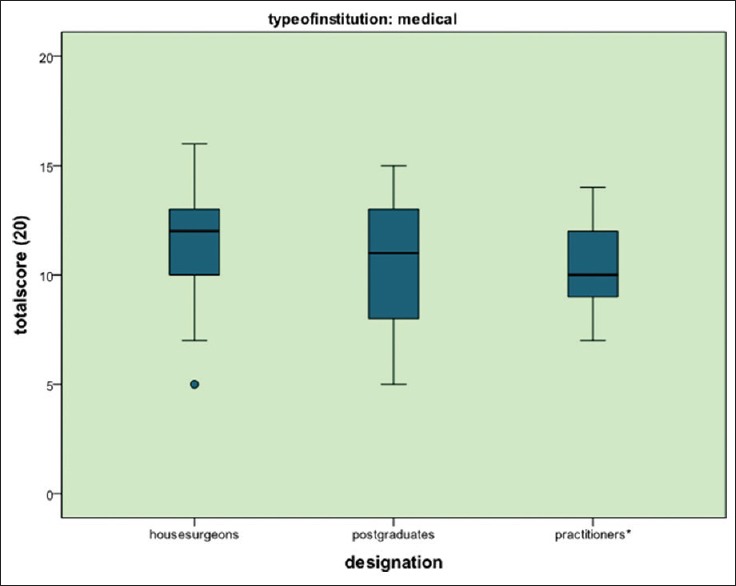
Total scores obtained by various groups in medical colleges
The mean scores obtained by medical and dental groups in the four domains are given in Table 2. The medical house surgeons and postgraduates fared better in the doctor identification domain. However, there was no significant difference in the practitioner's group. The knowledge about drug information domain was significantly higher among dental students and practitioners in comparison with their corresponding medical group. The legibility of prescriptions was better among dental house surgeons, medical postgraduates, and dental practitioners compared to their counterparts. The frequencies and percentage of responses obtained for different variables in medical and dental professionals are given in Table 3. Comparison of various groups of dental and medical professionals with regard to different domains is given in Table 4.
Table 2.
Mean scores obtained by medical and dental groups in four domains
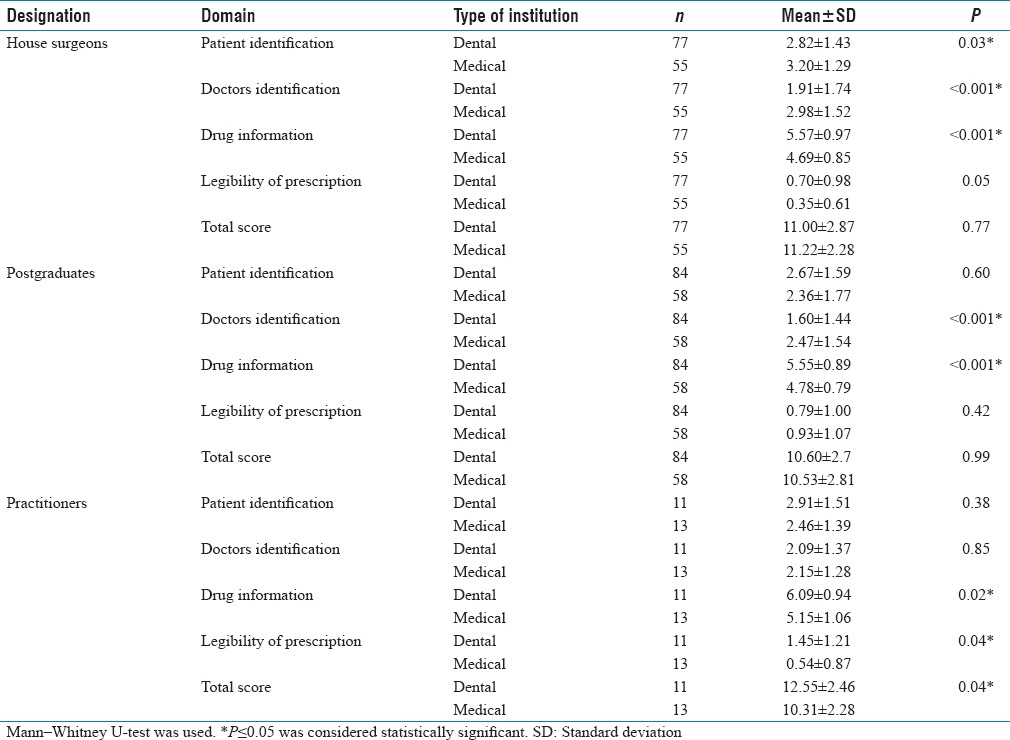
Table 3.
Frequencies and percentage of responses obtained for different variables in medical and dental professionals
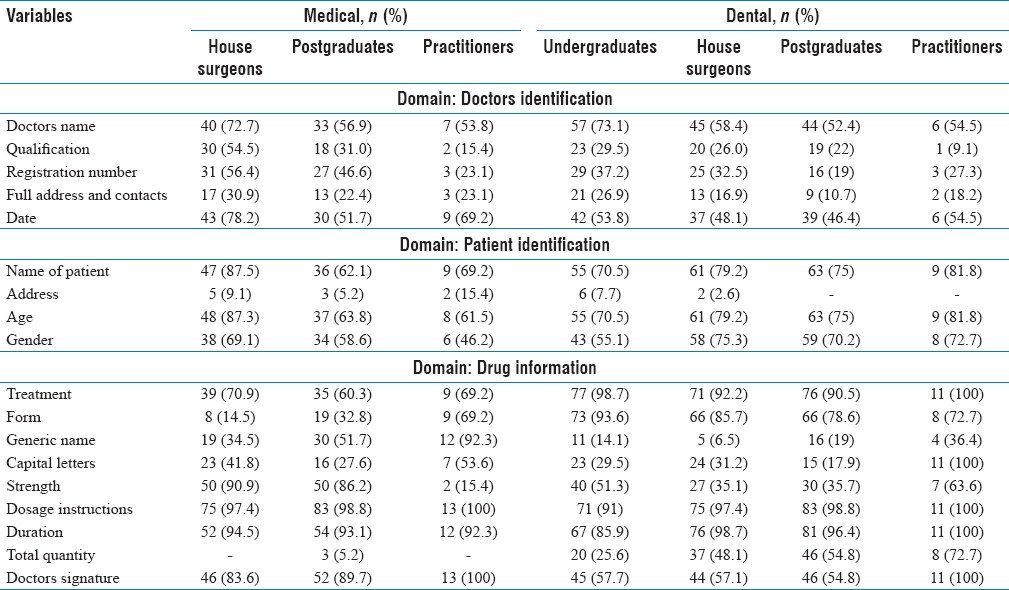
Table 4.
Comparison of various groups of dental and medical professionals with regard to different domains
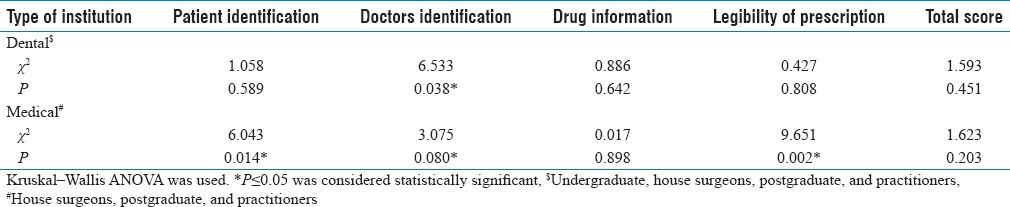
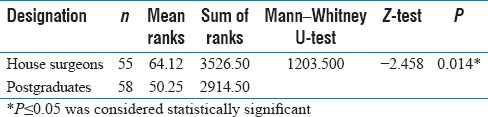
Among the dental professionals, there was a significant difference (P = 0.08) among the undergraduates (mean score = 2.24) and postgraduates (mean score = 1.60) in the doctor identification domain [Table 5]. No significant differences were seen in any of the other groups. However, among the medical professionals, in the patient identification domain, house surgeons had a significantly higher score (P = 0.01) compared to postgraduates [Table 6].
Table 5.
Mann–Whitney U-test showing significant difference among undergraduate and postgraduate dental students in doctor identification domain
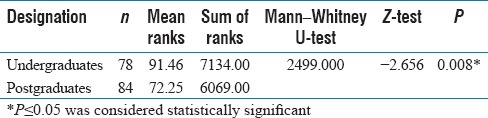
Table 6.
Mann–Whitney U-test showing significant difference among house surgeons and postgraduate dental students in patient identification domain
DISCUSSION
This study was undertaken to assess the quality of prescription written by dental and medical students and practitioners. Good medical practices require that a clinician should have up-to-date knowledge and skills in medical pharmacology and prescription norms.[6] This is also one of the indicators of a good health-care service of a region/country.[28]
Prescription errors are common among doctors. Several studies conducted in different parts of the world among dental and medical professionals bear testimony to this statement. The present study, probably the first of its kind, compared the errors committed by dental and medical doctors during their academic and professional life.
The strength of the study lies in its methodology where a simulation exercise was performed for writing the prescription where specific instructions were given to study participants to include all elements of an ideal prescription for the given medical/dental condition.
During the simulation exercise, it was observed that around 50% of both medical and dental professionals failed to write the prescribing doctor's name and about 90% of them did not mention the medical qualification. A similar study conducted in India showed that a quarter of the respondents failed to write the doctors name and half of the respondents did not mention their qualification pointing to large deficiencies in the information regarding the prescriber.[28] However, the findings were in contrast to an institution based study in Bengaluru, India, where almost all respondents (99.4%) identified their contact details correctly though the qualification was not mentioned in 13% of them.[17]
This study analyzed the prescription practices of various categories of medical professionals, viz., postgraduates, house surgeons, and practitioners. The majority of the dental and medical postgraduates (81% and 53.4%, respectively) did not mention the registration number despite being provided the same in the simulation exercise. This could probably be due to the practice that prescriptions are normally written on letter heads which contained information on registration number and complete address of doctor.[2] Nevertheless, knowledge about essential elements of a prescription is an essential requisite and its absence points to lack of knowledge and training.
Mention of patients name and date of prescription is of vital importance of prevent misuse and reuse of prescriptions.[2] In the present study, around 50% of the prescriptions written by dental professionals did not have the name of patient. In contrast, studies done in Maharashtra and Lahore reported that a majority of prescriptions (>87%) had a mention of patient name.[2,29] The present study had more than 65% of prescriptions without a date which was less compared to the study done in Maharashtra.[29]
More than 90% of respondents in this study failed to write the patients identification. The patient's identity and address are necessary to ensure that the correct medication goes to the patient[30] and also for identification and recordkeeping. Mention of patient's age and gender was also found to be lacking in our study since the patient identification part were printed in the prescription.
The “Rx” is a symbol meaning “prescription.”[31] “R” in Rx stands for the Latin word recipe, means “take.”[32] It is an important element of the prescription, and more than 90% of respondents wrote the symbol Rx in their prescriptions. The findings were similar to other studies conducted in Lahore and Warangal.[29,33]
The drug information domain consisted of variables such as name, strength, dosage form, dosage instructions, duration, and total quantity, and there has been a call to write medicines in their generic name rather than its trade names to deter doctors from promoting a particular brand and recently MCI has made order for Indian doctors. With numerous pharmaceutical companies manufacturing the same drug, prescribing a drug with generic name avoids possible confusion and gives the patient an option of choosing a cheaper brand. In spite of this recommendation, more than 80% of the dental professionals including students and practitioners wrote trade names of drugs in their prescriptions. The practice of generic prescribing was low in other studies conducted across India.[2,28,34]
Illegibility is a common place in medical prescriptions. Illegibility of handwritten prescription can lead to errors in drug dispensing and administration.[35] Legibility of prescriptions have found to be varied across studies.[36,37,38] However, in our study, 75% of the prescriptions were clear and legible as per the index used for assessing legibility. The chance of bias or subjective differences was avoided as the legibility was assessed by a single investigator. One of the methods to overcome this problem is the mandate to write the generic name of drug in upper case, which is also endorsed by the MCI.
The study results showed that knowledge about prescription writing was inadequate among both dental and medical professionals. However, though statistically insignificant, dental professionals performed better in terms of overall quality of prescription and the comparisons was difficult due to dearth of similar studies in literature.
Prescriptions errors can sometimes lead to ineffective treatment resulting in undesirable consequences such as worsening of treatment, long and repeated duration of medicine, etc., Hence, the knowledge of prescribing drugs is of utmost need for good dental practice and is essential to expand this knowledge related to pharmacological therapy.[39] The common human errors and errors in prescribing during high-risk procedures depend on the individuals as well as the institutions they are trained.[40]
CONCLUSION
The prescription errors were common in both medical and dental profession, and hence, students should be made aware of the importance of proper prescription writing for protecting the safety of patients and the doctor. Intensive training in prescription writing skills is required with continuous monitoring.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
I would like to thank my parents Dr. N O Varghese and Dr. Sara Varghese for their support in this research.
REFERENCES
- 1.Kumari S. A study on pattern of prescription writing practices at Rajendra Institute of Medical Sciences, Ranchi. Indian J Prev Soc Med. 2014;45:100–4. [Google Scholar]
- 2.Patil KR, Mali RS, Dhangar BK, Bafna PS, Gagarani MB, Bari SB. Assessment of prescribing trends and quality of handwritten prescriptions from rural India. J Pharma Sci Technol. 2015;5:54–60. [Google Scholar]
- 3.Panchbhai AS. Rationality of prescription writing. Indian J Pharm Educ Res. 2013;47:7–16. [Google Scholar]
- 4.Araghi S, Sharifi R, Ahmadi G, Esfehani M, Rezaei F. The study of prescribing errors among general dentists. Glob J Health Sci. 2015;8:32–43. doi: 10.5539/gjhs.v8n4p32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Donnelley RR. General principles of pharmacology. Principles of Prescription Writing and Other Pharmacotherapeutic Considerations. Vol. 9. China: 2008. pp. 25–31. [Google Scholar]
- 6.General Medical Council, Good Medical Practice. London: GMC; 2013. Good practice in prescribing and managing medicines and devices. [Google Scholar]
- 7.Fox A. Safer Prescribing Workbook – Prescription Writing. [Last accessed on 2016 Sep 25]. Available from: https://www.scribd.com/doc/314478039/Section1-Prescriptionwriting .
- 8.Aronson JK. Medication errors: What they are, how they happen, and how to avoid them. QJM. 2009;102:513–21. doi: 10.1093/qjmed/hcp052. [DOI] [PubMed] [Google Scholar]
- 9.Benet LZ, Gilman AG, Rall TW, Nies AS, Taylor P. Goodman and Gilman's Manual of Pharmacology and Therapeutics. 8th ed. Vol. 2. New York: Pergamon Press; 1991. Principles of prescription order writing and patient compliance; pp. 1640–9. [Google Scholar]
- 10.Yagiela JA, Dowd FJ, Johnson B, Mariotti A, Neidle EA. Pharmacology and Therapeutics for Dentistry – E-Book. United States: Elsevier Health Sciences; 2010. p. 957. [Google Scholar]
- 11.Torrey T. Why Do Prescription Drug Errors Occur? 2010. Available from: About.com. Guide.
- 12.de Vries TP, Henning RH, Hogerzeil HV, Fresle DA. Guide to Good Prescribing – A Practical Manual. Geneva: World Health Organization; 1994. Action programme on essential drugs. [Google Scholar]
- 13.Nuroloyuni S, Pirzadeh A, Nuroloyuni A, Asdagh S, Khabiri B. Investigating the prevalence of prescribing errors in general dentists prescriptions. J Physiol Pharmacol Adv. 2015;5:550–5. [Google Scholar]
- 14.Mendonça JM, Lyra DP, Jr, Rabelo JS, Siqueira JS, Balisa-Rocha BJ, Gimenes FR, et al. Analysis and detection of dental prescribing errors at primary health care units in Brazil. Pharm World Sci. 2010;32:30–5. doi: 10.1007/s11096-009-9335-7. [DOI] [PubMed] [Google Scholar]
- 15.Kshirsagar MJ, Langade D, Patil S, Patki PS. Prescribing patterns among medical practitioners in Pune, India. Bull World Health Organ. 1998;76:271–5. [PMC free article] [PubMed] [Google Scholar]
- 16.Ross S, Loke YK. Do educational interventions improve prescribing by medical students and junior doctors? A systematic review. Br J Clin Pharmacol. 2009;67:662–70. doi: 10.1111/j.1365-2125.2009.03395.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dyasanoor S, Urooge A. Insight into quality of prescription writing – An institutional study. J Clin Diagn Res. 2016;10:ZC61–4. doi: 10.7860/JCDR/2016/18011.7472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nazar H, Nazar M, Rothwell C, Portlock J, Chaytor A, Husband A. Teaching safe prescribing to medical students: Perspectives in the UK. Adv Med Educ Pract. 2015;6:279–95. doi: 10.2147/AMEP.S56179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Khor M. Irrational drug Use Causing Rise of Anti-Microbial Resistance. TWN Info Service on Health Issues. 2009 [Google Scholar]
- 20.Shtrestha S. Irrational prescription: A hurdle to quality health. Lancet. 2013 [Google Scholar]
- 21.Kadam A. Rational drug Use a Concern for Healthcare Professionals. Pharma Infonet. 2009;7 [Google Scholar]
- 22.Moura CS, Naves JO, Coelho EB, Lia EN. Assessment of quality of prescription by dental students. J Appl Oral Sci. 2014;22:204–8. doi: 10.1590/1678-775720130568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sudheer G, Sreenivasan K, Ravi Prabhu G. A study of prescription writing practices of doctors in medical units in a teaching hospital. J Dr NTR Univ Health Sci. 2013;2:22–14. [Google Scholar]
- 24.Oshikoya KA, Bello JA, Ayorinde EO. Prescribing knowledge and skills of final year medical students in Nigeria. Indian J Pharmacol. 2008;40:251–5. doi: 10.4103/0253-7613.45150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kia SJ, Behravesh M, Sigaroudi AK. Evaluation of drug prescription pattern among general dental practitioners in Rasht, Iran. J Dentomaxillofac Radiol Pathol Surg. 2013;1:18–23. [Google Scholar]
- 26.Kamarudin G, Penm J, Chaar B, Moles R. Educational interventions to improve prescribing competency: A systematic review. BMJ Open. 2013;3:e003291. doi: 10.1136/bmjopen-2013-003291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sandilands EA, Reid K, Shaw L, Bateman DN, Webb DJ, Dhaun N, et al. Impact of a focussed teaching programme on practical prescribing skills among final year medical students. Br J Clin Pharmacol. 2011;71:29–33. doi: 10.1111/j.1365-2125.2010.03808.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Phalke VD, Phalke DB, Syed MM, Mishra A, Sikchi S, Kalakoti P. Prescription writing practices in a rural tertiary care hospital in Western Maharashtra, India. Australas Med J. 2011;4:4–8. doi: 10.4066/AMJ.2011.515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Babar HS, Hussain S, Maqzood Z, Dad HA, Rahman AA, Buksh A. Adherence to prescription format and compliance with WHO core prescribing indicators. [Last accessed on 2016 Oct 03];J Pharm Sci Res. 2014 6:195–9. Available from: https://duckduckgo.com/ [Google Scholar]
- 30.Buxton IL. Goodman & Gilman's the Pharmacological Basis of Therapeutics. 12th ed. China: Goodman & Gilman's the Pharmacological Basis of Therapeutics; 2011. Principles of prescription order writing and patient compliance. [Google Scholar]
- 31.Medical Prescription. Wikipedia, the Free Encyclopedia. 2016. [Last accessed on 2016 Sep 25]. Available from: https://www.en.wikipedia.org/w/index.php?title=Medical_prescription&oldid=740537564 .
- 32.Merriam Webster. Oxford English Dictionary [Internet] [Last cited on 2016 Sep 25]. Available from: http://www.merriam-webster.com/dictionary/recipe .
- 33.Pavani V, Mihir YP, Shravani K, Prabhakar RV. Study of prescribing pattern for evaluation of rational drug therapy in Warangal. Indian J Pharm Pract. 2011;4:77–9. [Google Scholar]
- 34.Jain S, Khan ZY, Upadhyaya P, Abhijeet K. Assessment of prescription pattern in a private teaching hospital in India. Int J Pharma Sci. 2013;3:219–22. [Google Scholar]
- 35.Velo GP, Minuz P. Medication errors: Prescribing faults and prescription errors. Br J Clin Pharmacol. 2009;67:624–8. doi: 10.1111/j.1365-2125.2009.03425.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Winslow EH, Nestor VA, Davidoff SK, Thompson PG, Borum JC. Legibility and completeness of physicians' handwritten medication orders. Heart Lung. 1997;26:158–64. doi: 10.1016/s0147-9563(97)90076-5. [DOI] [PubMed] [Google Scholar]
- 37.Calligaris L, Panzera A, Arnoldo L, Londero C, Quattrin R, Troncon MG, et al. Errors and omissions in hospital prescriptions: A survey of prescription writing in a hospital. BMC Clin Pharmacol. 2009;9:9. doi: 10.1186/1472-6904-9-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Irshaid YM, Al Homrany M, Hamdi AA, Adjepon-Yamoah KK, Mahfouz AA. Compliance with good practice in prescription writing at outpatient clinics in Saudi Arabia. East Mediterr Health J. 2005;11:922–8. [PubMed] [Google Scholar]
- 39.Jain A, Gupta D, Singh D, Garg Y, Saxena A, Chaudhary H, et al. Knowledge regarding prescription of drugs among dental students: A descriptive study. J Basic Clin Pharm. 2015;7:12–6. doi: 10.4103/0976-0105.170584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Reason JT, Carthey J, de Leval MR. Diagnosing “vulnerable system syndrome”: An essential prerequisite to effective risk management. Qual Health Care. 2001;10(Suppl 2):ii21–5. doi: 10.1136/qhc.0100021... [DOI] [PMC free article] [PubMed] [Google Scholar]