

Description
Incomplete non-puerperal uterine inversion is a rare complication that can arise secondary to the presence of submucous fibroid.1 In the majority of cases reported in the literature, the definitive diagnosis is usually made at the time of hysterectomy.2 In reported cases where hysterectomy was not done, Haultain procedure was done to correct the inversion.3 In the following case, the diagnosis was made preoperatively and the fibroid was resected vaginally by LigaSure.
A 31-year-old nulliparous woman presented to the emergency room with history of excessive bleeding for a few months. She also had urine retention for 1 day. On examination, she was pale. Vaginal examination showed a large mass distending the vagina with foul smell and moderate bleeding. Her haemoglobin was 6.2 g/L. Pelvic ultrasound scan was not conclusive in ascertaining the origin of the mass. MRI revealed the presence of a pedunculated, large (6×7×12 cm) submucous fibroid (figure 1). The fibroid pedicle was broad and attached to the fundus. The uterine fundus was inverted in the uterine cavity. The cervix was dilated due to the large fibroid. There was also degeneration and haemorrhagic foci in the fibroid. Figure 2 shows a schematic presentation of the uterus and fibroid on MRI image.
Figure 1.
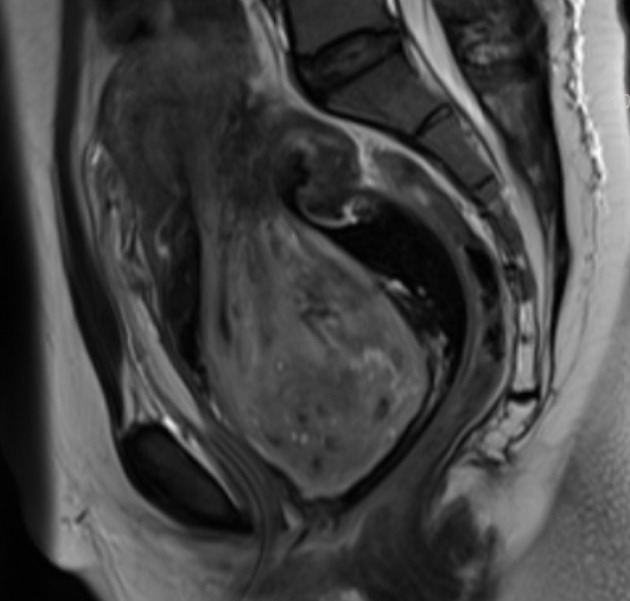
Sagittal MRI view of incomplete uterine inversion. The large submucous fibroid can be seen dilating the cervix and filling the vaginal cavity.
Figure 2.
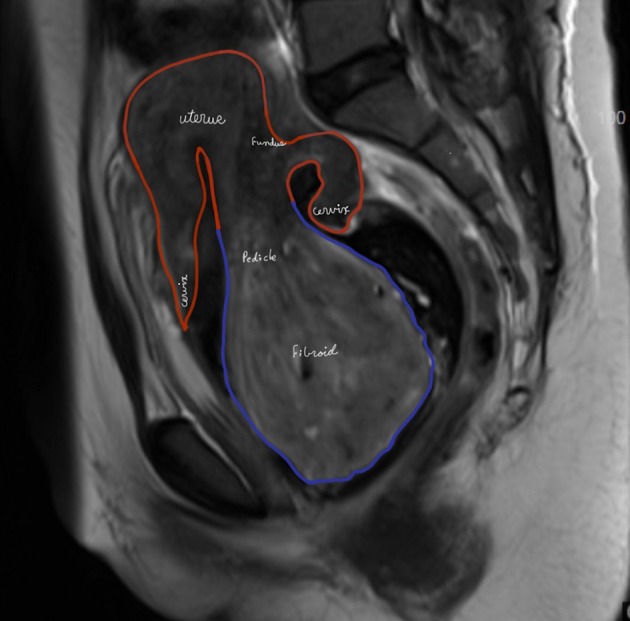
Schematic representation of the MRI image showing the incomplete inversion of the uterus, the fibroid and the dilated cervix.
The patient received blood transfusion prior to the surgery. She was counselled regarding the management. It was agreed that a trial will be made to ligate the pedicle of the fibroid through a vaginal approach using LigaSure. This management was proposed to make sure that the pedicle of the fibroid is sealed to minimise blood loss. It was also agreed that laparotomy will be done if there is difficulty reaching the pedicle. Hysterectomy will be done in the event of uncontrolled bleeding.
Intraoperatively, the fibroid was delivered vaginally almost like delivery of fetal head using myomectomy screw for traction. Once the pedicle was in view, we used LigaSure to seal and cut the fibroid pedicle. Once the huge weight of the fibroid was released from the uterine fundus, we inserted an ovum forceps to feel the uterine cavity. Bimanual examination also showed absence of the dent in the uterine fundus. As this was an incomplete inversion of the uterus due to the weight of the fibroid, we did not actually need to do any procedure to correct. It happened spontaneously after removing the fibroid. The procedure was completed with minimal bleeding. Ultrasound scan showed normal uterine outline. She was discharged home the following day in good condition. She was seen in the clinic after 6 weeks with no active complaints. She had normal menstrual period 4 weeks after the myomectomy.
Learning points.
MRI gives an accurate diagnosis of uterine inversion and the location of the pedicle of the fibroid when ultrasound scan is inconclusive.
Vaginal resection of large submucous fibroids can be considered when hysterectomy is not an option.
Footnotes
Contributors: NHQ wrote, reviewed and approved the final manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Shabbir S, Ghayasuddin M, Younus SM, et al. Chronic non puerperal uterine inversion secondary to sub-mucosal fibroid. J Pak Med Assoc 2014;64:586–8. [PubMed] [Google Scholar]
- 2.Sharma JB, Kumar S, Rahman SM, et al. Non-puerperal incomplete uterine inversion due to large sub-mucous fundal fibroid found at hysterectomy: a report of two cases. Arch Gynecol Obstet 2009;279:565–7. doi:10.1007/s00404-008-0754-9 [DOI] [PubMed] [Google Scholar]
- 3.Teimoori B, Esmailzadeh A. A large uterine leiomyoma leading to non-puerperal uterine inversion: A case report. Int J Reprod Biomed 2017;15:55–6. [PMC free article] [PubMed] [Google Scholar]