

Abstract
In the U.S., there is a growing Latino population, in which parents primarily speak Spanish to their children. Despite the evidence that language preference is associated with level of acculturation and influences parenting practices in these families, no study has compared how Spanish-and English-speaking Latino families acquire and utilize the skills taught during parent-training programs such as Parent-Child Interaction Therapy (PCIT). Twenty-seven mother-infant Latino dyads received a home-based adaptation of the Child-Directed Interaction (CDI) phase of PCIT as part of a larger randomized control trial. Most infants were male (63%), and their average age was 13.7 months (SD = 1.43). Most families (52%) lived below the poverty line. The Dyadic Parent-Child Interaction Coding System-Third Edition (DPICS-III) was employed to evaluate PCIT skills at baseline and post-treatment, as well as at 3- and 6-month follow-up, assessments. We conducted multiple linear regression analyses among Spanish-speaking (55%) and English-speaking (45%) families to examine differences in acquisition and utilization of do and don’t skills at each assessment while controlling for mother’s education. Results yielded no group differences in the acquisition rate of do or don’t skills at any time point. However, Spanish-speaking mothers used significantly more don’t skills than English-speaking mothers at each assessment. Specifically, Spanish-speaking families used significantly more commands at baseline, post-treatment, and the 6-month followup assessments, as well as more questions at post-treatment and at the 6-month follow-up assessments. These findings highlight the importance of addressing cultural values such as respeto to ensure culturally robust parent-training programs for Latino families.
Keywords: Latino, Parent training, PCIT, Mastery criteria, Cultural adaptation
A recent meta-analysis indicated that more than 13% of children worldwide experience psychological problems (Polanczyk et al. 2015). Similarly, in the United States, it is estimated that one in every five children has some type of psychological problem (Costello et al. 2003; Kataoka et al. 2002). Despite the evidence of what has come to be known as the “immigrant paradox” (i.e., foreign nativity protects against psychological problems; Takeuchi et al. 2007), some Spanish-speaking Latino immigrants present similar lifetime prevalence rates of psychological problems compared to non-Latino White populations. These prevalence rates persist after controlling for type of disorder and demographic variables (Alegría et al. 2008). Furthermore, there is evidence that the prevalence rate of these problems increases over time of residence in the country and generational status, where children of immigrant families present similar prevalence rates to the mainstream population (Vega and López 2001).
In order to address the high prevalence of these psychological problems, particularly among high-risk children and their families, research has highlighted the importance of early assessment and intervention to increase access to and reduce burden of existing evidence-based treatments (Bagner et al. 2012). There has been substantial research demonstrating the efficacy of several evidence-based parent-training interventions to treat early behavior problems, including Parent-Child Interaction Therapy (PCIT; Blizzard et al. 2017b; Zisser and Eyberg 2010), Helping the Noncompliant Child (McMahon and Forehand 2003), the Positive Parenting Program (Triple P; Sanders et al. 2003), Incredible Years (Webster-Stratton and Reid 2010), and Parent Management Training-Oregon model (PMTO; Patterson 2005). Unfortunately, outcome studies examining these intervention programs have been conducted with predominately non-Latino White, English-speaking participants (Borrego et al. 2006; Thomas and Zimmer-Gembeck 2007).
Even though more Latino families have been included in efficacy and effectiveness studies over the last 10 years, Latinos are still the most underrepresented ethno-cultural group in parent-training trials when the make-up of the entire population is taken into account (Ortiz and Del Vecchio 2013). This reliance on non-Latino White, English-speaking samples is especially problematic because there are approximately 55 million people of Latino heritage in the United States, which makes them the largest ethnic minority group in the country (U.S. Census Bureau 2015). Forty percent of the Latino population is 18 years or younger (Vega and López 2001), and 38 million individuals (approximately 73%) speak Spanish at home (U.S. Census Bureau 2015). These figures represent a 233% increase since 1980, when there were only 11 million Spanish speakers in the U.S. (López and González-Barrera 2013).
Moreover, there is evidence that Latino parenting practices differ from those of the mainstream population. For instance, widely referenced authoritarian, authoritative, and permissive parenting styles defined by Baumrind do not fully capture the types of interactions among Latino families, such as interactions that can be intrusive and warm simultaneously (Calzada and Eyberg 2002; Calzada et al. 2010, 2012; Livas-Dlott et al. 2010). Furthermore, these parenting practices are influenced by acculturation and adherence to cultural values such as respeto, which refers to the empathy and respect that children are expected to show toward authority figures (e.g., caregivers, teachers), and familismo, which is the strong bonds among the nuclear and extended family members (Barker et al. 2010; Calzada and Eyberg 2002; Calzada et al. 2010, 2012; Livas-Dlott et al. 2010). This acculturative process has been conceptualized as a bidirectional progression of adopting new values, customs, and behaviors from a culture-receiving country, as well as simultaneously retaining those from the culture of origin (Berry 2003). Among Latino families, language preference (Spanish vs. English) seems to be highly associated with level of acculturation and higher adherence to respeto- and familismo-related parenting practices (Calzada et al. 2012). Moreover, the use of language as a proxy for level of acculturation has been demonstrated to predict differences between Latino families (Berdahl and Torres Stone 2009; Ceballo and Hurd 2008; Kim et al. 2015).
Fortunately, there is an increasing number of parent-training interventions adapted for Latino, Spanish-speaking families, such as PMTO (Baumann et al. 2014; Domenech Rodríguez et al. 2011; Martínez and Eddy 2005; Parra Cardona et al. 2012) and PCIT (Borrego et al. 2006; Matos et al. 2006, 2009; McCabe et al. 2005, 2012; McCabe and Yeh 2009). PCIT is a behavioral parent-training intervention, which is designed to enhance the parent-child relationship to improve child behavior problems. This program is divided into two distinct phases: Child-Directed Interaction (CDI) and Parent-Directed Interaction (PDI). During CDI, parents learn how to follow their child’s lead in a 5-min play situation called “special time.” Specifically, they learn to use PRIDE skills (Praising the child, Reflecting the child’s speech, Imitating the child’s play, Describing the child’s behavior, and expressing Enjoyment in the play), of which the “do skills” represent the verbal skills (i.e., praising, reflecting, and describing). The do skills are implemented in play to reinforce appropriate child behaviors and teach concepts and language. At the same time, parents learn to avoid “don’t skills” (i.e., questions, commands, and criticisms), which take the lead away from the child during the 5-min play. Parents also learn to actively ignore inappropriate and attention-seeking behaviors and to end the play if the child displays aggressive or destructive behaviors. In the PDI phase, parents learn to improve their child’s compliance using clear direct commands and consequences (i.e., time out) for not following these commands. The average length of the intervention is from 12 to 16 one-hour weekly sessions (Blizzard et al. 2017b).
Studies have demonstrated PCIT to be effective across racially and culturally diverse populations such as African-American families (Fernández et al. 2011), Asian families (Chen and Fortson 2015; Leung et al. 2009), European families (Abrahamse et al. 2012; Bjørseth and Wichstrøm 2016), and Latino families (Borrego et al. 2006; Matos et al. 2006, 2009; McCabe et al. 2005, 2012; McCabe and Yeh 2009). Specifically, studies examining culturally-adapted PCIT protocols with Latino families have demonstrated efficacy among Spanish- and English-speaking families in single-case designs (Borrego et al. 2006), open clinical trials (Matos et al. 2006, 2009), and randomized control trials (McCabe et al. 2012; McCabe and Yeh 2009). These culturally robust protocols incorporated cultural constructs relevant for Latino populations, such as respeto and familismo, to improve treatment acceptability of the skills taught during the intervention as well as client satisfaction (Barker et al. 2010; Borrego et al. 2007; Calzada et al. 2013).
Despite significant efforts to provide culturally robust psychosocial interventions for diverse populations, there is no consensus about the overall effectiveness of such adaptations. Several meta-analyses suggest a range from small (Benish et al. 2011; Huey and Polo 2008) to medium (Hall et al. 2016; Smith et al. 2011) effects. In the specific case of parent-training interventions, meta-analyses have yielded a similar pattern of small effects on improving parenting behaviors and child outcomes (Ortiz and Del Vecchio 2013; van Mourik et al. 2016) and medium effects when these interventions go through deep structural changes (e.g., through incorporating cultural, social, and environmental factors; van Mourik et al. 2016). In PCIT, results from the only trials directly comparing a culturally-adapted protocol, the GANA program, to standard PCIT showed that both interventions led to similar effects on child externalizing behavior problems and client satisfaction (McCabe et al. 2012; McCabe and Yeh 2009), but GANA outperformed standard PCIT in leading to reductions in parent report of child internalizing behavior problems 6 to 24 months following treatment (McCabe et al. 2012). Differences across these studies highlight the need to conduct more empirical studies to understand when and how to culturally adapt parent-training protocols while overcoming non-data-supported assumptions about how families from diverse backgrounds respond to these interventions, such as the assumption that all interventions need to be culturally adapted to be effective (for an extensive review on this issue see Ortiz and Del Vecchio 2013).
For instance, there is evidence that immigrant families receiving parent-training interventions may need extra practice sessions to acquire the skills taught due to lack of cultural familiarity with these skills (Lau et al. 2011). Relatedly, in a study examining the implementation of a culturally-adapted PCIT protocol for Latino families, researchers found that some of the skills taught during the intervention (i.e., the CDI skills and the time-out procedure in the PDI phase) were negatively perceived by these families. This lack of cultural suitability seemed to impact the course of treatment as reflected by the additional and extended sessions needed by these Spanish-speaking families to learn how to avoid the CDI don’t skills and utilize the timeout procedure (Matos et al. 2006). Similarly, families that received the GANA program needed more sessions to master the parenting skills compared to previous PCIT trials with mainstream populations (McCabe and Yeh 2009). These findings suggest areas in which the standard protocols may need to be modified to improve clinical outcomes among Latino families. To our knowledge no study has specifically compared PCIT verbal skill acquisition (i.e., change over time across assessments in the use of do and don’t skills) and utilization (i.e., frequency of do and don’t skills at each assessment) between Spanish- and English-speaking Latino parents, which is critically important given that PCIT incorporates utilization standards (i.e., mastery criteria) to determine progress in and completion of the intervention. Thus, further examination of potential differences in skill acquisition and utilization between Spanish- and English-speaking Latino families is warranted to determine if cultural adaptations of this protocol are needed.
The objective of this study was to compare the acquisition and utilization of the PCIT verbal skills (i.e., do and don’t skills) between Spanish- and English-speaking Latino families receiving a home-based adaptation of the CDI phase of PCIT for high-risk infants and their families. The benefit of analyzing verbal skills following only the CDI phase is that parents learn how to use the do skills and avoid the don’t skills during this phase of the full-length protocol. Additionally, there is evidence that the most change in parenting practices during PCIT occurs within the first phase of treatment (Hakman et al. 2009; Timmer et al. 2016). Given the evidence that Spanish-speaking Latino families seem to need additional skill practice and extra sessions to learn and maintain the skills taught during PCIT (Matos et al. 2006; McCabe and Yeh 2009), we hypothesized that Spanish-speaking families would acquire the do and don’t skills at a lower rate (i.e., less change in do and don’t skills from baseline to post and follow-up assessments) compared to their English-speaking counterparts. Similarly, we predicted that Spanish-speaking families would use more don’t skills and fewer do skills than English-speaking families at all time points.
Method
Participants
This study was part of a larger randomized controlled trial with repeated outcome measures at baseline and posttest, as well as 3- and 6-month follow-up, assessments. Results of the main outcomes have been published elsewhere (Bagner et al. 2016). Sixty mother-infant dyads were recruited at a large hospital-based pediatric primary care clinic providing family-centered care to underserved families. For this study, only Latino families who received the intervention (n = 27) were included in the final analyses (see rationale below in Data Analysis below). Infants were on average 63% male and 13.7 months old (SD = 1.43). All mothers reported a Latino ethnicity and the following racial breakdown: 82% White, 4% Black, 7% Biracial, and 7% Other. For their infants, all mothers reported a Latino ethnicity and the following racial breakdown: 81% White, 11% Black, 4% Biracial, and 4% Other. Most families (52%) lived below the poverty line. The participants came from an urban center with a heterogeneous Latino population primarily from the Caribbean, South America, and Central America.
For study inclusion, all the infants were required to be rated above the 75th percentile on the Brief Infant-Toddler and Emotional Assessment (Carter and Briggs-Gowan 2006), a screener of infant behavior problems, by their primary caregiver (who was the mother in all cases), and that the primary caregiver speak and understand either English or Spanish. Bilingual mothers were asked to choose their language preference based on their comfort level; 57% of mothers chose to complete the screening and assessments in Spanish. To ensure ability to learn the intervention skills, and as an inclusion criterion, the mother was required to receive an estimated IQ score ≥70 on the two-subtest (vocabulary and matrix reasoning) version of the Wechsler Abbreviated Scale of Intelligence (Wechsler 1999). For Spanish-speaking families, mothers were required to receive an average scaled score ≥4 on the vocabulary and matrix reasoning subtests of the Escala de Inteligencia Wechsler Para Adultos—Third Edition (Pons et al. 2008a). No mothers were excluded based on this criterion. Additional exclusion criteria included infant major sensory impairments (e.g. deafness or blindness) or motor impairments that significantly affected mobility, as well as current child protection services involvement, although no families were excluded based on these criteria.
Procedure
Research staff approached families during well or sick visits for their infants between 12 and 15 months and obtained informed consent before the screening. All procedures were approved by the University and Hospital Institutional Boards. Of the 147 families participating in the screening, a total of 60 families (41%) met study criteria and were enrolled and randomized to the intervention (n = 31) or standard pediatric primary care (n = 29) using a computerized random number generator (see Fig. 1). In the standard care group, infants continued to receive health care at the pediatric primary care clinic, including well and sick visits, but did not receive the intervention (described in more detail below). There were no significant differences in demographic variables between families in the intervention condition or the control group. Data were collected from the primary caregiver, who was the mother in all cases. Families completed the baseline assessment in their home and were informed of their group status at that time. Independent assessors masked to group status conducted a post assessment (n = 48; 80% retention) 2 months after the baseline assessment and follow-up assessments (n = 46; 77% retention) 3 and 6 months after the post assessment. For the intervention group, there was a retention rate of 65%, which is consistent with retention rates observed in other PCIT trials (Eyberg et al. 2014). There was no statistically significant difference in attrition rate between Spanish- and English-speaking families. Families received $50 for participation in each assessment.
Fig. 1.
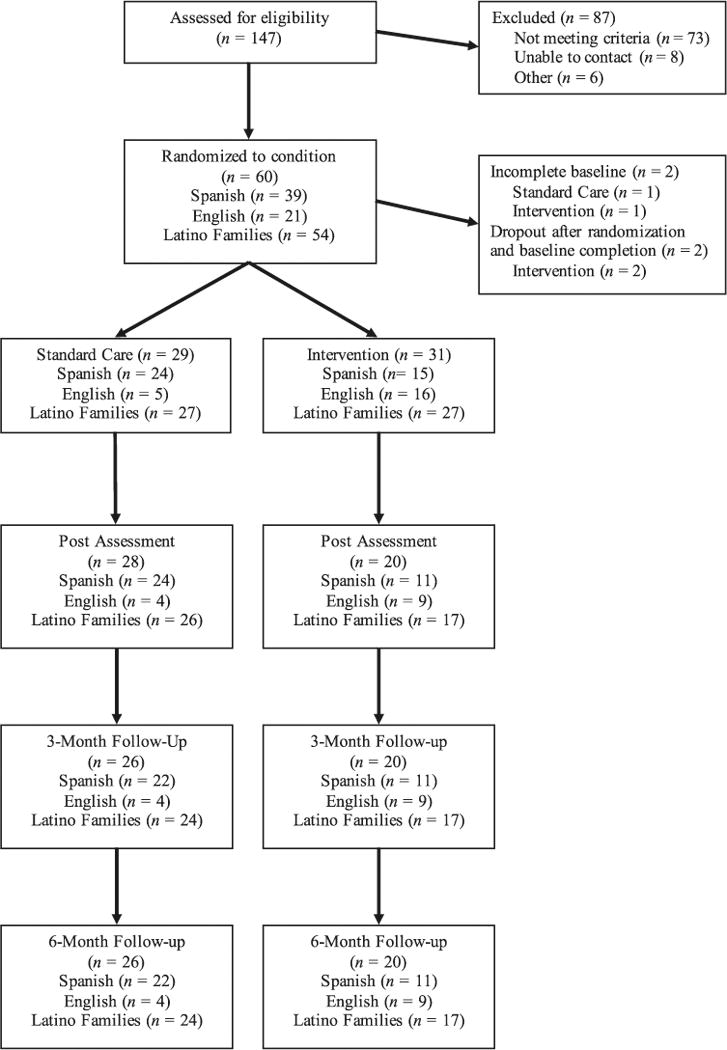
Participant flow through trial
Intervention
The Infant Behavior Program is a home-based adaptation of the CDI phase of PCIT (Bagner et al. 2016). Similar to standard PCIT, in the first teach session, the therapist taught the parent(s) to follow their infant’s lead in play by decreasing the don’t skills (i.e., commands, questions, and negative statements) and increasing the do/PRIDE skills (i.e., praises, reflections, imitation, descriptions, and enjoyment in the play). Parents were trained on how to direct the PRIDE skills to their infant’s appropriate play and to ignore disruptive behaviors (e.g., temper tantrums, whining). Following the teach session, parent skills were assessed during a 5-min observation at the start of each coach session, and data collected were used by the therapist to coach the parent(s) in their use of the skills. Furthermore, consistent with research on PCIT for children with intellectual disability (Bagner and Eyberg 2007), parents were encouraged to repeat appropriate infant vocalizations, as some of the infants in the current study did not yet use words.
Intervention Format
Each session was conducted weekly in the family’s home and lasted approximately 60 to 90 min. The therapists were all doctoral students in clinical psychology trained by the senior author, who is a PCIT Master Trainer. During each session, the therapist problem solved with each family ways to optimize in-home coaching, such as choosing an appropriate location for the session and developing strategies to minimize distractions (e.g., tuning off the television). Parents were instructed to practice the skills described above for 5 min every day. Of the 27 families attending the first session, seven (26%) dropped out before completing the intervention, which is consistent with the dropout rates in standard PCIT (Eyberg et al. 2014) and is relatively low given the high-risk nature of our sample. On average, families completed the intervention in 6.1 sessions (range from five to seven sessions), which included the initial teach session. Given the evidence that time-limited PCIT interventions fared as well as, and in some cases better than, variable PCIT where mastery criteria were required (Thomas and Zimmer-Gembeck 2012), we capped the intervention at seven sessions (including the teach session) and did not require the primary caregiver to reach mastery criteria to complete the intervention. However, 45% of families completed the intervention in less than seven sessions (range of five to six sessions) because the primary caregiver met mastery criteria (i.e., less than 3 questions, commands, and criticisms and 10 labeled praises, 10 behavior descriptions, and 10 reflections or reflected 75% of the infant’s speech, consistent with previous work with children with developmental delay; Bagner and Eyberg 2007) during a 5-min infant-led play. Of all the intervention completers, 65% of families met mastery criteria for both do and don’t skills at their final session, and 90% of families met criteria for either do or don’t skills. No group differences in meeting mastery criteria were found between Spanish- and English-speaking families. Families not completing the intervention dropped out after completing an average of 3.1 sessions, and no dropout family met mastery criteria.
Intervention Fidelity
All sessions were videotaped, and 63% of sessions were randomly selected and coded. Average fidelity across sessions, defined as the percent with which the therapist adhered to key elements of each session detailed in the manual, was 97%. Of the coded tapes, 40% were randomly selected and coded a second time for reliability and yielded an interobserver reliability estimate of 95%.
Measures
Brief Infant-Toddler Social and Emotional Assessment (BITSEA)
The BITSEA (Carter and Briggs-Gowan 2006) is a 42-item, nationally standardized screener designed to assess behavioral problems and competencies in 12- to 36- month-olds. The 31-item problem scale has excellent test- retest reliability (r = 0.91 to 0.92) and very good inter-rater reliability (r = 0.70 to 0.78), as well as support for discriminative validity yielding excellent sensitivity and good specificity for those scoring above the clinical cutoff of the 75th percentile. Examples of items on the problem scale include “restless and can’t sit still,” “is destructive,” and “hits, bites or kicks,” and are rated on a scale of 0 (not true/rarely), 1 (somewhat true/sometimes), or 2 (very true/often). Cronbach’s alpha for the problem scale in the current sample was 0.77.
Wechsler Abbreviated Scale of Intelligence (WASI) and Escala de Inteligencia Wechsler Para Adultos—Third Edition (EIWA-III)
The WASI (Wechsler 1999) is a brief measure of intelligence with high reliability and validity (Hays et al. 2002). The EIWA-III is the Spanish version of the full Wechsler Scale of Intelligence (Wechsler 1997) with demonstrated reliability (Pons et al. 2008a, b) and validity (Pons et al. 2008a, b). As indicated above, mothers speaking English were required to receive an estimated IQ score ≥70 on the two-subtest (vocabulary and matrix reasoning) version of the WASI, and mothers speaking Spanish were required to receive an average scaled score ≥4 on the vocabulary and matrix reasoning subtests of the EIWA-III.
Dyadic Parent-Child Interaction Coding System-Third Edition (DPICS-III)
The DPICS-III (Eyberg et al. 2004) is a behavioral coding system with documented reliability and validity that was used to assess observed parenting skills taught during PCIT. Specifically, we coded mother do skills (i.e., praises, behavior descriptions, and reflections) and don’t skills (i.e., questions, commands, and negative talk) during a 5-min infant-led play at all assessments to reflect positive and negative parent verbalizations used during infant-led play. The DPICS-III has demonstrated reliability and validity for Spanish-speaking dyads (Bagner et al. 2016; Borrego et al. 2006; Calzada and Eyberg 2002; Matos et al. 2006; McCabe et al. 2010, 2012, 2013; McCabe and Yeh 2009). Coders masked to group status were trained to 80% agreement with a criterion tape and coded half of the observations at baseline a second time for reliability, yielding an excellent overall kappa (0.84) for all codes examined in the current study.
Data Analyses
We compared do and don’t skill acquisition and utilization between Latino families that received the intervention (n = 27) and in which the primary caregiver spoke English or Spanish. Most primary caregivers spoke only English or only Spanish during the 5-min infant-led play. For the small number of primary caregivers who spoke both English and Spanish during the infant-led play (n = 3), independent evaluators coded the number of English and Spanish verbalizations. Given that most of the language production for these families was in Spanish (more than 60% for each family), they were all considered Spanish-speaking families. Based on the unequal composition of Spanish- vs. English-speaking Latino families in the standard-care group (24 Spanish-speaking families and 3 English-speaking families) compared to the intervention group (15 Spanish-speaking families and 12 English-Speaking families), we were unable to examine possible moderating effect of language on the relation between intervention group and skill acquisition and utilization across conditions. Instead, we used multiple linear regression analyses to analyze differences in acquisition and utilization of do and don’t skills between Spanish- and English-speaking Latino families only among families receiving the intervention (n = 27). Specifically, for acquisition, we included language (i.e., Spanish or English) as the independent variable and baseline levels of the skill analyzed (i.e., do or don’t skills) as a covariate to examine the extent to which language predicted change in skills from baseline to post-intervention and the 3- and 6-month follow-up assessments. For utilization, we included language as the independent variable to examine the extent to which language predicted the frequency of do and don’t skills at each assessment point. For both acquisition and utilization analyses, we also controlled for maternal education because this variable was significantly correlated to outcome variables in the larger randomized controlled trial (Bagner et al. 2016).
Results
Means and standard deviations of the frequency of do and don’t skills among Spanish- and English-speaking Latino families along are presented in Table 1. In the regression analyses examining the effect of language on the acquisition of do skills, language spoken did not predict change over time between the baseline and post-intervention assessments, β = 0.233, CI (−18.33, 38.79), p = 0.45, or between the baseline and 3-month, β = 0.263, CI (−19.85, 48.55), p = 0.37, and 6-month, β = 0.318, CI (−17.81, 50.31), p = 0.31, follow-up assessments. Similarly, in the regression analyses examining the effect of language on the acquisition of don’t skills, language spoken did not predict change over time between the baseline and post-intervention assessments, β = 0.261, CI (−6.93, 20.20), p = 0.31, or between the baseline and 3-month, β = 0.056, CI (−13.47, 17.31), p = 0.79, and 6-month, β = 0.446, CI (−0.43, 38.34), p = 0.055, follow-up assessments.
Table 1.
Means of do and don’t skills among spanish- and english-speaking Latino families
| Assessment | Do skills
|
|
|---|---|---|
| Spanish | English | |
| Baseline | M = 10.26 (SD = 10.35) | M = 6.63 (SD = 4.96) |
| Post-treatment | M = 34.66 (SD = 22.84) | M = 28.50 (SD = 23.48) |
| 3-Month follow-up | M = 33.37 (SD = 26.68) | M = 23.00 (SD = 30.50) |
| 6-Month follow-up | M = 38.33 (SD = 21.26) | M = 26.42 (SD = 31.84) |
|
| ||
| Assessment | Don’t Skills
|
|
| Spanish | English | |
|
| ||
| Baseline | M = 69.73 (SD = 42.62) | M = 24.36 (SD =16.64) |
| Post-treatment | M = 19.55 (SD = 13.68) | M = 3.00 (SD = 3.25) |
| 3-Month follow-up | M = 27.87 (SD = 18.83) | M = 6.62 (SD = 7.42) |
| 6-Month follow-up | M = 36.00 (SD = 20.01) | M = 6.14 (SD = 8.27) |
In the regression analyses examining the effect of language on the utilization of do skills, language spoken did not predict level of do skills at the baseline, β = 0.214, CI (−3.48, 10.75), p = 0.30, or post-intervention, β = 0.155, CI (−18.91, 32.58), p = 0.57, assessments, as well as at the 3-month, β = 0.299, CI (−16, 48.61), p = 0.29, and 6-month, β = 0.260, CI (−17.73, 44.29), p = 0.37, follow-up assessments. However, in the regression analyses examining the effect of language on the utilization of don’t skills, language significantly predicted level of don’t skills at the baseline, β = .562, CI (18.15, 72.48), p = 0.002, and post-intervention, β = 0.683, CI (6.08, 28.61), p = 0.005, assessments, as well as at the 3-month, β = 0.499, CI (1.84, 32.29), p = 0.031, and 6-month, β = 0.554, CI (9.43, 37.73), p = 0.003, follow-up assessments. The differences in the use of don’t skills at each assessment between Spanish- and English-speakers are illustrated in Fig. 2. Language spoken (and maternal education as a covariate) explained a significant proportion of variance in the number of don’t skills at the baseline, R2 = 0.39, F(2, 23) = 7.35, p = 0.003, and post-intervention, R2 = 0.43, F(2, 14) = 5.48, p = 0.017, assessment, as well as at the 3-month, R2 = 0.50, F(2, 13) = 6.70, p = 0.010, and 6-month, R2 = 0.71, F(2, 13) = 16.61, p < 0.001, follow-up assessments.
Fig. 2.
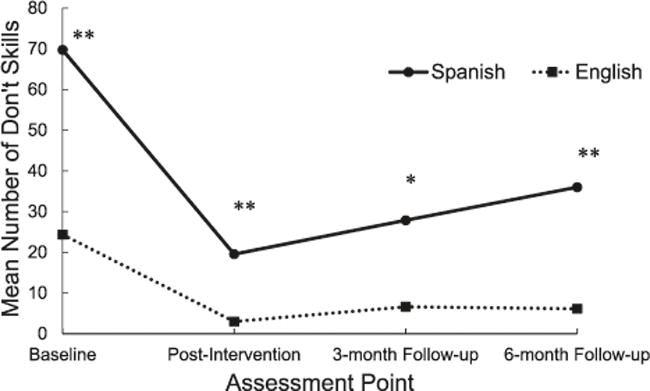
Differences in don’t skills between Spanish- and English-speaking Latino families. Note. *p < .05, **p < .01
Given the significant differences in the utilization of the don’t skills composite score at each time point between Spanish- and English-speaking families, we conducted additional multiple regression analyses to examine the utilization of each individual don’t skill (i.e., commands, criticisms, and questions) at each assessment (while controlling for maternal education as in previous analyses). There were no significant differences in the use of criticisms between groups at any time point. However, there were significant group differences in the use of commands at the baseline, β = 0.582, CI (16.65, 57.90), p = 0.001, post-intervention, β = 0.520, CI (0.16, 17.40), p = 0.046, and 6- month follow-up, β = 0.650, CI (5.52, 43.60), p = 0.016, assessments. Language spoken (and maternal education as a covariate) explained a significant proportion of variance in the number of commands at the baseline, R2 = 0.39, F(2, 23) = 9.17, p = 0.001, post-intervention, R2 = 0.25, F(2, 14) = 2.42, p = 0.12, and 6-month follow-up, R2 = 0.41, F(2, 12) = 4.22, p = 0.041, assessments. There were also significant group differences in the use of questions at the post-intervention, β = 0.711, CI (2.79, 11.33), p = 0.003, and 6-month follow-up, β = 0.445, CI (2.55, 20.62), p = 0.016, assessments. Language spoken (and maternal education as a covariate) explained a significant proportion of variance in the number of questions at the post-intervention, R2 = 0.47, F(2, 14) = 6.32, p = 0.011, and 6-month followup, R2 = 0.69, F(2, 13) = 14.74, p < 0.001, assessments. Means and standard deviations of the frequency of commands and questions among Spanish- and English-speaking Latino families along are presented in Table 2.
Table 2.
Means of commands and questions among spanish- and english-speaking Latino families
| Assessment | Commands
|
|
|---|---|---|
| Spanish | English | |
| Baseline | M = 53.60 (SD = 32.66) | M = 16.27 (SD = 15.16) |
| Post-treatment | M = 10.88 (SD = 10.39) | M = 2.37 (SD = 2.32) |
| 3-Month follow-up | M = 15.37 (SD = 14.20) | M = 3.25 (SD = 5.41) |
| 6-Month follow-up | M = 56.77 (SD = 17.50) | M = 32.50 (SD = 10.67) |
|
| ||
| Assessment | Questions
|
|
| Spanish | English | |
|
| ||
| Baseline | M = 13.00 (SD = 10.97) | M= 5.72 (SD =5.44) |
| Post-treatment | M = 7.33 (SD = 5.17) | M = 0.62 (SD = 1.40) |
| 3-Month follow-up | M = 9.75 (SD = 7.86) | M = 2.50 (SD = 4.75) |
| 6-Month follow-up | M = 21.66 (SD = 13.88) | M = 5.57 (SD = 4.23) |
Discussion
Previous studies have evaluated the effects of culturally-adapted PCIT protocols for Spanish speakers (Borrego et al. 2006; Matos et al. 2006; Matos et al. 2009) and compared a culturally-adapted version of PCIT to a non-adapted protocol (McCabe et al. 2012; McCabe and Yeh 2009), but none of these studies compared verbal skills targeted in PCIT between Spanish- and English-speaking Latino families. In the current study, we addressed this significant gap in the literature by comparing the acquisition and utilization of do and don’t skills among Spanish- and English-speaking Latino families receiving a non-culturally adapted version of the CDI phase of PCIT for high-risk infants and their families. These comparisons allowed us to identify how both English- and Spanish-speaking Latino families learn and maintain verbal skills following CDI.
The finding that English- and Spanish-speaking Latino families did not differ in change over time in their use of do and don’t skills (i.e., acquisition) suggests that the intervention was equally effective in promoting PCIT skills among parents in both groups, which contradicted our hypothesis and previous studies showing lower acquisition rates among Latino families (Matos et al. 2006; McCabe and Yeh 2009). However, previous studies included different mastery criteria standards that may explain these inconsistent findings. For example, in the GANA program (McCabe and Yeh 2009) the primary caregiver was required to meet mastery criteria to successfully complete treatment. On the other hand, the PCIT adaptation for Puerto Rican families (Matos et al. 2006) included a limit of eight sessions for CDI and nine sessions for PDI and did not require the primary caregiver to reach mastery criteria to complete the treatment. Thus, future studies should compare the role of language in the acquisition rate of skills in both mastery-based and time-limited PCIT protocols for Latino families. This line of research is pivotal to determine if mastery criteria standards in place are culturally robust for Latino families. Additionally, the impact of therapist’s characteristics on the acquisition rate of PCIT skills needs to be further examined. There is evidence that the didactic in vivo coaching model used in PCIT facilitates skill acquisition and leads to similar treatment change trajectories despite individual differences among families (Hakman et al. 2009). Therefore, it is possible that the acquisition rate of PCIT skills is equally influenced by therapists’ and families’ variables. In the future, studies should examine how therapist behaviors (e.g., coaching styles; see Barnett et al. 2015) interplay with families’ variables (e.g., language use, level of acculturation) to affect the acquisition rate of PCIT skills among Latino families.
Concerning the utilization of the parenting skills, the frequency in the use of do skills at each time point was similar between Spanish- and English-speaking families. This finding contradicted our initial hypothesis but is consistent with the results of other studies in which Mexican-American families used do skills similarly despite language preference (i.e., English or Spanish) and level of acculturation (McCabe et al. 2010). These results also support the finding that Latino families affectionately interact with their children regardless of language preference and level of acculturation (Calzada et al. 2013). On the other hand, Spanish-speaking families used significantly more don’t skills at each assessment compared to their English-speaking counterparts, which was consistent with our prediction and with the evidence that Spanish-speaking families use more don’t skills during PCIT (Matos et al. 2009). The current results suggest that some guidelines in the published PCIT protocol (Eyberg and Funderburk 2011) may be difficult for Spanish-speaking families to follow due to lack of familiarity with the skills and/or cultural acceptability of them. In PCIT, mastery criteria for don’t skills require less than three questions, commands, and criticisms and determine when families move on to the second phase of treatment and can successfully graduate from treatment (Blizzard et al. 2017b). Therefore, it may be more difficult for Spanish-speaking families than English-speaking families to meet this mastery criterion, which could impact satisfaction and treatment engagement. A further analysis to determine the extent to which mastery criteria facilitate the consolidation of parenting skills is warranted considering the high attrition rates in community settings and the evidence that the most significant gains in parenting skills occurs in the first few sessions of treatment before mastery criteria are achieved (Hakman et al. 2009; Timmer et al. 2016). The importance of this work is highlighted by evidence that non-completer families acquired PCIT skills at a similar rate than treatment completer families in community settings with primarily Latino families (Timmer et al. 2016), which suggest extra sessions to achieve mastery criteria may not necessarily result in a higher rate of skill acquisition or utilization. Nevertheless, additional empirical work is needed to better elucidate how mastery criteria standards could facilitate the rehearsal of less culturally familiar skills as previous work suggests (Lau et al. 2011; Matos et al. 2006; McCabe and Yeh 2009).
When examining differences in the utilization of specific don’t skills, we found that Spanish-speaking families used significantly more commands than English-speaking families at baseline, post-intervention, and the 6-month follow-up assessments. Similarly, Spanish-speaking families used more questions at the post-intervention and 6-month follow-up assessments. It is important to point out that the modest size of our sample may have limited power to detect significant differences in the use commands at the 3-month follow-up assessment, or questions at the baseline and 3-month follow-up assessments. Nevertheless, these findings may reflect the influence of the cultural variable respeto in parent-training interventions with Latino families. For example, it is a priority for Latino mothers to ensure their children obey rules and respect authority figures (Calzada et al. 2012), so they might use commands and questions to inculcate these cultural practices from an early age. This hypothesis is consistent with research on the behavioral manifestations of respeto (e.g., giving orders and not expecting any questioning, asking questions as a way to give commands) and how Latino mothers teach their children these practices (Calzada et al. 2010). For example, Mexican-American mothers seemed to rely on the use of commands as a way to indicate the normative behavior expected from their children (Livas-Dlott et al. 2010).
Additionally, there is evidence that among Latino families the socialization of respeto is influenced by language preference, where Spanish speakers used more respeto-related practices compared to English speakers (Calzada et al. 2012). Nevertheless, more empirical research is needed to understand whether the use of commands and questions in Latino families promote the same type of negative interactions described among non-Latino White families. For instance, there is evidence that at least among mostly Latino families, levels of PCIT don’t skills were not associated with attachment-based intrusive caregiving (Blizzard et al. 2017a). Thus, future studies examining the relations between PCIT skills and the perception of warmth and intrusive parenting practices among Latino families are warranted. The current results highlight the potential importance of addressing respeto-related behaviors during PCIT with Latino families. This possible modification to the existing protocols is consistent with a data-driven approach to culturally adapting interventions, especially parent-training programs, for diverse populations (see Lau 2006; Ortiz and Del Vecchio 2013).
Limitations
Despite the implications of these results have in understanding how English- and Spanish-speaking Latino families respond to parent-training programs, there are some limitations of this study that should be noted. First, the sample size of the current study was relatively small and did not allow us to use more sophisticated statistical analyses such as multilevel modeling (see Mass and Hox 2005; McNeish and Stapleton 2016). Moreover, the uneven distribution between Spanish- and English-speaking families prevented us from examining the possible moderating role of language across groups. The identification of moderators of treatment outcome has been neglected in the literature but is of pivotal importance to ensure that PCIT (and other parent-training interventions) are culturally robust for Latino families (see Ortiz and Del Vecchio, 2013). Second, the Infant Behavior Program was a time-limited adaptation of the CDI phase of the standard PCIT protocol. Therefore, as mentioned before, future research should examine differences in the acquisition and utilization of skills between Spanish- and English-speaking families following time-unlimited PCIT protocols. Third, we did not collect information on the nationality of the participants, which may have concealed other differences between these groups. Even though our sample consisted of a heterogeneous Latino population, and therefore may be more representative of the Latino community as a whole than previous studies, the term “Latino” subsumes a broad constellation of nationalities, traditions, practices, and acculturation trajectories, and Latinos do not necessary adhere similarly to certain parenting values and practices (Barker et al. 2010). In future studies, it would be important to compare specific Latino groups (e.g., Mexicans, Puerto Ricans, Dominicans, Cubans, etc.) to examine potential differences in the use of don’t skills, and specifically commands and questions, as a socialization of respeto in these subgroups. Forth, this study did not include a specific scale to measure level of acculturation or cultural attitudes and practices. In future studies, the use of psychometric scales to examine the relation between respeto-related attitudes, behaviors, and parenting practices is warranted.
Acknowledgments
Funding Funding for this work was provided by the FIU Ronald E. McNair Post Baccalaureate Achievement Program awarded to the first author, and the National Institute of Mental Health, K23MH085659, awarded to the senior author. We thank Tommy Chou for his consultation and feedback on an early version of this manuscript and all participating families for their commitment to our research program.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the Florida International University research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Footnotes
Author Contributions G.R.: designed the study, performed the data analyses, and wrote the paper. A.B.: assisted with the design of the study and with the editing of the manuscript. N.B.: assisted with execution of the study, the statistical analyses, and collaborated in editing of the manuscript. D.B.: designed and led the larger study on which this study was based, assisted with the design and execution of this study and collaborated with the editing of the manuscript.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no competing interests.
Informed Consent Informed consent was obtained from all individual participants included in the study.
References
- Abrahamse ME, Junger M, Chavannes EL, Coelman FJ, Boer F, Lindauer RJ. Parent-child interaction therapy for preschool children with disruptive behavior problems in the Netherlands. Child and Adolescent Psychiatry and Mental Health. 2012;6:1–9. doi: 10.1186/1753-2000-6-24. https://doi.org/10.1186/1753-2000-6-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alegría M, Canino G, Shrout PE, Woo M, Duan N, Vila D, Meng XL. Prevalence of mental illness in immigrant and non-immigrant U.S. Latino groups. American Journal of Psychiatry. 2008;165:359–369. doi: 10.1176/appi.ajp.2007.07040704. https://doi.org/10.1176/appi.ajp.2007.07040704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bagner DM, Coxe S, Hungerford GM, García D, Barroso NE, Hernández J, Rosa-Olivares J. Behavioral parent training in infancy: A window of opportunity for high-risk families. Journal of Abnormal Child Psychology. 2016;44:901–912. doi: 10.1007/s10802-015-0089-5. https://doi.org/10.1007/s10802-015-0089-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bagner DM, Eyberg SM. Parent-child interaction therapy for disruptive behavior in children with mental retardation: A randomized controlled trial. Journal of Clinical Child and Adolescent Psychology. 2007;36:418–429. doi: 10.1080/15374410701448448. https://doi.org/10.1080/15374410701448448. [DOI] [PubMed] [Google Scholar]
- Bagner DM, Rodríguez GM, Blake CA, Linares D, Carter AS. Assessment of behavioral and emotional problems in infancy: A systematic review. Clinical Child and Family Psychology Review. 2012;15:113–128. doi: 10.1007/s10567-012-0110-2. https://doi.org/10.1007/s10567-012-0110-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barker CH, Cook KL, Borrego J. Addressing cultural variables in parent training programs with Latino families. Cognitive and Behavioral Practice. 2010;17:157–166. https://doi.org/10.1016/j.cbpra.2010.01.002. [Google Scholar]
- Barnett ML, Niec LN, Peer SO, Jent JF, Weinstein A, Gisbert P, Simpson G. Successful therapist–parent coaching: How in vivo feedback relates to parent engagement in parent–child interaction therapy. Journal of Clinical Child & Adolescent Psychology. 2015:1–8. doi: 10.1080/15374416.2015.1063428. https://doi.org/10.1080/15374416.2015.1063428. [DOI] [PubMed]
- Baumann AA, Domenech Rodríguez MM, Amador NG, Forgatch MS, Parra-Cardona JR. Parent management training-oregon model (PMTO™) in Mexico City: Integrating cultural adaptation activities in an implementation model. Clinical Psychology: Science and Practice. 2014;21:32–47. doi: 10.1111/cpsp.12059. https://doi.org/10.1111/cpsp.12059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benish SG, Quintana S, Wampold BE. Culturally adapted psychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. Journal of Counseling Psychology. 2011;58:279–289. doi: 10.1037/a0023626. https://doi.org/10.1037/a0023626. [DOI] [PubMed] [Google Scholar]
- Berdahl TA, Torres Stone RA. Examining Latino differences in mental healthcare use: The roles of acculturation and attitudes towards healthcare. Community Mental Health Journal. 2009;45:393–403. doi: 10.1007/s10597-009-9231-6. https://doi.org/10.1007/s10597-009-9231-6. [DOI] [PubMed] [Google Scholar]
- Berry JW. Conceptual approaches to understanding acculturation. In: Chun KM, Organista PB, Marín G, editors. Acculturation: Advances in theory, measurement, and applied research. Washington, DC: American Psychological Association; 2003. pp. 17–38. [Google Scholar]
- Bjørseth Å, Wichstrøm L. Effectiveness of parent-child interaction therapy (PCIT) in the treatment of young children’s behavior problems. A randomized controlled study. PLoS ONE. 2016;11:1–19. doi: 10.1371/journal.pone.0159845. https://doi.org/10.1371/journal.pone.0159845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blizzard AM, Barroso NE, Ramos FG, Graziano P, Bagner DM. Behavioral parent training in infancy: What about the parent-infant relationship? Journal of Clinical Child and Adolescent Psychology. 2017a:1–13. doi: 10.1080/15374416.2017.1310045. https://doi.org/10.1080/15374416.2017.1310045. [DOI] [PMC free article] [PubMed]
- Blizzard A, Eyberg S, Bagner D. Parent-child interaction therapy for the treatment of externalizing behavior problems in children with intellectual and developmental disabilities. SAGE Encyclopedia of Intellectual and Developmental Disorders. 2017b in press. [Google Scholar]
- Borrego J, Anhalt K, Terao SY, Vargas EC, Urquiza AJ. Parent-child interaction therapy with a Spanish-speaking family. Cognitive and Behavioral Practice. 2006;13:121–133. https://doi.org/10.1016/j.cbpra.2005.09.001. [Google Scholar]
- Borrego J, Ibañez ES, Spendlove SJ, Pemberton JR. Treatment acceptability among Mexican American parents. Behavior Therapy. 2007;38:218–227. doi: 10.1016/j.beth.2006.08.007. https://doi.org/10.1016/j.beth.2006.08.007. [DOI] [PubMed] [Google Scholar]
- Calzada EJ, Basil S, Fernández Y. What Latina mothers think of evidence-based parenting practices: A qualitative study of treatment acceptability. Cognitive and Behavioral Practice. 2013;20:362–374. https://doi.org/10.1016/j.cbpra.2012.08.004. [Google Scholar]
- Calzada EJ, Eyberg SM. Self-reported parenting practices in Dominican and Puerto Rican mothers of young children. Journal of Clinical Child and Adolescent Psychology. 2002;31:354–363. doi: 10.1207/S15374424JCCP3103_07. https://doi.org/10.1207/S15374424JCCP3103. [DOI] [PubMed] [Google Scholar]
- Calzada EJ, Fernández Y, Cortés DE. Incorporating the cultural value of respeto into a framework of Latino parenting. Cultural Diversity and Ethnic Minority Psychology. 2010;16:77–86. doi: 10.1037/a0016071. https://doi.org/10.1037/a0016071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzada EJ, Huang KY, Anicama C, Fernández Y, Brotman LM. Test of a cultural framework of parenting with Latino families of young children. Cultural Diversity and Ethnic Minority Psychology. 2012;18:285–296. doi: 10.1037/a0028694. https://doi.org/10.1037/a0028694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter AS, Briggs-Gowan MJ. ITSEA/BITSEA: Infant toddler and brief infant toddler social and emotional assessment examiner’s manual. San Antonio: Harcourt Assessment; 2006. [Google Scholar]
- Ceballo R, Hurd N. Neighborhood context, SES, and parenting: Including a focus on acculturation among Latina mothers. Applied Developmental Science. 2008;12:176–180. https://doi.org/10.1080/10888690802387997. [Google Scholar]
- Chen YC, Fortson BL. Predictors of treatment attrition and treatment length in parent-child interaction therapy in Taiwanese families. Children and Youth Services Review. 2015;59:28–37. doi: 10.1016/j.childyouth.2015.10.009. https://doi.org/10.1016/j.childyouth.2015.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Archives General Psychiatry. 2003;60:837–844. doi: 10.1001/archpsyc.60.8.837. https://doi.org/10.1001/archpsyc.60.8.837. [DOI] [PubMed] [Google Scholar]
- Domenech Rodríguez MM, Baumann AA, Schwartz AL. Cultural adaptation of an evidence based intervention: From theory to practice in a Latino/a community context. American Journal of Community Psychology. 2011;47:170–186. doi: 10.1007/s10464-010-9371-4. https://doi.org/0.1007/s10464-010-9371-4. [DOI] [PubMed] [Google Scholar]
- Eyberg SM, Boggs SR, Jaccard J. Does maintenance treatment matter? Journal of Abnormal Child Psychology. 2014;42:355–366. doi: 10.1007/s10802-013-9842-9. https://doi.org/10.1007/s10802-013-9842-9. [DOI] [PubMed] [Google Scholar]
- Eyberg SM, Funderburk B. Parent-child interaction therapy protocol. Gainesville, FL: PCIT International; 2011. [Google Scholar]
- Eyberg SM, Nelson MM, Duke M, Boggs SR. Manual for the dyadic parent- child interaction coding system. 3rd. Thousand Oaks, CA: Sage; 2004. [Google Scholar]
- Fernández MA, Butler AM, Eyberg SM. Treatment outcome for low socioeconomic status African American families in parent-child interaction therapy: A pilot study. Child & Family Behavior Therapy. 2011;33:32–48. https://doi.org/10.1080/07317107.2011.545011. [Google Scholar]
- Hakman M, Chaffin M, Funderburk B, Silovsky JF. Change trajectories for parent-child interaction sequences during parent-child interaction therapy for child physical abuse. Child Abuse & Neglect. 2009;33:461–470. doi: 10.1016/j.chiabu.2008.08.003. https://doi.org/10.1016/j.chiabu.2008.08.003. [DOI] [PubMed] [Google Scholar]
- Hall GCN, Ibaraki AY, Huang ER, Marti CN, Stice E. A meta-analysis of cultural adaptations of psychological interventions. Behavior Therapy. 2016;47:993–1014. doi: 10.1016/j.beth.2016.09.005. https://doi.org/10.1016/j.beth.2016.09.005. [DOI] [PubMed] [Google Scholar]
- Hays JR, Reas DL, Shaw JB. Concurrent validity of the wechsler abbreviated scale of intelligence and the kaufman brief intelligence test among psychiatric inpatients. Psychological Reports. 2002;90:355–359. doi: 10.2466/pr0.2002.90.2.355. https://doi.org/10.2466/pr0.2002.90.2.355. [DOI] [PubMed] [Google Scholar]
- Huey SJ, Jr, Polo AJ. Evidence-based psychosocial treatments for ethnic minority youth. Journal of Clinical Child & Adolescent Psychology. 2008;37:262–301. doi: 10.1080/15374410701820174. https://doi.org/10.1080/15374410701820174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kataoka SH, Zhang L, Wells KB. Unmet need for mental health care among U.S. children: Variation by ethnicity and insurance status. The American Journal of Psychiatry. 2002;159:1548–1555. doi: 10.1176/appi.ajp.159.9.1548. https://doi.org/10.1176/appi.ajp.159.9.1548. [DOI] [PubMed] [Google Scholar]
- Kim RE, Lau AS, Chorpita BF. The impact of Latino caregiver acculturation on treatment engagement in children’s community mental health services. Journal of Child and Family Studies. 2015;25:891–901. https://doi.org/10.1007/s10826-015-0259-7. [Google Scholar]
- Lau AS. Making the case for selective and directed cultural adaptations of evidence-based treatments: Examples from parent training. Clinical Psychology: Science and Practice. 2006;13:295–310. https://doi.org/10.1111/j.1468-2850.2006.00042.x. [Google Scholar]
- Lau AS, Fung JJ, Ho LY, Liu LL, Gudiño OG. Parent training with high-risk immigrant Chinese families: A pilot group randomized trial yielding practice-based evidence. Behavior Therapy. 2011;42:413–426. doi: 10.1016/j.beth.2010.11.001. https://doi.org/10.1016/j.beth.2010.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung C, Tsang S, Heung K, Yiu I. Effectiveness of parent-child interaction therapy (PCIT) among Chinese families. Research on Social Work Practice. 2009;19:304–313. https://doi.org/10.1177/1049731508321713. [Google Scholar]
- Livas-Dlott A, Fuller B, Stein GL, Bridges M, Mangual Figueroa A, Mireles L. Commands, competence, and cariño: Maternal socialization practices in Mexican American families. Developmental Psychology. 2010;46:566–578. doi: 10.1037/a0018016. https://doi.org/10.1037/a0018016. [DOI] [PubMed] [Google Scholar]
- López M, González-Barrera A. What is the future of Spanish in the United States? 2013 http://www.pewresearch.org/fact-tank/2013/09/05/what-is-the-future-of-spanish-in-the-united-states/
- Martínez CR, Jr, Eddy JM. Effects of culturally adapted parent management training on Latino youth behavioral health outcomes. Journal of Consulting and Clinical Psychology. 2005;73:841–851. doi: 10.1037/0022-006X.73.5.841. https://doi.org/10.1037/0022-006X.73.5.841. [DOI] [PubMed] [Google Scholar]
- Maas CJ, Hox JJ. Sufficient sample sizes for multilevel modeling. Methodology. 2005;1:86–92. [Google Scholar]
- Matos M, Bauermeister JJ, Bernal G. Parent-child interaction therapy for Puerto Rican preschool children with ADHD and behavior problems: A pilot efficacy study. Family Process. 2009;48:232–252. doi: 10.1111/j.1545-5300.2009.01279.x. https://doi.org/10.1111/j.1545-5300.2009.01279.x. [DOI] [PubMed] [Google Scholar]
- Matos M, Torres R, Santiago R, Jurado M, Rodríguez I. Adaptation of parent-child interaction therapy for Puerto Rican families: A preliminary study. Family Process. 2006;45:205–222. doi: 10.1111/j.1545-5300.2006.00091.x. https://doi.org/10.1111/j.1545-5300.2006.00091.x. [DOI] [PubMed] [Google Scholar]
- McCabe KM, Shanley JR, Niec LN, Naaf M, Yeh M, Lau AS. Cultural differences in the parenting of young children: An observational study of low-income Mexican American and European American families. Child & Family Behavior Therapy. 2013;35:307–326. https://doi.org/10.1080/07317107.2013.846680. [Google Scholar]
- McCabe KM, Yeh M, Garland AF, Lau AS, Chavez G. The GANA program: A tailoring approach to adapting parent child interaction therapy for Mexican Americans. Education & Treatment of Children. 2005;28:111–129. [Google Scholar]
- McCabe K, Yeh M. Parent–child interaction therapy for Mexican Americans: A randomized clinical trial. Journal of Clinical Child & Adolescent Psychology. 2009;38:753–759. doi: 10.1080/15374410903103544. https://doi.org/10.1080/15374410903103544. [DOI] [PubMed] [Google Scholar]
- McCabe K, Yeh M, Lau A, Argote CB, Liang J. Parent-child interactions among low-income Mexican American parents and preschoolers: Do clinic-referred families differ from nonreferred families? Behavior Therapy. 2010;41:82–92. doi: 10.1016/j.beth.2009.01.003. https://doi.org/10.1016/j.beth.2009.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCabe K, Yeh M, Lau A, Argote CB. Parent-child interaction therapy for Mexican Americans: Results of a pilot randomized clinical trial at follow-up. Behavior Therapy. 2012;43:606–618. doi: 10.1016/j.beth.2011.11.001. https://doi.org/10.1016/j.beth.2011.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMahon RJ, Forehand RL. Helping the noncompliant child: Family-based treatment for oppositional defiant disorder. New York, NY: Guilford; 2003. [Google Scholar]
- McNeish DM, Stapleton LM. The effect of small sample size on two-level model estimates: A review and illustration. Educational Psychology Review. 2016;28:295–314. https://doi.org/10.1007/s10648-014-9287-x. [Google Scholar]
- Ortiz C, Del Vecchio T. Cultural diversity: Do we need a new wake-up call for parent training? Behavior Therapy. 2013;44:443–458. doi: 10.1016/j.beth.2013.03.009. https://doi.org/10.1016/j.beth.2013.03.009. [DOI] [PubMed] [Google Scholar]
- Parra Cardona JR, Domenech Rodríguez M, Forgatch M, Sullivan C, Bybee D, Holtrop K, Bernal G. Culturally adapting an evidence-based parenting intervention for Latino immigrants: The need to integrate fidelity and cultural relevance. Family Process. 2012;51:56–72. doi: 10.1111/j.1545-5300.2012.01386.x. https://doi.org/10.1111/j.1545-5300.2012.01386.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR. The next generation of PMTO models. The Behavior Therapist. 2005;28:25–32. [Google Scholar]
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry. 2015;56:345–365. doi: 10.1111/jcpp.12381. https://doi.org/10.1111/jcpp.12381. [DOI] [PubMed] [Google Scholar]
- Pons JI, Flores-Pabón L, Matías-Carrelo L, Rodríguez M, Rosario-Hernández E, Rodríguez JM, Yang J. Confiabilidad de la escala de inteligencia Wechsler para adultos versión III, Puerto Rico (EIWA-III) Revista Puertorriqueña de Psicología. 2008a;19:112–132. [Google Scholar]
- Pons JI, Matías-Carrelo L, Rodríguez M, Rodríguez JM, Herrans LL, Jiménez ME, Medina G. Estudios de validez de la escala de inteligencia Wechsler para adultos versión III, Puerto Rico (EIWA-III) Revista Puertorriqueña de Psicología. 2008b;19:75–111. [Google Scholar]
- Sanders MR, Cann W, Markie-Dadds C. The triple p-positive parenting programme: A universal population-level approach to the prevention of child abuse. Child Abuse Review. 2003;12:155–171. https://doi.org/10.1002/car.7. [Google Scholar]
- Smith TB, Domenech Rodríguez M, Bernal G. Culture. Journal of Clinical Psychology. 2011;67:166–175. doi: 10.1002/jclp.20757. https://doi.org/10.1002/jclp.20757. [DOI] [PubMed] [Google Scholar]
- Takeuchi D, Alegría M, Jackson JS, Williams DR. Immigration and mental health: Diverse findings in Asian, Black, and Latino populations. American Journal of Public Health. 2007;97:11–12. doi: 10.2105/AJPH.2006.103911. https://doi.org/10.2105/AJPH.2006.103911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas R, Zimmer-Gembeck MJ. Behavioral outcomes of parent-child interaction therapy and triple p—positive parenting program: A review and meta-analysis. Journal of Abnormal Child Psychology. 2007;35:475–495. doi: 10.1007/s10802-007-9104-9. https://doi.org/10.1007/s10802-007-9104-9. [DOI] [PubMed] [Google Scholar]
- Thomas R, Zimmer-Gembeck MJ. Parent-child interaction therapy: An evidence-based treatment for child maltreatment. Child Maltreatment. 2012;17:253–266. doi: 10.1177/1077559512459555. https://doi.org/10.1177/1077559512459555. [DOI] [PubMed] [Google Scholar]
- Timmer SG, Urquiza AJ, Boys DK, Forte LA, Quick-Abdullah D, Chan S, Gould W. Filling potholes on the implementation highway: Evaluating the implementation of parent–child interaction therapy in Los Angeles County. Child Abuse & Neglect. 2016;53:40–50. doi: 10.1016/j.chiabu.2015.11.011. https://doi.org/10.1016/j.chiabu.2015.11.011. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. FFF: Hispanic Heritage Month: 2015. 2015 http://www.census.gov/newsroom/facts-for-features/2015/cb15-ff18.html.
- van Mourik K, Crone MR, de Wolff MS, Reis R. Parent training programs for ethnic minorities: A meta-analysis of adaptations and effect. Prevention Science. 2016;18:95–105. doi: 10.1007/s11121-016-0733-5. https://doi.org/10.1007/s11121-016-0733-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vega WA, López SR. Priority issues in Latino mental health services research. Mental Health Services Research. 2001;3:189–200. doi: 10.1023/a:1013125030718. https://doi.org/10.1023/A:1013125030718. [DOI] [PubMed] [Google Scholar]
- Webster-Stratton C, Reid MJ. The incredible years parents, teachers, and children’s training series: A multifaceted approach for young children with conduct disorder. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York: Guilford; 2010. pp. 194–210. [Google Scholar]
- Wechsler D. Wechsler adult scale of intelligence. 3rd. San Antonio: Pearson; 1997. [Google Scholar]
- Wechsler D. Wechsler abbreviated scale of intelligence. San Antonio: Pearson; 1999. [Google Scholar]
- Zisser A, Eyberg SM. Treating oppositional behavior in children using parent-child interaction therapy. In: Kazdin AE, Weisz JR, editors. Evidence-based psychotherapies for children and adolescents. New York: Guilford; 2010. pp. 179–193. [Google Scholar]