

Abstract
We systematically searched available databases. We reviewed 6,143 studies published from 1833 to 2017. Reports in English, French, German, Italian, and Spanish were considered, as were publications in other languages if definitive treatment and recurrence at specific follow-up times were described in an English abstract. We assessed data in the manner of a meta-analysis of RCTs; further we assessed non-RCTs in the manner of a merged data analysis. In the RCT analysis including 11,730 patients, Limberg & Dufourmentel operations were associated with low recurrence of 0.6% (95%CI 0.3–0.9%) 12 months and 1.8% (95%CI 1.1–2.4%) respectively 24 months postoperatively. Analysing 89,583 patients from RCTs and non-RCTs, the Karydakis & Bascom approaches were associated with recurrence of only 0.2% (95%CI 0.1–0.3%) 12 months and 0.6% (95%CI 0.5–0.8%) 24 months postoperatively. Primary midline closure exhibited long-term recurrence up to 67.9% (95%CI 53.3–82.4%) 240 months post-surgery. For most procedures, only a few RCTs without long term follow up data exist, but substitute data from numerous non-RCTs are available. Recurrence in PSD is highly dependent on surgical procedure and by follow-up time; both must be considered when drawing conclusions regarding the efficacy of a procedure.
Introduction
For unknown reasons, the incidence of pilonidal sinus disease (PSD) has risen continuously during the past 50 years, particularly in European and North American young men1,2. In a German military cohort for example, the number of affected patients increased from 29/100,000 in 2000 to 48/100,000 in 2012, and the total number of PSD-related in-patient surgeries exceeded the number of inguinal hernia-related interventions in 20 to 40-year-old patients3. Recurrent disease may probably affect patients’ long-term satisfaction following PSD surgery4. Recurrence between 0 percent5 and 100 percent6 has been reported for PSD, and wide recurrence range can be seen even within the different surgical approach techniques as open treatment, primary midline closure or flap techniques and others. Some evidence suggests that recurrence is associated with surgical procedure and correlated with length of follow-up as well4,7. However, the data are conflicting, and applied follow-up times often appear to have been randomly chosen, which brings into question the validity of reported recurrence associated with different surgical procedures. The purpose of this meta-analysis and merged data analysis was therefore to obtain a comprehensive assessment of recurrence and to ascertain determinants of recurrence of PSD with respect to specific surgical procedures and follow-up time. We considered both randomised controlled trials (RCTs) and non-RCTs.
We thus assembled a database with sources from the first description of PSD in 1833 on, that included reported recurrence, year of publication, timeframes of follow-up, type of study, and patient- and procedure-specific factors. We grouped therapeutic procedures for cumulative statistical analyses (Table 1). Using this dataset, we assessed the efficacy of common surgical procedures employed in treating PSD as a function of recurrence. We found that the recurrence in PSD varied depending on the surgical procedure and on the length of follow-up. While naturally, an increase of recurrence could be observed with longer follow-up, the rate of this increase was varying among the different procedures. This indicates that a thorough evaluation of a procedure in view of recurrence has to include the specific relation of recurrence to follow-up time and cannot just be based on comparisons at one single follow-up time. The strength of our conclusions is substantially buttressed by the extensive analysis of a large database pertaining to particular therapeutic procedures.
Table 1.
Grouping of therapeutic strategies for analysis of recurrence rates in pilonidal sinus disease.
| Primary open | Excision, “exhairese”, vacuum assisted closure (VAC), sinusectomy/excision, atypical excision and any other primary open approaches including supplemental measures such as laser, phenol, cryotherapy, local or systemic antibiotics, and platelet rich plasma in wound |
| Primary median closure | Any primary midline closure approach including supplemental measures such as laser, phenol, cryotherapy, local antibiotics, drainage, wound closure over antibiotics (“all put in closed wound”), systemic antibiotics, platelet rich plasma in wound but not using advancement or rotation flap techniques |
| Primary asym. closure | S-shape closure, D-shape closure, D-flap, oblique crossing, Casten and modified Casten approach |
| Karydakis/Bascom* | Bascom cleft lift*, and modified Bascom cleft lift* approach, Karydakis and modified Karydakis approach, cleft lift procedure, including supplemental measures such as laser, phenol, cryotherapy, local antibiotics, drainage, wound closure over antibiotics (“all put in closed wound”), systemic antibiotics, platelet rich plasma in wound |
| Limberg/Dufourmentel | Limberg and Dufourmentel approach as well as their modifications, rhomboid flap, teardrop flap and z-plasty including supplemental measures such as local or systemic antibiotics |
| Flaps | Classical advancement flap, gluteus flap, VY-advancement flap, lateral advancement flap, local fasciocutaneous, infragluteal, and bilateral gluteus muscle advancement flap, “lembo di lalor”, pope musculofascial advancement flap, “Kopp gluteo-fascial plasty”, Rotation flap, Schrudde-Olivari and other flaps including combinations and supplemental measures such as local or systemic antibiotics |
| Marsupialisation | Marsupialisation as described by Obeid, McFee, Mutschmann, DePrizio, Colp and Buie |
| Limited excision | Lay open, curettage, drainage, sinotomy, sinotomy and cauterisation, “cystostomie”, minor excision, curettage, deroofing and curettage, cauterisation, and flush as described by Dorton |
| Pit picking* | Bascom pit picking with a lateral incision *, Trephines, pit picking, pit excision, pit excision and phenol, brushing, Farrell drills,Lord-Millar, primary open approach with subcutaneous excision of collateral tracts, tract coagulation |
| Partial closure | Partial closure techniques including supplemental measures such as local or systemic antibiotics |
| Incision and drainage | Incision, incision and curettage, and aspiration including supplemental measures such as, local or systemic antibiotics |
| Phenol treatment | Classic phenol treatment and supplemental measures such as laser, cryotherapy, and local or systemic antibiotics |
| Laser treatment | Primary laser techniques |
| Other treatments additionally included in the overall analysis | Plug and Seton technique, as well as endoscopic approaches, cryotherapy, histoacryl glue injection, aspiration and antibiotics, and conservative approaches such as Ayurveda therapy |
*Bascom described and used two different procedures: “Cleft closure/cleft lift” (merged with Karydakis group) and “Pit picking” (merged with Pit picking group).
Results
Our search criteria retrieved 5,840 studies and 303 book chapters across all databases. After excluding duplicates, 5,768 studies were screened. Reports on PSD in other than the classical presacral intergluteal location, studies in embryonic development, in carcinomas, etc. were excluded. Following exclusion, 1,148 articles on PSD at classical anatomical location with specific surgical treatment remained for analysis. Of these, 408 lacked detailed data on recurrence or follow-up time or both. Finally, 740 studies published from 1833 to 2017 were analysed. A flow chart describing the selection of literature sources, based on the Preferred reporting items for systematic reviews and meta-analysis (PRISMA)8, is illustrated in Fig. 1.
Figure 1.

Flow diagram based on Preferred reporting items for systematic reviews and meta-analysis (PRISMA)8 illustrating the systematic search for evidence regarding recurrence and long term follow-up data associated with common surgical procedures in PSD.
Results reported in the final set of publications were stratified according to the specific surgical technique employed to avoid bias across studies. This approach led to 14 groups for analysis. Additionally, we included an overall analysis. For each of the specific therapeutic approaches, the data included the number of patients, the reported follow-up time, and the recurrence.
Heterogeneity analysis
Considering prospective/randomized control trials only, the heterogeneity analysis showed I2 < 5%, p > 0.2 (Cochrane’s Q-test) except for the Bascom/Karydakis (0–12 months, p < 0.001, I2 = 80.36%, df = 4), marsupialisation (0–12 months; p < 0.001, I2 = 97.84%, df = 3), and other flap techniques (0–12 months, p = 0.062, I2 = 64%, df = 2). Considering all studies, the heterogeneity analysis showed I2 < 5%, p > 0.2 (Cochrane’s Q-test) except for the primary asymmetric closure (0–12 months, p = 0.023, I2 = 61.54%, df = 5), marsupialisation (0–12 months, p < 0.001, I2 = 64.43%, df = 18), and pit picking (0–12 months, p < 0.001, I2 = 98.31%, df = 6).
The above described analysis ascertains that there is no statistical evidence of heterogeneity in our study group, except for primary asymmetric closure, marsupialisation and pit picking.
Follow-up time and recurrence over all surgical therapies
Data on recurrence and follow-up times in all surgical PSD treatments together pertaining to 11,700 patients were extracted from 102 RCTs2,5,9–110. A recurrence of 1.5% (95% CI 1.3–1.8%) was observed in patients at 12 months, 4.3% (95% CI 3.8–4.8%) at 24 months, and 20.3% (95% CI 17.8–22.9%) at 60 months.
Further, data on recurrence and follow-up times in all surgical PSD treatments together pertaining to primary open PSD treatment pertaining to a total of 89,583 patients were extracted from 638 additional non-RCTs4,62,111–746. Among these patients, a recurrence of 2.0% (95% CI 1.9–2.1%) was observed in patients at 12 months, 4.4% (95% CI 4.3–4.6%) at 24 months, 10.8% (95% CI 10.5–11.3%) at 60 months, 16.9% (95% CI 16.3–17.5%) at 120 months, and 60.4% (95% CI 47.1–37.8%) at 240 months (Fig. 4).
Figure 4.

Recurrence free outcome as a function of follow-up time irrespective of specific therapeutic procedure. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
To enable an entire picture, this overall analysis included data on recurrence and follow-up times pertaining to 184 patients treated for PSD by other methods (Table 1) extracted from 3 RCTs. Among these patients, a recurrence of 3.8% (95% CI 0.9–6.7%) was observed in patients at 12 months and 7.8% (95% CI 0.4–15.1%) at 24 months and follow-up times pertaining to 2,916 patients treated for PSD by other methods extracted from 40 additional non-RCTs. Among these patients, a recurrence of 2.9% (95% CI 2.2–3.7%) was observed in patients at 12 months, 6.7% (95% CI 5.4–8.0%) at 24 months, and 26.0% (95% CI 22.6–29.4%) at 60 months.
To provide a rational basis for selecting treatment approaches, we assessed possible associations between recurrence of PSD and specific therapeutic procedures in the manner of a classical meta-analysis of RCTs, and found that recurrence in common surgical procedures for PSD were dependent on follow-up time (Figure 2); additional data from non-RCTs were included and processed in the manner of a merged data analysis (Figure 3).
Figure 2.

Procedure specific recurrence rates in PSD [%]* derived from RCTs. *Data of homogeneous recurrence rates (I2 < 5%, p > 0.2) are printed in bold, heterogeneous data in italic numbers; **includes Bascom cleft lift; ***includes Bascom Pit Picking.
Figure 3.

Procedure specific recurrence rates in PSD [%]* overall derived from RCTs and non-RCTs. *Data of homogeneous recurrence rates (I2 < 5%, p > 0.2) are printed in bold, heterogeneous data in italic numbers; **includes Bascom cleft lift, ***includes Bascom Pit Picking.
Recurrence in primary open PSD treatment
Data on recurrence and follow-up times in primary open PSD treatment pertaining to 1,713 patients were extracted from 32 RCTs9–38,747,748. Among these patients, a recurrence of 1.0% (95% CI 0.5–1.6%) was observed in patients at 12 months, 3.2% (95% CI 2.2–4.2%) at 24 months, and 16.5% (95% CI 11.9–21.2%) at 60 months.
Further, data on recurrence and follow-up times in primary open PSD treatment pertaining to 10,166 patients were extracted from 128 additional non-RCTs4,39,40,111–234. Among these patients, a recurrence of 1.5% (95% CI 1.2–1.7%) was observed in patients at 12 months, 4.2% (95% CI 3.7–4.7%) at 24 months, 13.1% (95% CI 11.9–14.4%) at 60 months, and 19.9% (95% CI 17.9–21.9%) at 120 months (Fig. 5).
Figure 5.
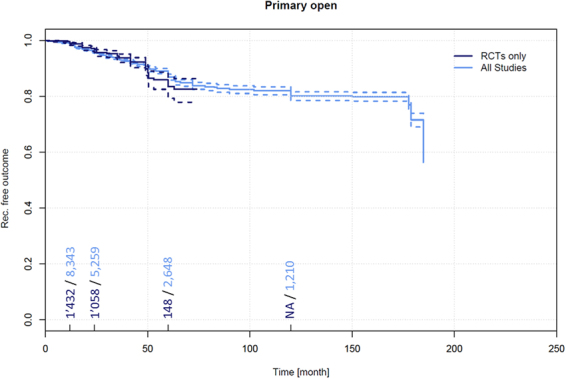
Recurrence free outcome as a function of follow-up time of patients receiving primary open treatment. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in primary midline closures
Data on recurrence and follow-up times in primary midline closures (not using advancement or rotation flap techniques) pertaining to 4,626 PSD patients which were extracted from 51 RCTs5,9,10,19,20,22,25–29,31,32,35,37,41–73,235,236,748. Among these patients, a recurrence of 2.1% (95% CI 1.7–2.6%) was observed in patients at 12 months, 7.0% (95% CI 6.0–8.0%) at 24 months, and 21.9% (95% CI 18.5–25.3%) at 60 months.
Data on recurrence and follow-up times in primary open PSD treatment pertaining to 21,583 patients were extracted from 205 additional non-RCTs4,60,74,75,111,112,114,115,117,118,121–126,128–134,136,137,141,143,149,153–156,160,161,163,167–171,174,175,177,181,182,188–192,194,196,197,199–201,203,206,208,215,216,218,220,221,223,224,230,233,237–373. Among these patients, a recurrence of 3.4% (95% CI 3.1–3.6%) was observed in patients at 12 months, 7.0% (95% CI 6.5–7.4%) at 24 months, 16.8% (95% CI 15.8–17.8%) at 60 months, 32.0% (95% CI 29.6–34.4%) at 120 months, and 67.9% (95% CI 53.3–82.4%) at 240 months (Fig. 6).
Figure 6.
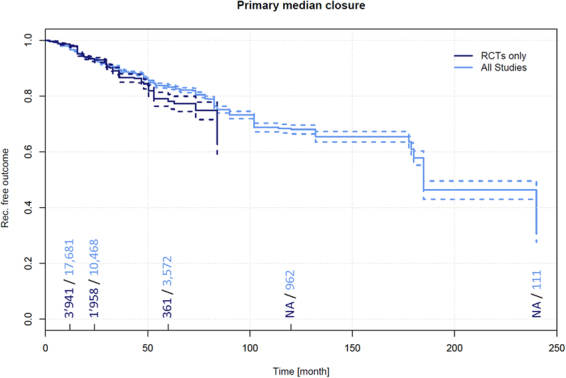
Recurrence free outcome as a function of follow-up time of patients treated with primary midline closure (not using advancement or rotation flap techniques). Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in primary asymmetric closure
Data on recurrence and follow-up times in primary asymmetric closure PSD treatment pertaining to 119 patients were extracted from 2 RCTs34,374. Among these patients, a recurrence of 7.3% (95% CI 0.0–19.9%) was observed in patients at 12 months.
Further, data on recurrence and follow-up times pertaining to 3,121 patients receiving primary open PSD treatment were extracted from 28 additional non-RCTs4,76,130,133,139,157,221,228,320,348,357,375–391. Among these patients, a recurrence of 1.0% (95% CI 0.6–1.4%) was observed in patients at 12 months, 1.6% (95% CI 1.1–2.1%) at 24 months, 3.2% (95% CI 2.3–4.0%) at 60 months, and 6.7% (95% CI 5.2–8.2%) at 120 months (Fig. 7).
Figure 7.
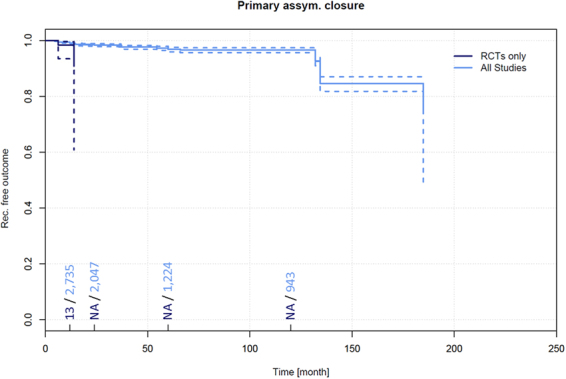
Recurrence free outcome as a function of follow-up time of patients treated with primary asymmetric closure. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in Karydakis and Bascom cleft lift techniques
Data on recurrence and follow-up times pertaining to 1,457 patients treated for PSD by a Karydakis or Bascom cleft lift technique were extracted from 21 RCTs24,33,59,62,63,77–90,392,393. Among these patients, a recurrence of 1.5% (95% CI 0.8–2.2%) was observed in patients at 12 months, 2.4% (95% CI 1.4–3.3%) at 24 months, and 10.2% (95% CI 5.4–15.0%) at 60 months.
Data on recurrence and follow-up times pertaining to 16,349 patients treated for PSD by a Karydakis and Bascom cleft lift technique were extracted from 66 additional non-RCTs91,92,136,146,161,163,184,198,206,254,263,313,335,346,348,361,379,391,394–441. Among these patients, a recurrence of 0.2% (95% CI 0.1–0.3%) was observed in patients at 12 months, 0.6% (95% CI 0.5–0.8%) at 24 months, 1.9% (95% CI 1.6–2.2%) at 60 months, and 2.7% (95% CI 2.4–3.1%) at 120 months (Fig. 8). Along with the Limberg/Dufourmentel approaches and other flap techniques, the Karydakis and Bascom cleft lift procedures resulted in the lowest recurrence at any follow-up time in our analysis (Tables 2 and 3).
Figure 8.
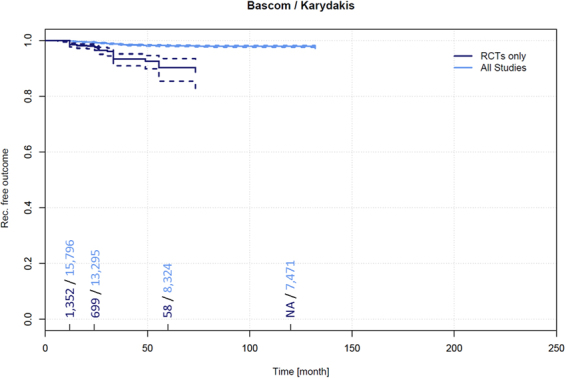
Recurrence free outcome as a function of follow-up time of patients treated with Bascom and Karydakis techniques. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in Limberg and Dufourmentel flaps
Data on recurrence and follow-up times pertaining to 2,380 patients treated for PSD by Limberg and Dufourmentel flap techniques were extracted from 36 RCTs5,14,21,23,43,44,46,49,53,54,56,61,64,65,73,77,78,80,82,83,90,93–102,236,392,393,442,443. Among these patients, a recurrence of 0.6% (95% CI 0.3–0.9%) was observed in patients at 12 months and 1.8% (95% CI 1.1–2.4%) at 24 months.
Data on recurrence and follow-up times pertaining to 12,384 patients treated for PSD by Limberg and Dufourmentel flaps were extracted from 139 additional non-RCTs4,60,103,104,115,126–128,133,156,157,196,199,201,208,221,224,242,261,262,267,289,302,303,313,318,321,322,334–336,348,372,399,407,410,415,417,426,433,438,439,444–541. Among these patients, a recurrence of 0.4% (95% CI 0.3–0.5%) was observed in patients at 12 months, 1.6% (95% CI 1.3–1.9%) at 24 months, 5.2% (95% CI 4.5–5.8%) at 60 months, and 11.4% (95% CI 9.2–13.7%) at 120 months (Fig. 9).
Figure 9.
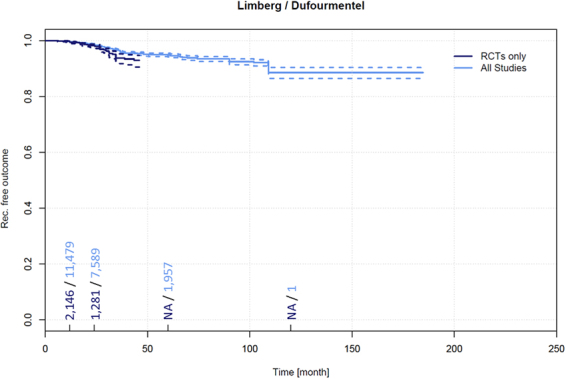
Recurrence free outcome as a function of follow-up time of patients treated with Limberg and Dufourmentel flap technique. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in other flap techniques
Data on recurrence and follow-up times pertaining to 283 patients treated for PSD by other flap techniques were extracted from 6 RCTs45,55,98,105,542,543. Among these patients, a recurrence of 0.4% (95% CI 0.0–1.1%) was observed in patients at 12 months and 7.5% (95% CI 2.4–12.5%) at 24 months.
Data on recurrence and follow-up times pertaining to 4,258 patients treated for PSD by other flap techniques were extracted from 89 additional non-RCTs106,107,111,126,137,160,167,182,192,208,221,224,233,245,259,283,312,321,339,354,368,410,433,449,492,511,512,525,532,538,544–602. Among these patients, a recurrence of 1.1% (95% CI 0.8–1.4%) was observed in patients at 12 months, 1.9% (95% CI 1.4–2.4%) at 24 months, and 7.9% (95% CI 6.4–9.4%) at 60 months (Fig. 10).
Figure 10.
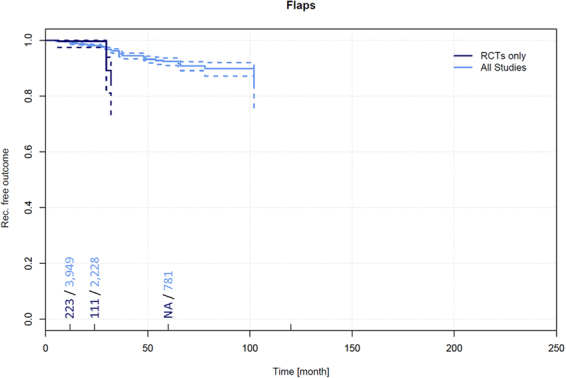
Recurrence free outcome as a function of follow-up time of patients treated with other flap techniques. Data presented are for RCTs only and for all available studies. Numbers of patients included in the analysis are indicated at 12, 24, 60, and 120 months. Dashed lines indicate 95% confidence intervals.
Recurrence in marsupialisation
Data on recurrence and follow-up times pertaining to 343 patients treated for PSD by marsupialisation were extracted from 8 RCTs17,18,30,47,96,101,603,604. Among these patients, a recurrence of 1.0% (95% CI 0.0–2.3%) was observed in patients at 12 months and 14.3% (95% CI 0.0–30.3%) at 24 months.
Data on recurrence and follow-up times pertaining to 3,207 patients treated for PSD by other flap techniques were extracted from 55 additional non-RCTs4,108,109,115,129,132,133,137,143,163,170,171,177,188,190,193,200,204,215,218,224,230,245,272,279,294,303,313,315,317,318,336,352,358,363,369,593,605–622. Among these patients, a recurrence of 1.8% (95% CI 1.2–2.3%) was observed in patients at 12 months, 5.6% (95% CI 4.5–6.7%) at 24 months, 9.4% (95% CI 7.6–11.1%) at 60 months, and 16.3% (95% CI 11.8–20.9%) at 120 months (Supplementary Fig. 1).
Recurrence in limited excision
Data on recurrence and follow-up times pertaining to 384 patients treated for PSD by limited excision were extracted from 5 RCTs29,50,105,604,623. Among these patients, a recurrence of 1.3% (95% CI 0.0–2.9%) was observed in patients at 12 months and 1.7% (95% CI 0.0–3.5%) at 24 months.
Data on recurrence and follow-up times pertaining to 6,366 patients treated for PSD by limited excision PSD treatment were extracted from 71 additional non-RCTs52,61,69,72,73,75,81,83,88,94,106,114,119,121,124,125,131,140,142,144,149,160,208,221,226,248,249,261,285,293,295,319,321,322,400,410,416,536,609,625–656. Among these patients, a recurrence of 5.0% (95% CI 4.3–5.6%) was observed in patients at 12 months, 6.8% (95% CI 6.0–7.7%) at 24 months, 16.2% (95% CI 14.3–18.2%) at 60 months, and 34.0% (95% CI 26.3–41.6%) at 120 months (Supplementary Fig. 2).
Recurrence in pit picking
Data on recurrence and follow-up times pertaining to 98 patients treated for PSD by pit picking were extracted from 2 RCTs85,86. Among these patients, a recurrence of 4.3% (95% CI 0.0–8.7%) was observed in patients at 12 months and 8.3% (95% CI 0.0–17.0%) at 24 months.
Data on recurrence and follow-up times pertaining to 6,272 patients treated for PSD by pit picking were extracted from 32 additional non-RCTs179,329,354,410,412,483,655–680. Among these patients, a recurrence of 2.7% (95% CI 2.2–3.1%) was observed in patients at 12 months, 6.5% (95% CI 5.7–7.3%) at 24 months, and 15.6% (95% CI 13.8–17.4%) at 60 months (Supplementary Fig. 3).
Recurrence in partial closure
Data on recurrence and follow-up times pertaining to 73 patients treated for PSD by partial closure were extracted from 1 RCT48. Due to the single observation, meta-analysis based on RCTs was not possible.
Data on recurrence and follow-up times pertaining to 530 patients treated for PSD by partial closure were extracted from 11 additional non-RCTs118,124,125,155,167,168,182,315,681–683. Among these patients, a recurrence of 2.8% (95% CI 1.2–4.4%) was observed in patients at 12 months, 5.1% (95% CI 2.8–7.3%) at 24 months, and 19.0% (95% CI 12.7–25.4%) at 60 months (Supplementary Fig. 4).
Recurrence in incision and drainage
No RCTs are available that report recurrence and follow-up times for incision and drainage.
Data on recurrence and follow-up times pertaining to 360 patients treated for PSD by incision and drainage were extracted from 13 non-RCTs118,162,177,179,197,199,206,254,264,378,684–686. Among these patients, a recurrence of 10.4% (95% CI 6.6–14.3%) was observed in patients at 12 months, 25.9% (95% CI 19.1–32.8%) at 24 months, and 40.2% (95% CI 29.4–50.9%) at 60 months (Supplementary Fig. 5).
Recurrence in phenol treatment alone
Data on recurrence and follow-up times pertaining to 70 patients treated for PSD by phenol alone were extracted from 1 RCT12. Due to the single observation, meta-analysis was not possible.
Data on recurrence and follow-up times pertaining to 1,947 patients treated for PSD by phenol alone were extracted from 26 additional non-RCTs194,219,338,355,445,457,687–706. Among these patients, a recurrence of 1.9% (95% CI 1.1–2.6%) was observed in patients at 12 months, 14.1% (95% CI 11.8–16.5%) at 24 months, and 40.4% (95% CI 27.8–52.9%) at 60 months (Supplementary Fig. 6).
Recurrence in laser alone
No RCTs are available that report recurrence and follow-up times for PSD treatment by laser alone.
Data on recurrence and follow-up times pertaining to 125 patients treated for PSD by incision and drainage were extracted 14 non-RCTs175,707–719. Among these patients, a recurrence of 1.9% (95% CI 0.0–4.7%) was observed in patients at 12 months, 5.1% (95% CI 0.4–9.8%) at 24 months, and 36.6% (95% CI 3.8–69.4%) at 60 months (Supplementary Fig. 7).
Comparing recurrence at 60 month following surgery amongst the RCT studies (11,730 patients, Figure 2, column “60”), range was 10.2%–21.9%; separated by a factor of 2.1. In all studies (Figure 3), range was from 1.9% to 40.4% at 60 months, giving a factor of 40.4/1.9 = 21. Thus, recurrence results differ by a factor of 2.1 in RCTs and by a factor of 21 in all studies through selection of a surgical therapy (when a given 5 year follow up is applied).
On the other hand, recurrence varies with time since surgery. In RCT primary open results (as shown in Figure 2), line primary open treatment, recurrence is 1.0% at 12 months and increases to 16.5% at 60 months. Recurrence varies by a factor of 16,5/1 through time in this primary open group, while this is lower in the Karydakis & Bascom group (10,2/1,5; 6,8).
In the 89,583 patients group combining RCT and non-RCT data, the quotient between longest and shortest recurrence result can be found in the Limberg & Dufourmentel group, with 0.4% at 12 months and 11.4% at 120 months following surgery (factor 28,5). Thus, recurrence results may differ by a factor of 6, 8 and more for a given surgical therapy if follow up time is not properly defined (or defined at all). This indicates that a thorough evaluation of a procedure in view of recurrence has to include the specific relation of recurrence to follow-up time.
Discussion
We have reviewed all pilonidal sinus treatment data from all available cases from the first published description of pilonidal sinus in 1833 to the present day. We have analysed data from more than 80,000 patients surgically treated for a single disease over the past 180 years, and have systematically assessed the relationship between recurrence, follow-up times, and surgical procedure. Our meta-analysis of the data identified a relationship between recurrence of PSD and follow-up times for each different therapeutic approach. The mean recurrence for all cases measured at the one-year time point differed from the five-year recurrence by a factor of 5; whereas, for the individual therapeutic procedures, one and five-year recurrence differed by a factor of 3 to 20 (Tables 2 and 3).
Recurrence varies between surgical procedures by a factor of 2,1 at 60 months in RCTs and 21 in all studies. On the other hand, recurrence varies by a factor of 19 to 29 within a given surgical therapy if comparing 12 months and longest follow up results (Tables 2 and 3). Thus, any report of a given surgical procedure without specified follow up may contain a10 fold higher or lower true recurrence as the postulated one.
Our study has several limitations that we identify as follows: The systematic review and meta-analysis was limited to reports in English, French, German, Italian, and Spanish. Publications in other languages were included where definitive treatment and recurrence at specific follow-up times were described in an English abstract. Consequently, Japanese and Chinese literature is not fully included. On the other hand, pilonidal sinus is exceptionally rare in the Asian population745, therefore, we do not anticipate an emergence of Asian data that would significantly skew the current results. Further, our strategy of including all available evidence since January 1st, 1833 ensured a broad picture. Although additional older literature may be found and studied, such literature is unlikely to add significantly to the findings reported here, as regular follow-up was not commonplace in early times; surgeons relied more on “return on recurrence” follow-up746,749. Furthermore, the older literature includes more primary open treatment methods with follow-up exceeding 120 months166,750, which are well-represented in the analysis. Therefore, the inclusion of additional new primary open patients is unlikely to change our findings. Given the design, the scope of this study is relatively narrow and specific. Yet, including more variables such as e.g. length of hospital stay, length of post-op course, and cost of post-op course would be a very extensive beyond the scope of a single study. Another source of bias may be our strategy for grouping therapeutic procedures. We had to condense multiple, sometimes minute, variants of mainstream surgical therapies into cohorts large enough for thorough analysis. While some therapies are gone, and will not return, others, such as marsupialisation, seem to be enjoying a resurgence, and new strategies such as endoscopic approaches are currently being investigated. Additionally, studies were picked regardless of their inclusion of primary or recurrent PSD cases what may affect the surgical technique of choice and the outcome in many ways. Statistical limitations are built into the design of this study. While detailed information about a single patient is commonly not available, it was necessary to simulate single patients from pools of patients reported in each single study. Therefore, no sub-analysis of links between recurrence and follow-up time for gender or age groups, etc., could be applied. Since the analysed studies reported follow-up times with various statistical measures (mean, median, and range), there could be a potential bias within the details in the survival curve structures. Abrupt drops, for example, are often due to studies in which large numbers of patients experienced recurrence at a specific (mean/median/centre of range) follow-up time. Therefore, the specific drops in the survival curves should be interpreted cautiously. For the purpose of this study, the goal was to acquire an understanding of general links between follow-up times and recurrence among therapeutic procedures. Although we cannot necessarily determine, by extrapolation from our results, a particular follow-up time at which recurrence increases, the trend over time is meaningful, and thanks to the very high case numbers, is reliably estimated.
The highest incidence of recurrence identified in our data, 67.9%, occurred 240 months after primary midline closures; so, this method should be abandoned straight away, while other traditional approaches such as primary open treatment can be justified, also when considering the development of more complicated surgeries involving flap techniques. Correctly, this leads to a call for more off-midline closure education for surgeons751. From our analysis of data from more than 80,000 patients over 18 decades, we found that the Karydakis and the Bascom cleft lift procedures show the lowest recurrence at any time of follow-up, followed by rhomboid flaps and other flaps. However, current RCT evidence only provides follow-up data for 10 years postoperatively for Karydakis/Bascom, and a longer-term study would be of interest. Nevertheless, non-RCT data point into the direction of a continued low recurrence with these advancement and rotational flap methods. Because of the high recurrence as early as 2 years (25.9%, rising to 40.2 after 5 years), incision and drainage cannot be recommended as definite therapy. The simple manoeuvre easily relieves a patient from pain in an acute situation, but must be followed by a definite technique with lower recurrence. Similarly, phenol treatment is associated with high recurrence, 14.1% at 24 months and 40.4% at 60 months; longer term follow-up data are unavailable. A Turkish group has reported on the phenol technique recently457. They praise its minimal invasiveness and concomitant short duration of stay in hospital. However, given the high recurrence, these might be misleading arguments. The data on laser treatment still remain weak; long term follow-up data and extensive cohorts have not yet been published.
Our results presented here suggest that the variances in recurrence are understandable once the follow-up time is taken into account. We found that recurrence is a function of follow-up time for every major surgical and non-surgical method analysed. Our endeavours here have established a respective benchmark, potentially increasing the comparability as also proposed, e.g., for a staging system410.
In conclusion, physicians must keep in mind that recurrence of surgical procedures in PSD impressively depend on follow-up time. This dependence, i.e. the steepness of increase of recurrence with longer follow-up times, is specific to a surgical procedure. Applying a recurrence without knowing the time since surgery may be open to a bias factor of up to 18 and above. The choice of surgical therapy influences recurrence by a factor of up to 21. As we are now able to understand recurrence in PSD in a more standardised way. Primary midline closure is dead, while older therapies (such as marsupialisation) may be reconsidered, while advancement flap (Karydakis & Bascom) and rotational flap procedures (Limberg/Dufourmentel) are undoubtedly primary league with asymmetrical procedures, as proven by RCT and combined RCT/non-RCT analysis in 89,583 patients available from 1833 to 2017. Follow-up of PSD patients should always be planned long term, i.e., five or ten years if reliable conclusions are to be drawn regarding the efficacy of a new procedure or on the efficacy of your own results using an already known technique.
Methods
Ethical approval and informed consent
The systematic review with meta-analysis and merged data analysis included no experiment carried out on live vertebrates (or higher invertebrates), humans or human samples. Thus, formal ethics approval was not required.
Search strategy and study selection criteria
To assemble a comprehensive database pertaining to PSD, we systematically searched for the NCBI Medical Subject Heading (MeSH) term, “pilonid*“, as well as “dermoid” AND “cyst” in MEDLINE, PubMed, PubMed Central, Scopus, Ovid, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL). We additionally searched these terms in Google, Google Scholar, ResearchGate, and references listed in national and international guidelines such as the S3 guidelines of the Association of the Scientific Medical Societies in Germany on the treatment of PSD. We also assessed the references listed in the literature cited of all documents retrieved by the searches. Documents retrieved included randomised, non-randomised, prospective, retrospective, and observational studies such as cohort, case-control, cross-sectional studies, and case reports published between 1833 to 2017. Four authors (VS, MML, MD, and DD) reviewed the retrieved documents for compliance with the inclusion criteria: specification of the definitive treatment, recurrence, and length of follow-up. Reports in English, French, German, Italian, and Spanish were considered, as were publications in other languages if definitive treatment and recurrence at specific follow-up times were described in an English abstract, or if the authors contacted via email or Research Gate provided an English translation of their surgical approach, recurrence, and follow-up time. Exclusion criteria were: PSD in other than presacral location, neoplasia involvement, double publication of data by an author. Further, studies lacking any component of the minimal data set which comprised of: definitive treatment strategy/recurrence/follow-up time were excluded. Prior meta-analysis reports and review articles were excluded, as well, although their reference lists were screened for potential additions to the evidence. Also, previously unpublished data presented in review articles were taken into account. Studies in which recurrence were deduced from patients returning with recurrent disease (“return on recurrence”), but which did not actively investigate the majority of non-returners, were excluded.
The review protocol is registered in the National Health Service (NHS) international prospective register of systematic reviews PROSPERO (42016051588).
Data collection, extraction and quality assessment
All studies were analysed and documented on paper. The transcript data were collected into a Microsoft Excel (Version 2016, Microsoft Corp., Redmond, WA) spreadsheet, and correct transfer was controlled. Every specific therapeutic strategy reported in a paper was assigned to a line. Columns included citation details, number of patients included, therapeutic procedures, reported follow-up times, study details and recurrence.
The statistical measures applied for reporting of follow-up times are not standardised, and thus, were not identical among different studies. However, given the relative clustering of the disease incidence in young adults, mean and median reports were treated as equivalent. For data that included a range of follow-up times, the centre of the given range was used in our analysis. For data in which minimum follow-up times were reported, the values were integrated as is.
Individual studies were assessed for consistency in described methods and reported results to minimize potential risk of bias in a thorough data synthesis. A subgroup of prospective randomized control trials was analysed separately in addition to check for consistency with the complete set of studies. The reported recurrence in each study were then linked to the study’s follow-up time. Follow-up time was defined as mean, median, centre of range, or minimum. To compare information across all studies, single patients were statistically simulated. I.e., for each study participant, a data sample was extracted containing recurrence, follow-up time, and therapeutic procedure. If, for example, a study included 500 patients and a recurrence of 20% for a particular therapeutic procedure, then 100 single samples would be defined as recurrent disease, whereas, the remaining 400 samples would be defined as recurrence-free. In this simulation, some information, such as gender ratios, could not be included since this information was only available cumulatively in the majority of studies.
In cases where an article addressed more than one therapeutic strategy, the data pertaining to each treatment strategy were considered separately in our analysis.
Grouping of therapeutic procedures and statistical analyses
Therapeutic procedures were analysed cumulatively (“overall”) and stratified as subgroups (Table 1). The overall analysis also included some other different techniques not specifically analysed as subgroup. For statistical analysis and visualizations, the statistical software package R (version 3.1.0) in the R-studio framework (version 0.98.982) was used. Statistical significance was assumed if p < 0.05. All tests were considered in a two-tailed set-up. For the analysis of recurrence free outcome over time, survival analysis according to Kaplan-Meier including pointwise 95% confidence intervals (CI) was used as implemented in the R-package ‘survival’ (version 2.40-1). These analyses were performed for each defined therapeutic procedure. Results were plotted as percent of recurrence-free outcomes with their 95% CI. In order to comprehend the data leading to the Kaplan-Meier curves, the numbers of patients included in the intervals of 0-12, 12-24, 24-60, 60-120, and > 120 months are included on the horizontal axes of the plots. If no specific data were available for an interval, linear interpolation of recurrence free outcome according to the two nearest observed follow-up times was used. To provide a comprehensive study on recurrence and a rational basis for selecting treatment procedures, we assessed data in the manner of a classical meta-analysis of RCTs, and further employed an analysis that included non-RCTs in the manner of a merged data analysis. Because the Kaplan-Meier curves were calculated as stepwise functions, small discrepancies between the plotted and the tabled values may occur.
Potential heterogeneity of the study outcomes was assessed through Cochrane analysis and I2 calculation as described previously752,753. Therefore, the articles were grouped according to procedures and follow-up time-intervals as applied for plotting the Kaplan-Meier curves. A separate analysis was conducted for studies based on randomized controlled trials (RCTs) and for the complete set of studies considered (RCTs and non-RCTs). The data used for computing Cochrane’s Qs were computed with the recurrence as reported in the corresponding studies, weighted with the respective numbers of study participants. For assessing significance of heterogeneity, a Chi2 test was employed. I2 was computed to complete the results of the Chi2 test.
Data Availability Statement
All data and calculations are available to readers upon request to the corresponding author.
Ethics
This article does not contain any studies with human participants, human samples or live vertebrates. Therefore, no informed consent had to be obtained prior to preparation of current manuscript.
Electronic supplementary material
Acknowledgements
The authors thank Dr. Eric Milner (Biomedical Science Writers, LLC www.biomedicalsciencewriters.com) for language editing the manuscript.
Author Contributions
V.S., M.M.L., M.D., K.W., D.D. acquired the data. V.S., M.M.L., P.K., M.S., D.D. performed statistical analysis and calculations. V.S., M.M.L., P.K., M.S., M.D., K.W., B.S., D.D. interpreted the data and edited the manuscript. V.S., M.M.L., P.K., B.S., D.D. wrote the manuscript. V.S., M.M.L., P.K., M.S., D.D. designed the graphics.
Competing Interests
The authors declare no competing interests.
Footnotes
Electronic supplementary material
Supplementary information accompanies this paper at 10.1038/s41598-018-20143-4.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Allen-Mersh TG. Pilonidal sinus: finding the right track for treatment. Br J Surg. 1990;77:123–132. doi: 10.1002/bjs.1800770203. [DOI] [PubMed] [Google Scholar]
- 2.Evers T, et al. Trends in incidence and long-term recurrence rate of pilonidal sinus disease and analysis of associated influencing factors. Zhonghua Wai Ke Za Zhi. 2011;49:799–803. [PubMed] [Google Scholar]
- 3.Luedi MM, Kauf P, Evers T, Sievert H, Doll D. Impact of spinal versus general anesthesia on postoperative pain and long term recurrence after surgery for pilonidal disease. Journal of clinical anesthesia. 2016;33:236–242. doi: 10.1016/j.jclinane.2016.03.061. [DOI] [PubMed] [Google Scholar]
- 4.Doll D, Luedi MM, Evers T, Kauf P, Matevossian E. Recurrence-free survival, but not surgical therapy per se, determines 583 patients’ long-term satisfaction following primary pilonidal sinus surgery. Int J Colorectal Dis. 2015;30:605–611. doi: 10.1007/s00384-015-2130-0. [DOI] [PubMed] [Google Scholar]
- 5.Akca T, Colak T, Ustunsoy B, Kanik A, Aydin S. Randomized clinical trial comparing primary closure with the Limberg flap in the treatment of primary sacrococcygeal pilonidal disease. Br J Surg. 2005;92:1081–1084. doi: 10.1002/bjs.5074. [DOI] [PubMed] [Google Scholar]
- 6.Clothier PR, Haywood IR. The natural history of the post anal (pilonidal) sinus. Ann R Coll Surg Engl. 1984;66:201–203. [PMC free article] [PubMed] [Google Scholar]
- 7.Sievert H, et al. The influence of lifestyle (smoking and body mass index) on wound healing and long-term recurrence rate in 534 primary pilonidal sinus patients. Int J Colorectal Dis. 2013;28:1555–1562. doi: 10.1007/s00384-013-1731-8. [DOI] [PubMed] [Google Scholar]
- 8.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS medicine. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Al-Hassan HKF, Neglén IM. P. Primary closure or secondary granulation after excision of pilonidal sinus. Acta Chir Scand. 1990;156:695–699. [PubMed] [Google Scholar]
- 10.Al-Salamah SM, Hussain MI, Mirza SM. Excision with or without primary closure for pilonidal sinus disease. J Pak Med Assoc. 2007;57:388–391. [PubMed] [Google Scholar]
- 11.Biter LU, et al. The use of negative-pressure wound therapy in pilonidal sinus disease: a randomized controlled trial comparing negative-pressure wound therapy versus standard open wound care after surgical excision. Dis Colon Rectum. 2014;57:1406–1411. doi: 10.1097/DCR.0000000000000240. [DOI] [PubMed] [Google Scholar]
- 12.Calikoglu I, et al. Phenol Injection Versus Excision With Open Healing in Pilonidal Disease: A Prospective Randomized Trial. Dis Colon Rectum. 2017;60:161–169. doi: 10.1097/DCR.0000000000000717. [DOI] [PubMed] [Google Scholar]
- 13.Duxbury MS, Blake SM, Dashfield A, Lambert AW. A randomised trial of knife versus diathermy in pilonidal disease. Ann R Coll Surg Engl. 2003;85:405–407. doi: 10.1308/003588403322520799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fazeli MS, Adel MG, Lebaschi AH. Comparison of outcomes in Z-plasty and delayed healing by secondary intention of the wound after excision of the sacral pilonidal sinus: results of a randomized, clinical trial. Dis Colon Rectum. 2006;49:1831–1836. doi: 10.1007/s10350-006-0726-8. [DOI] [PubMed] [Google Scholar]
- 15.Ghnnam WM, Hafez DM. Laser hair removal as adjunct to surgery for pilonidal sinus: our initial experience. J Cutan Aesthet Surg. 2011;4:192–195. doi: 10.4103/0974-2077.91251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gupta PJ. Comparative study between radiofrequency sinus excision and open excision in sacro-coccygeal pilonidal sinus disease. Dig Surg. 2005;22:459–463. doi: 10.1159/000092034. [DOI] [PubMed] [Google Scholar]
- 17.Gupta PJ. Radiofrequency sinus excision: better alternative to marsupialization technique in sacrococcygeal pilonidal sinus disease. J Natl Med Assoc. 2005;97:998–1002. [PMC free article] [PubMed] [Google Scholar]
- 18.Gupta P. A comparison of two operations for pilonidal sinus disease. Nig J Surg Res. 2004;6:41–45. [Google Scholar]
- 19.Holzer B, et al. Efficacy and tolerance of a new gentamicin collagen fleece (Septocoll) after surgical treatment of a pilonidal sinus. Colorectal Dis. 2003;5:222–227. doi: 10.1046/j.1463-1318.2003.00471.x. [DOI] [PubMed] [Google Scholar]
- 20.Hosseini SV, et al. The comparison between drainage, delayed excision and primary closure with excision and secondary healing in management of pilonidal abscess. Int J Surg. 2006;4:228–231. doi: 10.1016/j.ijsu.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 21.Jamal A, Shamim M, Hashmi F, Qureshi MI. Open excision with secondary healing versus rhomboid excision with Limberg transposition flap in the management of sacrococcygeal pilonidal disease. J Pak Med Assoc. 2009;59:157–160. [PubMed] [Google Scholar]
- 22.Kareem TS. Surgical treatment of chronic sacrococcygeal pilonidal sinus. Open method versus primary closure. Saudi Med J. 2006;27:1534–1537. [PubMed] [Google Scholar]
- 23.Kaser SA, Zengaffinen R, Uhlmann M, Glaser C, Maurer CA. Primary wound closure with a Limberg flap vs. secondary wound healing after excision of a pilonidal sinus: a multicentre randomised controlled study. Int J Colorectal Dis. 2015;30:97–103. doi: 10.1007/s00384-014-2057-x. [DOI] [PubMed] [Google Scholar]
- 24.Keshvari A, et al. Karydakis flap versus excision-only technique in pilonidal disease. J Surg Res. 2015;198:260–266. doi: 10.1016/j.jss.2015.05.039. [DOI] [PubMed] [Google Scholar]
- 25.Khatoon S, et al. Pilonidal sinus: Excision with primary midline closure versus open method. J. Liaquat Univ. Med. Health Sci. 2010;9:9–11. [Google Scholar]
- 26.Khawaja HT, Bryan S, Weaver PC. Treatment of natal cleft sinus: a prospective clinical and economic evaluation. BMJ (Clinical research ed.) 1992;304:1282–1283. doi: 10.1136/bmj.304.6837.1282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kronborg O, Christensen K, Zimmermann-Nielsen C. Chronic pilonidal disease: a randomized trial with a complete 3-year follow-up. Br J Surg. 1985;72:303–304. doi: 10.1002/bjs.1800720418. [DOI] [PubMed] [Google Scholar]
- 28.Lundhus E, Gottrup F. Outcome at three to five years of primary closure of perianal and pilonidal abscess. A randomised, double-blind clinical trial with a complete three-year followup of one compared with four days’ treatment with ampicillin and metronidazole. Eur J Surg. 1993;159:555–558. [PubMed] [Google Scholar]
- 29.Mohamed HA, Kadry I, Adly S. Comparison between three therapeutic modalities for non-complicated pilonidal sinus disease. Surgeon. 2005;3:73–77. doi: 10.1016/S1479-666X(05)80065-4. [DOI] [PubMed] [Google Scholar]
- 30.Ortiz Hurtado H, Marti Rague J, Sitges Creus A. Pilonidal sinus. Comparison of 3 surgical techniques. Cir. Esp. 1977;31:413–418. [Google Scholar]
- 31.Rao MM, Zawislak W, Kennedy R, Gilliland R. A prospective randomised study comparing two treatment modalities for chronic pilonidal sinus with a 5-year follow-up. Int J Colorectal Dis. 2010;25:395–400. doi: 10.1007/s00384-009-0804-1. [DOI] [PubMed] [Google Scholar]
- 32.Shah STA, Tahir M, Nasir M, Paracha SA, Wahab K. Outcome of open versus closed surgical technique for treatment of chronic pilonidal sinus: a randomized controlled trial. Khyber Med Univ J. 2013;5:146–151. [Google Scholar]
- 33.Shah A, Waheed A, Malik A. Recurrence rates in pilonidal sinus surgery: Comparison of two techniques (Karydakis Versus Conventional Open Excision) Pak. J. Med. Health Sci. 2009;3:91–95. [Google Scholar]
- 34.Sheikh, M. R., Malik, K. A. & Rehmann, S. Outcome of surgery for pilonidal sinus: Karydakis versus open procedure. Pak J Surg23 (2007).
- 35.Sondenaa K, Nesvik I, Andersen E, Soreide JA. Recurrent pilonidal sinus after excision with closed or open treatment: final result of a randomised trial. Eur.J Surg. 1996;162:237–240. [PubMed] [Google Scholar]
- 36.Spyridakis M, Christodoulidis G, Chatzitheofilou C, Symeonidis D, Tepetes K. The role of the platelet-rich plasma in accelerating the wound-healing process and recovery in patients being operated for pilonidal sinus disease: preliminary results. World J Surg. 2009;33:1764–1769. doi: 10.1007/s00268-009-0046-y. [DOI] [PubMed] [Google Scholar]
- 37.Testini M, et al. Treatment of chronic pilonidal sinus with local anaesthesia: a randomized trial of closed compared with open technique. Colorectal Dis. 2001;3:427–430. doi: 10.1046/j.1463-1318.2001.00278.x. [DOI] [PubMed] [Google Scholar]
- 38.Viciano V, et al. Effect of hydrocolloid dressings on healing by second intention after excision of pilonidal sinus. Eur.J Surg. 2000;166:229–232. doi: 10.1080/110241500750009339. [DOI] [PubMed] [Google Scholar]
- 39.Argov S, Golz A, Barzilai A. Single stage operation for pilonidal sinus. HAREFUAH. 1980;99:420–421. [PubMed] [Google Scholar]
- 40.Arnous J, Denis J, Dubois N. Treatment of pilonidal sinus by “en bloc excision”. Gastroenterol Clin Biol. 1977;1:945–949. [PubMed] [Google Scholar]
- 41.Andersson RE, Lukas G, Skullman S, Hugander A. Local administration of antibiotics by gentamicin-collagen sponge does not improve wound healing or reduce recurrence rate after pilonidal excision with primary suture: a prospective randomized controlled trial. World J Surg. 2010;34:3042–3048. doi: 10.1007/s00268-010-0763-2. [DOI] [PubMed] [Google Scholar]
- 42.Aysan E, Basak F, Kinaci E, Sevinc M. Efficacy of local adrenalin injection during sacrococcygeal pilonidal sinus excision. Eur Surg Res. 2004;36:256–258. doi: 10.1159/000078861. [DOI] [PubMed] [Google Scholar]
- 43.Dass TA, Zaz M, Rather A, Bari S. Elliptical excision with midline primary closure versus rhomboid excision with limberg flap reconstruction in sacrococcygeal pilonidal disease: a prospective, randomized study. Indian J Surg. 2012;74:305–308. doi: 10.1007/s12262-011-0400-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Galal Elshazly W, Said K. Clinical trial comparing excision and primary closure with modified Limberg flap in the treatment of uncomplicated sacrococcygeal pilonidal disease. Alexandria Journal of Medicine. 2012;48:13–18. doi: 10.1016/j.ajme.2011.10.002. [DOI] [Google Scholar]
- 45.Enshaei A, Motearefi S. Comparison of two surgical methods, primary closure and rotational flap, in patients with chronic pilonidal sinus. Glob J Health Sci. 2014;6:18–22. doi: 10.5539/gjhs.v6n7p18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ertan T, et al. Does technique alter quality of life after pilonidal sinus surgery? Am J Surg. 2005;190:388–392. doi: 10.1016/j.amjsurg.2004.08.068. [DOI] [PubMed] [Google Scholar]
- 47.Fuzun M, et al. Which technique for treatment of pilonidal sinus–open or closed? Dis Colon Rectum. 1994;37:1148–1150. doi: 10.1007/BF02049819. [DOI] [PubMed] [Google Scholar]
- 48.Gencosmanoglu R, Inceoglu R. Modified lay-open (incision, curettage, partial lateral wall excision and marsupialization) versus total excision with primary closure in the treatment of chronic sacrococcygeal pilonidal sinus: a prospective, randomized clinical trial with a complete two-year follow-up. Int J Colorectal Dis. 2005;20:415–422. doi: 10.1007/s00384-004-0710-5. [DOI] [PubMed] [Google Scholar]
- 49.Khan PS, Hayat H, Hayat G. Limberg flap versus primary closure in the treatment of primary sacrococcygeal pilonidal disease; a randomized clinical trial. Indian J Surg. 2013;75:192–194. doi: 10.1007/s12262-012-0430-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Lorant T, Ribbe I, Mahteme H, Gustafsson UM, Graf W. Sinus excision and primary closure versus laying open in pilonidal disease: a prospective randomized trial. Dis Colon Rectum. 2011;54:300–305. doi: 10.1007/DCR.0b013e31820246bf. [DOI] [PubMed] [Google Scholar]
- 51.Milone M, Musella M, Salvatore G, Leongito M, Milone F. Effectiveness of a drain in surgical treatment of sacrococcygeal pilonidal disease. Results of a randomized and controlled clinical trial on 803 consecutive patients. Int J Colorectal Dis. 2011;26:1601–1607. doi: 10.1007/s00384-011-1256-y. [DOI] [PubMed] [Google Scholar]
- 52.Milone M, et al. Intradermal absorbable sutures to close pilonidal sinus wounds: a safe closure method? Surg Today. 2014;44:1638–1642. doi: 10.1007/s00595-013-0741-z. [DOI] [PubMed] [Google Scholar]
- 53.Morrison PD. Is Z-plasty closure reasonable in pilonidal disease? Ir J Med Sci. 1985;154:110–112. doi: 10.1007/BF02937227. [DOI] [PubMed] [Google Scholar]
- 54.Muzi MG, et al. Randomized comparison of Limberg flap versus modified primary closure for the treatment of pilonidal disease. Am J Surg. 2010;200:9–14. doi: 10.1016/j.amjsurg.2009.05.036. [DOI] [PubMed] [Google Scholar]
- 55.Nursal TZ, et al. Prospective randomized controlled trial comparing V-Y advancement flap with primary suture methods in pilonidal disease. Am J Surg. 2010;199:170–177. doi: 10.1016/j.amjsurg.2008.12.030. [DOI] [PubMed] [Google Scholar]
- 56.Okus A, Sevinc B, Karahan O, Eryilmaz MA. Comparison of Limberg flap and tension-free primary closure during pilonidal sinus surgery. World J Surg. 2012;36:431–435. doi: 10.1007/s00268-011-1333-y. [DOI] [PubMed] [Google Scholar]
- 57.Othman I. Skin glue improves outcome after excision and primary closure of sacrococcygeal pilonidal disease. Indian J Surg. 2010;72:470–474. doi: 10.1007/s12262-010-0170-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Perepelitsa, G. F. & Dulinov, A. I. Use of lasers in the surgical treatment of suppurative pilonidal cysts. Klin Khir, 68 (1990). [PubMed]
- 59.Polat N, Albayrak D, Ibiş AC, Altan A. Comparison between karydakis flap repair and primary closure for surgical treatment of sacrococcygeal pilonidal sinus. Trakya Universitesi Tip Fakultesi Derg. 2008;25:87–94. [Google Scholar]
- 60.Pomazkin VI, Mansurov IV. Choice of operation for treatment of patients with pilonidal sinus. Vestn Khir Im I I Grek. 2008;167:85–87. [PubMed] [Google Scholar]
- 61.Roshdy H, Ali Y, Askar W, Awad I, Farid M. Rhomboid flap versus primary closure after excision of saccrococcigeal pilonidal sinus (a prospective randomized study) Egypt J Surg. 2010;29:146–152. [Google Scholar]
- 62.Sakr MF, Moussa M. A prospective controlled randomized trial comparing Karydakis technique and midline closure in patients with recurrent chronic pilonidal sinus. Surg. Chronicles. 2011;16:84–90. [Google Scholar]
- 63.Sakr M, Habib M, Shaheed AA. Assessment of Karydakis technique as compared with midline closure for the management of chronic pilonidal sinus. J. Pelvic Med. Surg. 2006;12:201–206. doi: 10.1097/01.spv.0000217399.78641.43. [DOI] [Google Scholar]
- 64.Sevinc, B. et al. Randomized prospective comparison of midline and off-midline closure techniques in pilonidal sinus surgery. Surgery159, 749–754, 10.1016/j.surg.2015.09.024 (2016). [DOI] [PubMed]
- 65.Shabbir F, et al. Modified Limberg’s flap versus primary closure for treatment of pilonidal sinus disease: a comparative study. J Pak Med Assoc. 2014;64:1270–1273. [PubMed] [Google Scholar]
- 66.Sondenaa K, et al. The role of cefoxitin prophylaxis in chronic pilonidal sinus treated with excision and primary suture. J Am Coll Surg. 1995;180:157–160. [PubMed] [Google Scholar]
- 67.Sondenaa K, et al. Influence of failure of primary wound healing on subsequent recurrence of pilonidal sinus. combined prospective study and randomised controlled trial. Eur.J Surg. 2002;168:614–618. doi: 10.1080/11024150201680007. [DOI] [PubMed] [Google Scholar]
- 68.Sondenaa K, Andersen E, Soreide JA. Morbidity and short term results in a randomised trial of open compared with closed treatment of chronic pilonidal sinus. Eur.J Surg. 1992;158:351–355. [PubMed] [Google Scholar]
- 69.Sondenaa K, Nesvik I, Andersen E, Natas O, Soreide JA. Bacteriology and complications of chronic pilonidal sinus treated with excision and primary suture. Int J Colorectal Dis. 1995;10:161–166. doi: 10.1007/BF00298540. [DOI] [PubMed] [Google Scholar]
- 70.Terzi C, Canda AE, Unek T, Dalgic E, Fuzun M. What is the role of mechanical bowel preparation in patients with pilonidal sinus undergoing surgery? Prospective, randomized, surgeon-blinded trial. World J Surg. 2005;29:1465–1471. doi: 10.1007/s00268-005-0007-z. [DOI] [PubMed] [Google Scholar]
- 71.Vogel P, Lenz J. Treatment of pilonidal sinus with excision and primary suture using a local, resorbable antibiotic carrier. Results of a prospective randomized study. Chirurg. 1992;63:748–753. [PubMed] [Google Scholar]
- 72.Yetim I, Ozkan OV, Dervisoglu A, Erzurumlu K, Canbolant E. Effect of gentamicin-absorbed collagen in wound healing in pilonidal sinus surgery: a prospective randomized study. J Int Med Res. 2010;38:1029–1033. doi: 10.1177/147323001003800329. [DOI] [PubMed] [Google Scholar]
- 73.Youssef TE-AS, Farid M. Tension-free primary closure compared with modified Limberg flap for pilonidal sinus disease: a prospective balanced randomized study. RR unglaublich niedrig bei 100% FUP. 2015;34:85–89. [Google Scholar]
- 74.Aaser P, Gruner OP. Pilonidal cysts. Excision and intracutaneous absorbable primary suture. Tidsskr Nor Laegeforen. 1992;112:206–207. [PubMed] [Google Scholar]
- 75.Abou-Zikry AS, Guindi A, Hashem M. Pilonidal sinus and cysts (sacro-coccygeal sinus); report of 22 cases treated by excision and primary suture. J Egypt Med Assoc. 1954;37:696–705. [PubMed] [Google Scholar]
- 76.Brusciano L, et al. D-shape asymmetric excision of sacrococcygeal pilonidal sinus with primary closure, suction drain, and subcuticular skin closure: an analysis of risks factors for long-term recurrence. Surg Innov. 2015;22:143–148. doi: 10.1177/1553350614535856. [DOI] [PubMed] [Google Scholar]
- 77.Bali I, et al. Effectiveness of Limberg and Karydakis flap in recurrent pilonidal sinus disease. Clinics (Sao Paulo) 2015;70:350–355. doi: 10.6061/clinics/2015(05)08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Bessa SS. Comparison of short-term results between the modified Karydakis flap and the modified Limberg flap in the management of pilonidal sinus disease: a randomized controlled study. Dis Colon Rectum. 2013;56:491–498. doi: 10.1097/DCR.0b013e31828006f7. [DOI] [PubMed] [Google Scholar]
- 79.Boereboom CL, Watson NFA, Liptrot SA, Lund JN. A randomised trial of fibrin glue vs surgery for pilonidal sinus disease: results and long term follow up. lq bassam diss. 2010;12:1280–1283. [Google Scholar]
- 80.Can MF, Sevinc MM, Hancerliogullari O, Yilmaz M, Yagci G. Multicenter prospective randomized trial comparing modified Limberg flap transposition and Karydakis flap reconstruction in patients with sacrococcygeal pilonidal disease. Am J Surg. 2010;200:318–327. doi: 10.1016/j.amjsurg.2009.08.042. [DOI] [PubMed] [Google Scholar]
- 81.Demircan F, et al. The effect of laser epilation on recurrence and satisfaction in patients with sacrococcygeal pilonidal disease: a prospective randomized controlled trial. Int J Clin Exp Med. 2015;8:2929–2933. [PMC free article] [PubMed] [Google Scholar]
- 82.Ersoy E, et al. Comparison of the short-term results after Limberg and Karydakis procedures for pilonidal disease: randomized prospective analysis of 100 patients. Colorectal Dis. 2009;11:705–710. doi: 10.1111/j.1463-1318.2008.01646.x. [DOI] [PubMed] [Google Scholar]
- 83.Guner A, et al. Limberg flap versus Bascom cleft lift techniques for sacrococcygeal pilonidal sinus: prospective, randomized trial. World J Surg. 2013;37:2074–2080. doi: 10.1007/s00268-013-2111-9. [DOI] [PubMed] [Google Scholar]
- 84.Gurer A, et al. Is routine cavity drainage necessary in Karydakis flap operation? A prospective, randomized trial. Dis Colon Rectum. 2005;48:1797–1799. doi: 10.1007/s10350-005-0108-7. [DOI] [PubMed] [Google Scholar]
- 85.Milone M, Fernandez LM, Musella M, Milone F. Safety and Efficacy of Minimally Invasive Video-Assisted Ablation of Pilonidal Sinus: A Randomized Clinical Trial. JAMA Surg. 2016;151:547–553. doi: 10.1001/jamasurg.2015.5233. [DOI] [PubMed] [Google Scholar]
- 86.Nordon IM, Senapati A, Cripps NP. A prospective randomized controlled trial of simple Bascom’s technique versus Bascom’s cleft closure for the treatment of chronic pilonidal disease. Am J Surg. 2009;197:189–192. doi: 10.1016/j.amjsurg.2008.01.020. [DOI] [PubMed] [Google Scholar]
- 87.Sahin A, Olcucuoglu E, Seker D, Kulacoglu H. The effect of using methylene blue in surgical treatments of pilonidal disease: a prospective randomized study. European Surgery. 2014;46:148–154. doi: 10.1007/s10353-014-0276-6. [DOI] [Google Scholar]
- 88.Sevinc, B. et al. Randomized prospective comparison of midline and off-midline closure techniques in pilonidal sinus surgery. Surgery, 10.1016/j.surg.2015.09.024 (2015). [DOI] [PubMed]
- 89.Sozen S, Emir S, Guzel K, Ozdemir CS. Are postoperative drains necessary with the Karydakis flap for treatment of pilonidal sinus? (Can fibrin glue be replaced to drains?) A prospective randomized trial. Ir J Med Sci. 2011;180:479–482. doi: 10.1007/s11845-010-0549-4. [DOI] [PubMed] [Google Scholar]
- 90.Tokac M, Dumlu EG, Aydin MS, Yalcin A, Kilic M. Comparison of modified limberg flap and karydakis flap operations in pilonidal sinus surgery: prospective randomized study. Int Surg. 2015;100:870–877. doi: 10.9738/INTSURG-D-14-00213.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Abdelrazeq AS, Rahman M, Botterill ID, Alexander DJ. Short-term and long-term outcomes of the cleft lift procedure in the management of nonacute pilonidal disorders. Dis Colon Rectum. 2008;51:1100–1106. doi: 10.1007/s10350-008-9262-z. [DOI] [PubMed] [Google Scholar]
- 92.Abdul-Ghani AK, Abdul-Ghani AN, Ingham Clark CL. Day-care surgery for pilonidal sinus. Ann R Coll Surg Engl. 2006;88:656–658. doi: 10.1308/003588406X149255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Colak T, Turkmenoglu O, Dag A, Akca T, Aydin S. A randomized clinical study evaluating the need for drainage after Limberg flap for pilonidal sinus. J Surg Res. 2010;158:127–131. doi: 10.1016/j.jss.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 94.Das K, et al. Diathermy versus scalpel in Limberg flap in pilonidal sinus surgery. A prospective randomized trial. Ann Ital Chir. 2014;85:148–152. [PubMed] [Google Scholar]
- 95.Erdem E, Sungurtekin U, Nessar M. Are postoperative drains necessary with the Limberg flap for treatment of pilonidal sinus? Dis Colon Rectum. 1998;41:1427–1431. doi: 10.1007/BF02237061. [DOI] [PubMed] [Google Scholar]
- 96.Karakayali F, et al. Unroofing and marsupialization vs. rhomboid excision and Limberg flap in pilonidal disease: a prospective, randomized, clinical trial. Dis Colon Rectum. 2009;52:496–502. doi: 10.1007/DCR.0b013e31819a3ec0. [DOI] [PubMed] [Google Scholar]
- 97.Kirkil C, et al. The effects of drainage on the rates of early wound complications and recurrences after Limberg flap reconstruction in patients with pilonidal disease. Tech Coloproctol. 2011;15:425–429. doi: 10.1007/s10151-011-0782-5. [DOI] [PubMed] [Google Scholar]
- 98.Saydam M, et al. Comparison of modified Limberg flap transposition and lateral advancement flap transposition with Burow’s triangle in the treatment of pilonidal sinus disease. Am J Surg. 2015;210:772–777. doi: 10.1016/j.amjsurg.2015.03.031. [DOI] [PubMed] [Google Scholar]
- 99.Sungurtekin H, Sungurtekin U, Erdem E. Local anesthesia and midazolam versus spinal anesthesia in ambulatory pilonidal surgery. J Clin Anesth. 2003;15:201–205. doi: 10.1016/S0952-8180(03)00032-1. [DOI] [PubMed] [Google Scholar]
- 100.Yabanoglu H, Karagulle E, Belli S, Turk E. Results of modified Dufourmentel rhomboid flap in patients with extensive Sacrococcygeal pilonidal disease. Acta Chir Belg. 2014;114:52–57. [PubMed] [Google Scholar]
- 101.Yetişir F, Kaya O, Baran I. The comparison of marsupialization and Limberg flap in the treatment of pilonidal disease. Turk. J. Surg. 2005;21:184–190. [Google Scholar]
- 102.Zorlu M, et al. Early results with the Mutaf technique: a novel off-midline approach in pilonidal sinus surgery !!writing. 2016;90:265–271. doi: 10.4174/astr.2016.90.5.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Abu Galala KH, Salam IMA, El Ashaal YI, Chandran VP, Sim AJW. Excision of pilonidal sinus and primary closure by a rhomboid flap transposition. Asian Journal of Surgery. 1996;19:305–308. [Google Scholar]
- 104.Afsarlar CE, et al. Treatment of adolescent pilonidal disease with a new modification to the Limberg flap: symmetrically rotated rhomboid excision and lateralization of the Limberg flap technique. J Pediatr Surg. 2013;48:1744–1749. doi: 10.1016/j.jpedsurg.2013.01.029. [DOI] [PubMed] [Google Scholar]
- 105.Malik GA, Choudary TH, Wahab A. Pilonidal Sinus; Prevalence and comparison of excision and primary closure with lay open procedure. Professional Med J. 2009;16:297–298. [Google Scholar]
- 106.Acarturk TO, Parsak CK, Sakman G, Demircan O. Superior gluteal artery perforator flap in the reconstruction of pilonidal sinus. J Plast Reconstr Aesthet Surg. 2010;63:133–139. doi: 10.1016/j.bjps.2008.07.017. [DOI] [PubMed] [Google Scholar]
- 107.Awad MM, Saad KM. Does closure of chronic pilonidal sinus still remain a matter of debate after bilateral rotation flap? (N-shaped closure technique) daten nachtragen. 2006;39:157–162. [Google Scholar]
- 108.Abramson DJ. A simple marsupialization technic for treatment of pilonidal sinus: long-term follow up. Ann Surg. 1960;151:261–267. doi: 10.1097/00000658-196002000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Abramson DJ. An open, semiprimary closure operation for pilonidal sinuses, using local anesthesia. Dis Colon Rectum. 1970;13:215–219. doi: 10.1007/BF02617211. [DOI] [PubMed] [Google Scholar]
- 110.Al-Naami MY. Outpatient pilonidal sinotomy complemented with good wound and surrounding skin care. Saudi Med J. 2005;26:285–288. [PubMed] [Google Scholar]
- 111.Awad MM, et al. A scoring system as a method to evaluate pilonidal sinus disease to make an easy decision for its management. Daten nachtragen. 2009;42:43–48. doi: 10.4103/0970-0358.53011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Baier PK, Baumgartner U, Furtwangler A, Holzinger F, Schoffel U. Therapy of the pilonidal sinus–Primary wound closure or open wound after excision. Zentralbl Chir. 2002;127:310–314. doi: 10.1055/s-2002-31557-1. [DOI] [PubMed] [Google Scholar]
- 113.Baldelli CM, et al. A short course of granulocyte-colony-stimulating factor to accelerate wound repair in patients undergoing surgery for sacrococcygeal pilonidal cyst: proof of concept. Cytotherapy. 2012;14:1101–1109. doi: 10.3109/14653249.2012.697147. [DOI] [PubMed] [Google Scholar]
- 114.Bianco V, Basile C, Tortorella M. Sacrococcygeal pilonidal sinus disease. Treatment by “open” and “closed” technique: personal experience. G Chir. 2003;24:145–147. [PubMed] [Google Scholar]
- 115.Blake P. et al. Tratamiento quirurgico del quiste pilonidal. Revista chilena de cirugía (1997).
- 116.Blanco G, Giordano M, Torelli I. Surgical treatment of pilonidal sinus with open surgical technique. Minerva Chir. 2003;58:181–187. [PubMed] [Google Scholar]
- 117.Bracho Bracho, J. & Lira Soto, N. M. Enfermedad pilonidal: tecnica cerrada Vs. tecnica abierta con anestesia local. Boletin médico de postgrado (1996).
- 118.Breidenbach L, Wilson HLP. Cysts and Sinuses. Ann Surg. 1935;102:455–463. doi: 10.1097/00000658-193509000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Brust JC, Sarner JB. Pilonidal cyst. N Y State J Med. 1948;48:2138–2144. [PubMed] [Google Scholar]
- 120.Butter A, Hanson M, VanHouwelingen L, Merritt N, Seabrook J. Hair epilation versus surgical excision as primary management of pilonidal disease in the pediatric population. Can J Surg. 2015;58:209–211. doi: 10.1503/cjs.011214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Carstensen E, Keichel F. Etiology and therapy of pilonidal sinus. Chirurg. 1963;34:303–308. [PubMed] [Google Scholar]
- 122.Castronovo G, Ciulla A, Urso G, Tomasello G, Damiani S. Pilonidal sinus: an retrospective analysis of 205 cases. Ann Ital Chir. 2003;74:559–563. [PubMed] [Google Scholar]
- 123.Chiedozi LC, Al-Rayyes FA, Salem MM, Al-Haddi FH, Al-Bidewi AA. Management of pilonidal sinus. Saudi Med J. 2002;23:786–788. [PubMed] [Google Scholar]
- 124.Cimarelli S, Magnano G. Treatment of pilonidal sinus. Our experience. Minerva Chir. 1989;44:1131–1134. [PubMed] [Google Scholar]
- 125.Close AS. Pilonidal cysts: an analysis of surgical failures. Ann Surg. 1955;141:523–526. doi: 10.1097/00000658-195504000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Coda A, Ferri F. Sinus pilonidalis: Removal and primary suture with aspirative draining. Chirurgia. 1990;3:433–437. [Google Scholar]
- 127.Dahmann S, Lebo PB, Meyer-Marcotty MV. Comparison of Treatments for an Infected Pilonidal Sinus: Differences in Scar Quality and Outcome Between Secondary Wound Healing and Limberg Flap in a Prospective Study. Handchir Mikrochir Plast Chir. 2016;48:111–119. doi: 10.1055/s-0041-111322. [DOI] [PubMed] [Google Scholar]
- 128.Falco M, et al. Surgical treatment of sinus pilonidalis by Dufourmentel’s flap technique. Il Giornale di chirurgia. 2007;28:93–97. [PubMed] [Google Scholar]
- 129.DeRosario JL, Khare U. Pilonidal disease–a surgical enigma. Can Med Assoc J. 1965;93:1262–1267. [PMC free article] [PubMed] [Google Scholar]
- 130.Destito C, Romagnoli A, Pucello D, Mercuri M, Marin AW. Pilonidal sinus: long term results of excision and closure technic. Review of the literature. G Chir. 1997;18:441–446. [PubMed] [Google Scholar]
- 131.Doll D, et al. Methylene Blue halves the long-term recurrence rate in acute pilonidal sinus disease. Int J Colorectal Dis. 2008;23:181–187. doi: 10.1007/s00384-007-0393-9. [DOI] [PubMed] [Google Scholar]
- 132.Doll D, et al. Timeline of recurrence after primary and secondary pilonidal sinus surgery. Dis Colon Rectum. 2007;50:1928–1934. doi: 10.1007/s10350-007-9031-4. [DOI] [PubMed] [Google Scholar]
- 133.Doll D, Matevossian E, Hoenemann C, Hoffmann S. Incision and drainage preceding definite surgery achieves lower 20-year long-term recurrence rate in 583 primary pilonidal sinus surgery patients. patienten info. 2013;11:60–64. doi: 10.1111/j.1610-0387.2012.08007.x. [DOI] [PubMed] [Google Scholar]
- 134.Donati A, et al. Heterologous lyophilized collagen in the secondary healing of pilonidal fistulae. Minerva Chir. 1993;48:141–145. [PubMed] [Google Scholar]
- 135.Dorman RM, Bass KD. Novel use of porcine urinary bladder matrix for pediatric pilonidal wound care: preliminary experience. Pediatr Surg Int. 2016;32:997–1002. doi: 10.1007/s00383-016-3915-0. [DOI] [PubMed] [Google Scholar]
- 136.Dudink R, Veldkamp J, Nienhuijs S, Heemskerk J. Secondary healing versus midline closure and modified Bascom natal cleft lift for pilonidal sinus disease. Scand J Surg. 2011;100:110–113. doi: 10.1177/145749691110000208. [DOI] [PubMed] [Google Scholar]
- 137.Dwight RW, Maloy JK. Pilonidal sinus; experience with 449 cases. N Engl J Med. 1953;249:926–930. doi: 10.1056/NEJM195312032492303. [DOI] [PubMed] [Google Scholar]
- 138.Eftaiha M, Abcarian H. The dilemma of pilonidal disease: surgical treatment. Dis Colon Rectum. 1977;20:279–286. doi: 10.1007/BF02586423. [DOI] [PubMed] [Google Scholar]
- 139.Eichfuss HP, Schontag H, Pfeiffer M. A new surgical procedure for treating sacrococcygeal fistulas and cysts. Aktuel Chir. 1982;17:138–140. [Google Scholar]
- 140.Elbanna HG, et al. Novel Approach of Treatment of Pilonidal Sinus Disease With Thrombin Gelatin Matrix as a Sealant. Dis Colon Rectum. 2016;59:775–780. doi: 10.1097/DCR.0000000000000604. [DOI] [PubMed] [Google Scholar]
- 141.Fahrni GT, et al. Five-year Follow-up and Recurrence Rates Following Surgery for Acute and Chronic Pilonidal Disease: A Survey of 421 Cases. Wounds. 2016;28:20–26. [PubMed] [Google Scholar]
- 142.Feigenbaum HA. Excision of acute pilonidal cyst abscess; a preliminary report. Am J Surg. 1957;94:636–637. doi: 10.1016/0002-9610(57)90595-0. [DOI] [PubMed] [Google Scholar]
- 143.Fitzpatrick EB, et al. Pilonidal disease in a military population: how far have we really come? Am J Surg. 2014;207:907–914. doi: 10.1016/j.amjsurg.2013.07.038. [DOI] [PubMed] [Google Scholar]
- 144.Fox PF. Pilonidal Cysts and Sinuses in Identical Twins. Journal of the American Medical Association (JAMA) 1944;125:120. doi: 10.1001/jama.1944.72850200004010a. [DOI] [Google Scholar]
- 145.Garcia JC, Dupuis F. Surgical treatment of pilonidal disease. A new simplified technic. J Chir (Paris) 1983;120:347–350. [PubMed] [Google Scholar]
- 146.Gendy AS, et al. A comparison of the cleft lift procedure vs wide excision and packing for the treatment of pilonidal disease in adolescents. J Pediatr Surg. 2011;46:1256–1259. doi: 10.1016/j.jpedsurg.2011.03.062. [DOI] [PubMed] [Google Scholar]
- 147.Gerhard H. On the understanding and treating coccygeal fustulae. Z Aerztl Fortbildg (Jena) 1963;57:841–843. [PubMed] [Google Scholar]
- 148.Golz A, Argov S, Barzilai A. Pilonidal sinus disease: comparison among various methods of treatment and a survey of 160 patients. Curr Surg. 1980;37:77–85. [PubMed] [Google Scholar]
- 149.Goodall P. The aetiology and treatment of pilonidal sinus. A review of 163 patients. Br J Surg. 1961;49:212–218. doi: 10.1002/bjs.18004921421. [DOI] [PubMed] [Google Scholar]
- 150.Grandjean JP, Al Nashawati G. Pilonidal disease treated by wide excision and controlled cicatrisation. A report on 73 patients. Lyon Chir. 1996;92:292–295. [Google Scholar]
- 151.Gupta PJ. Radio surgery in pilonidal sinus: a new approach for the old problem. Acta Chir Belg. 2005;105:183–186. [PubMed] [Google Scholar]
- 152.Guyuron B, Dinner MI, Dowden RV. Excision and grafting in treatment of recurrent pilonidal sinus disease. Surg Gynecol Obstet. 1983;156:201–204. [PubMed] [Google Scholar]
- 153.Hell E, Zimmermann G, Boeckl O. Pilonidal disorder (pilonidal cyst) and its treatment. Med Welt. 1971;6:230–232. [PubMed] [Google Scholar]
- 154.Hemati HR, Ghorbani R, Nayeri Tarshizi E. Recurrence rate in the pilonidal sinus after excision with or without primary closure. Koomesh. 2013;15:78–82. [Google Scholar]
- 155.Hoffert PW, Healy MJ., Jr. Pilonidal sinus and cyst: an analysis of the results of surgical therapy in 229 consecutive cases. Bull N Y Acad Med. 1952;28:612. [PubMed] [Google Scholar]
- 156.Holmebakk T, Nesbakken A. Surgery for pilonidal disease. Scand J Surg. 2005;94:43–46. doi: 10.1177/145749690509400111. [DOI] [PubMed] [Google Scholar]
- 157.Hosseini M, Heidari A, Jafarnejad B. Comparison of Three Surgical Methods in Treatment of Patients with Pilonidal Sinus: Modified Excision and Repair/Wide Excision/Wide Excision and Flap in RASOUL, OMID and SADR Hospitals (2004–2007) Indian J Surg. 2013;75:395–400. doi: 10.1007/s12262-012-0713-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Houston HE. One-stage cure of infected pilonidal cysts. Am Surg. 1977;43:517–519. [PubMed] [Google Scholar]
- 159.Hughes LE, Harding KG. Radical surgery for pilonidal sinus. Annals of the Royal College of Surgeons of England. 1983;65:64–65. [PMC free article] [PubMed] [Google Scholar]
- 160.Iesalnieks I, Furst A, Rentsch M, Jauch KW. Primary midline closure after excision of a pilonidal sinus is associated with a high recurrence rate. Chirurg. 2003;74:461–468. doi: 10.1007/s00104-003-0616-8. [DOI] [PubMed] [Google Scholar]
- 161.Iesalnieks I, Deimel S, Schlitt HJ. Karydakis flap for recurrent pilonidal disease. World J Surg. 2013;37:1115–1120. doi: 10.1007/s00268-013-1950-8. [DOI] [PubMed] [Google Scholar]
- 162.Jordan MH, Meinecke HM. Ambulatory surgery for pilonidal disease. Am Surg. 1979;45:360–363. [PubMed] [Google Scholar]
- 163.Kasim K, Abdlhamid NM, Badwan BR, Allowbany A. Is There a Relation Between Natal Cleft Depth and Post-Operative Morbidity After Different Methods of Excision of Sacro-Coccygeal Pilonidal Sinus? Indian J Surg. 2015;77:201–205. doi: 10.1007/s12262-012-0762-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Kement M, Oncel M, Kurt N, Kaptanoglu L. Sinus excision for the treatment of limited chronic pilonidal disease: results after a medium-term follow-up. Dis Colon Rectum. 2006;49:1758–1762. doi: 10.1007/s10350-006-0676-1. [DOI] [PubMed] [Google Scholar]
- 165.Khodakaram K, Stark J, Hoglund I, Andersson RE. Minimal Excision and Primary Suture is a Cost-Efficient Definitive Treatment for Pilonidal Disease with Low Morbidity: A Population-Based Interventional and a Cross-Sectional Cohort Study. World J Surg. 2016 doi: 10.1007/s00268-016-3828-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Kleckner MS. Pilonidal Sinus: Its surgical management. Trans Am Proctol Soc. 1936;36:166. [Google Scholar]
- 167.Kleiman A. Pilonidal cyst; follow-up studies on 481 patients. USArmed Forces Med J. 1952;3:575–580. [PubMed] [Google Scholar]
- 168.Kooistra HP. Pilonidal sinuses. Review of the literature and report of three hundred fifty cases. Am J Surg. 1942;LV 1:3–17. doi: 10.1016/S0002-9610(42)90210-1. [DOI] [Google Scholar]
- 169.Lamke LO, Larsson J, Nylen B. Results of different types of operation for pilonidal sinus. Acta Chir Scand. 1974;140:321–324. [PubMed] [Google Scholar]
- 170.Larsen BB. Comparative results-in operations for pilonidal cysts. Arch Surg. 1948;56:516–521. doi: 10.1001/archsurg.1948.01240010524006. [DOI] [PubMed] [Google Scholar]
- 171.Lawrence KB, Baker WJ. The marsupialization operation for pilonidal sinus; a comparison with other surgical methods in 359 cases. N Engl J Med. 1951;245:134–139. doi: 10.1056/NEJM195107262450403. [DOI] [PubMed] [Google Scholar]
- 172.Leak K, Widgerow A, Johnson S. Pilonidal sinus (Jeep’s disease): An improved model of care. Wounds UK. 2011;7:72–77. [Google Scholar]
- 173.Thompson JPS, Lee J. Radical surgery for pilonidal sinus. Annals of the Royal College of Surgeons of England. 1983;65:64–65. [PMC free article] [PubMed] [Google Scholar]
- 174.Leoni G, et al. Sinus pilonidalis. Critical review of our experience. Chirurgia. 1998;11:93–96. [Google Scholar]
- 175.Lukish JR, Kindelan T, Marmon LM, Pennington M, Norwood C. Laser epilation is a safe and effective therapy for teenagers with pilonidal disease. J Pediatr Surg. 2009;44:282–285. doi: 10.1016/j.jpedsurg.2008.10.057. [DOI] [PubMed] [Google Scholar]
- 176.Lynch JB, Laing AJ, Regan PJ. Vacuum-assisted closure therapy: a new treatment option for recurrent pilonidal sinus disease. Report of three cases. Dis Colon Rectum. 2004;47:929–932. doi: 10.1007/s10350-004-0522-2. [DOI] [PubMed] [Google Scholar]
- 177.Macfee WF. Pilonidal Cysts and Sinuses: A Method of Wound Closure: Review of 230 Cases. Ann Surg. 1942;116:687–699. doi: 10.1097/00000658-194211650-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Mathesheimer JL. An ambulant method for the treatment of pilonidal disease. Am J Surg. 1945;69:230–231. doi: 10.1016/S0002-9610(45)90377-1. [DOI] [Google Scholar]
- 179.Matter I, Kunin J, Schein M, Eldar S. Total excision versus non-resectional methods in the treatment of acute and chronic pilonidal disease. Br J Surg. 1995;82:752–753. doi: 10.1002/bjs.1800820612. [DOI] [PubMed] [Google Scholar]
- 180.McGuinness JG, Winter DC, O’Connell PR. Vacuum-assisted closure of a complex pilonidal sinus. Dis Colon Rectum. 2003;46:274–276. doi: 10.1007/s10350-004-6535-z. [DOI] [PubMed] [Google Scholar]
- 181.McKirdie M. Pilonidal Sinus. Ann Surg. 1938;107:389–399. doi: 10.1097/00000658-193803000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Meier HP. Recurrence in sacral dermoid (sinusitis pilonidalis sacralis) Helv Chir Acta. 1983;49:645–649. [PubMed] [Google Scholar]
- 183.Menzel T, Dorner A, Cramer J. Excision and open wound treatment of pilonidal sinus. Rate of recurrence and duration of work incapacity. Dtsch Med Wochenschr. 1997;122:1447–1451. doi: 10.1055/s-2008-1047784. [DOI] [PubMed] [Google Scholar]
- 184.Morden P, Drongowski RA, Geiger JD, Hirschl RB, Teitelbaum DH. Comparison of Karydakis versus midline excision for treatment of pilonidal sinus disease. Pediatr Surg Int. 2005;21:793–796. doi: 10.1007/s00383-005-1543-1. [DOI] [PubMed] [Google Scholar]
- 185.Mueller X, Rothenbuehler JM, Frede KE. Sacrococcygeal cysts. Is Lord Millar’s procedure an alternative to exeresis? J Chir. 1991;128:487–490. [PubMed] [Google Scholar]
- 186.Mustafi N, Engels P. Post-surgical wound management of pilonidal cysts with a haemoglobin spray: a case series. J Wound Care. 2016;25:191–198. doi: 10.12968/jowc.2016.25.4.191. [DOI] [PubMed] [Google Scholar]
- 187.Nahas SC, et al. Results of the surgical treatment of non-complicated pilonidal disease. Rev Hosp Clin Fac Med Sao Paulo. 1997;52:287–290. [PubMed] [Google Scholar]
- 188.Nasr A, Ein SH. A pediatric surgeon’s 35-year experience with pilonidal disease in a Canadian children’s hospital. Can J Surg. 2011;54:39–42. doi: 10.1503/cjs.028509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.Notaras MJ. A review of three popular methods of treatment of postanal (pilonidal) sinus disease. Br J Surg. 1970;57:886–890. doi: 10.1002/bjs.1800571204. [DOI] [PubMed] [Google Scholar]
- 190.Obedman M, Vaticon D. Pilonidal sinus: a high-incidence disease among adolescents. etiology, hair, recurrence, incidence. 1993;6:21–36. doi: 10.1515/IJAMH.1993.6.1.21. [DOI] [PubMed] [Google Scholar]
- 191.Ommer A, et al. Pilonidal Sinus–Primary Closure also in Case of Abscess? Zentralbl Chir. 2004;129:216–219. doi: 10.1055/s-2004-822742. [DOI] [PubMed] [Google Scholar]
- 192.Oram Y, Kahraman F, Karincaoglu Y, Koyuncu E. Evaluation of 60 patients with pilonidal sinus treated with laser epilation after surgery. Dermatol Surg. 2010;36:88–91. doi: 10.1111/j.1524-4725.2009.01387.x. [DOI] [PubMed] [Google Scholar]
- 193.Ortiz HH, Marti J, Sitges A. Pilonidal sinus: a claim for simple track incision. Dis Colon Rectum. 1977;20:325–328. doi: 10.1007/BF02586431. [DOI] [PubMed] [Google Scholar]
- 194.Oueidat D, Dirani RA, Assi M, Shams TB, Jurjus A. A. 25 years’ experience in the management of pilonidal sinus disease. Open Journal of Gastroenterology. 2014;4:5. doi: 10.4236/ojgas.2014.41001. [DOI] [Google Scholar]
- 195.Patti R, et al. Use of fibrin glue in the treatment of pilonidal sinus disease: a pilot study. G Chir. 2006;27:331–334. [PubMed] [Google Scholar]
- 196.Pazdirek F, Kouda M, Jech Z, Frajer L, J. JH. Pilonidal sinus - diagnosis at the intersection of general and plastic surgery. 2014;93:545–548. [PubMed] [Google Scholar]
- 197.Perruchoud C, Vuilleumier H, Givel JC. Pilonidal sinus: how to choose between excision and open granulation versus excision and primary closure? Study of a series of 141 patients operated on from 1991 to 1995. Swiss Surg. 2002;8:255–258. doi: 10.1024/1023-9332.8.6.255. [DOI] [PubMed] [Google Scholar]
- 198.Petersen S, et al. Short-term results of Karydakis flap for pilonidal sinus disease. Tech.Coloproctol. 2007;11:235–240. doi: 10.1007/s10151-007-0357-7. [DOI] [PubMed] [Google Scholar]
- 199.Rabie ME, et al. Sacrococcygeal pilonidal disease: sinotomy versus excisional surgery, a retrospective study. ANZ J Surg. 2007;77:177–180. doi: 10.1111/j.1445-2197.2006.04002.x. [DOI] [PubMed] [Google Scholar]
- 200.Riedler L, Weimann S, Steiner E. Operative therapy of the pilonidal sinus; 115 controlled patients. Zentralbl Chir. 1978;103:1410–1415. [PubMed] [Google Scholar]
- 201.Roberton HR. Pilonidal surgery. Med J Aust. 1981;1:375–376. [PubMed] [Google Scholar]
- 202.Rogers H, Dwight RW. Pilonidal Sinus: Observations on One Hundred Forty Cases Treated by Cautery Excision. Ann Surg. 1938;107:400–418. doi: 10.1097/00000658-193803000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Rosato L, Fornero G, Luc AR, Clerico G. The radical treatment of sacrococcygeal pilonidal cysts. Minerva Chir. 1997;52:1277–1279. [PubMed] [Google Scholar]
- 204.Rouch JD, et al. Short- and Long-term Results of Unroofing and Marsupialization for Adolescent Pilonidal Disease. JAMA Surg. 2016;151:877–879. doi: 10.1001/jamasurg.2016.0850. [DOI] [PubMed] [Google Scholar]
- 205.Ruf G. Pilonidal sinus. Coloproctology. 2006;28:315–321. doi: 10.1007/s00053-006-6024-z. [DOI] [Google Scholar]
- 206.Sakr, M. F., Hamed, H. H., Ramadan, M. A., Kantoush, H. E. & Al-Torky, H. M. Pilonidal sinus in Kuwait: Analysis of 801 consecutive patients. (2012).
- 207.Sasse, K. C., Brandt, J., Lim, D. C. & Ackerman, E. Accelerated healing of complex open pilonidal wounds using MatriStem extracellular matrix xenograft: nine cases. J Surg Case Rep2013, 10.1093/jscr/rjt025 (2013). [DOI] [PMC free article] [PubMed]
- 208.Schmitt JC, et al. Pilonidal cysts. 161 operated cases. Ann Chir. 1977;31:973–979. [PubMed] [Google Scholar]
- 209.Seleem MI, Al-Hashemy AM. Management of pilonidal sinus using fibrin glue: a new concept and preliminary experience. Colorectal Dis. 2005;7:319–322. doi: 10.1111/j.1463-1318.2005.00808.x. [DOI] [PubMed] [Google Scholar]
- 210.Shafik A. Electrocauterization in the treatment of pilonidal sinus. Int Surg. 1996;81:83–84. [PubMed] [Google Scholar]
- 211.Shinde P, Toshikhane H. Pilonidal sinus (Nadi vrana): A case study. Int J Ayurveda Res. 2010;1:181–182. doi: 10.4103/0974-7788.72492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 212.Shpitz B, Kaufman Z, Kantarovsky A, Reina A, Dinbar A. Definitive management of acute pilonidal abscess by loop diathermy excision. Dis Colon Rectum. 1990;33:441–442. doi: 10.1007/BF02156276. [DOI] [PubMed] [Google Scholar]
- 213.Soll C, Hahnloser D, Dindo D, Clavien PA, Hetzer F. A novel approach for treatment of sacrococcygeal pilonidal sinus: less is more. Int J Colorectal Dis. 2008;23:177–180. doi: 10.1007/s00384-007-0377-9. [DOI] [PubMed] [Google Scholar]
- 214.Soll C, et al. Sinusectomy for primary pilonidal sinus: less is more. Surgery. 2011;150:996–1001. doi: 10.1016/j.surg.2011.06.019. [DOI] [PubMed] [Google Scholar]
- 215.Solla JA, Rothenberger DA. Chronic pilonidal disease. An assessment of 150 cases. Dis Colon Rectum. 1990;33:758–761. doi: 10.1007/BF02052321. [DOI] [PubMed] [Google Scholar]
- 216.Sondenaa K, Nesvik I, Andersen E, Pollard ML, Soreide JA. Recurrent pilonidal sinus: Etiology and treatment. Dig. Surg. 1995;12:117–120. doi: 10.1159/000172329. [DOI] [Google Scholar]
- 217.Speter C, Zmora O, Nadler R, Shinhar D, Bilik R. Minimal incision as a promising technique for resection of pilonidal sinus in children. J Pediatr Surg. 2017 doi: 10.1016/j.jpedsurg.2017.03.040. [DOI] [PubMed] [Google Scholar]
- 218.Spivak H, Brooks VL, Nussbaum M, Friedman I. Treatment of chronic pilonidal disease. Dis Colon Rectum. 1996;39:1136–1139. doi: 10.1007/BF02081415. [DOI] [PubMed] [Google Scholar]
- 219.Stansby G, Greatorex R. Phenol treatment of pilonidal sinuses of the natal cleft. Br J Surg. 1989;76:729–730. doi: 10.1002/bjs.1800760727. [DOI] [PubMed] [Google Scholar]
- 220.Stelzmueller I, et al. Group Milleri Streptococci in perianal infections. Colorectal disease: the official journal of the Association of Coloproctology of Great Britain and Ireland. 2010;12:e121–127. doi: 10.1111/j.1463-1318.2009.01847.x. [DOI] [PubMed] [Google Scholar]
- 221.Sturniolo G, Carditello A, Bonavita G, Bartolotta M, Saitta E. Evaluation of the results of different types of surgical intervention for pilonidal fistula. Minerva Chir. 1984;39:1161–1164. [PubMed] [Google Scholar]
- 222.Swenson SAHHN, Groesbeck HP. Pilonidal Sinus - Clinical Experiences with the Rogers Operation in thirty-five consecutive cases. Am J Surg. 1944;66:49–57. doi: 10.1016/S0002-9610(44)90226-6. [DOI] [Google Scholar]
- 223.Tetirick JE. Limited excision of pilonidal cyst and sinus. Ohio State Med J. 1971;67:135–138. [PubMed] [Google Scholar]
- 224.Thomas D. Pilonidal sinus: a review of the literature and a report of 100 cases. Med J Aust. 1968;2:184–188. doi: 10.5694/j.1326-5377.1968.tb29395.x. [DOI] [PubMed] [Google Scholar]
- 225.Thomason TH. Cysts and sinuses of sacrococcygeal region. Ann Surg. 1934;32:80. doi: 10.1097/00000658-193404000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226.Val-Bernal JF, González-Vela MC, Hermana S, Garijo MF, González-López MA. Pilonidal sinus associated with cellular blue nevus. A previously unrecognized association. J. Cutaneous Pathol. 2007;34:942–945. doi: 10.1111/j.1600-0560.2007.00753.x. [DOI] [PubMed] [Google Scholar]
- 227.Vaughn CJ, Lalikos JF. The use of acellular dermal regeneration template for recalcitrant pilonidal disease. J Wound Care. 2011;20:275–277. doi: 10.12968/jowc.2011.20.6.275. [DOI] [PubMed] [Google Scholar]
- 228.Walfisch S, Mnitentag H, Baruchin AM, Sagi A. Nd: YAG and CO 2 Lasers for the Treatment of Pilonidal Sinuses: Advantages over Traditional Techniques. Medical Laser Application. 2004;19:155–159. doi: 10.1078/1615-1615-00138. [DOI] [Google Scholar]
- 229.Wang C, Yao Y, Cao Y. The integrative method “suture dragging and simplified vacuum assisted therapy” for complex pilonidal sinus disease. Case Rep Surg. 2014;2014:425497. doi: 10.1155/2014/425497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Weckner W, Zorner M. Treatment of pilonidal sinus. Z Aerztl Fortbildg (Jena) 1981;75:903–906. [PubMed] [Google Scholar]
- 231.Williams AC. Skin grafting in the treatment of extensive pilonidal disease and anal fistula. Am Surg. 1951;17:1137–1144. [PubMed] [Google Scholar]
- 232.Yamashita Y, Nagae H, Hashimoto I. Ambulatory Surgery for Pilonidal Sinus: Tract Excision and Open Treatment Followed by At-Home Irrigation. J Med Invest. 2016;63:216–218. doi: 10.2152/jmi.63.216. [DOI] [PubMed] [Google Scholar]
- 233.Zagory JA, Golden J, Holoyda K, Demeter N, Nguyen NX. Excision and Primary Closure May Be the Better Option in the Surgical Management of Pilonidal Disease in the Pediatric Population. Am Surg. 2016;82:964–967. [PubMed] [Google Scholar]
- 234.Zieger K. Complications after surgery for pilonidal cyst. An introduction to a new debate on a “costly” disease. Ugeskr Laeger. 1999;161:6056–6058. [PubMed] [Google Scholar]
- 235.Abbasi HRH, Hosseini SV, Yarmohammadi H, Bolandparvaz S. Comparison between two methods of excision and primary closure of pilonidal sinus. Electrocautery increases recurrence. 2007;9:143–146. [Google Scholar]
- 236.Abu Galala KH, et al. Treatment of pilonidal sinus by primary closure with a transposed rhomboid flap compared with deep suturing: a prospective randomised clinical trial. Eur.J Surg. 1999;165:468–472. doi: 10.1080/110241599750006721. [DOI] [PubMed] [Google Scholar]
- 237.Akinci OF, Coskun A, Ozgonul A, Terzi A. Surgical treatment of complicated pilonidal disease: limited separate elliptical excision with primary closure. Colorectal Dis. 2006;8:704–709. doi: 10.1111/j.1463-1318.2006.01022.x. [DOI] [PubMed] [Google Scholar]
- 238.Albahadili MA, Awazli LG. Pilonidal Sinus Excision Using Carbon Dioxide Laser 10600 nm. Iraqi J Laser. 2015;14:33–40. [Google Scholar]
- 239.Aldean I, Shankar PJ, Mathew J, Safarani N, Haboubi NY. Simple excision and primary closure of pilonidal sinus: a simple modification of conventional technique with excellent results. Colorectal Dis. 2005;7:81–85. doi: 10.1111/j.1463-1318.2004.00736.x. [DOI] [PubMed] [Google Scholar]
- 240.Al-Jaberi TM. Excision and simple primary closure of chronic pilonidal sinus. Eur J Surg. 2001;167:133–135. doi: 10.1080/110241501750070600. [DOI] [PubMed] [Google Scholar]
- 241.Almajid FM, Alabdrabalnabi AA, Almulhim KA. The risk of recurrence of Pilonidal disease after surgical management. Saudi Med J. 2017;38:70–74. doi: 10.15537/smj.2017.1.15892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242.Alptekin H, et al. Specimen index may be a predictive factor for recurrence after primary closure of pilonidal disease. J Korean Surg Soc. 2012;83:367–373. doi: 10.4174/jkss.2012.83.6.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 243.Angermann P, Beiter EC. Pilonidal cyst. A sequence treated with excision and primary suture. Ugeskr Laeger. 1984;146:24–26. [PubMed] [Google Scholar]
- 244.Arda IS, Guney LH, Sevmis S, Hicsonmez A. High body mass index as a possible risk factor for pilonidal sinus disease in adolescents. World J Surg. 2005;29:469–471. doi: 10.1007/s00268-004-7533-y. [DOI] [PubMed] [Google Scholar]
- 245.Aydede H, Erhan Y, Sakarya A, Kumkumoglu Y. Comparison of three methods in surgical treatment of pilonidal disease. ANZ J Surg. 2001;71:362–364. doi: 10.1046/j.1440-1622.2001.02129.x. [DOI] [PubMed] [Google Scholar]
- 246.Badawy EA, Kanawati MN. Effect of hair removal by Nd:YAG laser on the recurrence of pilonidal sinus. J Eur Acad Dermatol Venereol. 2009;23:883–886. doi: 10.1111/j.1468-3083.2009.03147.x. [DOI] [PubMed] [Google Scholar]
- 247.Bear NE, Woldman VF. Treatment of pilonidal cysts. Wis Med J. 1945;44:1166–1169. [PubMed] [Google Scholar]
- 248.Beardsley JM. Treatment of pilonidal cyst and sinus. AMA Arch Surg. 1954;68:608–611. doi: 10.1001/archsurg.1954.01260050610004. [DOI] [PubMed] [Google Scholar]
- 249.Bellis CJ. Pilonidal cyst; treatment by a uniformly successful method. dressing verband!! rö xrt. 1950;13:334–337. [PubMed] [Google Scholar]
- 250.Benfatto G, et al. Drainage useful in the excision and closure “per primam” of pilonidal sinus: technical notes. Chir Ital. 2003;55:621–624. [PubMed] [Google Scholar]
- 251.Bentivegna SS, Procario P. Primary closure of pilonidal cystectomy. Am Surg. 1977;43:214–216. [PubMed] [Google Scholar]
- 252.Bhushan TV. Surgical treatment of chronic sacrococcygeal pilonidal sinus. Open method versus primary closure. Saudi Med J. 2007;28:815. [PubMed] [Google Scholar]
- 253.Biffoni M, et al. Pilonidal sinus. Outpatient treatment with local anesthesia. G Chir. 2009;30:173–176. [PubMed] [Google Scholar]
- 254.Bissett IP, Isbister WH. The management of patients with pilonidal disease–a comparative study. Aust N Z J Surg. 1987;57:939–942. doi: 10.1111/j.1445-2197.1987.tb01298.x. [DOI] [PubMed] [Google Scholar]
- 255.Bouq YA, Fazili FM, Fawzi HAG, Parvez T. Surgical management of pilonidal disease: Our experience. JK Pract. 2004;11:21–26. [Google Scholar]
- 256.Bowers WF, Williamson WS. Pilonidal sinus; preliminary report on a fresh approach. AMA Arch Surg. 1956;73:931–935. doi: 10.1001/archsurg.1956.01280060031006. [DOI] [PubMed] [Google Scholar]
- 257.Braungart S, Powis M, Sutcliffe JR, Sugarman ID. Improving outcomes in pilonidal sinus disease. J Pediatr Surg. 2016;51:282–284. doi: 10.1016/j.jpedsurg.2015.10.076. [DOI] [PubMed] [Google Scholar]
- 258.Brearley R. Treatment of pilonidal sinus. Br Med J. 1959;2:1256. doi: 10.1136/bmj.2.5161.1256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 259.Britton DC, Marks CG, Ritchie JK, Thompson HR. The treatment of pilonidal sinus at St Mark’s Hospital. Proc R Soc Med. 1977;70:478–480. doi: 10.1177/003591577707000708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 260.Bunke HJ, Schultheis A, Meyer G, Dusel W. Surgical revision of the pilonidal sinus with single shot antibiosis. Chirurg. 1995;66:220–223. [PubMed] [Google Scholar]
- 261.Çaglayan K, et al. The effect of different surgical methods on complications and on the quality of life in pilonidal sinus disease. Turk. J. Surg. 2011;27:94–97. doi: 10.5097/1300-0705.UCD.950-11.03. [DOI] [Google Scholar]
- 262.Çaglayan K, et al. Investigation of Patient Dependent Factors Effecting Complications and Recurrence in Pilonidal Sinus Disease. Kolon Rektum Hast Derg. 2011;21:103–108. doi: 10.5505/KRHD.2011.43434. [DOI] [Google Scholar]
- 263.Can MF, Sevinc MM, Yilmaz M. Comparison of Karydakis flap reconstruction versus primary midline closure in sacrococcygeal pilonidal disease: results of 200 military service members. Surg Today. 2009;39:580–586. doi: 10.1007/s00595-008-3926-0. [DOI] [PubMed] [Google Scholar]
- 264.Christensen K, Kronborg O, Zimmermann-Nielsen C, Olsen H. Incision or primary suture in acute pilonidal abscesses. A prospective randomized study. Ugeskr Laeger. 1985;147:3479–3481. [PubMed] [Google Scholar]
- 265.Cianci F, Marinaccio F. Treatment of pilonidal sinus by radical excision and primary closure. Our experience. Minerva Chir. 1984;39:1111–1115. [PubMed] [Google Scholar]
- 266.Ciccolo A, et al. Treatment of pilonidal disease in short-stay surgery: personal method. Ann Ital Chir. 2004;75:603–605. [PubMed] [Google Scholar]
- 267.Cihan A, et al. Modified Limberg flap reconstruction compares favourably with primary repair for pilonidal sinus surgery. ANZ J Surg. 2004;74:238–242. doi: 10.1111/j.1445-2197.2004.02951.x. [DOI] [PubMed] [Google Scholar]
- 268.Comarr AE. Pilonidal cysts and/or sinuses: primary closure with the wirebution retention technic. Am J Surg. 1959;97:328–330. doi: 10.1016/0002-9610(59)90310-1. [DOI] [PubMed] [Google Scholar]
- 269.Corsi, P. R., Corsi, R. D. C. C., Moura, L. F. R. A. D., Guerreiro, T. D. T. & Vasconcellos, L. P. D. Tratamento cirurgico do cisto pilonidal atraves de resseccao e fechamento primario com retalhos cutaneos. Revista brasileira de colo-proctologia (2004).
- 270.Cortese M, Benedetti Valentini G, Giacomini S. Personal experience in the treatment of pilonidal sinus. Minerva Chir. 1985;40:1137–1139. [PubMed] [Google Scholar]
- 271.Courtney SP, Merlin MJ. The use of fusidic acid gel in pilonidal abscess treatment: cure, recurrence and failure rates. Ann R Coll Surg Engl. 1986;68:170–171. [PMC free article] [PubMed] [Google Scholar]
- 272.Cruz J, Ram MD. Sacrococcygeal pilonidal sinus. Dis Colon Rectum. 1971;14:356–359. doi: 10.1007/BF02553422. [DOI] [PubMed] [Google Scholar]
- 273.Dalenback J, Magnusson O, Wedel N, Rimback G. Prospective follow-up after ambulatory plain midline excision of pilonidal sinus and primary suture under local anaesthesia–efficient, sufficient, and persistent. Colorectal Dis. 2004;6:488–493. doi: 10.1111/j.1463-1318.2004.00693.x. [DOI] [PubMed] [Google Scholar]
- 274.de Quinta Frutosa R, et al. Enfermedad pilonidal. Tratamiento por exéresis en bloque con cierre primario. Cir Esp. 2000;68:570–572. [Google Scholar]
- 275.Del Papa, M., Mobili, M., Attardo, S., Paolucci, G. & Braccioni, U. Radical excision and primary suture of pilonidal sinus: our experience. Ann Ital Chir63, 507–509, discussion 509–510 (1992). [PubMed]
- 276.Denkers D, Girona J. Der abszedierte Sinus pilonidalis der Steißbeinregion - Möglichkeiten der chirurgischen Versorgung. coloproctology. 1996;18:257–259. [Google Scholar]
- 277.Diana G, Muscarella F, Pepe D, Speciale A. Primary closure in the treatment of pilonidal sinus. Evaluation of immediate and remote results. MINERVA CHIR. 1986;41:765–767. [PubMed] [Google Scholar]
- 278.Doll D, et al. Does gentamycin affect long term recurrence rate in pilonidal sinus surgery? European Surgery. 2011;43:236–243. doi: 10.1007/s10353-011-0615-9. [DOI] [Google Scholar]
- 279.Duchateau J, De Mol J, Bostoen H, Allegaert W. Pilonidal sinus. Excision–marsupialization–phenolization? Acta Chir Belg. 1985;85:325–328. [PubMed] [Google Scholar]
- 280.El-Shaer WM. The modified gluteal sliding plication closure in the treatment of chronic pilonidal sinus. Int J Colorectal Dis. 2010;25:887–894. doi: 10.1007/s00384-010-0911-z. [DOI] [PubMed] [Google Scholar]
- 281.Emir S, Topuz O, Kanat BH, Bali I. Sinotomy technique versus surgical excision with primary closure technique in pilonidal sinus disease. Bosn J Basic Med Sci. 2014;14:263–267. doi: 10.17305/bjbms.2014.4.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 282.Evangelou G, Tiniakos G. Treatment of pilonidal sinus disease based on pathological observations. Int Surg. 1974;59:493–496. [PubMed] [Google Scholar]
- 283.Favre R, Delacroix P. Apropos of 1,110 Cases of Pilonidal Disease of Coccy-Perineal Localization. Mem Acad Chir (Paris) 1964;90:669–676. [PubMed] [Google Scholar]
- 284.Ferguson LK. Pilonidal Cysts: Treatment by Excision and Primary Suture in Ambulatory Patients. Ann Surg. 1935;101:469–477. doi: 10.1097/00000658-193501000-00050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 285.Ferguson LKM. P. M. Pilonidal Cysts: Excision and primary suture in ambulatory patients. Am J Surg. 1937;36:270–277. doi: 10.1016/S0002-9610(37)90829-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286.Filingeri V, Gravante G. Radiofrequency sinus excision. Dig. Surg. 2006;23:125. doi: 10.1159/000094136. [DOI] [PubMed] [Google Scholar]
- 287.Finestone EO. Technic of excision and primary closure of pilonidal sinus. N Y State J Med. 1952;52:1291–1294. [PubMed] [Google Scholar]
- 288.Frostad H. Sacral dermoidcysts. Especially with a view to their treatment. Acta chir scand. 1946;93:23. [PubMed] [Google Scholar]
- 289.Galati G, Sterpetti AV, Tartaglia E. Therapeutic approaches to patients with pilonidal sinus based on specific clinical characteristic. Eur J Plast Surg. 2012;35:595–598. doi: 10.1007/s00238-011-0662-2. [DOI] [Google Scholar]
- 290.Ghnnam W, Ghazy H, Saed B, Farid M. Limited excision and primary closure for pilonidal sinus. Egypt J Surg. 2009;28:43–47. [Google Scholar]
- 291.Gilani SN, et al. Excision and primary closure of pilonidal sinus disease: worthwhile option with an acceptable recurrence rate. Ir J Med Sci. 2011;180:173–176. doi: 10.1007/s11845-010-0532-0. [DOI] [PubMed] [Google Scholar]
- 292.Gipponi M, Reboa G, Testa T, Giannini G, Strada P. Tension-free primary closure with autologous platelet gel versus Vivostat- for the definitive treatment of chronic sacrococcygeal pilonidal disease. In Vivo. 2010;24:583–589. [PubMed] [Google Scholar]
- 293.Goldman B. Combined therapy for pilonidal (sacrococcygeal) cyst and sinus; roentgen epilation of operative field prior to surgical excision with primary closure. 1952;18:903–909. [PubMed] [Google Scholar]
- 294.Goswitz JT. Sacrococcygeal Pilonidal Sinus Disease. Treatment and Long-Term Follow-up in a Military Hospital Serving Combat-Ready Units. Arch Surg. 1965;90:890–892. doi: 10.1001/archsurg.1965.01320120092007. [DOI] [PubMed] [Google Scholar]
- 295.Grubnik, V. V. & Bakhar, G. A. The use of a laser in the surgical treatment of an epithelial coccygeal cyst. Klin.Khir. 23–25 (1993). [PubMed]
- 296.Hamilton JE, Cattanach LM. Comparative study of chemotherapies in the surgery of pilonidal sinus. Am J Surg. 1947;74:449–454. doi: 10.1016/0002-9610(47)90138-4. [DOI] [PubMed] [Google Scholar]
- 297.Hamilton JE, Stephens G, Claugus CE. Pilonidal Sinus: Excision and Primary Closure. Surgery. 1963;54:597–603. [PubMed] [Google Scholar]
- 298.Heifetz CJ. Pilonidal disease; a study of fifty consecutive cases treated successfully by excision and primary closure. Am J Surg. 1958;96:405–410. doi: 10.1016/0002-9610(58)90934-6. [DOI] [PubMed] [Google Scholar]
- 299.Holm J, Hulten L. Simple primary closure for pilonidal disease. Acta Chir Scand. 1970;136:537–540. [PubMed] [Google Scholar]
- 300.Hurwitt ES. Subphrenic abscess following primary closure for pilonidal sinus; report of a case. N Engl J Med. 1947;237:398. doi: 10.1056/NEJM194709112371104. [DOI] [PubMed] [Google Scholar]
- 301.Inan A, Surgit O, Sen M, Bozer M, Dener C. One day surgery for pilonidal disease. Bratisl Lek Listy. 2011;112:572–574. [PubMed] [Google Scholar]
- 302.Jandik J. Sinus pilonidalis - possibilities of surgical treatment. 2014;93:496–501. [PubMed] [Google Scholar]
- 303.Jarufe C, et al. Enfermedad pilonidal cronica sacrococcigea. Revista chilena de cirugía. 1999;51:66–71. [Google Scholar]
- 304.Kam BH. A simple surgical method of treating pilonidal sinus. Arch Chir Neerl. 1976;28:43–53. [PubMed] [Google Scholar]
- 305.Karaman K, et al. S-shaped wide excision with primary closure for extensive chronic pilonidal sinus disease. Case Rep Surg. 2014;2014:451869. doi: 10.1155/2014/451869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 306.Karimi E. Surgical treatment of pilonidal sinus. Ann Chir. 1980;34:507–510. [PubMed] [Google Scholar]
- 307.Kathel P, Gupta A, Gupta A, Shiju KS. A Case Report of Pilonidal Sinus Managed By Primary Closure and Review of Literature. Sch J Med Case Rep. 2014;2:532–535. [Google Scholar]
- 308.Kaya B, Uctum Y, Simsek A, Kutanis R. Primary closure in the treatment of pilonidal disease. An easy and effective method. Kolon Rektum Hast Derg. 2010;20:59–65. [Google Scholar]
- 309.Khaira HS, Brown JH. Excision and primary suture of pilonidal sinus. Ann R Coll Surg Engl. 1995;77:242–244. [PMC free article] [PubMed] [Google Scholar]
- 310.Khanzada TW, Samad A. Recurrence after excision and primary closure of pilonidal sinus. Pak. J. Med. Sci. 2007;23:375–379. [Google Scholar]
- 311.Klug W, Knoch HG, Holland-Moritz A. Sinus pilonidalis. Zeitschrift für ärztliche Fortbildung. 1984;78:711–714. [PubMed] [Google Scholar]
- 312.Kopp JA. Primary Closure of Pilonidal Sinus, Using a Muscle Fascia Graft. Arch Chir Neerl. 1964;16:151–160. [PubMed] [Google Scholar]
- 313.Kücükkartallar TT, Kücükkartallar A, Vatansev C, et al. The comparison of the results of different operation techniques for pilonidal sinus disease. Genel Tip Derg. 2007;17:95–97. [Google Scholar]
- 314.Laforet EG. Pilonidal sinus; a method of treatment by primary closure. Am J Surg. 1957;93:873–875. doi: 10.1016/0002-9610(57)90566-4. [DOI] [PubMed] [Google Scholar]
- 315.Larkin LC. Pilonidal cyst; analysis of 100 consecutive cases, emphasizing treatment by radical excision, primary closure and penicillin therapy. Surg Gynecol Obstet. 1946;82:694–704. [PubMed] [Google Scholar]
- 316.Larsen BB. Pilonidal cysts and sinuses; a technic for excision and primary closure. Ann Surg. 1946;123:1090–1100. doi: 10.1097/00000658-194606000-00012. [DOI] [PubMed] [Google Scholar]
- 317.Lee SL, Tejirian T, Abbas MA. Current management of adolescent pilonidal disease. J Pediatr Surg. 2008;43:1124–1127. doi: 10.1016/j.jpedsurg.2008.02.042. [DOI] [PubMed] [Google Scholar]
- 318.Lee HC, Ho YH, Seow CF, Eu KW, Nyam D. Pilonidal disease in Singapore: clinical features and management. Aust N Z J Surg. 2000;70:196–198. doi: 10.1046/j.1440-1622.2000.01785.x. [DOI] [PubMed] [Google Scholar]
- 319.Liboni NS, Fregnani CHTG. Preliminary results from 28 cases of pilonidal cyst treated by excision and primary closure of the wound, reinforced with support suturing. Einstein. 2007;5:148–152. [Google Scholar]
- 320.Limongelli P, et al. D-shape asymmetric and symmetric excision with primary closure in the treatment of sacrococcygeal pilonidal disease. Am J Surg. 2014;207:882–889. doi: 10.1016/j.amjsurg.2013.06.013. [DOI] [PubMed] [Google Scholar]
- 321.Mahdy T. Surgical treatment of the pilonidal disease: primary closure or flap reconstruction after excision. Dis Colon Rectum. 2008;51:1816–1822. doi: 10.1007/s10350-008-9436-8. [DOI] [PubMed] [Google Scholar]
- 322.Maniscalco L, Speranza G, Maniscalco A. The pilonidal sinus: Which managment? Chirurgia. 2001;14:81–83. [Google Scholar]
- 323.Mecchia P, Tonizzo CA, Flamia M. Pilonidal cysts and fistulas: radical excision “en bloc” and closure “per primam”. Minerva Chir. 1995;50:553–556. [PubMed] [Google Scholar]
- 324.Mentes O, et al. Management of pilonidal sinus disease with oblique excision and primary closure: results of 493 patients. Dis Colon Rectum. 2006;49:104–108. doi: 10.1007/s10350-005-0226-2. [DOI] [PubMed] [Google Scholar]
- 325.Michotey G, Brandone H, Helaine R. Apropos of a Series of 20 Cases of So-Called Pilonidal Sacrococcygeal Cysts. Mars Chir. 1963;15:383–389. [PubMed] [Google Scholar]
- 326.Miller JM, Ginsberg M, Lipin RJ, Long PH. Streptokinase and streptodornase in the treatment of pilonidal cysts. USArmed Forces Med J. 1951;2:1423–1429. [PubMed] [Google Scholar]
- 327.Milone, M. et al. Pilonidal sinus surgery: could we predict postoperative complications? part 2, 10.1111/iwj.12310 (2014). [DOI] [PMC free article] [PubMed]
- 328.Miocinovic M, Horzic M, Bunoza D. The treatment of pilonidal disease of the sacrococcygeal region by the method of limited excision and open wound healing. Acta Med Croatica. 2000;54:27–31. [PubMed] [Google Scholar]
- 329.Muller XM, Rothenbuhler JM, Frede KE. Sacro-coccygeal cyst: surgical techniques and results. Helv.Chir Acta. 1992;58:889–892. [PubMed] [Google Scholar]
- 330.Muzi MG, Milito G, Nigro C, Cadeddu F, Farinon AM. A modification of primary closure for the treatment of pilonidal disease in day-care setting. Colorectal Dis. 2009;11:84–88. doi: 10.1111/j.1463-1318.2008.01534.x. [DOI] [PubMed] [Google Scholar]
- 331.Muzi MG, et al. Long-term results of pilonidal sinus disease with modified primary closure: new technique on 450 patients. Am Surg. 2014;80:484–488. [PubMed] [Google Scholar]
- 332.Novotny GME. and Primary Closure of Pilonidal Sinus. A Critical Review of Forty-Five Cases. Med Serv J Can. 1964;20:352–354. [PubMed] [Google Scholar]
- 333.Obeid SA. A new technique for treatment of pilonidal sinus. Dis Colon Rectum. 1988;31:879–885. doi: 10.1007/BF02554854. [DOI] [PubMed] [Google Scholar]
- 334.Onder A, et al. Pilonidal sinus disease: risk factors for postoperative complications and recurrence. Int Surg. 2012;97:224–229. doi: 10.9738/CC86.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 335.Örhalmi J, Sotona O, Dusek T, Ferko A. Pilonidal sinus - possibilities surgical treatment. 2014;93:491–495. [PubMed] [Google Scholar]
- 336.Osmanoglu G, Yetisir F. Limberg flap is better for the surgical treatment of pilonidal sinus. Results of a 767 patients series with an at least five years follow-up period. Chirurgia (Bucur) 2011;106:491–494. [PubMed] [Google Scholar]
- 337.Palmieri B, Gozzi G, Rossi A. Pilonidal cysts: the state of the art and the authors’ personal experiences. Minerva Chir. 1994;49:377–382. [PubMed] [Google Scholar]
- 338.Pezzangora V, Averno V, Barina R. Treatment of fistulized pilonidal sinuses by phenol injection. Chir Ital. 1980;32:848–854. [PubMed] [Google Scholar]
- 339.Powell BC, Webb CB, Ewing JA, Smith DE. Gluteal Fascial Advancement for Pilonidal Cyst Disease: A 10-year Review. Am Surg. 2016;82:622–625. [PubMed] [Google Scholar]
- 340.Pozzi C, Tritapepe R. Healing of the operative wound after radical removal of the Sinus pilonidalis. MINERVA CHIR. 1989;44:2329–2332. [PubMed] [Google Scholar]
- 341.Qadir H, Nazir A, Aslam M, Rasool I. Primary repair without drain after limited excision of pilonidal sinus. Pak. J. Med. Health Sci. 2009;3:242. [Google Scholar]
- 342.Rainsbury RM, Southam JA. Radical surgery for pilonidal sinus. Ann R Coll Surg Engl. 1982;64:339–341. [PMC free article] [PubMed] [Google Scholar]
- 343.Rossi P, et al. The pilonidal sinus: its surgical treatment, our experience and a review of the literature. G Chir. 1993;14:120–123. [PubMed] [Google Scholar]
- 344.Ross RL. Recurrent pilonidal cyst and sinus; a plan of preoperative preparation, operation and postoperative care. Calif Med. 1956;85:183–186. [PMC free article] [PubMed] [Google Scholar]
- 345.Russell JL. A method of excision and primary closure of pilonidal cysts and sinuses. Can Med Assoc J. 1949;60:267–270. [PMC free article] [PubMed] [Google Scholar]
- 346.Sakr MFE, Sakr ME, Hamed HM, et al. Management of 634 Consecutive Patients with Chronic Pilonidal Sinus: A Nine-Year Experience of a Single Institute. mehr RR im Text. 2012;3:145–154. [Google Scholar]
- 347.Sarles JC, Sastre B, Delecourt P. Treatment of pilonidal cyst with radical excision and primary closure. Gastroenterol Clin Biol. 1977;1:929–932. [PubMed] [Google Scholar]
- 348.Saylam B, Balli DN, Duzgun AP, Ozer MV, Coskun F. Which surgical procedure offers the best treatment for pilonidal disease? Langenbecks Arch Surg. 2011;396:651–658. doi: 10.1007/s00423-011-0768-9. [DOI] [PubMed] [Google Scholar]
- 349.Schonk JW. Some aspects of the treatment of the pilonidal sinus. Arch Chir Neerl. 1971;23:297–302. [PubMed] [Google Scholar]
- 350.Serour F, Somekh E, Krutman B, Gorenstein A. Excision with primary closure and suction drainage for pilonidal sinus in adolescent patients. Pediatr Surg Int. 2002;18:159–161. doi: 10.1007/s003830100683. [DOI] [PubMed] [Google Scholar]
- 351.Shons AR, Mountjoy JR. Pilonidal disease: the case for excision with primary closure. Dis Colon Rectum. 1971;14:353–355. doi: 10.1007/BF02553421. [DOI] [PubMed] [Google Scholar]
- 352.Sias F, Licheri S, Secci L, Loi R, Daniele GM. Ambulatory treatment of pilonidal sinus. Chirurgia. 1994;7:639–642. [Google Scholar]
- 353.Siddiqui SS, Khan MA. Pilonidal sinus: Following the Aristotelian middle! Pak. J. Med. Sci. 2008;24:845–848. [Google Scholar]
- 354.Smith CM, Jones A, Dass D, Murthi G, Lindley R. Early experience of the use of fibrin sealant in the management of children with pilonidal sinus disease. J Pediatr Surg. 2015;50:320–322. doi: 10.1016/j.jpedsurg.2014.11.022. [DOI] [PubMed] [Google Scholar]
- 355.Stewart TJ, Bell M. The treatment of pilonidal sinus by phenol injection. Ulster Med J. 1969;38:167–171. [PMC free article] [PubMed] [Google Scholar]
- 356.Sutalo N, et al. The influence of dreinage in the treatment of chronic pilonidal sinus disease using midline closure. Psychiatr Danub. 2015;27:593–595. [PubMed] [Google Scholar]
- 357.Talu MY, Talu O, User Y, et al. Oblique excision with primary closure for the treatment of pilonidal sinus. Eur J Plast Surg. 1996;19:200–203. doi: 10.1007/BF00176279. [DOI] [Google Scholar]
- 358.Tejirian T, Lee JJ, Abbas MA. Is wide local excision for pilonidal disease still justified? Am Surg. 2007;73:1075–1078. [PubMed] [Google Scholar]
- 359.Toccaceli S, Persico Stella L, Diana M, Dandolo R, Negro P. Treatment of pilonidal sinus with primary closure. A twenty-year experience. Chir Ital. 2008;60:433–438. [PubMed] [Google Scholar]
- 360.Tocchi A, et al. Ambulatory closed surgery for the treatment of pilonidal sinus. G Chir. 2001;22:303–307. [PubMed] [Google Scholar]
- 361.Toydemir T, Peşluk O, Ermeç ED, Turhan AN. Comparison of the clinical outcomes of karydakis flap versus primary closure procedures in the surgical treatment of sacrococcygeal pilonidal sinus disease. Med. J. Bakirkoy. 2012;8:78–81. [Google Scholar]
- 362.Tritapepe R, Di Padova C. Excision and primary closure of pilonidal sinus using a drain for antiseptic wound flushing. Am J Surg. 2002;183:209–211. doi: 10.1016/S0002-9610(01)00876-5. [DOI] [PubMed] [Google Scholar]
- 363.Turner FP, O’Neil JW. Treatment of pilonidal sinus by primary closure; a seven-year study. AMA Arch Surg. 1959;78:398–405. doi: 10.1001/archsurg.1959.04320030042008. [DOI] [PubMed] [Google Scholar]
- 364.Verbeek HO, Bender J. Results of treatment of pilonidal sinus by block excision and primary suture. Arch Chir Neerl. 1974;26:311–318. [PubMed] [Google Scholar]
- 365.Virgillo G, Mendicino F, Costanzo A. Sinus pilonidalis. Brief review of literature and contribution to surgical therapy. 1975;27:1–40. [Google Scholar]
- 366.Vitale A, Barberis G, Maida P, Salzano A. Use of biological glue in the surgical treatment of sacrococcygeal fistulas. G.Chir. 1992;13:271–272. [PubMed] [Google Scholar]
- 367.Wani, M., Shah, M., Wani, K. & Malik, A. Excision and primary closure of sacrococcygeal pilonidal sinus using suction drain. International Surgery Journal, 837–840, 10.18203/2349-2902.isj20161158 (2016).
- 368.Washer JD, Smith DE, Carman ME, Blackhurst DW. Gluteal fascial advancement: an innovative, effective method for treating pilonidal disease. Am Surg. 2010;76:154–156. [PubMed] [Google Scholar]
- 369.Watters N, Macdonald IB. Marsupialization of pilonidal sinus and abscess: a report of 50 cases. Can Med Assoc J. 1958;79:236–240. [PMC free article] [PubMed] [Google Scholar]
- 370.Weeder SD. Pilonidal Cyst, it’s etiology and treatment. Ann Surg. 1933;98:385–393. doi: 10.1097/00000658-193309000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 371.Williams, R. S. A simple technique for successful primary closure after excision of pilonidal sinus disease. Ann R Coll Surg Engl72, 313–314, discussion 314–315 (1990). [PMC free article] [PubMed]
- 372.Yildiz T, Ilce Z, Kucuk A. Modified Limberg flap technique in the treatment of pilonidal sinus disease in teenagers. J Pediatr Surg. 2014;49:1610–1613. doi: 10.1016/j.jpedsurg.2014.06.011. [DOI] [PubMed] [Google Scholar]
- 373.Ziegler HR, Murphey DR, Jr., Meek EM. Pilonidal cyst and sinus; a new method of excision with primary closure. Surgery. 1946;20:690–703. [PubMed] [Google Scholar]
- 374.Karip AB, et al. Effect of Triclosan-Coated Suture and Antibiotic Prophylaxis on Infection and Recurrence after Karydakis Flap Repair for Pilonidal Disease: A Randomized Parallel-Arm Double-Blinded ClinicalTrial. Surg Infect (Larchmt) 2016;17:583–588. doi: 10.1089/sur.2015.207. [DOI] [PubMed] [Google Scholar]
- 375.Brezin DL, Brezin C, Lawrence J. Pilonidal cyst. Am J Surg. 1943;60:264–266. doi: 10.1016/S0002-9610(43)90662-2. [DOI] [Google Scholar]
- 376.Bulus H, Coskun A. Is Asymmetric excision primary closure at treatment of pylonidal sinus disease an appropriate choice? J. Clin. Anal. Med. 2011;2:79–81. doi: 10.4328/JCAM.279. [DOI] [Google Scholar]
- 377.Casten DF, Tan BY, Ayuyao A. A technique of radical excision of pilonidal disease with primary closure. Surgery. 1973;73:109–114. [PubMed] [Google Scholar]
- 378.Ciftci F, Abdurrahman I, Tosun M, Bas G. A new approach: oblique excision and primary closure in the management of acute pilonidal disease. Int J Clin Exp Med. 2014;7:5706–5710. [PMC free article] [PubMed] [Google Scholar]
- 379.De Nardi P, Gazzetta PG, Fiorentini G, Guarneri G. The cleft lift procedure for complex pilonidal disease. European Surgery. 2016;48:250–257. doi: 10.1007/s10353-016-0428-y. [DOI] [Google Scholar]
- 380.Docimo L, et al. Primary closure of decentred wounds in surgical treatment of pilonidal sinus. Chirurgia. 1998;11:239–244. [Google Scholar]
- 381.Eichfuss HP, Eichen R, Koch G, Eckert P. Primary closure of the sinus pilonidalis. Chirurg. 1978;49:124–126. [PubMed] [Google Scholar]
- 382.Greenberg R, Kashtan H, Skornik Y, Werbin N. Treatment of pilonidal sinus disease using fibrin glue as a sealant. Tech Coloproctol. 2004;8:95–98. doi: 10.1007/s10151-004-0063-7. [DOI] [PubMed] [Google Scholar]
- 383.Ibrahim AMRR. Oblique excision and primary closure of pilonidal sinus (sacrococcygeal) Trends Med. Res. 2012;7:62–69. doi: 10.3923/tmr.2012.62.69. [DOI] [Google Scholar]
- 384.Kim JK, Jeong JC, Lee JB, Jung KH, Bae BK. S-plasty for pilonidal disease: modified primary closure reducing tension. J Korean Surg Soc. 2012;82:63–69. doi: 10.4174/jkss.2012.82.2.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 385.Kitchen PR. Pilonidal sinus: experience with the Karydakis flap. Br J Surg. 1996;83:1452–1455. doi: 10.1002/bjs.1800831040. [DOI] [PubMed] [Google Scholar]
- 386.Maghsoudi H, Nezami N, Ghamari AA. Ambulatory treatment of chronic pilonidal sinuses with lateral incision and primary suture. Can J Surg. 2011;54:78–82. doi: 10.1503/cjs.026309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 387.Marzouk DM, Abou-Zeid AA, Antoniou A, Haji A, Benziger H. Sinus excision, release of coccycutaneous attachments and dermal-subcuticular closure (XRD procedure): a novel technique in flattening the natal cleft in pilonidal sinus treatment. Ann R Coll Surg Engl. 2008;90:371–376. doi: 10.1308/003588408X285955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 388.Saber A. Modified off-midline closure of pilonidal sinus disease. N Am J Med Sci. 2014;6:210–214. doi: 10.4103/1947-2714.132936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 389.Senapati A, Cripps NP, Flashman K, Thompson MR. Cleft closure for the treatment of pilonidal sinus disease. Colorectal Dis. 2011;13:333–336. doi: 10.1111/j.1463-1318.2009.02148.x. [DOI] [PubMed] [Google Scholar]
- 390.Zimmerman CE. Outpatient excision and primary closure of pilonidal cysts and sinuses. Am J Surg. 1978;136:640–642. doi: 10.1016/0002-9610(78)90326-4. [DOI] [PubMed] [Google Scholar]
- 391.Yildiz MK, et al. Karydakis flap procedure in patients with sacrococcygeal pilonidal sinus disease: experience of a single centre in Istanbul. ScientificWorldJournal. 2013;2013:807027. doi: 10.1155/2013/807027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 392.Arslan K, et al. Which flap method should be preferred for the treatment of pilonidal sinus? A prospective randomized study. Tech Coloproctol. 2014;18:29–37. doi: 10.1007/s10151-013-0982-2. [DOI] [PubMed] [Google Scholar]
- 393.Ates M, Dirican A, Sarac M, Aslan A, Colak C. Short and long-term results of the Karydakis flap versus the Limberg flap for treating pilonidal sinus disease: a prospective randomized study. Am J Surg. 2011;202:568–573. doi: 10.1016/j.amjsurg.2010.10.021. [DOI] [PubMed] [Google Scholar]
- 394.Akinci, O. F., Coskun, A. & Uzunkoy, A. Simple and effective surgical treatment of pilonidal sinus: asymmetric excision and primary closure using suction drain and subcuticular skin closure. Dis Colon Rectum43, 701–706, discussion 706–707 (2000). [DOI] [PubMed]
- 395.Al-Khayat H, et al. Risk factors for wound complication in pilonidal sinus procedures. J Am Coll Surg. 2007;205:439–444. doi: 10.1016/j.jamcollsurg.2007.04.034. [DOI] [PubMed] [Google Scholar]
- 396.Anderson JH, Yip CO, Nagabhushan JS, Connelly SJ. Day-case Karydakis flap for pilonidal sinus. Dis Colon Rectum. 2008;51:134–138. doi: 10.1007/s10350-007-9150-y. [DOI] [PubMed] [Google Scholar]
- 397.Anyanwu AC, Hossain S, Williams A, Montgomery AC. Karydakis operation for sacrococcygeal pilonidal sinus disease: experience in a district general hospital. Ann R Coll Surg Engl. 1998;80:197–199. [PMC free article] [PubMed] [Google Scholar]
- 398.Bannura C, et al. Ambulatory karydakis procedure for sacrococcygeal pilonidal disease. Revista Chilena de Cirugia. 2009;61:256–260. [Google Scholar]
- 399.Guillermo Bannura C. Sacrococcygeal pilonidal disease. risks factors and surgical options. Revista Chilena de Cirugia. 2011;63:527–533. doi: 10.4067/S0718-40262011000500016. [DOI] [Google Scholar]
- 400.Bascom, J. & Bascom, T. Failed pilonidal surgery: new paradigm and new operation leading to cures. Arch Surg137, 1146–1150; discussion 1151 (2002). [DOI] [PubMed]
- 401.Bascom, J. & Bascom, T. Utility of the cleft lift procedure in refractory pilonidal disease. Am J Surg193, 606–609; discussion 609, 10.1016/j.amjsurg.2007.01.008 (2007). [DOI] [PubMed]
- 402.Bascom JU. Repeat pilonidal operations. Am J Surg. 1987;154:118–122. doi: 10.1016/0002-9610(87)90300-X. [DOI] [PubMed] [Google Scholar]
- 403.Bertelsen CA. Cleft-lift operation for pilonidal sinuses under tumescent local anesthesia: a prospective cohort study of peri- and postoperative pain. Dis Colon Rectum. 2011;54:895–900. doi: 10.1007/DCR.0b013e31820ee852. [DOI] [PubMed] [Google Scholar]
- 404.Bertelsen CA, Jorgensen LN. Bascom’s operation for pilonidal fistula. Ugeskr Laeger. 2008;170:2313–2317. [PubMed] [Google Scholar]
- 405.Bessa SS. Results of the lateral advancing flap operation (modified Karydakis procedure) for the management of pilonidal sinus disease. Dis Colon Rectum. 2007;50:1935–1940. doi: 10.1007/s10350-007-9049-7. [DOI] [PubMed] [Google Scholar]
- 406.Bannura G. Karydakis operation for sacrococcygeal pilonidal sinus disease. Rev Chil Cir. 2005;57:340–344. [Google Scholar]
- 407.Bostanoglu S, Sakcak I, Avsar FM, Cosgun E, Hamamci EO. Comparison of Karydakis technique with Limberg Flap Procedure in Pilonidal Sinus Disease: Advantages of Karydakis technique. Pak. J. Med. Sci. 2010;26:773–777. [Google Scholar]
- 408.Buczacki S, Drage M, Wells A, Guy R. Sacrococcygeal pilonidal sinus disease. Colorectal Dis. 2009;11:657. doi: 10.1111/j.1463-1318.2009.01818.x. [DOI] [PubMed] [Google Scholar]
- 409.Cripps N, Evans J, Nordon I, Senapati A. Sacrococcygeal pilonidal sinus disease. Colorectal Dis. 2008;11:105–106. doi: 10.1111/j.1463-1318.2008.01741.x. [DOI] [PubMed] [Google Scholar]
- 410.Guner A, Cekic AB, Boz A, Turkyilmaz S, Kucuktulu U. A proposed staging system for chronic symptomatic pilonidal sinus disease and results in patients treated with stage-based approach. BMC Surg. 2016;16:18. doi: 10.1186/s12893-016-0134-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 411.Guner A, Ozkan OF, Kece C, Kesici S, Kucuktulu U. Modification of the Bascom cleft lift procedure for chronic pilonidal sinus: results in 141 patients. Colorectal Dis. 2013;15:e402–406. doi: 10.1111/codi.12243. [DOI] [PubMed] [Google Scholar]
- 412.Iesalnieks I, Deimel S, Zulke C, Schlitt HJ. Smoking increases the risk of pre- and postoperative complications in patients with pilonidal disease. patienten info. 2013;11:1001–1005. doi: 10.1111/ddg.12140. [DOI] [PubMed] [Google Scholar]
- 413.Immerman SC. Treatment of pilonidal disease using the Bascom ‘Cleft-Lift’ procedure. Am Surg. 2014;80:E49–50. [PubMed] [Google Scholar]
- 414.Khan MI, Jawed M, Bhura S, Shaikh U, Arif A. To evaluate the outcome of sacrococcygeal pilonidal sinus excision using karydakis technique. Med. Forum Monthly. 2014;25:57–59. [Google Scholar]
- 415.Iribarren B, et al. Comparison between Limberg and Karydakis flap for wound closure after pilonidal cyst resection. Revista Chilena de Cirugia. 2015;67:399–406. doi: 10.4067/S0718-40262015000400009. [DOI] [Google Scholar]
- 416.Kanat BH, et al. Comparison of early surgery (unroofing-curettage) and elective surgery (Karydakis flap technique) in pilonidal sinus abscess cases. Ulus Travma Acil Cerrahi Derg. 2014;20:366–370. doi: 10.5505/tjtes.2014.62547. [DOI] [PubMed] [Google Scholar]
- 417.Karaca T, et al. Comparison of short-term results of modified Karydakis flap and modified Limberg flap for pilonidal sinus surgery. Int J Surg. 2012;10:601–606. doi: 10.1016/j.ijsu.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 418.Karydakis GE. New approach to the problem of pilonidal sinus. Lancet. 1973;2:1414–1415. doi: 10.1016/S0140-6736(73)92803-1. [DOI] [PubMed] [Google Scholar]
- 419.Karydakis GE. Easy and successful treatment of pilonidal sinus after explanation of its causative process. Aust N Z J Surg. 1992;62:385–389. doi: 10.1111/j.1445-2197.1992.tb07208.x. [DOI] [PubMed] [Google Scholar]
- 420.Keshava A, Young CJ, Rickard MJ, Sinclair G. Karydakis flap repair for sacrococcygeal pilonidal sinus disease: how important is technique? ANZ J Surg. 2007;77:181–183. doi: 10.1111/j.1445-2197.2006.04003.x. [DOI] [PubMed] [Google Scholar]
- 421.Keshvari A, Fazeli MS, Kazemeni A, Meisami A, Nouri-Taromloo MK. Prospective evaluation of outcome of karydakis flap for sacrococcygeal pilonidal disease. Tehran Uni. Med. J. 2015;72:823–830. [Google Scholar]
- 422.Keshvari A, Keramati MR, Fazeli MS, Kazemeini A, Nouritaromlou MK. Risk factors for complications and recurrence after the Karydakis flap. J Surg Res. 2016;204:55–60. doi: 10.1016/j.jss.2016.04.035. [DOI] [PubMed] [Google Scholar]
- 423.Kitchen PRB. Pilonidal sinus: Excision and primary closure with a lateralised wound - the Karydakis operation. AUST. NEW ZEALAND J. SURG. 1982;52:302–305. doi: 10.1111/j.1445-2197.1982.tb05405.x. [DOI] [PubMed] [Google Scholar]
- 424.Kulacoglu H, Dener C, Tumer H, Aktimur R. Total subcutaneous fistulectomy combined with Karydakis flap for sacrococcygeal pilonidal disease with secondary perianal opening. Colorectal Dis. 2006;8:120–123. doi: 10.1111/j.1463-1318.2005.00872.x. [DOI] [PubMed] [Google Scholar]
- 425.Kumar NA, Sutradhar P. Karydakis procedure for sacrococcygeal pilonidal sinus disease: Our experience. daten nachtragen. 2014;47:402–406. doi: 10.4103/0970-0358.146615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 426.Larsson JC, Aliaga FD, Granero L, Cornet M. Tratamiento de la Enfermedad Pilonidal Crónica. Comparación de 3 Técnicas Quirúrgicas. Rev Argent Coloproct. 2014;25:64–70. [Google Scholar]
- 427.Martinez Sanz N, Pena Ros E, Sanchez Cifuentes A, Benavides Buleje JA, Albarracin Marin-Blazquez A. Modified Karydakis procedure for giant pilonidal sinus. Cir Esp. 2016;94:609–611. doi: 10.1016/j.ciresp.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 428.Melkonian T, et al. Short-and long-term results with Karydaki’s technique for sacrococcygeal pilonidal disease. Revista Chilena de Cirugia. 2013;65:25–29. doi: 10.4067/S0718-40262013000100005. [DOI] [Google Scholar]
- 429.Mohamed SJ, Kristensen BB, Lindgaard L, Bisgaard T. Acceptable effect of multimodal analgesic treatment after a Bascom cleft lift operation. Dan Med J. 2015;62:A4985. [PubMed] [Google Scholar]
- 430.Moran DC, Kavanagh DO, Adhmed I, Regan MC. Excision and primary closure using the Karydakis flap for the treatment of pilonidal disease: outcomes from a single institution. World J Surg. 2011;35:1803–1808. doi: 10.1007/s00268-011-1138-z. [DOI] [PubMed] [Google Scholar]
- 431.Ortega PM, et al. Is the cleft lift procedure for non-acute sacrococcygeal pilonidal disease a definitive treatment? Long-term outcomes in 74 patients. Surg Today. 2014;44:2318–2323. doi: 10.1007/s00595-014-0923-3. [DOI] [PubMed] [Google Scholar]
- 432.Patel H, Lee M, Bloom I, Allen-Mersh TG. Prolonged delay in healing after surgical treatment of pilonidal sinus is avoidable. Colorectal Dis. 1999;1:107–110. doi: 10.1046/j.1463-1318.1999.00030.x. [DOI] [PubMed] [Google Scholar]
- 433.Piskin T, et al. Orifice location guided excision and flap procedures for treatment of sacrococcygeal pilonidal disease. Adv. Clin. Exp. Med. 2011;20:481–488. [Google Scholar]
- 434.Ramzan DM, Khalid Mirza DM, Arif Ali DM. Pilonidal Sinus; Experience with Modified Karydakis Procedure Using Subcuticular Skin Closure. The Professional Medical Journal. 2016;23:1499–1504. doi: 10.17957/TPMJ/16.3602. [DOI] [Google Scholar]
- 435.Rushfeldt C, Bernstein A, Norderval S, Revhaug A. Introducing an asymmetric cleft lift technique as a uniform procedure for pilonidal sinus surgery. Scand J Surg. 2008;97:77–81. doi: 10.1177/145749690809700111. [DOI] [PubMed] [Google Scholar]
- 436.Sakr M, El-Hammadi H, Moussa M, Arafa S, Rasheed M. The effect of obesity on the results of Karydakis technique for the management of chronic pilonidal sinus. Int J Colorectal Dis. 2003;18:36–39. doi: 10.1007/s00384-002-0407-6. [DOI] [PubMed] [Google Scholar]
- 437.Senapati, A., Cripps, N. P., Flashman, K. & Thompson, M. R. Cleft Closure for the Treatment of Pilonidal Sinus Disease. Colorectal Dis. (2009). [DOI] [PubMed]
- 438.Sit M, Aktas G, Yilmaz EE. Comparison of the three surgical flap techniques in pilonidal sinus surgery. Am Surg. 2013;79:1263–1268. [PubMed] [Google Scholar]
- 439.Sözen S, et al. Comparison between Karydakis flap repair and Limberg flap for surgical treatment of sacrococcygeal pilonidal sinus (short term results) Turk. J. Surg. 2010;26:153–156. doi: 10.5097/1300-0705.UCD.609-10.01. [DOI] [Google Scholar]
- 440.Tezel E, Bostanci H, Anadol AZ, Kurukahvecioglu O. Cleft lift procedure for sacrococcygeal pilonidal disease. Dis Colon Rectum. 2009;52:135–139. doi: 10.1007/DCR.0b013e31819734f8. [DOI] [PubMed] [Google Scholar]
- 441.Theodoropoulos GE, Vlahos K, Lazaris AC, Tahteris E, Panoussopoulos D. Modified Bascom’s asymmetric midgluteal cleft closure technique for recurrent pilonidal disease: early experience in a military hospital. Dis Colon Rectum. 2003;46:1286–1291. doi: 10.1007/s10350-004-6729-4. [DOI] [PubMed] [Google Scholar]
- 442.Altinli E, Koksal N, Onur E, Celik A, Sumer A. Impact of fibrin sealant on Limberg flap technique: results of a randomized controlled trial. Tech Coloproctol. 2007;11:22–25. doi: 10.1007/s10151-007-0320-7. [DOI] [PubMed] [Google Scholar]
- 443.Cihan A, et al. Superiority of asymmetric modified Limberg flap for surgical treatment of pilonidal disease. Dis Colon Rectum. 2006;49:244–249. doi: 10.1007/s10350-005-0253-z. [DOI] [PubMed] [Google Scholar]
- 444.Aithal SK, Rajan CS, Reddy N. Limberg flap for sacrococcygeal pilonidal sinus a safe and sound procedure. Indian J Surg. 2013;75:298–301. doi: 10.1007/s12262-012-0489-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 445.Akan K, et al. Comparison of surgical Limberg flap technique and crystallized phenol application in the treatment of pilonidal sinus disease: a retrospective study. Ulus Cerrahi Derg. 2013;29:162–166. doi: 10.5152/UCD.2013.2457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 446.Akin M, et al. Rhomboid excision and Limberg flap for managing pilonidal sinus: long-term results in 411 patients. Colorectal Dis. 2008;10:945–948. doi: 10.1111/j.1463-1318.2008.01563.x. [DOI] [PubMed] [Google Scholar]
- 447.Akin M, et al. Comparison of the classic Limberg flap and modified Limberg flap in the treatment of pilonidal sinus disease: a retrospective analysis of 416 patients. Surg Today. 2010;40:757–762. doi: 10.1007/s00595-008-4098-7. [DOI] [PubMed] [Google Scholar]
- 448.Al-Haifi MB, et al. Rhomboid flap - A primary cure for pilonidal sinus. Kuwait Med. J. 2010;42:282–285. [Google Scholar]
- 449.Altintoprak F, et al. Comparision of the Limberg flap with the V-Y flap technique in the treatment of pilonidal disease. J Korean Surg Soc. 2013;85:63–67. doi: 10.4174/jkss.2013.85.2.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 450.Altintoprak F, et al. Retrospective review of pilonidal sinus patients with early discharge after Limberg flap procedure. Int Surg. 2014;99:28–34. doi: 10.9738/INTSURG-D-13-00150.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 451.Ardelt M, et al. Sequential intervention with primary excision and Limberg plastic surgery procedure for treatment of sacrococcygeal pilonidal sinus: Results of a pilot study. Chirurg. 2015;86:771–775. doi: 10.1007/s00104-014-2963-z. [DOI] [PubMed] [Google Scholar]
- 452.Azab AS, Kamal MS, Saad RA, Abou al Atta KA, Ali NA. Radical cure of pilonidal sinus by a transposition rhomboid flap. Br J Surg. 1984;71:154–155. doi: 10.1002/bjs.1800710227. [DOI] [PubMed] [Google Scholar]
- 453.Azab AS, Kamal MS, el Bassyoni F. The rationale of using the rhomboid fasciocutaneous transposition flap for the radical cure of pilonidal sinus. J Dermatol Surg Oncol. 1986;12:1295–1299. doi: 10.1111/j.1524-4725.1986.tb01070.x. [DOI] [PubMed] [Google Scholar]
- 454.Arumugam PJ, Chandrasekaran TV, Morgan AR, Beynon J, Carr ND. The rhomboid flap for pilonidal disease. Colorectal Dis. 2003;5:218–221. doi: 10.1046/j.1463-1318.2003.00435.x. [DOI] [PubMed] [Google Scholar]
- 455.Aslam MN, Shoaib S, Choudhry AM. Use of Limberg flap for pilonidal sinus–a viable option. J Ayub Med Coll Abbottabad. 2009;21:31–33. [PubMed] [Google Scholar]
- 456.Azizi R, Alemrajabi M, Naderan M, Shoar S. Efficacy of modified Limberg flap in surgical treatment of infected pilonidal abscess: a case–control study. European Surgery. 2014;46:144–147. doi: 10.1007/s10353-014-0273-9. [DOI] [Google Scholar]
- 457.Bayhan Z, et al. Crystallized phenol application and modified Limberg flap procedure in treatment of pilonidal sinus disease: A comparative retrospective study. Asian J Surg. 2016;39:172–177. doi: 10.1016/j.asjsur.2015.12.007. [DOI] [PubMed] [Google Scholar]
- 458.Behdad A, Hosseinpoor M. Z-plasty for the treatment of residual cavity after pilonidal sinus excision. Medical Journal of the Islamic Republic of Iran. 2001;14:317–319. [Google Scholar]
- 459.Bose B, Candy J. Radical cure of pilonidal sinus by Z-plasty. Am J Surg. 1970;120:783–786. doi: 10.1016/S0002-9610(70)80049-6. [DOI] [PubMed] [Google Scholar]
- 460.Bozkurt MK, Tezel E. Management of pilonidal sinus with the Limberg flap. Dis Colon Rectum. 1998;41:775–777. doi: 10.1007/BF02236268. [DOI] [PubMed] [Google Scholar]
- 461.Casula G, Uccheddu A, Figus M. Long term results of the Z-plasty method in the treatment of pilonidal sinus. Minerva Chir. 1983;38:617–620. [PubMed] [Google Scholar]
- 462.Cervelli V, et al. Plastic surgery by the Limberg-Dufourmentel method in the treatment of a pilonidal sinus. The anatomicosurgical considerations and an emblematic case. Minerva Chir. 1997;52:659–662. [PubMed] [Google Scholar]
- 463.Cubukcu A, et al. The role of obesity on the recurrence of pilonidal sinus disease in patients, who were treated by excision and Limberg flap transposition. Int J Colorectal Dis. 2000;15:173–175. doi: 10.1007/s003840000212. [DOI] [PubMed] [Google Scholar]
- 464.Daphan C, Tekelioglu MH, Sayilgan C. Limberg flap repair for pilonidal sinus disease. Dis Colon Rectum. 2004;47:233–237. doi: 10.1007/s10350-003-0037-2. [DOI] [PubMed] [Google Scholar]
- 465.Darwish AM, Hassanin A. Reconstruction following excision of sacrococcygeal pilonidal sinus with a perforator-based fasciocutaneous Limberg flap. J Plast Reconstr Aesthet Surg. 2010;63:1176–1180. doi: 10.1016/j.bjps.2009.05.051. [DOI] [PubMed] [Google Scholar]
- 466.Do Amaral Braga J, Jr., Haertel Gomes N. Intergluteal dermoid cyst. REV. BRAS. MED. 1973;30:543–545. [Google Scholar]
- 467.Dogra S, Rao PP. Z-Plasty a Rational and Effective Technique for Pilonidal Sinus. Hellenic Journal of Surgery. 2014;86:208–211. doi: 10.1007/s13126-014-0131-z. [DOI] [Google Scholar]
- 468.El-Khadrawy O, Hashish M, Ismail K, Shalaby H. Outcome of the rhomboid flap for recurrent pilonidal disease. World J Surg. 2009;33:1064–1068. doi: 10.1007/s00268-009-9920-x. [DOI] [PubMed] [Google Scholar]
- 469.El-Tawil S, Carapeti E. Use of a double rhomboid transposition flap in the treatment of extensive complex pilonidal sinus disease. Colorectal Dis. 2009;11:313–317. doi: 10.1111/j.1463-1318.2008.01596.x. [DOI] [PubMed] [Google Scholar]
- 470.Eryilmaz R, Sahin M, Alimoglu O, Dasiran F. Surgical treatment of sacrococcygeal pilonidal sinus with the Limberg transposition flap. Surgery. 2003;134:745–749. doi: 10.1016/S0039-6060(03)00163-6. [DOI] [PubMed] [Google Scholar]
- 471.Fahim M, et al. Limberg FLAP Reconstruction for Pilonidal Sinus Disease: An Experience. Ann. Pak. Inst. Med. Sci. 2013;9:215–218. [Google Scholar]
- 472.Faux W, Pillai SC, Gold DM. Limberg flap for pilonidal disease: the “no-protractor” approach, 3 steps to success. Tech Coloproctol. 2005;9:153–155. doi: 10.1007/s10151-005-0216-3. [DOI] [PubMed] [Google Scholar]
- 473.Ferreira Montero V, Garcia Fabian AP, Martinez Laganga A, Perez Ruiz L. Rhombic plastia in the form of an ‘L’ for treating pilonidal cysts. Cir. Esp. 1977;31:153–158. [Google Scholar]
- 474.Friedl PG, Rappold EM, Jager C. Effective and minimally painful surgery of pilonidal sinus - asymmetric transposition flap according to Dufourmentel. patienten info. 2011;9:333–335. doi: 10.1111/j.1610-0387.2011.07662.x. [DOI] [PubMed] [Google Scholar]
- 475.Gwynn BR. Use of the rhomboid flap in pilonidal sinus. Ann R Coll Surg Engl. 1986;68:40–41. [PMC free article] [PubMed] [Google Scholar]
- 476.Hasse FM, Rademacher C, Bingham K, Lohlein D. The Dufourmentel flap-plasty for treatment of chronic pilonidal sinus. Chirurg. 1998;69:663–666. doi: 10.1007/s001040050472. [DOI] [PubMed] [Google Scholar]
- 477.Hegele A, Strombach FJ, Schonbach F. Reconstructive surgical therapy of infected pilonidal sinus. Chirurg. 2003;74:749–752. doi: 10.1007/s00104-003-0657-z. [DOI] [PubMed] [Google Scholar]
- 478.Jaschke CW, Mahrlein R, Mangold G. Results of the Limberg transposition flap in the treatment of pilonidal sinus. Zentralbl Chir. 2002;127:712–715. doi: 10.1055/s-2002-33579. [DOI] [PubMed] [Google Scholar]
- 479.Jimenez Romero C, Alcalde M, Martin F, Pulido A, Rico P. Treatment of pilonidal sinus by excision and rhomboid flap. Int J Colorectal Dis. 1990;5:200–202. doi: 10.1007/BF00303275. [DOI] [PubMed] [Google Scholar]
- 480.Johnson HA. On treatment of pilonidal sinus and cysts by conservative excision and W-plasty closure. Plast Reconstr Surg. 1978;62:107–108. doi: 10.1097/00006534-197807000-00020. [DOI] [PubMed] [Google Scholar]
- 481.Jonas J, Blaich S, Bahr R. Surgery of pilonidal sinus using the Limberg flap. Zentralbl Chir. 2000;125:976–981. doi: 10.1055/s-2000-10076. [DOI] [PubMed] [Google Scholar]
- 482.Kapan M, Kapan S, Pekmezci S, Durgun V. Sacrococcygeal pilonidal sinus disease with Limberg flap repair. Tech Coloproctol. 2002;6:27–32. doi: 10.1007/s101510200005. [DOI] [PubMed] [Google Scholar]
- 483.Kapp T, Zadnikar M, Hahnloser D, Soll C, Hetzer FH. New concept in the treatment of the pilonidal sinus. Praxis (Bern 1994) 2007;96:1171–1176. doi: 10.1024/1661-8157.96.31.1171. [DOI] [PubMed] [Google Scholar]
- 484.Karaca AS, Ali R, Capar M, Karaca S. Comparison of Limberg flap and excision and primary closure of pilonidal sinus disease, in terms of quality of life and complications. J Korean Surg Soc. 2013;85:236–239. doi: 10.4174/jkss.2013.85.5.236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 485.Karakas, B. R. et al. Is the lateralization distance important in terms in patients undergoing the modified Limberg flap procedure for treatment of pilonidal sinus? Tech.Coloproctol. (2014). [DOI] [PubMed]
- 486.Karakas BR. Comparison of Z-plasty, limberg flap, and asymmetric modified Limberg flap techniques for the pilonidal sinus treatment: review of literature. Acta Chir Iugosl. 2013;60:31–37. doi: 10.2298/ACI1303031K. [DOI] [PubMed] [Google Scholar]
- 487.Katsoulis IE, Hibberts F, Carapeti EA. Outcome of treatment of primary and recurrent pilonidal sinuses with the Limberg flap. Surgeon. 2006;4(7–10):62. doi: 10.1016/s1479-666x(06)80014-4. [DOI] [PubMed] [Google Scholar]
- 488.Kaya B, et al. Modified Limberg transposition flap in the treatment of pilonidal sinus disease. Tech Coloproctol. 2012;16:55–59. doi: 10.1007/s10151-011-0799-9. [DOI] [PubMed] [Google Scholar]
- 489.Kicka M, Toporcer T, Radonak J. Pilonidal sinus–a classical plastic procedure according to Limberg (Limberg flap procedure) or its modified version? 2011;90:482–487. [PubMed] [Google Scholar]
- 490.Kushwaha R, El-Tawil S, Hibberts F, Katsoulis IE, Carapeti E. Treatment of complex primary and recurrent pilonidal sinus with a Rhomboid Transposition Flap. Br J Surg. 2006;93:1–104. [Google Scholar]
- 491.Lahooti M, Taheri PA, Nezami BG, Assa S. Sacrococcygeal pilonidal sinus treated by a new fascio-cutaneous flap. Dis Colon Rectum. 2008;51:588–592. doi: 10.1007/s10350-008-9211-x. [DOI] [PubMed] [Google Scholar]
- 492.Lamke LO, Larsson J, Nylen B. Treatment of pilonidal sinus by radical excision and reconstruction by rotation flap surgery of Z-plasty technique. Scand J Plast Reconstr Surg. 1979;13:351–353. doi: 10.3109/02844317909013081. [DOI] [PubMed] [Google Scholar]
- 493.Lauterbach HH, Konrad U. Zweiphasenkonzept zur Therapie des infizierten Sinus pilonidalis. Chir Praxis. 1999;55:623–628. [Google Scholar]
- 494.Lieto E, et al. Dufourmentel rhomboid flap in the radical treatment of primary and recurrent sacrococcygeal pilonidal disease. Dis Colon Rectum. 2010;53:1061–1068. doi: 10.1007/DCR.0b013e3181defd25. [DOI] [PubMed] [Google Scholar]
- 495.Lodha SC. Treatment of pilonidal sinus by ‘Z’ plasty. J Indian Med Assoc. 1974;62:307–309. [PubMed] [Google Scholar]
- 496.Madbouly KM. Day-case Limberg flap for recurrent pilonidal sinus: does obesity complicate the issue? Am Surg. 2010;76:995–999. [PubMed] [Google Scholar]
- 497.Mansoory A, Dickson D. Z-plasty for treatment of disease of the pilonidal sinus. Surg Gynecol Obstet. 1982;155:409–411. [PubMed] [Google Scholar]
- 498.Manterola C, Barroso M, Araya JC, Fonseca L. Pilonidal disease: 25 cases treated by the Dufourmentel technique. Dis Colon Rectum. 1991;34:649–652. doi: 10.1007/BF02050344. [DOI] [PubMed] [Google Scholar]
- 499.McDermott FT. Pilonidal sinus treated by Z-plasty. Aust N Z J Surg. 1967;37:64–69. doi: 10.1111/j.1445-2197.1967.tb06989.x. [DOI] [PubMed] [Google Scholar]
- 500.Mentes O, Bagci M, Bilgin T, Ozgul O, Ozdemir M. Limberg flap procedure for pilonidal sinus disease: results of 353 patients. Langenbecks Arch Surg. 2008;393:185–189. doi: 10.1007/s00423-007-0227-9. [DOI] [PubMed] [Google Scholar]
- 501.Mentes BB, et al. Modified Limberg transposition flap for sacrococcygeal pilonidal sinus. Surg Today. 2004;34:419–423. doi: 10.1007/s00595-003-2725-x. [DOI] [PubMed] [Google Scholar]
- 502.Middleton MD. Treatment of pilonidal sinus by Z-plasty. Br J Surg. 1968;55:516–518. doi: 10.1002/bjs.1800550706. [DOI] [PubMed] [Google Scholar]
- 503.Milito G, Cortese F, Casciani CU. Rhomboid flap procedure for pilonidal sinus: results from 67 cases. Int J Colorectal Dis. 1998;13:113–115. doi: 10.1007/s003840050146. [DOI] [PubMed] [Google Scholar]
- 504.Milito G, et al. Modified Limberg’s transposition flap for pilonidal sinus. Long term follow up of 216 cases. Ann Ital Chir. 2007;78:227–231. [PubMed] [Google Scholar]
- 505.Misiakos EP, et al. Limberg flap reconstruction for the treatment of pilonidal sinus disease. Chirurgia (Bucur) 2006;101:513–517. [PubMed] [Google Scholar]
- 506.Monro RS, McDermott FT. The Elimination of Causal Factors in Pilonidal Sinus Treated by Z-Plasty. Br J Surg. 1965;52:177–181. doi: 10.1002/bjs.1800520306. [DOI] [PubMed] [Google Scholar]
- 507.Moosavi SR, Kharazm P, Vaghardoost R. Surgical treatment of pilonidal sinus with a fasciocutaneous rotation flap based on an inferior pedicle. Scand J Plast Reconstr Surg Hand Surg. 2006;40:281–283. doi: 10.1080/02844310600869811. [DOI] [PubMed] [Google Scholar]
- 508.Müller K, et al. Prospective analysis of cosmesis, morbidity, and patient satisfaction following Limberg flap for the treatment of sacrococcygeal pilonidal sinus. Dis Colon Rectum. 2011;54:487–494. doi: 10.1007/DCR.0b013e3182051d96. [DOI] [PubMed] [Google Scholar]
- 509.Mutaf M, Temel M, Koc MN. A New Surgical Technique for Closure of Pilonidal Sinus Defects: Triangular Closure Technique. Med Sci Monit. 2017;23:1033–1042. doi: 10.12659/MSM.899879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 510.Naveen N, Kumar MK, Babu KR, Dhanraj P. Tandem rhomboid flap repair: a new technique in treatment of extensive pilonidal disease of the natal cleft. J Clin Diagn Res. 2014;8:ND03-04. doi: 10.7860/JCDR/2014/9283.4824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 511.Omer Y, Hayrettin D, Murat C, Mustafa Y, Evren D. Comparison of modified limberg flap and modified elliptical rotation flap for pilonidal sinus surgery: a retrospective cohort study. Int J Surg. 2015;16:74–77. doi: 10.1016/j.ijsu.2015.02.024. [DOI] [PubMed] [Google Scholar]
- 512.Öz, B. et al. A comparison of surgical outcome of fasciocutaneous V-Y advancement flap and Limberg transposition flap for recurrent sacrococcygeal pilonidal sinus disease. Asian J Surg, 6, 10.1016/j.asjsur.2015.10.002 (2015). [DOI] [PubMed]
- 513.Ozgultekin R, et al. Therapy of pilonidal sinus with the Limberg transposition flap. Chirurg. 1995;66:192–195. [PubMed] [Google Scholar]
- 514.Rabbani, S. et al. Rhomboid excision with limberg transposition flap in the management of sacrococcygeal pilonidal sinus - a reliable surgical technique. Pakistan J of Medical and Health Sci8 (2014).
- 515.Rao J, Deora H, Mandia R. A Retrospective Study of 40 Cases of Pilonidal Sinus with Excision of Tract and Z-plasty as Treatment of Choice for Both Primary and Recurrent Cases. Indian J Surg. 2013;77:691–693. doi: 10.1007/s12262-013-0983-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 516.Raza MW, et al. Limberg flap for pilonidal sinus. J Rawal Med coll. 2012;16:132–134. [Google Scholar]
- 517.Rojas Gorigoytia GR. Pilonidal sinuses. Treatment using the L.L.L. plasty. Cir. Plast. Ibero-Latinoam. 1981;7:245–252. [Google Scholar]
- 518.Romero CJ, Alcalde M, Martin F, Pulido A, Rico P. Treatment of pilonidal sinus by excision and rhomboid flap. Int J Colorect Dis. 1990;5:200–202. doi: 10.1007/BF00303275. [DOI] [PubMed] [Google Scholar]
- 519.Roth RF, Moorman WL. Treatment of pilonidal sinus and cyst by conservative excision and W-plasty closure. Plast Reconstr Surg. 1977;60:412–415. [PubMed] [Google Scholar]
- 520.Sabiani P, Le Treut YP, Bouloudnine G, Maillet B, Bricot R. Le traitement de la maladie pilonidale par la technique d’exérèse-plastie “LLL”. A propos de 27 cas. Annales de gastroentérologie et d’hépatologie. 1985;21:287–290. [PubMed] [Google Scholar]
- 521.Sabuncuoglu MZ, et al. Eyedrop-shaped, modified Limberg transposition flap in the treatment of pilonidal sinus disease. Asian J Surg. 2015;38:161–167. doi: 10.1016/j.asjsur.2015.03.007. [DOI] [PubMed] [Google Scholar]
- 522.Sellés R, et al. Complete excision and marsupialization of chronic pilonidal sacrococcygeal sinus: The ideal technique? Cir. Esp. 2002;72:92–94. doi: 10.1016/S0009-739X(02)72016-2. [DOI] [Google Scholar]
- 523.Shabir F, Khan BA, Mian MA. Rhomboid excision with Limberg flap a novel treatment for sacrococcygeal pilonidal sinus. Pak. J. Med. Health Sci. 2014;8:687–690. [Google Scholar]
- 524.Sharma PP. Multiple Z-plasty in pilonidal sinus–a new technique under local anesthesia. World J Surg. 2006;30:2261–2265. doi: 10.1007/s00268-005-0632-6. [DOI] [PubMed] [Google Scholar]
- 525.Singh R, Pavithran NM. Adipo-fascio-cutaneous flaps in the treatment of pilonidal sinus: experience with 50 cases. Asian J Surg. 2005;28:198–201. doi: 10.1016/S1015-9584(09)60343-2. [DOI] [PubMed] [Google Scholar]
- 526.Spychala A, Murawa D. The Limberg flap procedure in the treatment of pilonidal cyst disease of the sacrum - initial report. Pol Przegl Chir. 2014;86:257–262. doi: 10.2478/pjs-2014-0046. [DOI] [PubMed] [Google Scholar]
- 527.Tardu, A., Haşlak, A., Özçinar, B. & Başak, F. Comparison of Limberg and Dufourmentel flap in surgical treatment of pilonidal sinus disease. Turk. J. Surg. 27, 35–40, 10.5097/1300-0705.UCD.659-11.04
- 528.Tekin A. Pilonidal sinus: experience with the Limberg flap. Colorectal Dis. 1999;1:29–33. doi: 10.1046/j.1463-1318.1999.00007.x. [DOI] [PubMed] [Google Scholar]
- 529.Topgul K, Ozdemir E, Kilic K, Gokbayir H, Ferahkose Z. Long-term results of limberg flap procedure for treatment of pilonidal sinus: a report of 200 cases. Dis Colon Rectum. 2003;46:1545–1548. doi: 10.1007/s10350-004-6811-y. [DOI] [PubMed] [Google Scholar]
- 530.Toubanakis G. Treatment of pilonidal sinus disease with the Z-plasty procedure (modified) Am Surg. 1986;52:611–612. [PubMed] [Google Scholar]
- 531.Tschudi J, Ris HB. Morbidity of Z-plasty in the treatment of pilonidal sinus. Chirurg. 1988;59:486–490. [PubMed] [Google Scholar]
- 532.Unalp HR, Derici H, Kamer E, Nazli O, Onal MA. Lower recurrence rate for Limberg vs. V-Y flap for pilonidal sinus. Dis Colon Rectum. 2007;50:1436–1444. doi: 10.1007/s10350-007-0276-8. [DOI] [PubMed] [Google Scholar]
- 533.Urhan MK, Kucukel F, Topgul K, Ozer I, Sari S. Rhomboid excision and Limberg flap for managing pilonidal sinus: results of 102 cases. Dis Colon Rectum. 2002;45:656–659. doi: 10.1007/s10350-004-6263-4. [DOI] [PubMed] [Google Scholar]
- 534.Wroński K, Bocian R, Pakuła D. Surgical treatment of pilonidal sinus by means of Z-plasty - Case report and literature review. Prz. Dermatol. 2010;97:329–334. [Google Scholar]
- 535.Yamout SZ, et al. Early experience with the use of rhomboid excision and Limberg flap in 16 adolescents with pilonidal disease. J Pediatr Surg. 2009;44:1586–1590. doi: 10.1016/j.jpedsurg.2008.11.033. [DOI] [PubMed] [Google Scholar]
- 536.Yeo MS, Shim TW, Cheong WK, Leong AP, Lee SJ. Simultaneous laser depilation and perforator-based fasciocutaneous limberg flap for pilonidal sinus reconstruction. J Plast Reconstr Aesthet Surg. 2010;63:e798–800. doi: 10.1016/j.bjps.2010.06.032. [DOI] [PubMed] [Google Scholar]
- 537.Yildar M, Cavdar F, Yildiz MK. The evaluation of a modified Dufourmentel flap after S-type excision for pilonidal sinus disease. ScientificWorldJournal. 2013;2013:459147. doi: 10.1155/2013/459147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 538.Yildar M, Cavdar F. Comparison of the Limberg flap and bilateral gluteus maximus advancing flap following oblique excision for the treatment of pilonidal sinus disease. Surg Today. 2014;44:1828–1833. doi: 10.1007/s00595-013-0764-5. [DOI] [PubMed] [Google Scholar]
- 539.Yilmaz S, Kirimlioglu V, Katz D. Role of simple V-Y advancement flap in the treatment of complicated pilonidal sinus. Eur.J Surg. 2000;166:269. doi: 10.1080/110241500750009410. [DOI] [PubMed] [Google Scholar]
- 540.Yoldas T, et al. Recurrent pilonidal sinus: lay open or flap closure, does it differ? Int Surg. 2013;98:319–323. doi: 10.9738/INTSURG-D-13-00081.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 541.Sood SC, Green JR, Parui R. Results of various operations for sacrococcygeal pilonidal disease. Plast Reconstr Surg. 1975;56:559–566. doi: 10.1097/00006534-197511000-00014. [DOI] [PubMed] [Google Scholar]
- 542.Berkem H, et al. V-Y advancement flap closures for complicated pilonidal sinus disease. Int J Colorectal Dis. 2005;20:343–348. doi: 10.1007/s00384-004-0699-9. [DOI] [PubMed] [Google Scholar]
- 543.Awad MM, Saad KM, Tolba AM, Gharib OH. A simple novel technique for closure of simple and complex pilonidal sinus with either simple (tongue-shaped) or bilobed rotation flap. daten nachtragen. 2007;44:47–50. [Google Scholar]
- 544.Ay A, Aytekin O, Aytekin A. Interdigitating Fasciocutaneous Gluteal V-Y Advancement Flaps for Reconstruction of Sacral Defects. Ann. Plast. Surg. 2003;50:636–638. doi: 10.1097/01.SAP.0000054241.94281.D2. [DOI] [PubMed] [Google Scholar]
- 545.Basterzi Y, et al. Reconstruction of extensive pilonidal sinus defects with the use of S-GAP flaps. Ann Plast Surg. 2008;61:197–200. doi: 10.1097/SAP.0b013e3181587a06. [DOI] [PubMed] [Google Scholar]
- 546.Behan FC, Rozen WM, Tan S. Yin-Yang flaps: the mathematics of two keystone island flaps for reconstructing increasingly large defects. ANZ J. Surg. 2011;81:574–575. doi: 10.1111/j.1445-2197.2011.05814.x. [DOI] [PubMed] [Google Scholar]
- 547.Boyce DE, Shokrollahi K. Reconstructive surgery. BMJ (Clinical research ed.) 2006;332:710–712. doi: 10.1136/bmj.332.7543.710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 548.Cherry JK. Primary closure of pilonidal sinus. Surg Gynecol Obstet. 1968;126:1263–1269. [PubMed] [Google Scholar]
- 549.Demiryilmaz I, et al. Application of fasciocutaneous V-Y advancement flap in primary and recurrent sacrococcygeal pilonidal sinus disease. Med Sci Monit. 2014;20:1263–1266. doi: 10.12659/MSM.890752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 550.Dilek ON, Bekerecioglu M. Role of simple V-Y advancement flap in the treatment of complicated pilonidal sinus. eur J Surg. 1998;164:961–964. doi: 10.1080/110241598750005147. [DOI] [PubMed] [Google Scholar]
- 551.Dizen H, Yoldas O, Yildiz M, Cilekar M, Dilektasli E. Modified elliptical rotation flap for sacrococcygeal pilonidal sinus disease. ANZ J Surg. 2014;84:769–771. doi: 10.1111/ans.12818. [DOI] [PubMed] [Google Scholar]
- 552.Dwight RW. Pilonidal sinus; an evaluation of plastic closure using flaps of gluteal muscle. AMA Arch Surg. 1952;64:438–442. doi: 10.1001/archsurg.1952.01260010454003. [DOI] [PubMed] [Google Scholar]
- 553.Dylek ON, Bekereciodlu M. Role of simple V-Y advancement flap in the treatment of complicated pilonidal sinus. Eur.J Surg. 1998;164:961–964. doi: 10.1080/110241598750005147. [DOI] [PubMed] [Google Scholar]
- 554.Ekci B, Gokce O. A new flap technique to treat pilonidal sinus. Tech Coloproctol. 2009;13:205–209. doi: 10.1007/s10151-009-0500-8. [DOI] [PubMed] [Google Scholar]
- 555.Elalfy K, Emile S, Lotfy A, Youssef M, Elfeki H. Bilateral gluteal advancement flap for treatment of recurrent sacrococcygeal pilonidal disease: A prospective cohort study. Int J Surg. 2016;29:1–8. doi: 10.1016/j.ijsu.2016.03.006. [DOI] [PubMed] [Google Scholar]
- 556.El-Khatib HA, Al-Basti HB. A perforator-based bilobed fasciocutaneous flap: an additional tool for primary reconstruction following wide excision of sacrococcygeal pilonidal disease. J Plast Reconstr Aesthet Surg. 2009;62:494–498. doi: 10.1016/j.bjps.2007.11.043. [DOI] [PubMed] [Google Scholar]
- 557.Elshahat A. The versatility of the hatchet flap in soft tissue reconstruction and a proposed new classification. Eur J Plast Surg. 2012;35:351–357. doi: 10.1007/s00238-011-0615-9. [DOI] [Google Scholar]
- 558.Ersen B, Kahveci R, Aksu I, Tunalı O. Multiple perforator preserving SGAP flap for the reconstruction of sacral wounds. Eur J Plast Surg. 2015 [Google Scholar]
- 559.Eryilmaz R, Okan I, Coskun A, Bas G, Sahin M. Surgical treatment of complicated pilonidal sinus with a fasciocutaneous V-Y advancement flap. Dis Colon Rectum. 2009;52:2036–2040. doi: 10.1007/DCR.0b013e3181beb537. [DOI] [PubMed] [Google Scholar]
- 560.Fjermeros H. Pilonidal cysts; treatment by Holman’s operation. Acta Chir Scand. 1957;113:374–379. [PubMed] [Google Scholar]
- 561.Garrido A, Ali R, Ramakrishnan V, Spyrou G, Stanley PR. Reconstruction of the natal cleft with a perforator-based flap. Br.J Plast.Surg. 2002;55:671–674. doi: 10.1054/bjps.2002.3943. [DOI] [PubMed] [Google Scholar]
- 562.Geuenich A, Hannekum A. Primary closure of pilonidal sinus through a slide-swing operation. Chirurg. 1981;52:114–117. [PubMed] [Google Scholar]
- 563.Gordon KJ, Hunt TM. Osteomyelitis as a complication of a pilonidal sinus. Int J Colorectal Dis. 2016;31:155–156. doi: 10.1007/s00384-015-2184-z. [DOI] [PubMed] [Google Scholar]
- 564.Ho Quoc C, et al. Reconstruction fessière esthétique fiabilisée par une artère perforante glutéale. Annales de chirurgie plastique et esthétique. 2013;58:347–351. doi: 10.1016/j.anplas.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 565.Hobbs AF. An operative technique for the treatment of pilonidal sinus. Aust N Z J Surg. 1967;36:337–342. doi: 10.1111/j.1445-2197.1967.tb05545.x. [DOI] [PubMed] [Google Scholar]
- 566.Josvay J, Sashegyi M, Kelemen P, Donath A. Clinical experience with the hatchet-shaped gluteus maximus musculocutaneous flap. Ann.Plast.Surg. 2005;55:179–182. doi: 10.1097/01.sap.0000171147.73420.25. [DOI] [PubMed] [Google Scholar]
- 567.Kajisa T, Usami Y, Kikuchi F. Lumbar adipofascial turnover flap for reconstruction of pilonidal sinus; A case report. Jpn. J. Plast. Surg. 2009;52:1357–1361. [Google Scholar]
- 568.Krand O, Yalt T, Berber I, Kara VM, Tellioglu G. Management of pilonidal sinus disease with oblique excision and bilateral gluteus maximus fascia advancing flap: result of 278 patients. Dis Colon Rectum. 2009;52:1172–1177. doi: 10.1007/DCR.0b013e31819ef582. [DOI] [PubMed] [Google Scholar]
- 569.Kauer O, et al. Utilizacion del colgajo romboidal simple en el tratamiento quirurgico de la enfermedad pilonidal. Revista chilena de cirugía. 1999;51:623–626. [Google Scholar]
- 570.Kayaalp C, Olmez A, Aydin C, Piskin T. Tumescent local anesthesia for excision and flap procedures in treatment of pilonidal disease. Dis Colon Rectum. 2009;52:1780–1783. doi: 10.1007/DCR.0b013e3181b553bb. [DOI] [PubMed] [Google Scholar]
- 571.Khatri VP, Espinosa MH, Amin AK. Management of recurrent pilonidal sinus by simple V-Y fasciocutaneous flap. Dis Colon Rectum. 1994;37:1232–1235. doi: 10.1007/BF02257787. [DOI] [PubMed] [Google Scholar]
- 572.Lasheen AE, Saad K, Raslan M. Crossed triangular flaps technique for surgical treatment of chronic pilonidal sinus disease. Arch Surg. 2008;143:503–505. doi: 10.1001/archsurg.143.5.503. [DOI] [PubMed] [Google Scholar]
- 573.Lin CT, Chen SY, Chen SG, Tzeng YS, Chang SC. Parasacral Perforator Flaps for Reconstruction of Sacral Pressure Sores. Ann.Plast.Surg. 2015;75:62–65. doi: 10.1097/SAP.0000000000000024. [DOI] [PubMed] [Google Scholar]
- 574.Lodhi FB, Ijaz S, Shafio M. Pilonidal sinus: use of Limberg flap in the treatment. Professional Med J. 2006;13:435–439. [Google Scholar]
- 575.Mackowski, A. & Levitt, M. Outcomes of the house advancement flap for pilonidal sinus. ANZ J Surg, 10.1111/ans.13077 (2015). [DOI] [PubMed]
- 576.Mathur BS, Tan SS, Bhat FA, Rozen WM. The transverse lumbar perforator flap: An anatomic and clinical study. J Plast Reconstr Aesthet Surg. 2016;69:770–776. doi: 10.1016/j.bjps.2016.03.023. [DOI] [PubMed] [Google Scholar]
- 577.Al Najjar MJA-H, Al Najjar SHA. Elliptical Rotation Flap for Complicated Pilonidal Sinus. Iraqi JMS. 2015;13:56–63. [Google Scholar]
- 578.Nelson R, Lalonde D. Treatment of the chronic pilonidal sinus wound with a local perforator-assisted transposition flap. Plast Reconstr Surg. 2008;122:47e–49e. doi: 10.1097/PRS.0b013e31817746c8. [DOI] [PubMed] [Google Scholar]
- 579.Nessar G, Kayaalp C, Seven C. Elliptical rotation flap for pilonidal sinus. Am J Surg. 2004;187:300–303. doi: 10.1016/j.amjsurg.2003.11.012. [DOI] [PubMed] [Google Scholar]
- 580.Onishi K, Maruyama Y. Sacral adipofascial turn-over flap for the excisional defect of pilonidal sinus. Plast Reconstr Surg. 2001;108:2006–2010. doi: 10.1097/00006534-200112000-00026. [DOI] [PubMed] [Google Scholar]
- 581.Ozdemir H, Unal Ozdemir Z, Tayfun Sahiner I, Senol M. Whole natal cleft excision and flap: an alternative surgical method in extensive sacrococcygeal pilonidal sinus disease. Acta Chir Belg. 2014;114:266–270. [PubMed] [Google Scholar]
- 582.Özmen S, Kandal S, Findikçioglu F, Menteş B. Superior gluteal artery perforator flap: An alternative in the treatment of complicated pilonidal sinus. 2006;1(17):176–178. [Google Scholar]
- 583.Perez-Gurri JA, Temple WJ, Ketcham AS. Gluteus maximus myocutaneous flap for the treatment of recalcitrant pilonidal disease. Dis Colon Rectum. 1984;27:262–264. doi: 10.1007/BF02553803. [DOI] [PubMed] [Google Scholar]
- 584.Polat C, et al. Is oval flap reconstruction a good modification for treating pilonidal sinuses? Am J Surg. 2011;201:192–196. doi: 10.1016/j.amjsurg.2010.01.025. [DOI] [PubMed] [Google Scholar]
- 585.Rosen W, Davidson JS. Gluteus maximus musculocutaneous flap for the treatment of recalcitrant pilonidal disease. Ann Plast Surg. 1996;37:293–297. doi: 10.1097/00000637-199609000-00010. [DOI] [PubMed] [Google Scholar]
- 586.Sahasrabudhe P, Panse N, Waghmare C, Waykole P. V-y advancement flap technique in resurfacing postexcisional defect in cases with pilonidal sinus disease-study of 25 cases. Indian J Surg. 2012;74:364–370. doi: 10.1007/s12262-011-0403-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 587.Saray A, Dirlik M, Caglikulekci M, Turkmenoglu O. Gluteal V-Y advancement fasciocutaneous flap for treatment of chronic pilonidal sinus disease. Scand J Plast Reconstr Surg Hand Surg. 2002;36:80–84. doi: 10.1080/028443102753575211. [DOI] [PubMed] [Google Scholar]
- 588.Schoeller T, Wechselberger G, Otto A, Papp C. Definite surgical treatment of complicated recurrent pilonidal disease with a modified fasciocutaneous V-Y advancement flap. Surgery. 1997;121:258–263. doi: 10.1016/S0039-6060(97)90354-8. [DOI] [PubMed] [Google Scholar]
- 589.Schoeller T, Wechselberger G, Otto A, Papp C. Pilonidal sinus: experience with the Karydakis flap. Br J Surg. 1997;84:890–891. doi: 10.1002/bjs.1800840650. [DOI] [PubMed] [Google Scholar]
- 590.Schrögendorfer KF, et al. Prospective evaluation of a single-sided innervated gluteal artery perforator flap for reconstruction for extensive and recurrent pilonidal sinus disease: functional, aesthetic, and patient-reported long-term outcomes. World J Surg. 2012;36:2230–2236. doi: 10.1007/s00268-012-1639-4. [DOI] [PubMed] [Google Scholar]
- 591.Stroosma OC. Gluteal fasciaplasty as a method of primary closure in the treatment of pilonidal sinus. Arch Chir Neerl. 1978;30:61–64. [PubMed] [Google Scholar]
- 592.Sungur N, et al. V-Y rotation advancement fasciocutaneous flap for excisional defects of pilonidal sinus. Plast Reconstr Surg. 2006;117:2448–2454. doi: 10.1097/01.prs.0000219170.74059.94. [DOI] [PubMed] [Google Scholar]
- 593.Trooskin SZ. Pilonidal cyst: wide excision and primary closure with an advancement flap. J Med Soc N J. 1985;82:367–370. [PubMed] [Google Scholar]
- 594.Tuncbilek G, Nasir S, Ozkan O, Kayikcioglu A, Mavili E. Partially de-epithelialised and buried V-Y advancement flap for reconstruction of sacrococcygeal and ischial defects. Scand. J Plast. Reconstr. Surg Hand Surg. 2004;38:94–99. doi: 10.1080/02844310310006431. [DOI] [PubMed] [Google Scholar]
- 595.Turan A, Isler C, Bas SC, Genc B, Ozsoy Z. A new flap for reconstruction of pilonidal sinus: lumbar adipofascial turnover flap. Ann Plast Surg. 2007;58:411–415. doi: 10.1097/01.sap.0000243999.36577.3f. [DOI] [PubMed] [Google Scholar]
- 596.Turner FP. Pilonidal sinus: primary closure with equal musculofascial flaps and removable far-and-near sutures; analysis of fifty-nine consecutive cases. Ann Surg. 1954;140:687–694. doi: 10.1097/00000658-195411000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 597.Venus MR, Titley OG. The use of the Limberg flap for reconstruction of pilonidal sinus excision wounds. Surgeon. 2007;5:127. doi: 10.1016/S1479-666X(07)80080-1. [DOI] [PubMed] [Google Scholar]
- 598.Venus MR, Titley OG. Outcomes in the repair of pilonidal sinus disease excision wounds using a parasacral perforator flap. Ann R Coll Surg Engl. 2012;94:12–16. doi: 10.1308/003588412X13171221499748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 599.Windhofer C, Michlits W, Gruber S, Papp C. Reconstruction in the buttock region using the local fasciocutaneous infragluteal (FCI) flap. hair syndrome. 2010;63:126–132. doi: 10.1016/j.bjps.2008.08.050. [DOI] [PubMed] [Google Scholar]
- 600.Yazar M, et al. Cosmetic closure of pilonidal sinus defects with bilateral transpositional adipofascial flaps. J Plast Surg Hand Surg. 2013;47:292–296. doi: 10.3109/2000656X.2013.765884. [DOI] [PubMed] [Google Scholar]
- 601.Yucel, E. T. L. T. & Yilmaz, O. C. “Flag Excision an Flap” Procedure: a Novel Modification for Off-Midline Closure After Pilonidal Sinus Excision. Indian J Surg (2015). [DOI] [PMC free article] [PubMed]
- 602.Yuksel BC, Berkem H, Ozel H, Hengirmen S. A new surgical method of pilonidal sinus treatment: a bilaterally paralel elliptic fascio-cutaneous advancement flap technique. Bratisl Lek Listy. 2012;113:728–731. doi: 10.4149/bll_2012_165. [DOI] [PubMed] [Google Scholar]
- 603.Aldemir M, Kara IH, Erten G, Tacyildiz I. Effectiveness of collagenase in the treatment of sacrococcygeal pilonidal sinus disease. Surg Today. 2003;33:106–109. doi: 10.1007/s005950300022. [DOI] [PubMed] [Google Scholar]
- 604.Oncel M, et al. Excision and marsupialization versus sinus excision for the treatment of limited chronic pilonidal disease: a prospective, randomized trial. Tech Coloproctol. 2002;6:165–169. doi: 10.1007/s101510200037. [DOI] [PubMed] [Google Scholar]
- 605.Abramson DJ. Excision and delayed closure of pilonidal sinuses. Surg Gynecol Obstet. 1977;144:205–207. [PubMed] [Google Scholar]
- 606.Abramson DJ. Outpatient management of pilonidal sinuses: excision and semiprimary closure technic. Mil Med. 1978;143:753–757. [PubMed] [Google Scholar]
- 607.Abramson DJ, Cox PA. The marsupialization operation for pilonidal cysts and sinuses under local anesthesia with lidocaine; an ambulatory method of treatment. Ann Surg. 1954;139:341–349. doi: 10.1097/00000658-195403000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 608.Arauz S, Yamaguchi N, Schmidt Goffi F, Zanoto A. Surgical treatment of sacrococcigeal pilonidal disease: a comparative study between marsupialization and incision plus curettage techniques. Rev Col Bras Cir. 2002;29:659–662. doi: 10.1590/S0100-69912002000500008. [DOI] [Google Scholar]
- 609.Brockbank MJ. Pilonidal Cyst. Am J Surg. 1945;68:4. doi: 10.1016/0002-9610(45)90422-3. [DOI] [Google Scholar]
- 610.Cavanagh CR, Schnug GE. Definitive Treatment of the Pilonidal Abscess. Northwest Med. 1964;63:449–451. [PubMed] [Google Scholar]
- 611.Cavanagh CR, Schnug GE, Girvin GW, McGonigle DJ. Definitive marsupialization of the acute pilonidal abscess. Am Surg. 1970;36:650–651. [PubMed] [Google Scholar]
- 612.Gonzalo Inostroza L, et al. Pilonidal cyst abscess: Definitive treatment in a single time during the acute, short-term results. Revista Chilena de Cirugia. 2011;63:54–58. doi: 10.4067/S0718-40262011000100009. [DOI] [Google Scholar]
- 613.Licheri S, et al. Radical treatment of acute pilonidal abscess by marsupialization. G Chir. 2004;25:414–416. [PubMed] [Google Scholar]
- 614.Neumeister CA. A modification of the marsupialization operation for pilonidal disease. tract coag max voltage. 1963;56:730–732. doi: 10.1097/00007611-196307000-00006. [DOI] [PubMed] [Google Scholar]
- 615.Ozbalci GS, Tuncal S, Bayraktar K, Tasova V, Ali Akkus M. Is gentamicin-impregnated collagen sponge to be recommended in pilonidal sinus patient treated with marsupialization? A prospective randomized study. Ann Ital Chir. 2014;85:576–582. [PubMed] [Google Scholar]
- 616.Perez Oberreuter, G. et al. Tecnica de marsupializacion en quiste pilonidal: 7 anos de experiencia. Revista chilena de cirugía50 (1998).
- 617.Sahsamanis G, et al. Semi-closed surgical technique for treatment of pilonidal sinus disease. Ann Med Surg (Lond) 2017;15:47–51. doi: 10.1016/j.amsu.2017.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 618.Struijk DG, Krediet RT, de Glas-Vos JW, Boeschoten EW, Arisz L. Experiences with acute peritoneal dialysis in adults. Ned Tijdschr Geneeskd. 1984;128:751–755. [PubMed] [Google Scholar]
- 619.Van Ess LJ. Surgical management of pilonidal disease. Am J Proctol. 1965;16:389–393. [PubMed] [Google Scholar]
- 620.Yildirim D, Sunamak O, Pergel A, Mounla M. Combined single step definitive treatment in acute pilonidal sinus abscess. Surg Sci. 2010;1:24–26. doi: 10.4236/ss.2010.11005. [DOI] [Google Scholar]
- 621.Zambouras DH, Karavas N. Operative Behandlung des Sakraldermoids durch eine neue modifizierte Marsupialisationsmethode. Chirurg. 1971;7:330–331. [PubMed] [Google Scholar]
- 622.Zimmerman K. unknown. Am J Surg. 1953;86:569. [Google Scholar]
- 623.Vahedian J, Nabavizadeh F, Nakhaee N, Vahedian M, Sadeghpour A. Comparison between drainage and curettage in the treatment of acute pilonidal abscess. Saudi Med J. 2005;26:553–555. [PubMed] [Google Scholar]
- 624.Al Homoud SJ, Habib ZS, Abdul Jabbar AS, Isbister WH. Management of sacrococcygeal pilonidal disease. Saudi. Med. J. 2001;22:762–764. [PubMed] [Google Scholar]
- 625.Arik MK, Borazan E. Phenol application combined with minimally invasive surgery for pilonidal sinus treatment. Anatolian J. Clin. Invest. 2011;5:165–168. [Google Scholar]
- 626.Balsamo F, Borges AMP, Formiga GJS. Pilonidal sinus: Surgical treatment results with incision and curettage. Rev. Bras. Coloproctologia. 2009;29:325–328. doi: 10.1590/S0101-98802009000300006. [DOI] [Google Scholar]
- 627.Biegeleisen HI. Sclerotherapy for pilonidal cyst. Am J Surg. 1939;64:622–625. doi: 10.1016/S0002-9610(39)90711-7. [DOI] [Google Scholar]
- 628.Boulay J, Prudent J. Continuous drainage by thread applied to treatment of pilonidal disease. Annales de Gastroenterologie et d’Hepatologie. 1980;16:317–323. [Google Scholar]
- 629.Crile G., Jr. A definitive ambulatory treatment for infected pilonidal cysts. Surgery. 1948;24:677–679. [PubMed] [Google Scholar]
- 630.Elsey E, Lund JN. Fibrin glue in the treatment for pilonidal sinus: high patient satisfaction and rapid return to normal activities. Tech Coloproctol. 2013;17:101–104. doi: 10.1007/s10151-012-0956-9. [DOI] [PubMed] [Google Scholar]
- 631.Gage AA, Dutta P. Cryosurgery for pilonidal disease. Am J Surg. 1977;133:249–254. doi: 10.1016/0002-9610(77)90093-9. [DOI] [PubMed] [Google Scholar]
- 632.Garg P, Garg M, Gupta V, Mehta SK, Lakhtaria P. Laying open (deroofing) and curettage under local anesthesia for pilonidal disease: An outpatient procedure. World J Gastrointest Surg. 2015;7:214–218. doi: 10.4240/wjgs.v7.i9.214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 633.Gidwani AL, Murugan K, Nasir A, Brown R. Incise and lay open: an effective procedure for coccygeal pilonidal sinus disease. Ir J Med Sci. 2010;179:207–210. doi: 10.1007/s11845-009-0450-1. [DOI] [PubMed] [Google Scholar]
- 634.Gul VO, et al. Minimally Invasive Surgical Approach to Complicated Recurrent Pilonidal Sinus. Case Rep Surg. 2015;2015:759316. doi: 10.1155/2015/759316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 635.Gupta PJ. Radiofrequency incision and lay open technique of pilonidal sinus (clinical practice paper on modified technique) Kobe J Med Sci. 2003;49:75–82. [PubMed] [Google Scholar]
- 636.Isbister WH, Prasad J. Pilonidal disease. Aust N Z J Surg. 1995;65:561–563. doi: 10.1111/j.1445-2197.1995.tb01695.x. [DOI] [PubMed] [Google Scholar]
- 637.Jain V, Jain A. Use of lasers for the management of refractory cases of hidradenitis suppurativa and pilonidal sinus. J Cutan Aesthet Surg. 2012;5:190–192. doi: 10.4103/0974-2077.101377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 638.Jensen SL, Harling H. Prognosis after simple incision and drainage for a first-episode acute pilonidal abscess. Br J Surg. 1988;75:60–61. doi: 10.1002/bjs.1800750122. [DOI] [PubMed] [Google Scholar]
- 639.Kepenekci I, Demirkan A, Celasin H, Gecim IE. Unroofing and curettage for the treatment of acute and chronic pilonidal disease. World J Surg. 2010;34:153–157. doi: 10.1007/s00268-009-0245-6. [DOI] [PubMed] [Google Scholar]
- 640.Klin B, Heller ON, Kaplan I. The use of the CO2 laser in pilonidal sinus disease: preliminary results of an ambulatory prospective study. J Clin Laser Med Surg. 1990;8:31–37. [PubMed] [Google Scholar]
- 641.Korb JH. Infected pilonidal cysts; a simplified method of treatment. Mil Surg. 1951;108:29–34. [PubMed] [Google Scholar]
- 642.Lewin RA. Pilonidal Sinus in Infancy. Pediatrics. 1965;35:795–797. [PubMed] [Google Scholar]
- 643.Matino JJ, Banerjee S, Brown SH, Waldron JE. Human dermal tissue allograft use in treating chronic pilonidal sinus. Conn Med. 2010;74:393–398. [PubMed] [Google Scholar]
- 644.Mikkelsen K. Pilonidal sinus. A follow-up study of out-patients treated by simple incision. Ugeskr Laeger. 1975;137:789–791. [PubMed] [Google Scholar]
- 645.Miller RJ. Pilonidal disease. A logical approach. Postgrad Med. 1967;41:382–385. doi: 10.1080/00325481.1967.11696173. [DOI] [PubMed] [Google Scholar]
- 646.O´Connor JJ. Surgery plus freezing as a technique for treating pilonidal disease. Dis Colon Rectum. 1979;22:306–307. doi: 10.1007/BF02609310. [DOI] [PubMed] [Google Scholar]
- 647.Olmez A, Kayaalp C, Aydin C. Treatment of pilonidal disease by combination of pit excision and phenol application. Tech Coloproctol. 2013;17:201–206. doi: 10.1007/s10151-012-0903-9. [DOI] [PubMed] [Google Scholar]
- 648.Qayyum I, Bai D, Tsoraides SS. Loop drainage after debridement (LDAD): minimally invasive treatment for pilonidal cyst. Tech Coloproctol. 2016;20:591–594. doi: 10.1007/s10151-016-1469-8. [DOI] [PubMed] [Google Scholar]
- 649.Shafiroff BG, Doubilet H. The conservative treatment of pilonidal cyst. N Y State J Med. 1946;46:891–893. [PubMed] [Google Scholar]
- 650.Shirah B, Shirah H. The Effect of Hydrogen Peroxide on the Healing of the Laid Open Wound in the Treatment of Chronic Sacrococcygeal Pilonidal Sinus: A Retrospective Database Analysis of 500 Patients. International Journal of Surgery and Medicine. 2016;2:17. doi: 10.5455/ijsm.woundhealing. [DOI] [Google Scholar]
- 651.Sozen SO, Sozen V, Das V, et al. Day–Care Surgery for Pilonidal Sinus Using Sinotomy Technique and Fibrin Glue Injection. Arch Clin Exp Surg. 2012;1:138–141. doi: 10.5455/aces.20120625121721. [DOI] [Google Scholar]
- 652.Thomson JP, Lee J. Radical Surgery for pilonidal sinus. Ann R Coll Surg Engl. 1983;65:64. [PMC free article] [PubMed] [Google Scholar]
- 653.Thorlakson RH. An Unusual Type of Pilonidal Sinus: Report of a Case. Dis Colon Rectum. 1963;6:345–351. doi: 10.1007/BF02618391. [DOI] [PubMed] [Google Scholar]
- 654.Yalcin S, Ergul E. A single-surgeon, single-institute experience of 59 sinotomies for sacrococcygeal pilonidal disease under local anesthesia. Bratisl Lek Listy. 2010;111:284–285. [PubMed] [Google Scholar]
- 655.Bascom J. Pilonidal disease: long-term results of follicle removal. Dis Colon Rectum. 1983;26:800–807. doi: 10.1007/BF02554755. [DOI] [PubMed] [Google Scholar]
- 656.Bascom J. Pilonidal disease: origin from follicles of hairs and results of follicle removal as treatment. Surgery. 1980;87:567–572. [PubMed] [Google Scholar]
- 657.Cherian TK. A simple out-patient treatment for pilonidal sinus (Millar-Lord method) INDIAN J. SURG. 1980;42:119–122. [Google Scholar]
- 658.Colov EP, Bertelsen CA. Short convalescence and minimal pain after out-patient Bascom’s pit-pick operation. Danish medical bulletin. 2011;58:A4348. [PubMed] [Google Scholar]
- 659.Di Castro A, Guerra F, Levi Sandri GB, Ettorre GM. Minimally invasive surgery for the treatment of pilonidal disease. The Gips procedure on 2347 patients. Int J Surg. 2016;36:201–205. doi: 10.1016/j.ijsu.2016.10.040. [DOI] [PubMed] [Google Scholar]
- 660.Edwards MH. Pilonidal sinus: a 5-year appraisal of the Millar-Lord treatment. Br J Surg. 1977;64:867–868. doi: 10.1002/bjs.1800641209. [DOI] [PubMed] [Google Scholar]
- 661.Chen CL, Fitzpatrick L, Kamel H. Who uses the emergency department for dermatologic care? A statewide analysis. Journal of the American Academy of Dermatology. 2014;71:308–313. doi: 10.1016/j.jaad.2014.03.013. [DOI] [PubMed] [Google Scholar]
- 662.Froidevaux A, Marti MC. Sacro coccygeal cysts. Results of a new series of 51 cases. Lyon Chir. 1977;73:269–271. [Google Scholar]
- 663.Gips, M., Melki, Y., Salem, L., Weil, R. & Sulkes, J. Minimal surgery for pilonidal disease using trephines: description of a new technique and long-term outcomes in 1,358 patients. Dis Colon Rectum 51, 1656–1662, discussion 1662–1653, 10.1007/s10350-008-9329-x (2008). [DOI] [PubMed]
- 664.Iesalnieks I, Deimel S, Kienle K, Schlitt HJ, Zulke C. Pit-picking surgery for pilonidal disease. Chirurg. 2011;82:927–931. doi: 10.1007/s00104-011-2077-9. [DOI] [PubMed] [Google Scholar]
- 665.Iesalnieks I, Deimel S, Schlitt HJ. “Pit picking” surgery for patients with pilonidal disease: mid-term results and risk factors. Chirurg. 2015;86:482–485. doi: 10.1007/s00104-014-2776-0. [DOI] [PubMed] [Google Scholar]
- 666.Jensen SL, Nielsen OV. Lord-Millar brush method in ambulatory treatment of pilonidal cysts. Ugeskr Laeger. 1988;150:98–100. [PubMed] [Google Scholar]
- 667.Khodakaram K, Stark J, Hoglund I, Andersson RE. Minimal Excision and Primary Suture is a Cost-Efficient Definitive Treatment for Pilonidal Disease with Low Morbidity: A Population-Based Interventional and a Cross-Sectional Cohort Study. World J Surg. 2017;41:1295–1302. doi: 10.1007/s00268-016-3828-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 668.Klaiber C, Staub A, Ackermann D, Akovbiantz A. The Lord-Millar operation of pilonidal sinus. HELV. CHIR. ACTA. 1982;49:221–222. [Google Scholar]
- 669.Lord PH, Millar DM. Pilonidal Sinus: A Simple Treatment. Br J Surg. 1965;52:298–300. doi: 10.1002/bjs.1800520413. [DOI] [PubMed] [Google Scholar]
- 670.Lund JN, Leveson SH. Fibrin glue in the treatment of pilonidal sinus: results of a pilot study. Dis Colon Rectum. 2005;48:1094–1096. doi: 10.1007/s10350-004-0905-4. [DOI] [PubMed] [Google Scholar]
- 671.Majeski J, Stroud J. Sacrococcygeal pilonidal disease. Int Surg. 2011;96:144–147. doi: 10.9738/1393.1. [DOI] [PubMed] [Google Scholar]
- 672.Millar DM, Lord PH. The treatment of acute postanal pilonidal abscess. Br J Surg. 1967;54:598–599. doi: 10.1002/bjs.1800540707. [DOI] [PubMed] [Google Scholar]
- 673.Mosquera DA, Quayle JB. Bascom’s operation for pilonidal sinus. J R Soc Med. 1995;88:45P–46P. [PMC free article] [PubMed] [Google Scholar]
- 674.Neola, B., Capasso, S., Caruso, L., Falato, A. & Ferulano, G. P. Scarless outpatient ablation of pilonidal sinus: a pilot study of a new minimally invasive treatment. part 2, 10.1111/iwj.12350 (2014). [DOI] [PMC free article] [PubMed]
- 675.Parvaiz A, Kennedy R. Bascom’s procedure in the day-surgical management of symptomatic pilonidal sinus. Br J Surg. 2001;88:155–156. doi: 10.1046/j.1365-2168.2001.01712-10.x. [DOI] [PubMed] [Google Scholar]
- 676.Petersen S. Skin preserving pit excision, so-called pit picking. Pilonidal Sinus Journal. 2017;3:7. [Google Scholar]
- 677.Petrovic J, Dimitrijevic I, Krivokapic Z. Minor vs complete excision of pilonidal sinus–early postoperative period. Acta Chir Iugosl. 2012;59:81–85. doi: 10.2298/ACI1202081P. [DOI] [PubMed] [Google Scholar]
- 678.Senapati A, Cripps NP, Thompson MR. Bascom’s operation in the day-surgical management of symptomatic pilonidal sinus. Br J Surg. 2000;87:1067–1070. doi: 10.1046/j.1365-2168.2000.01472.x. [DOI] [PubMed] [Google Scholar]
- 679.Smart PJ, Dungerwalla M, Heriot AG. Bascom’s Simple Pilonidal Sinus Surgery: Simpler with Ultrasound Guidance. Journal of Medical Ultrasound. 2013;21:97–99. doi: 10.1016/j.jmu.2013.04.001. [DOI] [Google Scholar]
- 680.Zorcolo L, Capra F, Scintu F, Casula G. Surgical treatment of pilonidal disease. Results with the Bascom’s technique. Minerva Chir. 2004;59:387–395. [PubMed] [Google Scholar]
- 681.Postlethwait RW. Extensive Pilonidal Cyst - Case Report. Am J Surg. 1944;64:416–418. doi: 10.1016/S0002-9610(44)90357-0. [DOI] [Google Scholar]
- 682.Pyrtek LJ, Bartus SA. Excision of Pilonidal Cyst with Simplified Partial Wound Closure. Surg Gynecol Obstet. 1964;118:605–608. [PubMed] [Google Scholar]
- 683.Rahoma AH. Pilonidal sinus: Why does It recur. Malays. J. Med. Health Sci. 2009;5:69–77. [Google Scholar]
- 684.Anderson AW. Hair extracted from an ulcer. Boston Med Surg J. 1847;36:74. [Google Scholar]
- 685.Javed MA, et al. Comparison of conventional incision and drainage for pilonidal abscess versus novel endoscopic pilonidal abscess treatment (EPAT) Tech Coloproctol. 2016;20:871–873. doi: 10.1007/s10151-016-1546-z. [DOI] [PubMed] [Google Scholar]
- 686.Klass AA. The so-called pilo-nidal sinus. hiair clothes breaking shoulder etc. 1956;75:737–742. [PMC free article] [PubMed] [Google Scholar]
- 687.Aksoy HM, Aksoy B, Egemen D. Effectiveness of topical use of natural polyphenols for the treatment of sacrococcygeal pilonidal sinus disease: a retrospective study including 192 patients. Eur J Dermatol. 2010;20:476–481. doi: 10.1684/ejd.2010.0978. [DOI] [PubMed] [Google Scholar]
- 688.Aygen E, Arslan K, Dogru O, Basbug M, Camci C. Crystallized phenol in nonoperative treatment of previously operated, recurrent pilonidal disease. Dis Colon Rectum. 2010;53:932–935. doi: 10.1007/DCR.0b013e3181d8283b. [DOI] [PubMed] [Google Scholar]
- 689.Dag A, Colak T, Turkmenoglu O, Sozutek A, Gundogdu R. Phenol procedure for pilonidal sinus disease and risk factors for treatment failure. Surgery. 2012;151:113–117. doi: 10.1016/j.surg.2011.07.015. [DOI] [PubMed] [Google Scholar]
- 690.Dogru O, Camci C, Aygen E, Girgin M, Topuz O. Pilonidal sinus treated with crystallized phenol: an eight-year experience. Dis.Colon Rectum. 2004;47:1934–1938. doi: 10.1007/s10350-004-0720-y. [DOI] [PubMed] [Google Scholar]
- 691.Girgin M, Kanat BH. The results of a one-time crystallized phenol application for pilonidal sinus disease. Indian J Surg. 2014;76:17–20. doi: 10.1007/s12262-012-0548-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 692.Girgin M, et al. Minimally invasive treatment of pilonidal disease: crystallized phenol and laser depilation. Int Surg. 2012;97:288–292. doi: 10.9738/CC130.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 693.Gulpinar, K., Pampal, A., Ozis, S. E. & Kuzu, M. A. Non-operative therapy for pilonidal sinus in adolescence: crystallised phenol application, ‘report of a case’. BMJ Case Rep2013, 10.1136/bcr-2012-008382 (2013). [DOI] [PMC free article] [PubMed]
- 694.Hegge HG, Vos GA, Patka P, Hoitsma HF. Treatment of complicated or infected pilonidal sinus disease by local application of phenol. Surgery. 1987;102:52–54. [PubMed] [Google Scholar]
- 695.Kayaalp C, Olmez A, Aydin C, Piskin T, Kahraman L. Investigation of a one-time phenol application for pilonidal disease. Med Princ Pract. 2010;19:212–215. doi: 10.1159/000285291. [DOI] [PubMed] [Google Scholar]
- 696.Kaymakcioglu N, et al. Treatment of pilonidal sinus by phenol application and factors affecting the recurrence. Tech Coloproctol. 2005;9:21–24. doi: 10.1007/s10151-005-0187-4. [DOI] [PubMed] [Google Scholar]
- 697.Kelly SB, Graham WJ. Treatment of pilonidal sinus by phenol injection. Ulster Med J. 1989;58:56–59. [PMC free article] [PubMed] [Google Scholar]
- 698.Maurice BA, Greenwood RK. A Conservative Treatment of Pilonidal Sinus. Br J Surg. 1964;51:510–512. doi: 10.1002/bjs.1800510711. [DOI] [PubMed] [Google Scholar]
- 699.Owen Smith MS. Phenol irrigation for pilonidal sinus. 1975;121:79–86. [Google Scholar]
- 700.Rignault D, Pailler JL, Bon JC, Chauvet J, Emani A. Clinical aspects of pilonidal sinus: a study of 572 cases. Gastroenterol Clin Biol. 1977;1:925–929. [PubMed] [Google Scholar]
- 701.Rignault D, Pailler JL, Brillac J, Essioux H, Bon JC. Nonsurgical treatment of pilonidal fistulas by the curettage-phenolization method. Gastroenterol Clin Biol. 1977;1:941–944. [PubMed] [Google Scholar]
- 702.Sakcak I, Avsar FM, Cosgun E. Comparison of the application of low concentration and 80% phenol solution in pilonidal sinus disease. JRSM.Short Rep. 2010;1:5. doi: 10.1258/shorts.2009.100047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 703.Schneider IH, Thaler K, Kockerling F. Treatment of pilonidal sinuses by phenol injections. Int J Colorectal Dis. 1994;9:200–202. doi: 10.1007/BF00292250. [DOI] [PubMed] [Google Scholar]
- 704.Stephens FO, Sloane DR. Management of pilonidal sinus–a modern approach. Med J Aust. 1968;1:395–396. [PubMed] [Google Scholar]
- 705.Vara-Thorbeck R, Mekinassi K, Berchid S. Phenol treatment of pilonidal sinuses. Zentralbl Chir. 1990;115:777–780. [PubMed] [Google Scholar]
- 706.Yilmaz ME, Yilmaz O, Uyar ME, et al. Crystalline Phenol Practices and Clinical Results in our Patients with Pilonidal Sinus. J Universal Surg. 2015;3:1–4. [Google Scholar]
- 707.Benedetto AV, Lewis AT. Pilonidal sinus disease treated by depilation using an 800 nm diode laser and review of the literature. Dermatol Surg. 2005;31:587–591. doi: 10.1097/00042728-200505000-00020. [DOI] [PubMed] [Google Scholar]
- 708.Downs AM, Palmer J. Laser hair removal for recurrent pilonidal sinus disease. J Cosmet Laser Ther. 2002;4:91. doi: 10.1080/147641702321136264. [DOI] [PubMed] [Google Scholar]
- 709.Kandamany N, Mahaffey PJ. The importance of hair control and personal hygiene in preventing recurrent pilonidal sinus disease. J Plast Reconstr Aesthet Surg. 2008;61:986–987. doi: 10.1016/j.bjps.2007.11.065. [DOI] [PubMed] [Google Scholar]
- 710.Koch D, Pratsou P, Szczecinska W, Lanigan S, Abdullah A. The diverse application of laser hair removal therapy: a tertiary laser unit’s experience with less common indications and a literature overview. tabs!! 2015;30:453–467. doi: 10.1007/s10103-013-1464-5. [DOI] [PubMed] [Google Scholar]
- 711.Landa N, Aller O, Landa-Gundin N, Torrontegui J, Azpiazu JL. Successful treatment of recurrent pilonidal sinus with laser epilation. Dermatol Surg. 2005;31:726–728. doi: 10.1097/00042728-200506000-00024. [DOI] [PubMed] [Google Scholar]
- 712.Lavelle M, Jafri Z, Town G. Recurrent pilonidal sinus treated with epilation using a ruby laser. J Cosmet Laser Ther. 2002;4:45–47. doi: 10.1080/147641702320602564. [DOI] [PubMed] [Google Scholar]
- 713.Lindholt, C. S., Lindholt, J. S. & Lindholt, J. Nd-YAG laser treatment in a patient with complicated pilonidal cysts. BMJ Case Rep2009, 10.1136/bcr.07.2008.0552 (2009). [DOI] [PMC free article] [PubMed]
- 714.Lindholt-Jensen CS, Lindholt JS, Beyer M. Nd-YAG laser treatment of primary and recurrent pilonidal sinus. Lasers Med Sci. 2012;27:505–508. doi: 10.1007/s10103-011-0990-2. [DOI] [PubMed] [Google Scholar]
- 715.Odili J, Gault D. Laser depilation of the natal cleft–an aid to healing the pilonidal sinus. Ann R Coll Surg Engl. 2002;84:29–32. [PMC free article] [PubMed] [Google Scholar]
- 716.Piccolo D, et al. Unconventional use of intense pulsed light. Biomed.Res.Int. 2014;2014:618206. doi: 10.1155/2014/618206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 717.Sadick NS, Yee-Levin J. Laser and light treatments for pilonidal cysts. Cutis. 2006;78:125–128. [PubMed] [Google Scholar]
- 718.Saraceno R, Teoli M, Casciello C, Chimenti S. Methyl aminolaevulinate photodynamic therapy for the treatment of hidradenitis suppurativa and pilonidal cysts. Photodermatol Photoimmunol Photomed. 2009;25:164–165. doi: 10.1111/j.1600-0781.2009.00428.x. [DOI] [PubMed] [Google Scholar]
- 719.Shafigh Y, Beheshti A, Charkhchian M, Rad FS. Successful treatment of pilonidal disease by intense pulsed light device. Adv Clin Exp Med. 2014;23:277–282. doi: 10.17219/acem/37077. [DOI] [PubMed] [Google Scholar]
- 720.Armstrong, J. H. & Barcia, P. J. Pilonidal sinus disease. The conservative approach. Arch Surg129, 914–917, discussion 917–919 (1994). [DOI] [PubMed]
- 721.Berger H. The medical treatment of pilonidal disease. N Y State J Med. 1949;49:1313. [PubMed] [Google Scholar]
- 722.Borde CM, Bruck HG. The indications for split thickness skin grafting in recurrent pilonidal sinus. Wiener Klinische Wochenschrift. 1973;85:624–628. [PubMed] [Google Scholar]
- 723.Chia CL, Tay VW, Mantoo SK. Endoscopic pilonidal sinus treatment in the Asian population. Surg Laparosc Endosc Percutan Tech. 2015;25:e95–97. doi: 10.1097/SLE.0000000000000131. [DOI] [PubMed] [Google Scholar]
- 724.Conroy FJ, Kandamany N, Mahaffey PJ. Laser depilation and hygiene: preventing recurrent pilonidal sinus disease. J Plast Reconstr Aesthet Surg. 2008;61:1069–1072. doi: 10.1016/j.bjps.2007.06.022. [DOI] [PubMed] [Google Scholar]
- 725.Dwivedi AP. Management of pilonidal sinus by Kshar Sutra, a minimally invasive treatment. Int J Ayurveda Res. 2010;1:122–123. doi: 10.4103/0974-7788.64408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 726.Encabo B, et al. Pilonidal sinus: clinical and ultrasonographic response to topical resorcinol 15. Br J Dermatol. 2016;175:1103–1104. doi: 10.1111/bjd.14872. [DOI] [PubMed] [Google Scholar]
- 727.Feit HL. The use of thorium X in treatment of pilonidal cyst: a preliminary report. Dis Colon Rectum. 1960;3:61–64. doi: 10.1007/BF02616500. [DOI] [PubMed] [Google Scholar]
- 728.Flannery BP, Kidd HA. A review of pilonidal sinus lesions and a method of treatment. Postgrad Med J. 1967;43:353–358. doi: 10.1136/pgmj.43.499.353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 729.Hemanta P, Kumar RR, Rao MM. Ksharasutra therapy - a minimal invasive parasurgical method in the treatment of sacrococcygeal pilonidal sinus (Nadi vrana): Result of a pilot study. Intern. J. Res. Ayurveda Pharm. 2012;3:668–670. doi: 10.7897/2277-4343.03518. [DOI] [Google Scholar]
- 730.Hirshowitz B, Mahler D, Kaufmann-Friedmann K. Treatment of pilonidal sinus. Surg Gynecol Obstet. 1970;131:119–122. [PubMed] [Google Scholar]
- 731.Hussain ZI, Aghahoseini A, Alexander D. Converting emergency pilonidal abscess into an elective procedure. Dis Colon Rectum. 2012;55:640–645. doi: 10.1097/DCR.0b013e31824b9527. [DOI] [PubMed] [Google Scholar]
- 732.Isik A, et al. The use of fibrin glue without surgery in the treatment of pilonidal sinus disease. Int J Clin Exp Med. 2014;7:1047–1051. [PMC free article] [PubMed] [Google Scholar]
- 733.Jain, Y. et al. Endoscopic pilonidal abscess treatment: a novel approach for the treatment of pilonidal abscess. Ann R Coll Surg Engl, 1–3, 10.1308/rcsann.2016.0260 (2016). [DOI] [PMC free article] [PubMed]
- 734.Lewis AT, Benedetto AV. Lasers in dermatology: Unapproved treatments. Clin. Dermatol. 2002;20:700–714. doi: 10.1016/S0738-081X(02)00292-4. [DOI] [PubMed] [Google Scholar]
- 735.Lu JG, Wang C, Cao YQ, Yao YB. Thread-dragging and pad pressure therapy in traditional Chinese medicine for treatment of pilonidal sinus: a case report. Zhong Xi Yi Jie He Xue Bao. 2011;9:36–37. doi: 10.3736/jcim20110107. [DOI] [PubMed] [Google Scholar]
- 736.Meinero, P. et al. Endoscopic pilonidal sinus treatment (EPSiT): a prospective multicentre trial. Colorectal Dis, 10.1111/codi.13322 (2016). [DOI] [PubMed]
- 737.Meinero P, Mori L, Gasloli G. Endoscopic pilonidal sinus treatment (E.P.Si.T.) Tech Coloproctol. 2014;18:389–392. doi: 10.1007/s10151-013-1016-9. [DOI] [PubMed] [Google Scholar]
- 738.Mendes CRS, Ferreira LSdM, Sapucaia RA, Lima MA. Endoscopic pilonidal sinus treatment (E.P.Si.T.): a minimally invasive approach. Journal of Coloproctology. 2015;35:72–75. doi: 10.1016/j.jcol.2015.01.007. [DOI] [Google Scholar]
- 739.Milone M, et al. Video-assisted ablation of pilonidal sinus: a new minimally invasive treatment–a pilot study. Surgery. 2014;155:562–566. doi: 10.1016/j.surg.2013.08.021. [DOI] [PubMed] [Google Scholar]
- 740.Milone M, Bianco P, Musella M, Milone F. A technical modification of video-assisted ablation for recurrent pilonidal sinus. Colorectal Dis. 2014;16:O404–406. doi: 10.1111/codi.12770. [DOI] [PubMed] [Google Scholar]
- 741.Rao AC. Cutting seton for pilonidal disease: a new approach. Tech Coloproctol. 2006;10:242–244. doi: 10.1007/s10151-006-0287-9. [DOI] [PubMed] [Google Scholar]
- 742.Sangamesh H, Chandrakanth H, Vijaykumar B. A case discussion on pilonidal sinus: Case report. Intern. J. Res. Ayurveda Pharm. 2012;3:746–747. doi: 10.7897/2277-4343.03535. [DOI] [Google Scholar]
- 743.Williams DW. Free graft repair in pilonidal sinus. Postgrad Med J. 1954;30:430–433. doi: 10.1136/pgmj.30.346.430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 744.Ypsilantis E, Carapeti E, Chan S. The use of topical 10% metronidazole in the treatment of non-healing pilonidal sinus wounds after surgery. Int J Colorectal Dis. 2015 doi: 10.1007/s00384-015-2269-8. [DOI] [PubMed] [Google Scholar]
- 745.Ishida H. Five cases of pilonidal sinus (Japanese) J. Clin. Surg. 1973;28:1597–1599. [Google Scholar]
- 746.Rains AJ. Treatment of pilonidal sinus by excision and primary closure. Br Med J. 1959;2:171–173. doi: 10.1136/bmj.2.5145.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 747.Agren MS, et al. A randomized, double-blind, placebo-controlled multicenter trial evaluating topical zinc oxide for acute open wounds following pilonidal disease excision. Wound Repair Regen. 2006;14:526–535. doi: 10.1111/j.1743-6109.2006.00159.x. [DOI] [PubMed] [Google Scholar]
- 748.Aldaqal SM, Kensarah AA, Alhabboubi M, Ashy AA. A new technique in management of pilonidal sinus, a university teaching hospital experience. Int Surg. 2013;98:304–306. doi: 10.9738/INTSURG-D-13-00064.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 749.Weeks RBY, Weeks GG. Sacrococcygeal Cysts - Report of 200 cases in an army hospital. Am J Surg. 1943;60:260–263. doi: 10.1016/S0002-9610(43)90661-0. [DOI] [Google Scholar]
- 750.Hopping RA. Pilonidal disease; review of the literature with comments on the etiology, differential diagnosis and treatment of the disease. Am J Surg. 1954;88:780–788. doi: 10.1016/0002-9610(54)90275-5. [DOI] [PubMed] [Google Scholar]
- 751.Doll, D. Pilonidal Disease Surgery Needs More Off-Midline Closure Education. World J Surg, 10.1007/s00268-016-3809-2 (2016). [DOI] [PubMed]
- 752.Higgins J, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 2002;21:1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 753.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data and calculations are available to readers upon request to the corresponding author.