

Abstract
Objectives
Chronic low back pain (CLBP) is the most prevalent of the painful musculoskeletal conditions. CLBP is a heterogeneous condition with many causes and diagnoses, but there are few established therapies with strong evidence of effectiveness (or cost effectiveness). CLBP for which it is not possible to identify any specific cause is often referred to as non‐specific chronic LBP (NSCLBP). One type of NSCLBP is continuing and recurrent primarily nociceptive CLBP due to vertebral joint overload subsequent to functional instability of the lumbar spine. This condition may occur due to disruption of the motor control system to the key stabilizing muscles in the lumbar spine, particularly the lumbar multifidus muscle (MF).
Methods
This review presents the evidence for MF involvement in CLBP, mechanisms of action of disruption of control of the MF, and options for restoring control of the MF as a treatment for NSCLBP.
Results
Imaging assessment of motor control dysfunction of the MF in individual patients is fraught with difficulty. MRI or ultrasound imaging techniques, while reliable, have limited diagnostic or predictive utility. For some patients, restoration of motor control to the MF with specific exercises can be effective, but population results are not persuasive since most patients are unable to voluntarily contract the MF and may be inhibited from doing so due to arthrogenic muscle inhibition.
Conclusions
Targeting MF control with restorative neurostimulation promises a new treatment option.
Keywords: Arthrogenic muscle inhibition, chronic low back pain, lumbar multifidus, motor control exercises, restorative neurostimulation
Introduction
Low back pain (LBP) is usually defined as pain and discomfort, localized below the costal margin and above the inferior gluteal fold, with or without referred leg pain 1, 2. The NIH Task Force on Research Standards for Chronic LBP (CLBP) recommended 3 that CLBP be defined as a back pain problem that has persisted for at least three months and has resulted in pain on at least half the days in the past 6 months.
The World Health Organization reports that “Low back pain is the most prevalent of musculoskeletal conditions; it affects nearly everyone at some point in time and about 4–33% of the population at any given point” 2. LBP is now the leading cause of disability globally 4, 5 There are many publications on the epidemiology 6 of back pain including its prevalence 7, 8, 9, natural history, demographics, and country by country variability.
There are many causes for CLBP, and the differential diagnosis can be challenging 10. Specific causes for LBP are uncommon (<15% of all back pain) 1, 11. Specific LBP is defined as symptoms caused by a specific pathophysiologic mechanism, such as herniated nuclei pulposus, infection, osteoporosis, rheumatoid arthritis, fracture, or tumor 12. The remaining patients, who comprise the majority of patients, are commonly referred to as having “non‐specific LBP” (NSLBP) or “axial LBP” (ALBP) or “Mechanical LBP.” These terms can have different meanings to different audiences of clinicians and researchers.
LBP presents on a spectrum between primarily neuropathic pain and primarily nociceptive pain, and guidelines 13 and tools exist for clinical classification 14, 15. Inconsistent nomenclature complicates a review, for example merely describing CLBP as “axial” does not help with understanding if the described therapy is for predominantly neuropathic or predominantly nociceptive CLBP, as axial LBP is a syndrome that may have both nociceptive and neuropathic components 16. This review will concentrate on primarily nociceptive CLBP, which is poorly served with most of today's treatments. In many cases, the therapy of last resort is opioids.
Clinical Instability and CLBP
Panjabi 17, 18 described the stabilizing system of the spine as divided into three subsystems: 1) the spinal column; 2) the spinal muscles; and 3) the neural control unit; spine stability depends on the complex interplay of these three systems. This is illustrated conceptually in Figure 1 (after Panjabi). Disturbances in one or more of these three stabilizing mechanisms leads to spinal segments moving outside of their normal range of motion (the so‐called neutral zone), causing tissue injury and initiating LBP. If, for instance, the muscle control system exerts suboptimal stabilizing forces on the spinal column, overload of the joints and soft tissues surrounding the joints is more likely to occur, leading to primarily nociceptive pain. This lesser muscular control could be caused by decreased neural drive from or feedback to the neurologic structures controlling the muscles and the joints 19.
Figure 1.

Model of spine stability.
When looking into muscular stabilization of the lumbar spine, the role of the lumbar multifidus (MF) becomes immediately apparent. The anatomic architecture of the MF is shown in Figure 2 (reproduced from Rosatelli 20 with permission). The deep fascicles of the multifidus generally span a single segment, and are “strategically positioned to provide proprioceptive feedback from the lumbar spine.” In contrast, the intermediate fascicles may have a role in controlling intersegmental movement, whereas the superficial fascicles are capable of providing significant torque in a cranio‐caudal direction.
Figure 2.
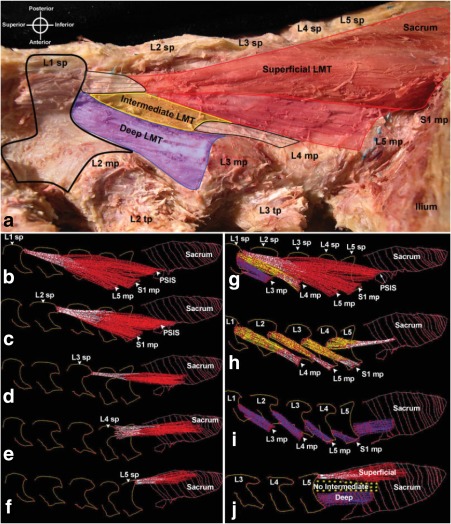
Dissection, digitization, and three‐dimensional modeling of lumbar multifidus, lateral views. a. Dissection of superficial (red), intermediate (yellow), and deep (purple) regions. b–f. Segments of the superficial region attaching to L1–L5 spinous processes. g. Three dimensional reconstruction of the digital specimen shown in a. h. Segments of the intermediate region attaching to the L1–L4 spinous processes. Note that there is no intermediate fascicle of the MF attaching to the spinous process at L5. i. Segments of the deep region attaching to the L1–L5 laminae. j. Regions of the LMT attaching to the L5 spinous process. LMT, lumbar multifidus; sp, spinous process; mp, mammillary process; tp, transverse process; PSIS, posterior superior iliac spine; L, lumbar. Reproduced from Rosatelli 20 with permission.
The MF is the strongest stabilizer of the lumbar spine 21, and the combined actions of the bilateral multifidi account for more than two thirds of the stiffness of the spine when in the neutral zone 22. Changes in MF are strongly evident in people with cLBP 23, and many patients with LBP exhibit atrophy of the MF within days of new back pain 24, 25. This atrophy can be seen easily and reliably 26 on MRI. Atrophy may be seen unilaterally or bilaterally, and bilateral atrophy is frequently seen in patients who complain of unilateral pain 25, 27. MF changes are apparent in chronic LBP 28, 29, in proportion to the duration of symptoms 30, and are not due to a change in muscle fiber type 31. The radiology literature 32 reports that fat infiltration of the MF is apparent in chronic LBP 33, 34, and there is evidence that the non‐contractile tissue seen on MRI is, indeed, fat 35. Fat infiltration and tissue remodeling may be independent of atrophy 36. Examples of fat infiltration in the MF are shown in Figure 3, with a three level classification system 37. A systematic review 38 provided evidence for the presence of macroscopic changes in lumbar muscle structures of CLBP: “especially a loss of muscle size is seen in the lower lumbar levels, but not in the more cranial lumbar levels.”
Figure 3.
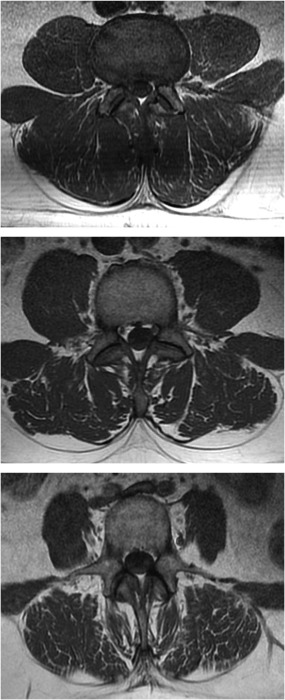
Examples of T1 weighted MRI images of lumbar spine at L3 showing mild (<10%), moderate (10–50%) and severe (>50%) fat infiltration of the lumbar multifidus muscle (images from subjects enrolled in the ReActiv8‐B Clinical Trial with permission).
Acute LBP usually resolves within weeks in most patients 39, although a meta‐analysis with a more stringent definition of acute NSLBP suggests that the majority of patients still experience pain one year from the onset of symptoms 40. MF atrophy, on the other hand, typically persists after resolution of pain 41 in patients with CLBP. This persistent defect in the key local stabilizer muscle could explain why many patients with back pain suffer from recurrences or a waxing and waning course after the initial episode 42.
The mechanism leading to MF atrophy in LBP is probably closely related to arthrogenic muscle inhibition 43. This phenomenon can be readily observed in the quadriceps muscle after traumatic and experimental knee injury 44, and is also encountered in the calf muscles after ankle injury 45. It refers to a mechanism by which pain in a skeletal joint leads to reduced neural drive to the muscle(s) that move or stabilize that joint.
Arthrogenic inhibition is thought to be caused by a change in the discharge of articular sensory receptors due to factors such as swelling, inflammation, joint laxity, and damage to joint afferents. Spinal reflex pathways likely contribute to arthrogenic inhibition, as can be measured by changes in reflex activity in experimentally induced cases 44 and evidence suggests that supra‐spinal pathways may also play an important role 44, 46, 47. Interestingly, arthrogenic inhibition in peripheral joint pathology may involve both type I and type II muscle fibers selectively or both together 48.
Arthrogenic muscle inhibition can occur in the spine consequent to an episode of LBP. Electromyogram (EMG) evidence of reduced neural drive to the MF in back pain patients includes diminished EMG activity 49, 50, and alterations in the timing of the recruitment of the short (deep) fascicles of the MF in response to perturbations 29. Pain alters the magnitude of activation of deep MF during certain types of activity 51. Ultrasound imaging evidence of reduced neural drive in back pain patients includes reduced muscle thickness changes with contraction 52, 53, 54, 55, reduced ability to cause a muscle thickness change on command 56, and altered contraction patterns with changes in posture 57.
There is evidence from humans and animal models, including ovine 58, porcine 59, 60, and feline 61 that induced local injury compromises neural drive to the MF, seen as changes in electrical activity on MF electromyography. Experimentally induced intervertebral disc degeneration in the cat induces pathophysiologic changes to the MF 62. In a rabbit model, the MF becomes stiffer, both in individual fibers and in fiber bundles, in response to experimentally induced intervertebral disc degeneration, and a stiffer muscle can alter the biomechanical properties of the spine stabilizing system 62.
Injury to the spine structures (e.g., joints, ligaments, disc) can disrupt one or more of the spine stability sub‐systems 19, 63, 64, 65. Induced pain studies in humans confirm that local pain of the spinal column leads to reduction of neural drive to the adjacent MF, apparent on functional MRI 66 and ultrasound 67, 68. EMG studies of populations of patients with acute or chronic LBP show altered recruitment of the MF 69, 70 due to pain, pain avoidance, and deconditioning. Pain has been experimentally shown to reduce neural drive not only to the MF, but also the lumbar erector spinae muscles in both healthy volunteers and back pain patients 71.
Figure 4 shows a representation of compromised spine stability as a result of arthrogenic inhibition. Nociceptive signals (pain) from the spine inhibit the neuromuscular control system (in the brain and spinal cord) which results in reduced neural drive to the muscles which compromises stability and movement. Disrupted neural drive also alters the proprioceptive feedback from the muscles themselves.
Figure 4.
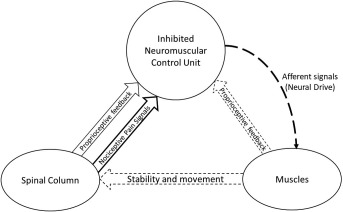
Compromised spine stability.
Cortical changes in the brain are associated with chronic LBP 72. Impaired motor control of the MF in patients with CLBP is associated with changes in cortical representation of the multifidus and subsequent ability to exert voluntary control 73 and there is evidence of reorganization of trunk muscle representation at the motor cortex in individuals with recurrent LBP. This reorganization is associated with deficits in postural control 74. Individual fascicles of MF are activated by different regions in the motor cortex 75, and motor control training for back pain patients can reverse the cortical reorganization 76. Evidence of cortical remodeling may be assessed with research techniques of brain mapping using transcranial magnetic stimulation (TMS) and surface EMG recorded at the L3 level, and magnitude of cortical remodeling is associated with severity and location of LBP 77. There is evidence that motor training can reverse pathologic reorganization of neuronal networks of the motor cortex in people with recurrent pain, at least for motor training that focuses on the transverse abdominus 76. Reduction in back pain as a result of facet joint injections or spine surgery has also been shown to be associated with restoration of normal brain anatomy and function 78.
In summary
The spine stabilization system consists of the spine, the muscles, and the neural control system.
Arthrogenic muscle inhibition can disrupt control to the key segmental stabilizing muscle of the spine—the lumbar multifidus.
Disrupted muscle control can lead to compromised clinical stability of the spine, allowing joint overload and consequent persistent and recurrent pain.
Back pain due to disrupted muscle control is associated with neuroplastic changes in the motor cortex, which can be reversed with elimination of back pain.
Diagnostic Tests for Motor Control Dysfunction
Since disruption of the MF is clearly associated with CLBP in many cases, it is logical to examine diagnostic tools that can identify patients with this particular pathology.
Imaging Assessment of Motor Control Dysfunction
Changes to the MF apparent with MRI imaging are strongly associated with back pain, but the diagnostic value in individual patients of such changes is limited, since back pain of any cause can lead to changes of the MF cross sectional area and amount of fat infiltration 79. Prolonged bed rest in the absence of back pain can also lead to atrophy of the MF seen on imaging 80 and the atrophy can be reversed with appropriate exercises 81. There appears to be no relationship between MF function and amount of fat infiltration 82. There is some evidence 83 that the severity of fat infiltration correlates with decreased range of motion in flexion, and that the amount of fat infiltration may be a predictor for continued CLBP 84, but the diagnostic utility of these observations is unclear.
Ultrasound imaging has been used to document reduced MF muscle mass, a consequence of reduced neural drive, which in back pain patients includes diminished thickness change with activation 52, 53 and reduced ability to cause a muscle thickness change on command 56. Although the measurement techniques have been validated and are reliable, the diagnostic utility is unclear, and ultrasound measured MF activation does not appear to be predictive of which CLBP patients will benefit from stabilization exercises 85. A review 86 states there is “a convincing body of evidence [that] suggests that US imaging is a reliable and valid tool for differentiating LBP patients from normal subjects and monitoring rehabilitation outcome measures.” A later systematic review 87 found “conflicting evidence for a relation between baseline percent thickness change of lumbar multifidus during contraction and the clinical outcomes of patients after various conservative treatments.”
EMG Assessment of Motor Control Dysfunction
EMG evidence has been used to show changes in MF recruitment in populations of patients with CLBP, but has not been shown to be useful as a tool for diagnosis or monitoring therapy in individual patients. Surface EMG cannot be used to accurately record from the MF 88 so fine wire or needle electrodes are more commonly used, but there is no easy way to isolate the EMG signals from the deeper multifidus layers from the surrounding muscles. Even with needle or wire EMG, some far field potentials originating in co‐contracting muscles are seen, making it difficult to correctly identify the onset of muscle activity in the multifidus. European Guidelines on NSLBP 1 state the EMG procedures “have no clear relevance to clinical diagnostics although they may still be useful in experimental studies and/or in the rehabilitation environment for examining mechanisms of back muscle function/dysfunction.”
Physical Diagnostic Tests for Motor Control Dysfunction
Several tests have been investigated to diagnose patients with CLBP due to motor control impairment including the standing back extension test 89, the prone instability test (PIT) 90, and the multifidus lift test (MLT) 91. The standing back extension test has reliability reported as a Kappa of 0.87, but, the test was validated against the function of deep abdominal muscles only to determine if motor control deficit of the spine were present.
The PIT has adequate interrater reliability 92 (reported as K = 0.87) 93 and good face validity. A positive PIT was one of the four variables shown to be predictive of success with a stabilization exercise program for patients with sub‐acute LBP (a sample of 40 subjects with an average duration of 75 days) that included exercises designed to reactivate the LM 94. In another study 95, subjects with LBP (a sample of 105 with an average duration of 65 days) who had a positive PIT in conjunction with aberrant movement patterns were shown to have reduced disability and pain following a course of motor control re‐training exercises when compared to those subjects who did not have these clinically findings.
The PIT is performed with the patient prone in a relaxed and neutral spine posture (Fig. 5). The tester applies posterior to anterior glides (pressure) over each lumbar segment. If one or more glides produces pain, the glides are repeated when the subject's posterior spinal muscles are activated (extending the hips by lifting the feet off the floor, Fig. 6). If the pain is significantly diminished when the glides are performed during muscle activation, the test is considered positive and suggestive of the presence of a motor control deficit, including MF dysfunction.
Figure 5.

Positioning for starting the Prone Instability Test. We obtained consent for inclusion of the photo from the patient.
Figure 6.

Activation condition for the PIT (note feet are lifted slightly off the floor). We obtained consent for inclusion of the photo from the patient.
Hebert et al. reported the reliability of the MLT, a palpation technique designed to test for MF function. This study used the MLT procedure and compared the results of palpation for the determination of diminished compared to normal multifidus contraction to the measurement of MF muscle thickness change via sonography in 32 subjects with LBP 91. “During the arm lift, the examiner made a qualitative judgment as to whether the participant demonstrated a normal or abnormal lumbar multifidus contraction. This judgment was based on the degree of contraction as determined by muscle palpation. We operationally defined a normal contraction as one in which a robust and obvious muscle contraction could be palpated during the arm lift. We operationally defined an abnormal contraction as occurring when there was little or no palpable contraction of the muscle during the arm lift.”
Inter‐tester reliability of the MLT at the L4–L5 was reported to be K = 0.75 with 86% agreement and at the L5–S1 level demonstrated a K = 0.81 with 91% agreement. To establish validity of the test, they assessed the correlation between outcome of the MLT and the ultrasound measure of thickness change. The correlation coefficients demonstrated a consistent relationship (0.59–0.73, p < 0.01) between the MLT findings and the ultrasound measures of lumbar multifidus function at L4–L5 and at L5–S1. They reported one examiner that was significant and one was not with a p value = 0.056.
While the PIT has not been specifically validated for LM function, there are data suggesting a relationship between a positive PIT and MF dysfunction. MF reduced thickness change, measured with ultrasound, has been shown to be associated with those who do respond well to a stabilization exercise program 94. Additionally, subjects that were more likely to respond well to the stabilization exercise program had reduced LM thickness change during the MLT. Finally, Herbert et al. demonstrated that subjects who had a positive PIT also had reduced LM thickness change (8.5%) when compared with subjects who had a negative PIT (14.9%). These findings collectively suggest that subjects who test positive on the PIT, may have associated MF dysfunction.
In summary:
Imaging (x‐ray, MRI, ultrasound) diagnostic tests for CLBP due to motor control dysfunction have limited value in individual patients.
EMG has little value as a diagnostic tool for individual patients with CLBP.
Physical movement tests (in particular the prone instability test) may be useful to identify patients with CLBP who will benefit for therapies to address motor control dysfunction.
Therapies for Patients with CLBP due to MF Disruption
Exercise Intervention for Restoration of Muscle Control to the MF
The “core stabilizing muscles” of the trunk consists of the erector spinae (ES), transverse abdominus (TrA), and MF, which is the only muscle in this group that provides segmental stability. Many exercise programs for LBP have focused on “core stabilization exercises” which include the MF. The concept of core stability has both its proponents 96 and its critics 85, 97 with strongly held views on both sides and much controversy 98.
There have been many studies on core stabilization exercises to improve back pain associated with spine instability 99, 100, 101. Several terms are used with approximately the same meaning including “motor control exercises” (MCE), “spine stabilization exercises,” “lumbar stabilization exercises” and “core strengthening.” There have also been many reviews and meta‐analyses of the value of core stabilization exercises 102, 103, 104, 105, 106, 107, 108, and the conclusions range between great value and no additional value over normal exercises. Unfortunately, there are no “standards” for core stabilization exercises, so comparison of clinical studies is challenging at best. Furthermore, most studies make no attempt to use diagnostic tests to identify in advance those patients likely to benefit from restoration of MCE, hence any true effect is buried in the noise.
There are few published studies of exercise programs that focus on just the multifidus. Interestingly, “generalized” core stabilization exercises have quite mixed results, whereas exercises that target the MF alone or in combination with another muscle generally have more positive clinical results 109, 110.
Specific MCE targeting the atrophied MF in some cLBP patients can override the normally involuntary motor control system, restore neural drive to the MF, and lead to recovery from back pain. Ultrasound image guided biofeedback 86 of the MF can help the patient learn to voluntarily contract a muscle not normally subject to voluntary control 111.
This therapy can result in improvements in pain and function in people with CLBP 112, 113, 114, 115 including athletes 116, 117, and chronic back pain related to spondylosis and spondylolisthesis 118. In addition to reducing symptoms in chronic pain, targeted motor control training can reduce long‐term recurrence of back pain in patients with MF atrophy, and reduce the severity of recurrences that do occur 42. The presence of reduced MF activation is a strong predictor (and may be the only useful predictor) of the success of specific targeted training exercises 94.
Unfortunately, targeted MF exercises are difficult to perform and teach, and many patients are simply unable to voluntarily contract a muscle group not normally amenable to voluntary control. In addition, back pain induced arthrogenic muscle inhibition of the spine stabilizing muscles may prohibit any voluntary contraction of the MF.
Neuromuscular Electrical Stimulation (NMES) to Restore Motor Control
In a similar situation, many patients find it difficult or impossible to perform quadriceps strengthening exercises following knee surgery as a result of persistent arthrogenic muscle inhibition. Transcutaneous neuromuscular electrical stimulation (NMES) to cause episodic contraction of the quadriceps alone has been used to restore motor control to allow voluntary contractions and hence facilitate rehabilitation 119, 120 following total knee arthroplasty 121 or other surgical procedures 122, 123. This treatment has been analyzed in a systematic review 124. Painful knee osteoarthritis can be treated without surgery but may also lead to pain mediated inhibition of neural drive to the quadriceps, which can be treated with NMES 125. It is clear that NMES can restore motor control in some circumstances, and in fact can do so prior to improvements in strength of the quadriceps 126, 127. NMES has also been used to restore motor control for swallowing 128.
NMES of the spine stabilizing muscles has not been well researched.1 Transcutaneous NMES cannot selectively activate deep muscles without also activating the overlying muscles. For example, NMES over the lumbar spine can cause contractions of the superficial fascicles of the MF, but also causes contractions of the transverse abdominus and obliquis internus 129. Transcutaneous NMES over the multifidus has been shown to have no effect 130.
In summary
A program of biofeedback guided motor control exercise of the MF can restore disrupted motor control to the MF.
Motor control exercises of the MF may be impossible in the context of arthrogenic inhibition of the MF due to CLBP.
In the situation of disrupted motor control of the quadriceps from arthrogenic inhibition due to knee pain, transcutaneous neuromuscular electrical stimulation has been shown to restore motor control of the quadriceps.
Transcutaneous NMES is not suitable for the MF, because the muscle is deep, diffuse, and has extensive overlying muscles.
Restorative Neurostimulation for CLBP
In the same way that electrical stimulation to cause episodic quadriceps contraction can restore neuromuscular control following knee surgery, it was hypothesized that targeted electrical stimulation to cause episodic contraction of the MF alone could lead to restoration of neuromuscular control of the MF, leading to improved functional stability of the lumbar spine and resolution of CLBP. Whereas transcutaneous stimulation to elicit selective MF contractions is not feasible, stimulation of electrodes placed adjacent to the nerve supply to the MF can cause MF only contractions. Direct stimulation of motor nerves to elicit muscle contraction requires two orders of magnitude lower energy than direct stimulation of the muscle mass. Furthermore, direct electrical stimulation of the motor nerves supplying the MF will lead to contraction of the whole muscle innervated by the motor nerve, and not just the region of muscle in the vicinity of the electrodes used for direct muscle stimulation.
A feasibility study to explore this concept using “off the shelf” neurostimulation hardware showed encouraging results 131. Based on the results of this study, a custom implantable neurostimulator was developed and subjected to a single arm clinical trial, which subsequently led to CE Mark approval of the device (see https://clinicaltrials.gov/ct2/show/NCT01985230). Results of this trial are presented in this issue of Neuromodulation 132.
An international, multi‐center, prospective randomized trial with sham control and triple blinding is under way to gather data for a potential submission to the FDA for a Pre‐Market Approval (see https://clinicaltrials.gov/show/NCT02577354).
Conclusion
A significant number of people with primarily nociceptive CLBP have impaired neuromuscular control of the key stabilizing muscles of the lumbar spine as the root cause of their pain, especially impaired control of the lumbar multifidus. These people are generally not candidates for surgery, and are poorly served by existing therapies. Exercise therapy targeting restoration of neuromuscular control of the MF has been shown to be effective in some cases, but most people find it difficult or impossible to voluntarily contract the MF. The application of exercise therapy to the MF is limited by the fact that the MF is not normally amenable to voluntary control and may also be subject to arthrogenic muscle inhibition.
Electrical stimulation to restore neuromuscular control of the quadriceps following knee injury or knee surgery has been shown to be effective. The same approach has not been systematically applied to the lumbar spine. Restorative neurostimulation of the MF to mimic the effects of targeted exercise therapy of the MF has been explored in two single‐arm clinical trials with encouraging results, and a prospective sham‐controlled RCT is under way.
Restorative neurostimulation to cause contraction of the lumbar multifidus holds promise as a new and different approach to treating primarily nociceptive mechanical chronic LBP.
Authorship Statements
Dr. Russo provided overall guidance for the development of the manuscript. Dr. Deckers, Dr. Kiesel, and Mr. Vieceli provided specialized input to the sections on arthrogenic inhibition, and diagnostic tests for mechanical low back pain. Dr. Gilligan contributed to the manuscript in general, and specifically the sections on therapies for CLBP. Mr. Crosby maintained the database of publications, and developed the first draft of the manuscript, and was instrumental in coordinating reviews among all authors. All authors approved the final version of the manuscript.
COMMENT
I congratulate the authors on a comprehensive and yet succinct review of the existing body of knowledge regarding multifidus motor control and chronic low back pain. Have they identified the nociceptive elephant in the neuromodulation room of low back pain treatment? Is there causation buried in the correlation? Has it been this small muscle, which has frustrated so many neuromodulators, patients and possibly insurers? Physical therapists and chiropractors have for decades dissented our penchant for ablative destruction of the medial branch of the dorsal primary ramus arguing we should be rather be applauding and emboldening the multifidus. Clearly there exists an association between multifidus malfunction and CLBP, and motor dysfunction has been clearly linked to multiple other painful maladies in other regions of the body (many of which also respond to peripheral, direct NMES or upstream NMES). The sibling article published alongside this one reveals the precocious efforts to provide implantable NMES to this formerly challenging neural target. Time will tell. My suspicion: the success of peripheral neuromodulation which serves to specifically rehabilitate and ameliorate downstream muscle dysfunction will eclipse sensory only peripheral nerve stimulation efforts. Formerly shunned mixed or motor nerves may have very specific orthodromic value when, possibly even central, pain relates to downstream motor dysfunction.
W. Porter McRoberts, MD
Fort Lauderdale, FL, USA
Comments not included in the Early View version of this paper.
For more information on author guidelines, an explanation of our peer review process, and conflict of interest informed consent policies, please go to http://www.wiley.com/WileyCDA/Section/id‐301854.html
Source(s) of financial support: The review was sponsored by Mainstay Medical International plc.
Conflict of Interest: Dr. Russo consults for Medtronic, Abbott, Boston Scientific, Nevro, Stimwave, Saluda, and Mainstay Medical. He also has equity holdings in Freedom Neuro, Lungpacer, and SPR Therapeutics. Dr. Russo has a patent licensed to Nevro. Dr. Deckers consults for Mainstay Medical, and is a shareholder and advisor for TrainM NV (Antwerp, Belgium). Prof. Eldabe consults for Mainstay Medical, Medtronic, St Jude Medical, Boston Scientific, Saluda Medical and Axonics. Prof Kiesel consults for Mainstay Medical and an equity partner in Functional Movement Systems. Dr. Gilligan consults for Mainstay Medical, Medtronic, Whale Imaging, Axial Healthcare, and Nuvectra. Mr. Vieceli consults for Mainstay Medical. Mr. Crosby is an employee and shareholder of Mainstay Medical.
Footnotes
Note that NMES differs from Transcutaneous Electrical Stimulation (TENS) used as a pain therapy. There are different electrical parameters of stimulation, different proposed mechanisms of action and different modes of use. There is no evidence that TENS is effective for treatment of CLBP 133.
REFERENCES
- 1. Airaksinen O, Brox JI, Cedraschi C et al. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J 2006;15(Suppl 2):S192–S300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81:646–656. [PMC free article] [PubMed] [Google Scholar]
- 3. Deyo R, Dworkin SF, Amtmann D et al. Report of the NIH Task Force on research standards for chronic low back pain. Spine J 2014;14:1375–1391. [DOI] [PubMed] [Google Scholar]
- 4. Global Burden of Disease Stud y 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;6736:1990–2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Buchbinder R, Blyth FM, March LM et al. Placing the global burden of low back pain in context. Best Pract Res Clin Rheumatol 2013;27:575–589. [DOI] [PubMed] [Google Scholar]
- 6. Kent PM, Keating JL. The epidemiology of low back pain in primary care. Chiropr Osteopat 2005;13:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Strine TW, Hootman JM. US national prevalence and correlates of low back and neck pain among adults. Arthritis Rheum 2007;57:656–665. [DOI] [PubMed] [Google Scholar]
- 8. Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine (Phila Pa 1976) 2006;31:2724–2727. [DOI] [PubMed] [Google Scholar]
- 9. Freburger JK, Holmes GM, Agans RP et al. The rising prevalence of chronic low back pain. Arch Intern Med 2009;169:251–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Amirdelfan K, McRoberts P, Deer TR. The differential diagnosis of low back pain: a primer on the evolving paradigm. Neuromodulation Technol Neural Interface 2014;17:11–17. [DOI] [PubMed] [Google Scholar]
- 11. Deyo RA, Weinstein JN. Low back pain. N Engl J Med 2001;344:363–370. [DOI] [PubMed] [Google Scholar]
- 12. Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. Br Med J 2006;332:1430–1434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nijs J. Low back pain: Guidelines for the clinical classification of predominant neuropathic, nociceptive, or central sensitization pain. Pain Physcian 2015;18:E333–E346. [PubMed] [Google Scholar]
- 14. Freynhagen R, Baron R, Gockel U, Tölle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin 2006;22:1911–1920. [DOI] [PubMed] [Google Scholar]
- 15. Nijs J, Torres‐Cueco R, van Wilgen CP et al. Applying modern pain neuroscience in clinical practice: criteria for the classification of central sensitization pain. Pain Physician 2014;17:447–457. [PubMed] [Google Scholar]
- 16. Förster M, Mahn F, Gockel U et al. Axial low back pain: one painful area – many perceptions and mechanisms. PLoS One 2013;8:e68273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord 1992;5:383–389. discussion: 397. [DOI] [PubMed] [Google Scholar]
- 18. Panjabi MM. Panjabi – 1992 – the stabilizing system of the spine. Part II. Neutral zone and instability hypothesis.pdf. J Spinal Disord 1992;5:390–396. discussion: 397. [DOI] [PubMed] [Google Scholar]
- 19. Panjabi MM. Clinical spinal instability and low back pain. J Electromyogr Kinesiol 2003;13:371–379. [DOI] [PubMed] [Google Scholar]
- 20. Rosatelli AL, Ravichandiran K, Agur AM. Three‐dimensional study of the musculotendinous architecture of lumbar multifidus and its functional implications. Clin Anat 2008;21:539–546. [DOI] [PubMed] [Google Scholar]
- 21. Kim CW, Gottschalk LJ, Eng C, Ward SR, Lieber RL. The multifidus muscle is the strongest stabilizer of the lumbar spine. Spine J 2007;7:76S. [Google Scholar]
- 22. Wilke H‐J, Wolf S, Claes LE, Arand M, Wiesend A. Stability increase of the lumbar spine with different muscle groups. A biomechanical in vitro study. Spine (Phila Pa 1976) 1995;20:192–198. [DOI] [PubMed] [Google Scholar]
- 23. Freeman MD, Woodham MA, Woodham AW. The role of the lumbar multifidus in chronic low back pain: a review. PM R 2010;2:142–146. [DOI] [PubMed] [Google Scholar]
- 24. Hides JA, Stokes M, Saide M, Jull GA, Cooper DH. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine (Phila Pa 1976) 1994;19:165–172. [DOI] [PubMed] [Google Scholar]
- 25. Fortin M, Macedo LG. Multifidus and paraspinal muscle group cross‐sectional areas of patients with low back pain and control patients: a systematic review with a focus on blinding. Phys Ther 2013;93:873–888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hu Z‐J, He J, Zhao F‐D et al. An assessment of the intra‐ and inter‐reliability of the lumbar paraspinal muscle parameters using CT scan and magnetic resonance imaging. Spine (Phila Pa 1976) 2011;36:E868–E874. [DOI] [PubMed] [Google Scholar]
- 27. Beneck GJ, Kulig K. Multifidus atrophy is localized and bilateral in active persons with chronic unilateral low back pain. Arch Phys Med Rehabil 2012;93:300–306. [DOI] [PubMed] [Google Scholar]
- 28. Hides JA, Stanton WR, Gilmore C, Bohlscheid E. Multifidus size and symmetry among chronic LBP and healthy asymptomatic subjects. Man Ther 2008;13:43–49. [DOI] [PubMed] [Google Scholar]
- 29. Macdonald DA, Moseley GL, Hodges PW. Why do some patients keep hurting their back? Evidence of ongoing back muscle dysfunction during remission from recurrent back pain. Pain 2009;142:183–188. [DOI] [PubMed] [Google Scholar]
- 30. Barker KL, Shamley DR, Jackson D. Changes in the cross‐sectional area of multifidus and psoas in patients with unilateral back pain: the relationship to pain and disability. Spine (Phila Pa 1976) 2004;29:E515–E519. [DOI] [PubMed] [Google Scholar]
- 31. Crossman K, Mahon M, Watson PJ, Oldham JA, Cooper RG. Chronic low back pain‐associated paraspinal muscle dysfunction is not the result of a constitutionally determined ‘adverse’ fiber‐type composition. Spine (Phila Pa 1976) 2004;29:628–634. [DOI] [PubMed] [Google Scholar]
- 32. Hides JA, Stanton W, Dilani Mendis M, Sexton M. The relationship of transversus abdominis and lumbar multifidus clinical muscle tests in patients with chronic low back pain. Man Ther 2011;10–14: 573–577. doi:10.1016/j.math.2011.05.007 [DOI] [PubMed] [Google Scholar]
- 33. Danneels LA, Vanderstraeten GG, Cambier DC, Witvrouw EE, De Cuyper HJ. CT imaging of trunk muscles in chronic low back pain patients and healthy control subjects. Eur Spine J 2000;9:266–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yanik B, Keyik B, Conkbayir I. Fatty degeneration of multifidus muscle in patients with chronic low back pain and in asymptomatic volunteers: quantification with chemical shift magnetic resonance imaging. Skeletal Radiol 2013;42:771–778. [DOI] [PubMed] [Google Scholar]
- 35. Théron J, Guimaraens L, Casasco A, Coellar H, Sola T. Lumbosacral liposuction. A new tool for the treatment of low back pain. Interv Neuroradiol 2007;13:153–160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Hodges PW, James G, Blomster L et al. Multifidus muscle changes after back injury are characterized by structural remodeling of muscle, adipose and connective tissue, but not muscle atrophy. Spine (Phila Pa 1976) 2015;40:1057–1071. [DOI] [PubMed] [Google Scholar]
- 37. Kjaer P, Bendix T, Sorensen JS, Korsholm L, Leboeuf‐Yde C. Are MRI‐defined fat infiltrations in the multifidus muscles associated with low back pain? BMC Med 2007;5:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Goubert D, Van Oosterwijck J, Meeus M, Danneels L. Structural changes of lumbar muscles in non‐specific low back pain. Pain Physician 2016;19:E985–E1000. [PubMed] [Google Scholar]
- 39. Pengel LHM, Herbert RD, Maher CG, Refshauge KM. Acute low back pain: systematic review of its prognosis. BMJ 2003;327:323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Itz CJ, Geurts JW, van Kleef M, Nelemans P. Clinical course of non‐specific low back pain: a systematic review of prospective cohort studies set in primary care. Eur J Pain 2013;17:5–15. [DOI] [PubMed] [Google Scholar]
- 41. Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not automatic after resolution of acute, first‐episode low back pain. Spine (Phila Pa 1976) 1996;21:2763–2769. [DOI] [PubMed] [Google Scholar]
- 42. Hides JA, Jull GA, Richardson CA. Long‐term effects of specific stabilizing exercises for first‐episode low back pain. Spine (Phila Pa 1976) 2001;26:E243–E248. [DOI] [PubMed] [Google Scholar]
- 43. Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum 2009;40:250–266. doi:10.1016/j.semarthrit.2009.10.001 [DOI] [PubMed] [Google Scholar]
- 44. Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum 2010;40:250–266. [DOI] [PubMed] [Google Scholar]
- 45. Palmieri RM, Ingersoll CD, Hoffman MA et al. Arthrogenic muscle response to a simulated ankle joint effusion. Br J Sports Med 2004;38:26–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Tsao H, Danneels LA, Hodges PW. ISSLS prize winner: smudging the motor brain in young adults with recurrent low back pain. Spine (Phila Pa 1976) 2011;36:1721–1727. [DOI] [PubMed] [Google Scholar]
- 47. Fritz JM, Koppenhaver SL, Kawchuk GN, Teyhen DS, Hebert JJ, Childs JD. Preliminary investigation of the mechanisms underlying the effects of manipulation: exploration of a multivariate model including spinal stiffness, multifidus recruitment, and clinical findings. Spine (Phila Pa 1976) 2011;36:1772–1781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Young A. Current issues in arthrogenous inhibition. Ann Rheum Dis 1993;52:829–834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Stevens VK, Coorevits PL, Bouche KG et al. The influence of specific training on trunk muscle recruitment patterns in healthy subjects during stabilization exercises. Man Ther 2006;12:271–279. [DOI] [PubMed] [Google Scholar]
- 50. D'Hooge R, Hodges P, Tsao H, Hall L, Macdonald D, Danneels L. Altered trunk muscle coordination during rapid trunk flexion in people in remission of recurrent low back pain. J Electromyogr Kinesiol 2013;23:173–181. [DOI] [PubMed] [Google Scholar]
- 51. Kiesel KB, Butler RJ, Duckworth A et al. Experimentally induced pain alters the EMG activity of the lumbar multifidus in asymptomatic subjects. Man Ther 2012;17:236–240. doi:10.1016/j.math.2012.01.008 [DOI] [PubMed] [Google Scholar]
- 52. Wallwork TL, Stanton WR, Freke M, Hides JA. The effect of chronic low back pain on size and contraction of the lumbar multifidus muscle. Man Ther 2009;14:496–500. [DOI] [PubMed] [Google Scholar]
- 53. Chan S‐T, Fung P‐K, Ng N‐Y et al. Dynamic changes of elasticity, cross‐sectional area, and fat infiltration of multifidus at different postures in men with chronic low back pain. Spine J 2012;12:381–388. [DOI] [PubMed] [Google Scholar]
- 54. Teyhen D, Koppenhaver S. Rehabilitative ultrasound imaging. J Physiother 2011;57:196. [DOI] [PubMed] [Google Scholar]
- 55. Annaswamy TM, Bierner SM, Doppalapudi H. Does lumbar dorsal ramus syndrome have an objective clinical basis? PM R 2013;5:996–1006. [DOI] [PubMed] [Google Scholar]
- 56. Kiesel KB, Uhl TL, Underwood FB, Rodd DW, Nitz AJ. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imaging. Man Ther 2007;12:161–166. [DOI] [PubMed] [Google Scholar]
- 57. Lee S‐W, Chan C. K‐M, Lam T‐S et al. Relationship between low back pain and lumbar multifidus size at different postures. Spine (Phila Pa 1976) 2006;31:2258–2262. [DOI] [PubMed] [Google Scholar]
- 58. Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE. Effects of disc degeneration on neurophysiological responses during dorsoventral mechanical excitation of the ovine lumbar spine. J Electromyogr Kinesiol 2007;18:829–837. [DOI] [PubMed] [Google Scholar]
- 59. Hodges P, Galea M, Holm S, Kaigle Holm A. Response of the Deep Paraspinal Muscles to Cortical but Not Transmastoid Stimulation Is Increased at a Single Lumbar Level Following Interverebral Disc Lesion Paper presented at Progress in Motor Control VI, Mendes Convention Center, Santos, São Paulo, Brazil 2007. http://demotu.org/pmcvi/viewabstract.php?id=228.
- 60. Hodges PW, Holm AK, Hansson T, Holm S. Rapid atrophy of the lumbar multifidus follows experimental disc or nerve root injury. Spine (Phila Pa 1976) 2006;31:2926–2933. [DOI] [PubMed] [Google Scholar]
- 61. Zhou B‐H, Williams M, Solomonow M, Baratta RV, Harris M. Multifidus spasms elicited by prolonged lumbar flexion. Spine (Phila Pa 1976) 2000;25:2916–2924. [DOI] [PubMed] [Google Scholar]
- 62. Brown SHM, Gregory DE, Carr JA et al. Adaptations to the multifidus muscle in response to experimentally induced intervertebral disc degeneration. Spine (Phila Pa 1976) 2011; 36:1728–1736. doi:10.1097/BRS.0b013e318212b44b [DOI] [PubMed] [Google Scholar]
- 63. Panjabi MM. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction. Eur Spine J 2006;15:668–676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: effect and possible mechanisms. J Electromyogr Kinesiol 2003;13:361–370. [DOI] [PubMed] [Google Scholar]
- 65. Brumagne S, Cordo P, Lysens R, Verschueren S, Swinnen S. The role of paraspinal muscle spindles in lumbosacral position sense in individuals with and without low back pain. Spine (Phila Pa 1976) 2000;25:989–994. [DOI] [PubMed] [Google Scholar]
- 66. Dickx N, Cagnie B, Achten E, Vandemaele P, Parlevliet T, Danneels L. Changes in lumbar muscle activity because of induced muscle pain evaluated by muscle functional magnetic resonance imaging. Spine (Phila Pa 1976) 2008;33:E983–E989. [DOI] [PubMed] [Google Scholar]
- 67. Kiesel KB, Underwood FB, Mattacola CG, Nitz AJ, Malone TR. A comparison of select trunk muscle thickness changes between subjects with low back pain classified in the treatment‐based classification system and asymptomatic controls. J Orthop Sports Phys Ther 2007;37:596–607. doi:10.2519/jospt.2007.2574 [DOI] [PubMed] [Google Scholar]
- 68. Kiesel KB, Uhl T, Underwood FB, Nitz AJ. Rehabilitative ultrasound measurement of select trunk muscle activation during induced pain. Man Ther 2008;13:132–138. [DOI] [PubMed] [Google Scholar]
- 69. Danneels L, Coorevits P, Cools A et al. Differences in electromyographic activity in the multifidus muscle and the iliocostalis lumborum between healthy subjects and patients with sub‐acute and chronic low back pain. Eur Spine J 2002;11:13–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. D'Hooge R, Cagnie B, Crombez G, Vanderstraeten G, Achten E, Danneels L. Lumbar muscle dysfunction during remission of unilateral recurrent nonspecific low‐back pain: evaluation with muscle functional MRI. Clin J Pain 2013;29:187–194. [DOI] [PubMed] [Google Scholar]
- 71. Dubois J‐D, Piché M, Cantin V, Descarreaux M. Effect of experimental low back pain on neuromuscular control of the trunk in healthy volunteers and patients with chronic low back pain. J Electromyogr Kinesiol 2011;21:774–781. doi:10.1016/j.jelekin.2011.05.004 [DOI] [PubMed] [Google Scholar]
- 72. Wand BM, Parkitny L, O'Connell NE et al. Cortical changes in chronic low back pain: current state of the art and implications for clinical practice. Man Ther 2011;16:15–20. [DOI] [PubMed] [Google Scholar]
- 73. Massé‐Alarie H, Beaulieu L‐D, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double‐pulse transcranial magnetic stimulation. Exp Brain Res 2015; 234:1033–1045. doi:10.1007/s00221-015-4528-x [DOI] [PubMed] [Google Scholar]
- 74. Tsao H, Galea MP, Hodges PW. Reorganization of the motor cortex is associated with postural control deficits in recurrent low back pain. Brain 2008;131:2161–2171. [DOI] [PubMed] [Google Scholar]
- 75. Tsao H, Danneels L, Hodges PW. Individual fascicles of the paraspinal muscles are activated by discrete cortical networks in humans. Clin Neurophysiol 2011;122:1580–1587. [DOI] [PubMed] [Google Scholar]
- 76. Tsao H, Galea MP, Hodges PW. Driving plasticity in the motor cortex in recurrent low back pain. Eur J Pain 2010;14:832–839. [DOI] [PubMed] [Google Scholar]
- 77. Schabrun SM, Elgueta‐Cancino EL, Hodges PW. Smudging of the Motor Cortex is related to the Severity of Low Back Pain. Spine (Phila Pa 1976) 2015;1:38. doi:10.1097/BRS.0000000000000938 [DOI] [PubMed] [Google Scholar]
- 78. Seminowicz DA, Wideman TH, Naso L et al. Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function. J Neurosci 2011;31:7540–7550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Kalichman L, Carmeli E, Been E. The association between imaging parameters of the paraspinal muscles, spinal degeneration, and low back pain. Biomed Res Int 2017;2017:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Hides JA, Belavý DL, Stanton W et al. Magnetic resonance imaging assessment of trunk muscles during prolonged bed rest. Spine (Phila Pa 1976) 2007;32:1687–1692. [DOI] [PubMed] [Google Scholar]
- 81. Hides JA, Lambrecht G, Richardson CA et al. The effects of rehabilitation on the muscles of the trunk following prolonged bed rest. Eur Spine J 2011;20:808–818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Le Cara EC, Marcus RL, Dempsey AR, Hoffman MD, Hebert JJ. Morphology versus function: the relationship between lumbar multifidus intramuscular adipose tissue and muscle function among patients with low back pain. Arch Phys Med Rehabil 2014;95:1846–1852. [DOI] [PubMed] [Google Scholar]
- 83. Hildebrandt M, Fankhauser G, Meichtry A, Luomajoki H. Correlation between lumbar dysfunction and fat infiltration in lumbar multifidus muscles in patients with low back pain. BMC Musculoskelet Disord 2017;18:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Fortin M, Gibbons LE, Videman T, Battié MC. Do variations in paraspinal muscle morphology and composition predict low back pain in men? Scand J Med Sci Sports 2014;25:880–887. doi:10.1111/sms.12301 [DOI] [PubMed] [Google Scholar]
- 85. Zielinski KA, Henry SM, Ouellette‐Morton RH, DeSarno MJ. Lumbar multifidus muscle thickness does not predict patients with low back pain who improve with trunk stabilization exercises. Arch Phys Med Rehabil 2013;94:1132–1138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Ghamkhar L, Emami M, Mohseni‐Bandpei MA, Behtash H. Application of rehabilitative ultrasound in the assessment of low back pain: a literature review. J Bodyw Mov Ther 2011;15:465–477. [DOI] [PubMed] [Google Scholar]
- 87. Wong AYL, Parent EC, Funabashi M, Stanton TR, Kawchuk GN. Do various baseline characteristics of transversus abdominis and lumbar multifidus predict clinical outcomes in nonspecific low back pain? A systematic review. Pain 2013;154:2589–2602. [DOI] [PubMed] [Google Scholar]
- 88. Stokes IAF, Henry SM, Single RM. Surface EMG electrodes do not accurately record from lumbar multifidus muscles. Clin Biomech (Bristol, Avon) 2003;18:9–13. [DOI] [PubMed] [Google Scholar]
- 89. Gondhalekar GA, Kumar SP, Eapen C, Mahale A. Reliability and validity of standing back extension test for detecting motor control impairment in subjects with low back pain. J Clin Diagn Res 2016;10:KC07–KC11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil 2005;86:1753–1762. [DOI] [PubMed] [Google Scholar]
- 91. Hebert JJ, Koppenhaver SL, Teyhen DS, Walker BF, Fritz JM. The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. Spine J 2015;15:1196–1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Denteneer L, Stassijns G, De Hertogh W, Truijen S, Van Daele U. Inter‐ and intrarater reliability of clinical tests associated with functional lumbar segmental instability and motor control impairment in patients with low back pain: a systematic review. Arch Phys Med Rehabil 2017;98:151–164.e6. [DOI] [PubMed] [Google Scholar]
- 93. Hicks GE, Fritz JM, Delitto A, Mishock J. Interrater reliability of clinical examination measures for identification of lumbar segmental instability. Arch Phys Med Rehabil 2003;84:1858–1864. [DOI] [PubMed] [Google Scholar]
- 94. Hebert JJ, Koppenhaver SL, Magel JS, Fritz JM. The relationship of transversus abdominis and lumbar multifidus activation and prognostic factors for clinical success with a stabilization exercise program: a cross‐sectional study. Arch Phys Med Rehabil 2010;91:78–85. [DOI] [PubMed] [Google Scholar]
- 95. Rabin A, Shashua A, Pizem K, Dickstein R, Dar G. A clinical prediction rule to identify patients with low back pain who are likely to experience short‐term success following lumbar stabilization exercises: a randomized controlled validation study. J Orthop Sports Phys Ther 2014;44:6–B13. [DOI] [PubMed] [Google Scholar]
- 96. Barr KP, Griggs M, Cadby T. Lumbar stabilization: core concepts and current literature, Part 1. Am J Phys Med Rehabil 2005;84:473–480. [DOI] [PubMed] [Google Scholar]
- 97. Lederman E. The myth of core stability. J Bodyw Mov Ther 2010;14:84–98. [DOI] [PubMed] [Google Scholar]
- 98. Standaert CJ, Herring SA. Expert opinion and controversies in musculoskeletal and sports medicine: core stabilization as a treatment for low back pain. Arch Phys Med Rehabil 2007;88:1734–1736. [DOI] [PubMed] [Google Scholar]
- 99. Kumar S, Sharma VP, Aggarwal A, Shukla R, Dev R. Effect of dynamic muscular stabilization technique on low back pain of different durations. J Back Musculoskelet Rehabil 2012;25:73–79. [DOI] [PubMed] [Google Scholar]
- 100. Hides JA, Stanton WR, Mendis MD, Gildea J, Sexton MJ. Effect of motor control training on muscle size and football games missed from injury. Med Sci Sports Exerc 2011;44:1141–1149. doi:10.1249/MSS.0b013e318244a321 [DOI] [PubMed] [Google Scholar]
- 101. Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent, nonspecific low back pain: a systematic review. Phys Ther 2009;89:9–25. [DOI] [PubMed] [Google Scholar]
- 102. Saragiotto BT, Maher CG, Yamato TP et al. Motor control exercise for chronic non‐specific low‐back pain. Cochrane Database Syst Rev 2016;1:CD012004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Hauggaard A, Persson AL. Specific spinal stabilisation exercises in patients with low back pain – a systematic review. Phys Ther Rev 2007;12:233–248. [Google Scholar]
- 104. May S, Johnson R. Stabilisation exercises for low back pain: a systematic review. Physiotherapy 2008;94:179–189. [Google Scholar]
- 105. Byström MG, Rasmussen‐Barr E, Johannes W, Grooten A, Grooten WJA. Motor control exercises reduces pain and disability in chronic and recurrent low back pain: a meta‐analysis. Spine (Phila Pa 1976) 2013;38:E350–E358. [DOI] [PubMed] [Google Scholar]
- 106. Standaert CJ, Weinstein SM, Rumpeltes J. Evidence‐informed management of chronic low back pain with lumbar stabilization exercises. Spine J 2008;8:114–120. [DOI] [PubMed] [Google Scholar]
- 107. Smith BE, Littlewood C, May S. An update of stabilisation exercises for low back pain: a systematic review with meta‐analysis. BMC Musculoskelet Disord 2014;15:1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108. Wang X‐Q, Zheng JJ, Yu ZW et al. A meta‐analysis of core stability exercise versus general exercise for chronic low back pain. PLoS One 2012;7:e52082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Willemink MJ, van Es HW, Helmhout PH et al. The effects of dynamic isolated lumbar extensor training on lumbar multifidus functional cross‐sectional area and functional status of patients with chronic nonspecific low back pain. Spine (Phila Pa 1976) 2012;37:E1651–E1658. [DOI] [PubMed] [Google Scholar]
- 110. Akuthota V, Nadler S. Core strengthening. Arch Phys Med Rehabil 2004;85:86–92. [DOI] [PubMed] [Google Scholar]
- 111. Van K, Hides JA, Richardson CA. The use of real‐time ultrasound imaging for biofeedback of lumbar multifidus muscle contraction in healthy subjects. J Orthop Sports Phys Ther 2006;36:920–925. [DOI] [PubMed] [Google Scholar]
- 112. Goldby LJ, Moore AP, Doust J, Trew ME. A randomized controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine (Phila Pa 1976) 2006;31:1083–1093. [DOI] [PubMed] [Google Scholar]
- 113. França FR, Burke TN, Caffaro RR, Ramos LA, Marques AP. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized, controlled trial. J Manipulative Physiol Ther 2012;35:279–285. [DOI] [PubMed] [Google Scholar]
- 114. Koppenhaver SL, Fritz JM, Hebert JJ et al. Association between history and physical examination factors and change in lumbar multifidus muscle thickness after spinal manipulation in patients with low back pain. J Electromyogr Kinesiol 2012;22:724–731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Koppenhaver SL, Fritz JM, Hebert JJ et al. Association between changes in abdominal and lumbar multifidus muscle thickness and clinical improvement after spinal manipulation. J Orthop Sports Phys Ther 2011;41:389–399. doi:10.2519/jospt.2011.3632 [DOI] [PubMed] [Google Scholar]
- 116. Hides JA, Stanton WR, McMahon S, Sims K, Richardson CA. Effect of stabilization training on multifidus muscle cross‐sectional area among young elite cricketers with low back pain. J Orthop Sports Phys Ther 2008;38:101–108. [DOI] [PubMed] [Google Scholar]
- 117. Harringe ML, Nordgren JS, Arvidsson I, Werner S. Low back pain in young female gymnasts and the effect of specific segmental muscle control exercises of the lumbar spine: a prospective controlled intervention study. Knee Surg Sports Traumatol Arthrosc 2007;15:1264–1271. [DOI] [PubMed] [Google Scholar]
- 118. O'Sullivan PB, Phyty GD, Twomey LT, Alon G. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine (Phila Pa 1976) 1997;22:2959–2967. [DOI] [PubMed] [Google Scholar]
- 119. Imoto AM, Peccin S, Almeida GJM, Saconato H, Atallah ÁN. Effectiveness of electrical stimulation on rehabilitation after ligament and meniscal injuries: a systematic review. Sao Paulo Med J 2011;129:414–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. Stevens JE, Mizner RL, Snyder‐Mackler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res 2003;21:775–779. [DOI] [PubMed] [Google Scholar]
- 121. Stevens‐Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther 2012;92:210–226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Avramidis K, Strike PW, Taylor PN, Swain ID. Effectiveness of electric stimulation of the vastus medialis muscle in the rehabilitation of patients after total knee arthroplasty. Arch Phys Med Rehabil 2003;84:1850–1853. [DOI] [PubMed] [Google Scholar]
- 123. Stevens JE, Mizner RL, Snyder‐Mackler L. Neuromuscular electrical stimulation for quadriceps muscle strengthening after bilateral total knee arthroplasty: a case series. J Orthop Sports Phys Ther 2004;34:21–29. [DOI] [PubMed] [Google Scholar]
- 124. Kim K‐M, Croy T, Hertel J, Saliba S. Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient‐oriented outcomes: a systematic review. J Orthop Sports Phys Ther 2010;40:383–391. [DOI] [PubMed] [Google Scholar]
- 125. Walls RJ, McHugh G, Moyna NM, O'Byrne J. Efficacy and compliance of a quadriceps femoris neuromuscular stimulation program in subjects with severe knee osteoarthritis. Orthopaedic Proc 2009;91‐B(Supp III):457. [Google Scholar]
- 126. Gondin J, Guette M, Martin A. Neural and muscular changes after 4 and 8 weeks of electromyostimulation training. Comput Methods Biomech Biomed Eng 2005;8:119–120. [Google Scholar]
- 127. Gondin J, Duclay J, Martin A. Neural drive preservation after detraining following neuromuscular electrical stimulation training. Neurosci Lett 2006;409:210–214. [DOI] [PubMed] [Google Scholar]
- 128. Carnaby‐Mann GD, Crary MA. Examining the evidence on neuromuscular electrical stimulation for swallowing: a meta‐analysis. Arch Otolaryngol Head Neck Surg 2007;133:564–571. [DOI] [PubMed] [Google Scholar]
- 129. Baek SO, Ahn SH, Jones R et al. Activations of deep lumbar stabilizing muscles by transcutaneous neuromuscular electrical stimulation of lumbar paraspinal regions. Ann Rehabil Med 2014;38:506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Bilgin S, Temucin CM, Nurlu G et al. Effects of exercise and electrical stimulation on lumbar stabilization in asymptomatic subjects: a comparative study. J Back Musculoskelet Rehabil 2013;26:261–266. [DOI] [PubMed] [Google Scholar]
- 131. Deckers K, De Smedt K, van Buyten J‐P et al. Chronic low back pain: restoration of dynamic stability. Neuromodulation 2015;18:478–486. [DOI] [PubMed] [Google Scholar]
- 132. Deckers K, De Smedt K, Mitchell B, et al. New therapy for refractory chronic mechanical low back pain – restorative neurostimulation to activate the lumbar multifidus: one year results of a prospective multicenter clinical trial. Neuromodulation 2018;21:48–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Brosseau L, Milne S, Robinson V et al. Efficacy of the transcutaneous electrical nerve stimulation for the treatment of chronic low back pain: a meta‐analysis. Spine (Phila Pa 1976) 2002;27:596–603. [DOI] [PubMed] [Google Scholar]