

Abstract
Rationale:
Toothpicks are widely used as a tooth cleaning tool after meals in China. Most of the Chinese toothpicks are made of wood or bamboo with a hard texture and sharp ends. This characteristic has proven to be potentially dangerous when toothpicks are accidentally ingested, as they can cause damage and perforation of the digestive tract and other subsequent complications.
Patient concerns:
The main clinical complaints of 5 patients in this study were mainly acute or chronic abdominal pain, duration from 2 days to 2 months, 1 case with vomiting, 1 case with fever.
Diagnoses:
Four cases were initially diagnosed by computed tomography (CT) scan; However, the first case was misdiagnosed as appendicitis so the patient did not undertake a preoperative CT scan and it was diagnosed by laparoscopy.
Interventions:
All the cases were treated by laparoscopy and the toothpicks were removed successfully.
Outcomes:
Toothpick-caused digestive perforation was confirmed by laparoscopy in all this 5 cases, the perforation sites were 2 cases at the antrum of stomach, 1 case at the third part of duodenum, 1 case at the ileocecal junction and 1 case at the sigmoid colon. 4 cases had perforation repair . Operative time :48-67 min. Intraoperative bleeding: 25-80 ml. 1 patient had a secondary liver injury. No postoperative complications occurred in all cases. The length of hospital stay was between 4-25 days.
Lessons:
Our case series study suggests that laparoscopy is a safe and feasible surgical procedure for definitive management of digestive tract perforation by toothpick ingestion. We also suggest all the people should have healthy life behaviors and use the toothpicks correctly.
Keywords: case report, laparoscopy, perforation, toothpick
1. Introduction
Cases of accidental toothpick ingestion have been reported in the literature.[1] Generally, ingested toothpicks pass inadvertently through the entire digestive tract without causing any damage; however, some cases may produce a digestive tract perforation leading to serious complications such as secondary damage to the liver, pancreas, kidney, or heart as the sharp ends of the toothpick pierce through the digestive tract.[2] Therefore, it is a rare and intractable circumstance when these cases reach the Emergency Unit. Our center treated 5 cases of digestive tract perforation, caused by accidentally ingesting toothpicks over the past 2 years (the latter 4 cases were concentrated in the summer of the same year), one of which developed into a liver abscess. All 5 patients had to undergo laparoscopy (done by the same physician) for the removal of the object. After the surgical proceedings, all the patients had a successful recovery with no further complications.
2. Cases presentation
2.1. Case 1
Male patient, 28 years old, was admitted on December 15, 2014, with complaint of recurrent right lower quadrant abdominal pain, on and off for a period of over 2 months. The patient had the habit of drinking beer from a glass containing a toothpick as a label. Physical examination: vital signs were stable, mild tenderness was observed on the right lower abdominal quadrant, with no rebound tenderness. White blood cell (WBC): 6.8×109/L, Neutrophil count% (NEUT%): 68%, C-reactive protein (CRP): 4.27 mg/L. Tentative diagnosis: chronic appendicitis. Laparoscopy was performed. Appendix intraoperative exploration showed no abnormalities. Upon further exploration, a toothpick was identified at the ileocecal junction protruding through the intestinal wall by 2 cm (Fig. 1). The toothpick (6 cm) was extracted and the perforation site was closed by a purse string suture. Four days postsurgery the patient recovered well and was discharged with no further complications.
Figure 1.
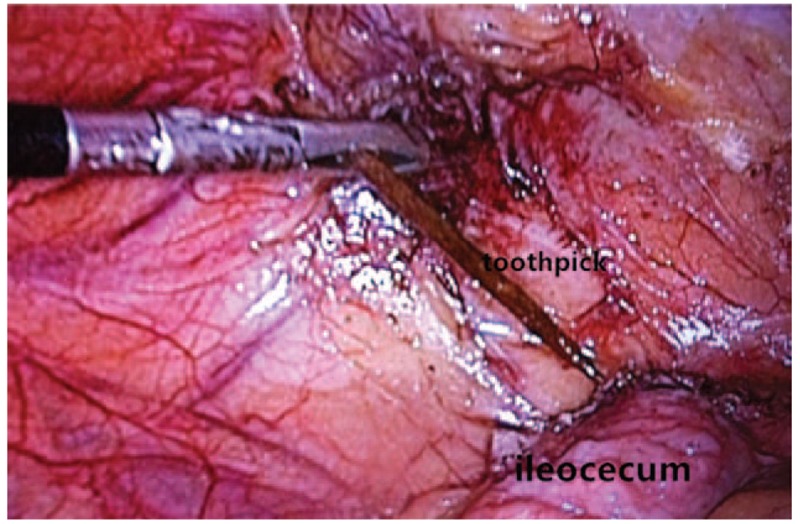
Toothpick removal from the ileocecal junction.
2.2. Case 2
Male patient, 31 years old, admitted on April 15, 2016, with complaint of abdominal pain and vomiting for 3 consecutive days. The patient had a history of alcohol abuse and reported he might have accidentally ingested a toothpick while drinking, 10 days prior to symptom presentation. Physical examination: vital signs were stable, with mild upper abdominal tenderness and no rebound tenderness. WBC: 11.8×109/L NEUT%: 82%, CRP: 54.4 mg/L. Abdominal contrast-enhanced computed tomography (CT) scans demonstrated: a 62 mm long opaque foreign body at the third part of the duodenum, piercing the transverse mesocolon and forming an abscess (4×3 cm), considered possibly to be a toothpick (Fig. 2A). Emergency laparoscopy was conducted. Intraoperative exploration revealed upper abdominal adhesions. Underneath the transverse colon, a mesentery encapsulated abscess was exposed with fibrin and pus on the surface (Fig. 2B), where the penetrating wooden foreign body was identified as a toothpick (6 cm) (Fig. 2C). The toothpick was extracted and the wound was left open. An indwelling drainage tube was placed during the surgical procedure. Five days postsurgery the patient fully recovered and was discharged with no further complications.
Figure 2.
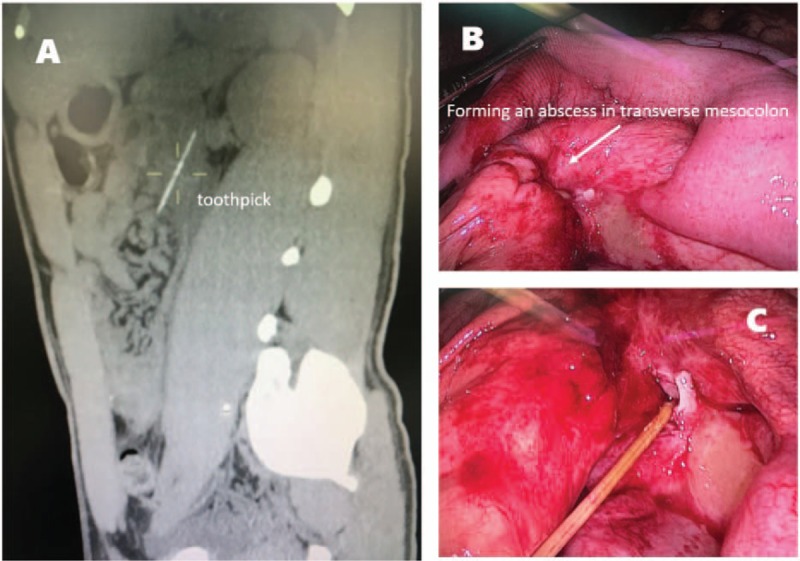
Ingested toothpick's CT scan (A) and laparoscopic view of the abscess (B) and the extracted toothpick (C). CT = computed tomography.
2.3. Case 3
Male patient, 41 years old, admitted on July 11, 2016, with complaint of abdominal pain for 2 consecutive days. The patient reported that he habitually maintained a toothpick in his mouth after meals. Physical examination: vital signs were stable, with mild upper abdominal tenderness but no rebound tenderness. WBC: 9.8×109/L NEUT%: 72%, CRP: 34.4 mg/L. Abdominal contrast-enhanced CT scans showed that a 60 mm long opaque object was piercing the posterior wall of the antrum, close to the right kidney (Fig. 3A and B), which was considered possibly to be a toothpick. Emergency laparoscopy was conducted. Intraoperative exploration revealed a sharp wooden foreign body penetrating out approximately 3 cm at the posterior wall of the antrum, partially piercing into the perinephric fat of the kidney (Fig. 3C and D). The kidney was not damaged. The entire toothpick (6 cm) was extracted and the wound was closed by a purse string suture. Four days postsurgery the patient had recovered smoothly and was discharged with no further complications.
Figure 3.
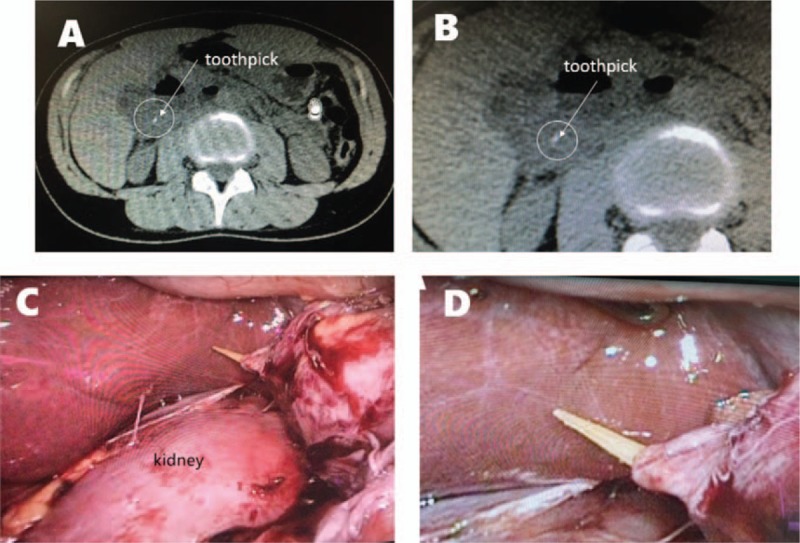
CT scan showing a toothpick piercing the posterior wall of the antrum (A) (panel B shows a close-up view of the image displayed in panel A), and laparoscopic imaging showing the toothpick's proximity to the right kidney (C) (panel D shows a close-up view of the image displayed in panel C). CT = computed tomography.
2.4. Case 4
Female patient, 19 years old, admitted on August 19, 2016, with complaint of abdominal pain and fever for 2 consecutive weeks. The patient reported that 1 week prior to the first onset of pain, she might have unintentionally swollen a toothpick. Physical examination: T: 39.6oC, P: 110/min, R: 20/min, BP: 109/63 mm Hg, with tenderness of the upper abdomen without rebound tenderness. WBC: 14.37×109/L, NEUT%: 84.3%, CRP: 43.8 mg/L. Abdominal contrast-enhanced CT showed liver abscess formation (48 mm × 44 mm) in the liver segment 4, and a 64 mm long opaque object lying between the liver and the anterior wall of the stomach, which was considered to be a toothpick piercing the stomach and the liver (Fig. 4A). Cross-departmental discussion between the Gastrointestinal Surgery, the Digestive System Department and the Infection Department, decided on treatment management with gastrointestinal decompression, parenteral nutrition and antibiotic therapy, under close monitoring. Two weeks later, biochemical lab tests indicated that the indices/markers of inflammation had returned to normal levels. However, CT scan showed that, although the size of the liver abscess was reduced, the foreign body remained in the same position (Fig. 4B). Laparoscopy was performed to locate and remove the object on September 6, 2016. It showed significant epigastric adhesions; a wooden foreign body was located between the gastric antrum and the anterior inferior border of the left liver. One end of the foreign object had pierced into the gastric wall and the other end was penetrating into the liver (Fig. 4E–G). The entire object was extracted from the liver, and was identified to be a toothpick (6 cm) (Fig. 4D), the gastric perforation was suture repaired and a drainage tube was inserted (Fig. 4C). The patient was transferred to the Infectious Disease Department for further antibiotic therapy. The drainage tube was removed 4 days postsurgery and the patient was discharged eight days postsurgery with no further complications.
Figure 4.
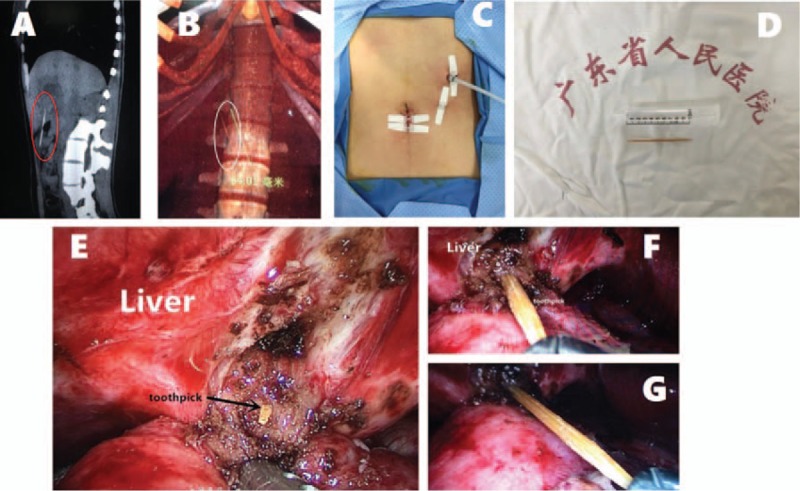
CT scan on the first day of admission (A) and 2 weeks after treatment (B). The drainage tube inserted after laparoscopic removal of the toothpick (C). The entire toothpick (6 cm) was removed by laparoscopy (D). Laparoscopic view of the toothpick located between the gastric wall and the liver (E–G). CT = computed tomography.
2.5. Case 5
Male patient, 23 years old, admitted on November 20, 2016, with complaint of hypogastralgia for 2 consecutive days at the time of admission. The patient reported that he was drinking from a glass containing a toothpick 3 days prior to the onset of the abdominal pain. Physical examination: vital signs were normal, with slight tenderness in the left lower abdominal quadrant and without rebound tenderness. WBC: 12.79×109/L NEUT%: 73.8%, CRP: 66 mg/L. Abdominal CT showed a left lower quadrant solid strip opacity (62 mm in length) in the vicinity of the sigmoid colon, which was considered possibly to be a toothpick. Emergency laparoscopic exploration was performed identifying both ends of the foreign body penetrating the sigmoid colon wall, and induced mesenteric adhesions on one side (Fig. 5A and C). Adhesions were separated, the foreign object was extracted and was identified to be a toothpick (6 cm) (Fig. 5B). The perforation was closed by a purse string suture and a drainage tube was inserted and removed 3 days postsurgery. The patient was discharged 4 days postsurgery with no further complications.
Figure 5.
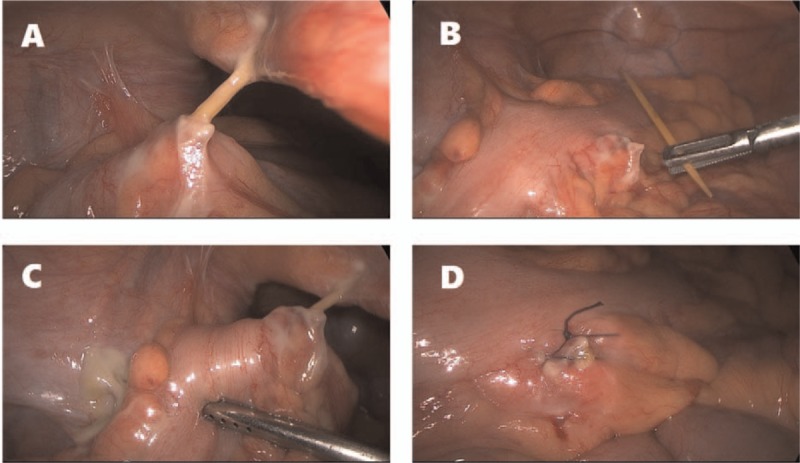
Laparoscopic view of the sigmoid colon perforation; both ends of the foreign body had penetrated the sigmoid colon wall (A and C). The entire toothpich was extracted (B). The perforation was closed by a purse string suture (D).
3. Discussion
Toothpicks are relatively small in length, thin, and with sharpened ends.[3] These characteristics can facilitate accidental ingestion. Intestinal perforation with secondary injury of other intra-abdominal viscera and death are well reported.[4,5] In China, most cases occur whilst eating and drinking, especially under the influence of alcohol consumption.
3.1. Epidemiology
A report by the CPSCNIC (consumer product safety commission national injury information clearinghouse) of America in 1984 showed that the incidence of digestive tract damage caused by inadvertent ingestion of a toothpick was 0.2/100. It was more common in teenagers.[3] Relying on the symptoms alone to make a clinical diagnosis of intestinal perforation by ingested toothpick is difficult especially as most patients are unaware of the toothpick ingestion prior to presenting symptoms. In the published literature ingestion of toothpicks occurs mainly during food or alcoholic beverage consumption.[6] In America, the toothpick design includes only 1 sharp end, while in China it usually has 2, which increases the possibility of perforating the digestive tract. The toothpicks extracted from our case studies all had 2 sharp ends. According to the report of Li and Ender,[7] the presentation of symptoms of inadvertent toothpick ingestion was between 1 and 15 years after ingestion. The presentation of symptoms in our case studies was between 1 week and 2 months after ingestion. Four patients were unable to recall the details of the incidence of toothpick ingestion; however, their medical history revealed that they all had been consuming alcohol at the suspected time of accidental toothpick ingestion and prior to the onset of the abdominal pain. The fifth case was due to misuse of the toothpick (holding a toothpick at the corner of the mouth after dinner).
3.2. Clinical characteristics
Five patients visited the Emergency Unit of the Hospital due to the symptoms of localized abdominal pain, in which the diagnosis of accidental toothpick ingestion was confirmed in 4 cases via a CT scan. The CT 3D reconstruction technique can show the shape of a toothpick and its relation to the surrounding organs, which is helpful for planning surgery. The first patient sought medical attention due to chronic right lower abdominal pain, and was misdiagnosed as a delayed presentation of appendicitis before the operation. A preoperative CT scan was not ordered and the toothpick perforation at the ileocecal junction was diagnosed at the time of laparoscopy. Some researchers report that the sensitivity of the abdominal CT scan is between 42.6 and 78%.[8] For the wooden or bamboo toothpicks in our case series, the CT diagnostic rate was 100%. The most frequent sites of perforation caused by the ingested toothpicks are at the narrow parts of the digestive tract (pylorus and ileocecal valve) and at the anatomical corners of the digestive tract (duodenum and sigmoid colon). Steinbach et al's[9] summary of 136 cases of accidental toothpick ingestion in 2013 showed that the most common sites of the perforation caused by the toothpicks were the gastric antrum (20%), the duodenum (23%), the ileocecal junction (9%), and the sigmoid colon (16%). The 5 cases reported here were confirmed by laparoscopic operation to have perforations. The perforation sites were in 2 cases at the gastric antrum, in 1 case in the third part of the duodenum, in 1 case at the ileocecal junction and in 1 case at the sigmoid colon, which are all consistent with the published literature. Therefore, in cases of suspected perforation by ingested toothpicks and in the absence of a prior CT scan, we should focus on the high incidence perforation sites such as the gastric antrum, the duodenum, and the sigmoid colon when planning the operation. At the same time, we should inspect for secondary damages caused by the gastrointestinal tract perforation. According to the literature the most common additional organs affected are the liver,[5] the pancreas, the kidney, the gall bladder, and the inferior vena cava.[10] Patient mortality due to the ingestion of a toothpick has been reported.[4] In our series of case studies, there was 1 patient with secondary damage to the liver, the toothpick had penetrated the liver through the anterior gastric wall with the consequent formation of a liver abscess. Following a course of intravenous antibiotic therapy, the toothpick was removed via laparoscopic surgery, with further antibiotic treatment after the operation (Table 1).
Table 1.
Clinical characteristics of 5 patients.

3.3. Treatment
In the surgical management of toothpick ingestion, we need to invest more time and pay special attention for signs of secondary injury sites. If the perforation site is located in the upper gastrointestinal tract or colorectum without any complications of secondary injuries to the liver or the pancreas, nor the formation of an intra-abdominal abscess, then the toothpick may be removed by therapeutic endoscopy. During the process of removal, the complete removal of the toothpick should be confirmed, if the toothpick is not completely removed or the toothpick failed to be removed by endoscopy, then the patient should proceed to surgery.[9–11] In the published literature, the surgical approach is predominantly via laparotomy, and the fraction by laparoscopic surgery is less than 10%.[12] In general, laparoscopic surgery possesses the following potential advantages:[9,13] (1) smaller incisions, better cosmesis, less pain, and faster recovery. At the same time, in cases with abdominal infection due to the perforation, laparoscopy can reduce the infection rate of an open incision and facilitate a shorter length of stay; (2) broad visual field, the access to the epigastrium is adequate and, in our experience, with careful trocar positioning the toothpick can be removed reliably, and the perforation site can be repaired via intracorporal suturing; (3) local drainage can be inserted at the infected site to prevent further abdominal contamination, and the entire abdominal cavity can be washed out at the same time. All 5 patients underwent successful laparoscopic surgery, with complete toothpick removal and purse string sutured repair of the perforation sites. Postoperative recoveries were successful and had no further complications (Table 2).
Table 2.
Surgical outcome in 5 cases.

4. Conclusion
In summary, we suggest that in patients who present an acute abdominal pain, after acute appendicitis digestive ulcers and other common abdominal malignancies have been excluded, we should consider the possibility of the perforation caused by ingested foreign bodies, especially toothpicks. When clinically suspected, auxiliary examinations such as CT scans, should be undertaken to confirm and localize the site of perforation and then extract the toothpick via laparoscopic surgery. Meanwhile, we recommend to inform the public about the hazards of toothpick misuse, especially under the influence of alcohol.
Footnotes
Abbreviations: CRP = C-reactive protein, CT = computed tomography, LAP = laparoscopy, NEUT = neutrophil count, WBC = white blood cell.
YZF and WDQ equally contributed to this article.
Informed Consent: All the patients provided an informed consent prior to surgery. We have obtained an ethical approval for this case series from the hospital's ethical board/committee, and a signed consent for publication from the patients.
Funding: This study is supported by Natural Science Foundation of Guangdong Province (2016A030310328). Research was funded by the Guangdong General Hospital, Guangzhou, China.
The authors have no conflicts of interest to disclose.
References
- [1].Schoffstall JM, Mcnamara RM. More on ingestion of a toothpick. N Engl J Med 1989;321:476–7. [PubMed] [Google Scholar]
- [2].Gelsomino S, Romagnoli S, Stefano P. Right coronary perforation due to a toothpick ingested at a barbecue. N Engl J Med 2005;352:2249–50. [DOI] [PubMed] [Google Scholar]
- [3].Budnick LD. Toothpick-related injuries in the United States, 1979 through 1982. JAMA 1984;252:796–7. [PubMed] [Google Scholar]
- [4].Bee DM, Citron M, Vannix RS, et al. Delayed death from ingestion of a toothpick. N Engl J Med 1989;320:673. [DOI] [PubMed] [Google Scholar]
- [5].Bloch DB. Venturesome toothpick. A continuing source of pyogenic hepatic abscess. JAMA 1984;252:797–8. [DOI] [PubMed] [Google Scholar]
- [6].Malamud D, Murphy MH. Martini toothpick warning. N Engl J Med 1986;315:1031–2. [PubMed] [Google Scholar]
- [7].Li SF, Ender K. Toothpick injury mimicking renal colic: case report and systematic review. J Emerg Med 2002;23:35–8. [DOI] [PubMed] [Google Scholar]
- [8].Mark D, Ferris K, Martel G, et al. Radiological diagnosis of a small bowel perforation secondary to toothpick ingestion. BMJ Case Rep 2013;2013:pii: bcr2013009869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Dente M, Santi F, Solinas L, et al. Laparoscopic diagnosis and management of jejunal perforation resulting from accidental toothpick ingestion. Am Surg 2009;75:178–9. [PubMed] [Google Scholar]
- [10].Lynch SM, Wu GY. A novel dual snare technique for removing long sharp foreign bodies. J Dig Dis 2016;17:274–6. [DOI] [PubMed] [Google Scholar]
- [11].Kim J, Ahn JY, So S, et al. Fluoroscopy-guided endoscopic removal of foreign bodies. Clin Endosc 2017;50:197–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Steinbach C, Stockmann M, Jara M, et al. Accidentally ingested toothpicks causing severe gastrointestinal injury: a practical guideline for diagnosis and therapy based on 136 case reports. World J Surg 2013;38:371. [DOI] [PubMed] [Google Scholar]
- [13].Schwartz JT, Graham DY. Toothpick perforation of the intestines. Ann Surg 1977;185:64–6. [DOI] [PMC free article] [PubMed] [Google Scholar]