

Abstract
Background
Hypoglycemia occurs in an appreciable number of individuals with type 2 diabetes mellitus (T2DM) who are receiving glycemic therapy. Iatrogenic hypoglycemia induces not only complications but also a substantial medical expense. Intervention for relevant risk factors may help avert severe hypoglycemia and enhance quality of life in at-risk individuals. This study investigates the relationship between body mass index (BMI) and plasma glucose concentration during iatrogenic hypoglycemia in people with T2DM.
Methods
Enrollment criteria were people above 20 years of age, with existing diagnosis of T2DM, a documented plasma glucose level ≤70 mg/dL, and acute cognitive impairment requiring hospitalization. Participants were classified into two groups according to their BMI. Specifically, lower BMI subgroup denotes individuals whose BMI fall within lower half of the study population, and vice versa. Plasma glucose concentration, length of hospital stay, and serum electrolyte level at hospitalization were compared between these BMI subgroups. Moreover, multivariate regression analysis was performed to identify covariates associated with plasma glucose level during iatrogenic hypoglycemia.
Results
This study enrolled 107 participants for whom 54 were assigned to a higher BMI subgroup and the remainder to a lower BMI subgroup. People with lower BMI harbored substantially reduced plasma glucose concentration during iatrogenic hypoglycemia compared to those with higher BMI (30.1 ± 9.6 mg/dL vs. 38.4 ± 12.3 mg/dL, P < 0.001). Nonetheless, the length of stay (6.2 ± 4.6 days vs. 5.7 ± 4.0 days, P = 0.77) and serum potassium level (3.7 ± 0.9 meq/L vs. 3.9 ± 0.8 meq/L, P = 0.14) were comparable between subgroups. Multivariate regression analysis identified BMI as a determinant of plasma glucose concentration in diabetic individuals with iatrogenic hypoglycemia (β coefficient: 0.72, P = 0.008).
Discussion
In individuals with T2DM who experience severe iatrogenic hypoglycemia, BMI influences the plasma glucose level at hospitalization. People with lower BMI harbored appreciably reduced plasma glucose concentration relative to their higher BMI counterparts. In lower weight people, therefore, appropriate dosing of antidiabetic medications, frequent self-monitoring of blood glucose level and adequate nutritional support may help avert more severe hypoglycemia. Overall, BMI potentially influences the severity of iatrogenic hypoglycemia in people with T2DM.
Keywords: Type 2 diabetes mellitus, Body mass index, Complications, Hypoglycemia
Introduction
Hypoglycemia occurs in an appreciable number of individuals with type 2 diabetes mellitus (T2DM) who are receiving antidiabetic therapy (Shafiee et al., 2012). Iatrogenic hypoglycemia induces not only complications but also a substantial medical expense related to hospitalization (Rhee et al., 2016). Prevention of hypoglycemia in diabetes is therefore an integral component of treatment (Clayton, Woo & Yale, 2013). Importantly, intervention for relevant risk factors may reduce severe hypoglycemia and enhance quality of life in people with T2DM.
Iatrogenic hypoglycemia is associated with clinical complications. Elderly people with recurrent hypoglycemia are at risk of cognitive impairment (McNay & Cotero, 2010). Severe hypoglycemia also contributes to a higher incidence of cardiovascular event and mortality (Hanefeld, Frier & Pistrosch, 2016). Moreover, risk of traumatic injury is notably increased in patients who experience severe hypoglycemia (Kachroo et al., 2015).
Epidemiologic studies have identified several risk factors for hypoglycemia in people with T2DM. Stringent glycemic targets are closely linked to the incidence of hypoglycemia (Lipska et al., 2013). In addition, severe hypoglycemia occurs more frequently in the elderly, presumably due to lack of symptom recognition (Abdelhafiz et al., 2015). Studies have also implicated diabetes duration as a risk factor, as demonstrated by progressive deterioration of hypoglycemic counterregulatory mechanism in people with longstanding disease (Dailey et al., 2013; Amiel et al., 2008).
The body mass index (BMI), as defined by dividing the weight in kilograms by the square of the height in meters, may be an important but overlooked risk factor for severe hypoglycemia. People with T2DM who have a lower BMI are also likely to have lower hepatic glycogen stores and this can diminish the secretion of glucose counterregulatory hormones during hypoglycemia (Winnick et al., 2016). Reduced counterregulatory hormones may compromise an individual’s capacity to stabilize blood glucose level during fasting (Izumida et al., 2013). Furthermore, lower BMI in elderly individuals may reflect underlying frailty (Lee et al., 2014), which impairs both the recognition of and behavioral defense against hypoglycemia.
This study investigates the relationship between BMI and plasma glucose concentration during iatrogenic hypoglycemia in people with T2DM.
Materials and Methods
This is a cross-sectional study conducted at Changhua Christian Hospital in central Taiwan. Individuals hospitalized at the Endocrinology ward from September 2011 to August 2017 were assessed for eligibility. Enrollment criteria were people above 20 years of age, with existing diagnosis of T2DM, a documented plasma glucose level ≤70 mg/dL (Cryer, 2015), and acute cognitive impairment that required hospitalization.
Candidates were excluded if they had chronic infection, traumatic injury, acute cerebro- or cardiovascular event, organ failure, or whose hypoglycemia was considered independent of antidiabetic medications. Moreover, people with malignancy, eating disorders, and previous gastrointestinal surgery were ineligible. The study was approved by the Institutional Review Board of Changhua Christian Hospital (CCH IRB number: 171105). Written consent to participate in the study was provided by the patients’ next of kin.
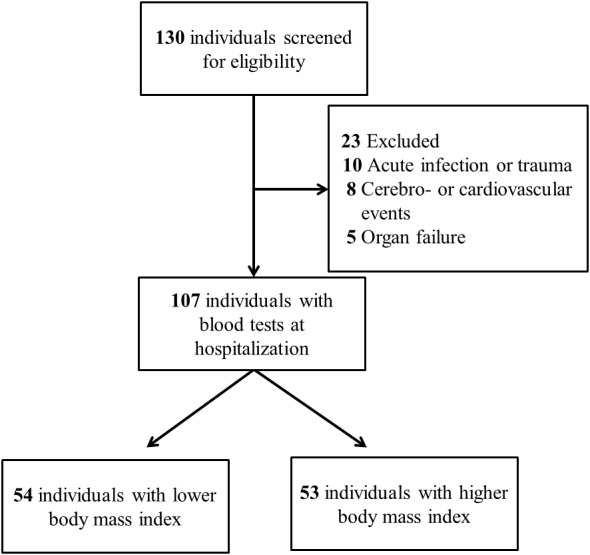
Participants were assigned to two equally sized subgroups according to their BMI. Specifically, lower BMI subgroup denotes individuals whose BMI fall within lower half of the study population, and vice versa. Blood tests were performed at hospitalization except for glycosylated hemoglobin A1c (HbA1c), which was extracted from existing laboratory data prior to the hypoglycemic event. Serum HbA1c was measured by ion-exchange high-performance liquid chromatography using BioRad VARIANT™ II Turbo system. Serum biochemistry including glucose, creatinine, and potassium were measured by Beckman Coulter UniCel DxC 800 Synchron™ Clinical Systems (Beckman Coulter, Brea, CA, USA). The analytical precision for serum glucose is within 2 mg/dL. Prescription details were collected from electronic medical records. The enrollment process is illustrated in Fig. 1.
Figure 1. Enrollment process of the study.
Demographic data between BMI subgroups were compared using Mann–Whitney U test for continuous variables and Pearson’s χ2 test for categorical variables. The plasma glucose concentration, serum potassium, and length of hospital stay were compared using Mann–Whitney U test. Multivariate regression analysis was performed to identify predictors of plasma glucose level at hospitalization. A two-tailed P value of less than 0.05 indicated statistical significance. Analysis was performed using IBM SPSS version 22.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA).
Results
The study enrolled 107 participants with T2DM who were hospitalized due to severe iatrogenic hypoglycemia. As shown in Table 1, demographic characteristics including age (76.5 ± 13.8 years vs. 73.8 ± 11.7 years, P = 0.172), preceding HbA1c (6.7 ± 1.1% vs. 6.8 ± 1.3%, P = 0.52), duration of diabetes (7.6 ± 4.5 years vs. 9.3 ± 4.9 years, P = 0.051), and serum creatinine (1.6 ± 1.0 mg/dL vs. 1.9 ± 1.6 mg/dL, P = 0.336) were comparable between BMI subgroups. Moreover, the proportion of participants using antidiabetic medication commonly implicated in iatrogenic hypoglycemia, such as insulin (26% vs. 32%, P = 0.31) or sulfonylurea (65% vs. 64%, P = 0.55), were also similar.
Table 1. Demographic characteristics of the body mass index subgroups.
| Variables | Lower BMI (n = 54) | Higher BMI (n = 53) | P value |
|---|---|---|---|
| Age (years) | 76.5 ± 13.8 | 73.8 ± 11.7 | 0.172 |
| Sex (Female) | 29 (54%) | 29 (55%) | 0.53 |
| BMI (kg/m2) | 20.1 ± 1.78 | 27.0 ± 3.90 | <0.001 |
| HbA1c (%) | 6.7 ± 1.1 | 6.8 ± 1.3 | 0.52 |
| Creatinine (mg/dL) | 1.60 ± 1.00 | 1.91 ± 1.63 | 0.336 |
| Duration of diabetes (years) | 7.6 ± 4.5 | 9.3 ± 4.9 | 0.051 |
| Use of insulin | 14 (26%) | 17 (32%) | 0.31 |
| Use of sulfonylurea | 35 (65%) | 34 (64%) | 0.55 |
Notes.
Data are expressed as mean with standard deviation for continuous variables and number (%) for categorical variables. Continuous variables were compared using the Mann–Whitney U test for independent samples.
- BMI
- body mass index
- HbA1c
- glycated hemoglobin A1c
As demonstrated in Table 2, participants with lower BMI harbored substantially reduced plasma glucose concentration compared to those with higher BMI during iatrogenic hypoglycemia (30.1 ± 9.6 mg/dL vs. 38.4 ± 12.3 mg/dL, P < 0.001). Nonetheless, individuals with lower BMI did not have an appreciably longer length of stay compared to their higher weight counterparts (6.2 ± 4.6 days vs. 5.7 ± 4.0 days, P = 0.77). Furthermore, mean serum potassium levels were similar between subgroups (3.7 ± 0.9 meq/L vs. 3.9 ± 0.8 meq/L, P = 0.14).
Table 2. Clinical features of the body mass index subgroups.
| Variables | Lower BMI (n = 54) | Higher BMI (n = 53) | P value |
|---|---|---|---|
| Plasma glucose concentration (mg/dL) | 30.1 ± 9.61 | 38.4 ± 12.3 | <0.001 |
| Length of stay (days) | 6.2 ± 4.6 | 5.7 ± 4.0 | 0.77 |
| Potassium (mEq/L) | 3.7 ± 0.86 | 3.9 ± 0.80 | 0.14 |
Notes.
Data are expressed as mean with standard deviation for continuous variables. Continuous variables were compared using the Mann–Whitney U test for independent samples.
- BMI
- body mass index
Multivariate regression analysis identified covariates that potentially influence the plasma glucose concentration at hospitalization. The standardized coefficient of each independent variable is listed in Table 3. As can be seen, BMI was significantly related to plasma glucose concentration during iatrogenic hypoglycemia in people with T2DM (β coefficient: 0.72, P = 0.008) after adjusting for confounding variables.
Table 3. Multivariate regression analysis of covariates associated with plasma glucose concentration during iatrogenic hypoglycemia.
| Covariates | β coefficient | P value |
|---|---|---|
| Age (years) | 0.014 | 0.88 |
| BMI (kg/m2) | 0.72 | 0.008 |
| HbA1c (%) | −1.18 | 0.26 |
| Creatinine (mg/dL) | −1.1 | 0.21 |
| Duration of diabetes (years) | −0.037 | 0.88 |
Notes.
- BMI
- body mass index
- HbA1c
- glycated hemoglobin A1c
Discussion
People with T2DM are vulnerable to the detrimental effect of hypoglycemia, which may become a limiting factor in antidiabetic therapy (Seaquist et al., 2013). Apart from requiring the assistance of caregivers, severe hypoglycemia also induces harmful cardiac arrhythmia and functional brain failure (Chow et al., 2014). Moreover, hypoglycemia-associated autonomic failure can impair the physiologic and behavioral defense against a subsequent hypoglycemic event (Cryer, 2013a; Cryer, 2013b).
The observation in this study that lower weight people with T2DM had reduced plasma glucose concentration during iatrogenic hypoglycemia may be attributable to attenuated glucose counterregulatory mechanisms. People with lower BMI, perhaps reflecting less availability of hepatic glycogen, may have diminished secretion of glucagon and epinephrine (Winnick et al., 2016), resulting in inadequate hepatic glucose production during iatrogenic hypoglycemia. Furthermore, the effect of glucagon may be compromised in people with inadequate glycogen since this hormone raises blood glucose level through hepatic glycogenolysis (Melmed et al., 2016).
Moreover, unintentional weight loss may reflect frailty and functional disability (Xue, 2011). In lower weight people, delayed recognition of hypoglycemia may partly explain their appreciably lower plasma glucose level at hospitalization. People with lower BMI may therefore have limited ability to counteract hypoglycemia due to reduced secretion of glucose counterregulatory hormones, as discussed previously, and functional disability that leads to hypoglycemic unawareness.
Adipose tissue modifies insulin sensitivity through the production of adipokines (Waki & Tontonoz, 2007; Fasshauer & Blüher, 2015). Weight loss improves insulin sensitivity by decreasing free fatty acid mobilization and by changing adipokine profile in obesity (Schenk et al., 2009; Greco et al., 2014). Moreover, intentional weight loss in T2DM correlates with lower fasting plasma glucose concentration (Wing et al., 2011). Weight loss is therefore an established risk factor for iatrogenic hypoglycemia in diabetes (Melmed et al., 2016). In clinical practice, BMI may indirectly mirror an individual’s insulin sensitivity and subsequent risk of hypoglycemia. Therefore, dynamic change in body weight during glycemic treatment may require a corresponding adjustment in therapeutic regimen.
Intriguingly, although participants with lower BMI harbored reduced plasma glucose level at hospitalization, length of stay and serum potassium level were similar to their higher BMI counterparts. In other words, hypoglycemia may not cause immediately perceivable complications. Nonetheless, plasma glucose level below 30 mg/dL has been linked to permanent brain injury in an animal model (Oyer, 2013), and lower weight people in this study with a mean blood glucose close to this level were at risk of long-term neurologic damage.
Several implications arise from the study’s finding that lower weight participants had reduced plasma glucose level during iatrogenic hypoglycemia. Hypoglycemia in diabetes involves a combination of therapeutic insulin excess and compromised physiologic defense (Cryer, 2013a; Cryer, 2013b). Appropriate dosing of antidiabetic medications, especially sulfonylurea and insulin (Heller et al., 2007), is prudent for people with lower BMI. Lower weight people may also benefit from less stringent treatment target, frequent self-monitoring of blood glucose (SMBG), and continuous glucose monitoring (CGM) to detect asymptomatic hypoglycemia (Cryer, 2014). Nutritional support to increase hepatic glycogen in at risk individuals may enhance physiologic defense against more severe hypoglycemia (Décombaz et al., 2011). Moreover, since the glucose-raising efficacy of glucagon is unreliable in people with inadequate glycogen, an alternative method may be necessary to restore normoglycemia in underweight patients.
The design of this study has limitations. To be hospitalized for treatment, participants obviously circumvented lethal complications such as cardiac arrhythmia, which may lead to selection bias. Furthermore, participants may have initially received management for hypoglycemia at home, and blood tests at hospitalization may not reveal the lowest plasma glucose concentration. A longer observation time may be necessary to identify potential complications associated with severe hypoglycemia. Hypoglycemic risk may also relate to the dose of antidiabetic medications, which was not addressed by the study. Moreover, neither hepatic glycogen quantity nor counterregulatory hormone level was measured, both of which may influence the severity of iatrogenic hypoglycemia.
Conclusions
Lower weight individuals with T2DM harbored reduced plasma glucose concentration during iatrogenic hypoglycemia. People with lower BMI may have compromised defense against iatrogenic hypoglycemia due to reduced secretion of counterregulatory hormones and functional disability. Appropriate dosing of antidiabetic medications, individualized treatment target, frequent SMBG and CGM technology may help avert more severe hypoglycemia in people with lower BMI. Ultimately, nutritional support to increase hepatic glycogen may defend lower weight patients against severe hypoglycemia.
Supplemental Information
Funding Statement
The authors received no funding for this work.
Additional Information and Declarations
Competing Interests
The authors declare there are no competing interests.
Author Contributions
Po Chung Cheng conceived and designed the experiments, performed the experiments, contributed reagents/materials/analysis tools, wrote the paper, reviewed drafts of the paper.
Shang Ren Hsu and Shih Te Tu conceived and designed the experiments, performed the experiments, wrote the paper, reviewed drafts of the paper.
Yun Chung Cheng analyzed the data, wrote the paper, prepared figures and/or tables, reviewed drafts of the paper.
Yu Hsiu Liu analyzed the data, contributed reagents/materials/analysis tools, wrote the paper, prepared figures and/or tables, reviewed drafts of the paper, qualified statistician.
Human Ethics
The following information was supplied relating to ethical approvals (i.e., approving body and any reference numbers):
The study was approved by the Institutional Review Board of Changhua Christian Hospital (CCH IRB number: 171105).
Data Availability
The following information was supplied regarding data availability:
The raw data is provided as a Supplemental File.
References
- Abdelhafiz et al. (2015).Abdelhafiz AH, Rodríguez-Mañas L, Morley JE, Sinclair AJ. Hypoglycemia in older people—a less well recognized risk factor for frailty. Aging and Disease. 2015;6:156–167. doi: 10.14336/AD.2014.0330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amiel et al. (2008).Amiel SA, Dixon T, Mann R, Jameson K. Hypoglycaemia in type 2 diabetes. Diabetic Medicine. 2008;25:245–254. doi: 10.1111/j.1464-5491.2007.02341.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chow et al.(2014).Chow E, Bernjak A, Williams S, Fawdry RA, Hibbert S, Freeman J, Sheridan PJ, Heller SR. Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk. Diabetes. 2014;63(5):1738–1747. doi: 10.2337/db13-0468. [DOI] [PubMed] [Google Scholar]
- Clayton, Woo & Yale (2013).Clayton D, Woo V, Yale JF. Hypoglycemia. Canadian Journal of Diabetes. 2013;37(Suppl 1):S69–S71. doi: 10.1016/j.jcjd.2013.01.022. [DOI] [PubMed] [Google Scholar]
- Cryer (2013a).Cryer PE. Hypoglycemia in diabetes: pathophysiology, prevalence and prevention. 2nd Edition American Diabetes Association; Alexandria: 2013a. [Google Scholar]
- Cryer (2013b).Cryer PE. Mechanisms of hypoglycemia-associated autonomic failure in diabetes. New England Journal of Medicine. 2013b;369:362–372. doi: 10.1056/NEJMra1215228. [DOI] [PubMed] [Google Scholar]
- Cryer (2014).Cryer PE. Glycemic goals in diabetes: trade-off between glycemic control and iatrogenic hypoglycemia. Diabetes. 2014;63:2188–2195. doi: 10.2337/db14-0059. [DOI] [PubMed] [Google Scholar]
- Cryer (2015).Cryer PE. Minimizing hypoglycemia in diabetes. Diabetes Care. 2015;38:1583–1591. doi: 10.2337/dc15-0279. [DOI] [PubMed] [Google Scholar]
- Dailey et al. (2013).Dailey GE, Gao L, Aurand L, Garg SK. Impact of diabetes duration on hypoglycaemia in patients with type 2 diabetes treated with insulin glargine or NPH insulin. Diabetes, Obesity and Metabolism. 2013;15:1085–1092. doi: 10.1111/dom.12131. [DOI] [PubMed] [Google Scholar]
- Décombaz et al. (2011).Décombaz J, Jentjens R, Ith M, Scheurer E, Buehler T, Jeukendrup A, Boesch C. Fructose and galactose enhance postexercise human liver glycogen synthesis. Medicine and Science in Sports and Exercise. 2011;43:1964–1971. doi: 10.1249/MSS.0b013e318218ca5a. [DOI] [PubMed] [Google Scholar]
- Fasshauer & Blüher (2015).Fasshauer M, Blüher M. Adipokines in health and disease. Trends in Pharmacological Sciences. 2015;36:461–470. doi: 10.1016/j.tips.2015.04.014. [DOI] [PubMed] [Google Scholar]
- Greco et al. (2014).Greco M, Chiefari E, Montalcini T, Accattato F, Costanzo FS, Pujia A, Foti D, Brunetti A, Gulletta E. Early effects of a hypocaloric, Mediterranean diet on laboratory parameters in obese individuals. Mediators of Inflammation. 2014;2014:750860–750868. doi: 10.1155/2014/750860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanefeld, Frier & Pistrosch (2016).Hanefeld M, Frier BM, Pistrosch F. Hypoglycemia and cardiovascular risk: is there a major link? Diabetes Care. 2016;39(Suppl 2):S205–S209. doi: 10.2337/dcS15-3014. [DOI] [PubMed] [Google Scholar]
- Heller et al. (2007).Heller SR, Choudhary P, Davies C, Emery C, Campbell MJ, Freeman J, Amiel SA, Malik R, Frier BM, Allen KV, Zammitt NN, Macleod K, Lonnen KF, Kerr D, Richardson T, Hunter S, Mclaughlin D. Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia. 2007;50:1140–1147. doi: 10.1007/s00125-007-0599-y. [DOI] [PubMed] [Google Scholar]
- Izumida et al. (2013).Izumida Y, Yahagi N, Takeuchi Y, Nishi M, Shikama A, Takarada A, Masuda Y, Kubota M, Matsuzaka T, Nakagawa Y, Iizuka Y, Itaka K, Kataoka K, Shioda S, Niijima A, Yamada T, Katagiri H, Nagai R, Yamada N, Kadowaki T, Shimano H. Glycogen shortage during fasting triggers liver–brain–adipose neurocircuitry to facilitate fat utilization. Nature Communications. 2013;4:2316–2324. doi: 10.1038/ncomms3316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kachroo et al. (2015).Kachroo S, Kawabata H, Colilla S, Shi L, Zhao Y, Mukherjee J, Iloeje U, Fonseca V. Association between hypoglycemia and fall-related events in type 2 diabetes mellitus: analysis of a U.S. commercial database. Journal of Managed Care & Specialty Pharmacy. 2015;21:243–253. doi: 10.18553/jmcp.2015.21.3.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee et al. (2014).Lee Y, Kim J, Han ES, Ryu M, Cho Y, Chae S. Frailty and body mass index as predictors of 3-year mortality in older adults living in the community. Gerontology. 2014;60:475–482. doi: 10.1159/000362330. [DOI] [PubMed] [Google Scholar]
- Lipska et al. (2013).Lipska KJ, Warton EM, Huang ES, Moffet HH, Inzucchi SE, Krumholz HM, Karter AJ. HbA1c and risk of severe hypoglycemia in type 2 diabetes: the Diabetes and aging study. Diabetes Care. 2013;36(11):3535–3542. doi: 10.2337/dc13-0610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNay & Cotero (2010).McNay EC, Cotero VE. Mini-review: impact of recurrent hypoglycemia on cognitive and brain function. Physiology and Behavior. 2010;100:234–238. doi: 10.1016/j.physbeh.2010.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melmed et al. (2016).Melmed S, Polonsky KS, Larsen PR, Kronenberg HM. Williams textbook of endocrinology. 13th edition Elsevier; 2016. [Google Scholar]
- Oyer (2013).Oyer DS. The science of hypoglycemia in patients with diabetes. Current Diabetes Reviews. 2013;9:195–208. doi: 10.2174/15733998113099990059. [DOI] [PubMed] [Google Scholar]
- Rhee et al. (2016).Rhee SY, Hong SM, Chon S, Ahn KJ, Kim SH, Baik SH, Park YS, Nam MS, Lee KW, Woo JT, Kim YS. Hypoglycemia and medical expenses in patients with type 2 diabetes mellitus: an analysis based on the Korea National Diabetes Program Cohort. PLOS ONE. 2016;11(2):e0148630. doi: 10.1371/journal.pone.0148630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schenk et al. (2009).Schenk S, Harber MP, Shrivastava CR, Burant CF, Horowitz JF. Improved insulin sensitivity after weight loss and exercise training is mediated by a reduction in plasma fatty acid mobilization, not enhanced oxidative capacity. Journal de Physiologie. 2009;587:4949–4961. doi: 10.1113/jphysiol.2009.175489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seaquist et al. (2013).Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, Heller SR, Rodriguez H, Rosenzweig J, Vigersky R. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care. 2013;36(5):1384–1395. doi: 10.2337/dc12-248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shafiee et al. (2012).Shafiee G, Mohajeri-Tehrani M, Pajouhi M, Larijan B. The importance of hypoglycemia in diabetic patients. Journal of Diabetes & Metabolic Disorders. 2012;11:17–24. doi: 10.1186/2251-6581-11-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waki & Tontonoz (2007).Waki H, Tontonoz P. Endocrine functions of adipose tissue. Annual Review of Pathology. 2007;2:31–56. doi: 10.1146/annurev.pathol.2.010506.091859. [DOI] [PubMed] [Google Scholar]
- Wing et al. (2011).Wing RR, Lang W, Wadden TA, Safford M, Knowler WC, Bertoni AG, Hill JO, Brancati FL, Peters A, Wagenknecht L. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care. 2011;34:1481–1486. doi: 10.2337/dc10-2415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winnick et al. (2016).Winnick JJ, Kraft G, Gregory JM, Edgerton DS, Williams P, Hajizadeh IA, Kamal MZ, Smith M, Farmer B, Scott M, Neal D, Donahue EP, Allen E, Cherrington AD. Hepatic glycogen can regulate hypoglycemic counterregulation via a liver-brain axis. Journal of Clinical Investigation. 2016;126:2236–2248. doi: 10.1172/JCI79895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xue (2011).Xue QL. The frailty syndrome: definition and natural history. Clinics in Geriatric Medicine. 2011;27:1–15. doi: 10.1016/j.cger.2010.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The following information was supplied regarding data availability:
The raw data is provided as a Supplemental File.