

Abstract
Context:
Carpal tunnel syndrome (CTS) is one of the most common peripheral neuropathies, and there is no consensus on the preferred method of treatment.
Aims:
The aim of this study is to determine the effects of hand exercise performed with a ball on symptoms and to evaluate the results in hemodialysis (HD) patients with CTS.
Settings and Design:
This study was conducted in patients with HD who were treated in dialysis centers and state hospitals in Turkey between 2011 and 2012.
Subjects and Methods:
This study included 19 patients (28 hands) that were diagnosed as CTS. For exercise treatment, a hand and finger exercise ball that consists of two parts: a foam body and flexible rubber cords was used. Patients placed their fingers through each cord, squeezed it for 1 s, and then opened their fingers against the cord for 1 s. Patients repeated this exercise for 30 s to 1 min/day.
Statistical Analysis Used:
The McNemar, Friedman ANOVA, and the Wilcoxon test with a Bonferroni correction were used on SPSS 20.0 software package program. P < 0.05 was considered statistically significant.
Results:
Results showed that recovery was performed from physical examination results, grip strength, and Boston questionnaire scores. About 21.4% of patients’ electrophysiological results were negative at the end of the 1st month and 32.1% of them at the end of the 3rd month.
Conclusion:
Due to the slowed progress of CTS and detection of slight improvement in evaluation parameters, this self-applicable and practical exercise can be used as an alternative treatment of mild CTS in patients with HD.
Keywords: Carpal tunnel syndrome, exercise, hand, hemodialysis
Introduction
Carpal tunnel syndrome (CTS) is one of the most common peripheral neuropathies. Increased intracarpal tunnel pressure plays an important role in the etiology of CTS. This affects the circulation of the median nerve, and intermittent changes in pressure lead to nerve damage. Repetitive flexion/extension movements and forceful sustained motions are also important risk factors of CTS.[1,2] Long-term hemodialysis (HD) is also a well-known cause of CTS. The prevalence ranges between 2% and 30% for patients with HD.[3,4] Although numerous studies have been performed since the first report of CTS developing in patients with HD, the true pathogenesis is not clearly understood.[5,6]
Due to limited evidence, there is no consensus on the preferred method of treatment for CTS. Surgical release of the transverse carpal ligament is commonly performed in patients with severe symptoms of HD-associated CTS. Advocates of conservative options refer to the potential benefits and complications of surgery.[5,7] However, the American Academy of Orthopedic Surgeons recommends starting with a conservative treatment, and if it fails to resolve the symptoms within 2–7 weeks, trying another nonoperative treatment or surgery.[8] Seradge et al. demonstrated through measurements of carpal tunnel pressure in vivo that intermittent exercises with active wrist and finger motions for 1 min can lower pressure in the carpal tunnel.[9] These exercises may have a positive effect on CTS by facilitating venous return or edema in the median nerve. By stretching and lengthening the restrictive flexor muscles that “close” the hands and strengthening and shortening the extensor muscles that “open” the hands, the carpal tunnel can return to its normal size. In addition, decreasing impingement of the tendons and median nerve eliminates friction and carpal tunnel symptoms.[10]
Because studies on exercise treatment in CTS and include exercise treatment for patients with HD are scarce, this study aimed to determine the effects of the exercise performed with a ball on symptoms and the evaluation results.
Subjects and Methods
This one-group pretest–posttest designed quasi-experimental study was conducted in patients with HD who were treated in dialysis centers and state hospitals in Bursa City Center, Turkey, between October 15, 2011, and October 16, 2012. Ethical approval was received from the Medical Faculty Research Ethics Committee (2011-3/10). Permission to conduct this study was obtained from the Bursa Provincial Directorate of Health and institutional approval of the study and publication was obtained from the clinical directors of the dialysis centers. Information about the study was given to all patients, and informed consent of the patients to be enrolled and have their data published was obtained.
One thousand and ten patients with HD underwent treatment at the dialysis centers and state hospitals during the study; 436 patients were excluded for having metabolic disorders such as diabetes mellitus, thyroid disease, or rheumatoid arthritis; history of carpal tunnel surgery; physiotherapy, hand and arm deformity; or diagnosis of severe CTS. Using the self-administered Katz hand diagrams, an additional 466 patients were excluded because they had “unlikely” CTS patterns. Based on the clinical and electrophysiologic test results, 19 patients (28 hands) with a diagnosis of mild and moderate stage CTS were included in the study. They underwent dialysis for an average of 4 h and three times a week with a synthetic membrane. Sampling steps are shown in Flowchart 1.
Flowchart 1.
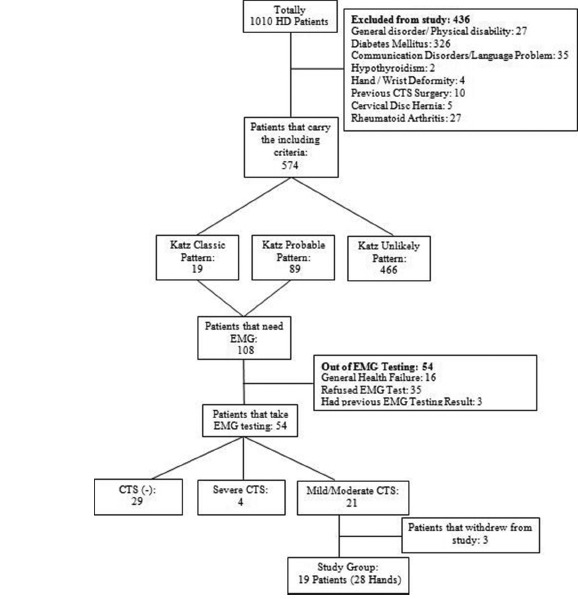
Sampling steps
Outcome assessments
Phalen and Tinel tests
Phalen test was performed with full flexion of the patients’ wrists for 60 s, and Tinel test was performed with percussion on the median nerve at the wrist. These tests were recorded as positive if the patient experienced paresthesia in at least one of three radial digits.
Carpal tunnel questionnaire
This is a self-report questionnaire and comprises two subscales. The 11-item symptom severity scale assesses symptoms such as pain, numbness, and tingling. Responses are recorded on a 5-point Likert scale, ranging from 1 (no symptoms) to 5 (most severe pain). The 8-item functional status scale measures daily activities that may be affected by hand and wrist symptoms (e.g., writing, buttoning, and opening a jar), and responses are recorded on a 5-point Likert scale, ranging from 1 (no difficulty) to 5 (cannot do all owing to hand or wrist symptoms). The scores for each scale are the average of the scale items. Higher scores indicate greater symptom severity and disability.[11]
Motor function
Motor function of the muscles of the hand was measured (in kg) with the Jamar hand dynamometer. All measurements were performed when the patient was in the sitting position, the shoulder in adduction and neutral position, the elbow in 90° flexion, and the forearm in a neutral position, and repeated three times by exerting the maximum force to ensure reliability. The mean value of the three measurements was recorded.[12,13]
Electrophysiologic test
Motor nerve conduction evaluations were conducted according to the recommendations by the American Association of Electrodiagnosis, the American Academy of Neurology, and the American Academy of Physical Medicine and Rehabilitation for diagnosing mild-to-moderate CTS.[13,14]
All the participants underwent these assessments at the baseline and after the 1- and 3-month exercise sessions. The assessments were carried out by the same researcher and neurologist.
Exercise protocol
This hand and finger exercise treatment was a home program in which patients were instructed to perform with a ball. This ball is a hand exercise therapy device that strengths nine muscles that close the hand and nine muscles that open and spread the hand. This therapy improves the balance between the muscles and increases the strength, balance, and blood flow to the hand, wrist, and elbow.
The exercise ball consists of two parts: a foam body and flexible rubber exercise cords. According to the user instructions, the neck and shoulder are kept in a neutral position, and the elbow remains at 90° of flexion and fingers are placed through each cord (Step 1). During the exercise, the patients squeezed the ball for 1 s (Step 2) and then opened their fingers against the cord for 1 s (Step 3). The exercise was performed actively for 30 s to 1 min, and patients instructed to continue with the exercise program at home two times/day for a 3-month period. Exercise steps are shown in Flowchart 2.
Flowchart 2.

Exercise steps
An educational brochure about exercise was given to patients, and they were informed to stop performing the exercises if they felt pain or fatigue. Patients recorded the time they performed the exercises every day on the monthly follow-up schedule. This schedule was given them at the beginning of the treatment, and they received instructions for filling out the schedule.
Statistics analysis
Continuous variables were expressed as the median and range or as a number and percentage. Categorical variables were expressed as relative frequencies. The McNemar Chi-square (χ2) test was used for the variables that consisted of two categories. The Friedman ANOVA test was used to compare quantitative values, and the Wilcoxon test with a Bonferroni correction was used to detect the significant differences between repeated measurements at the baseline, 1 month, and 3 months of exercise treatment. P < 0.05 was considered statistically significant.
The statistical analysis was performed by the Department of Biostatistics and Medical Informatics, and the SPSS 20.0 software package (SPSS Inc., Chicago, IL, USA) was used for all analysis.
Results
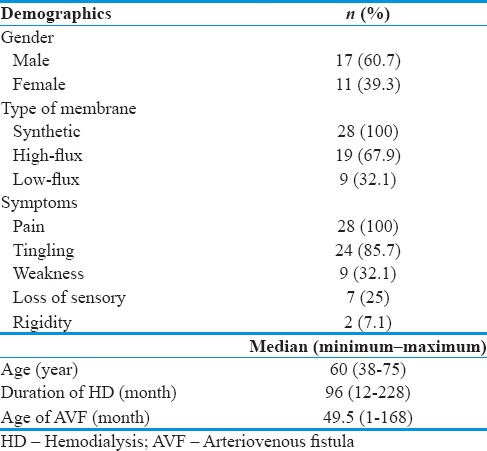
A total of 19 patients (28 hands) who met the criteria were included in the study. Demographic characteristics and clinical features of patients before the exercise treatment are shown in Table 1.
Table 1.
Demographic characteristics and clinical features of patients
The Tinel and Phalen test results were better at the end of the 1 and 3 months of the treatment than the baseline results. This difference between the baseline and 1-month rates was statistically significant (P0-1= 0.021) [Table 2].
Table 2.
Comparison of outcome measurements between treatment months
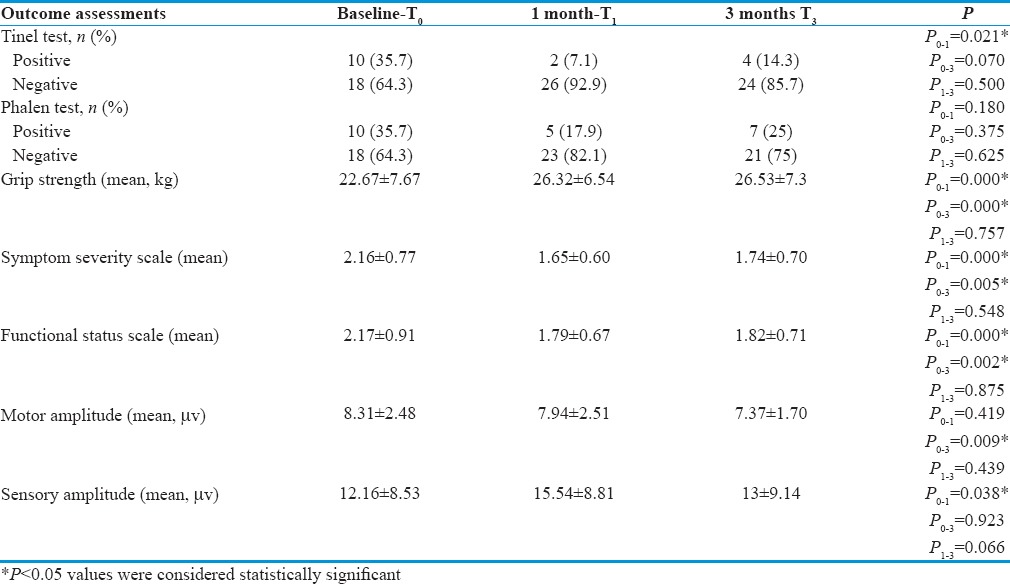
When the baseline and posttreatment parameters were compared, the handgrip strength scores were significantly improved (P0-1,0-3 < 0.001). All participants’ grip strength was significantly increased at the end of 3 months from 22.67 ± 7.67 to 26.53 ± 7.3 kg (P0-1 = 0.000, P0-3 = 0.000) [Table 2].
According to the symptom severity and functional status scales, there were statistically significant differences between the baseline, 1 month, and 3 months of treatment (symptom severity: p0-1 = 0.000, P0-3 = 0.005; functional status scale: p0-1 = 0.000, P0-3 = 0.002). Over time, patients had significantly decreased CTS symptoms and improved functional status [Table 2].
When the electrophysiological parameters were compared according to the treatment months, there was a significant decrease between the baseline and 3-month motor amplitude values (P0-3 = 0.009), whereas a significant increase was found in the sensory amplitude of the baseline and 1-month values (P0-1 = 0.038) [Table 2].
Discussion
Tendon gliding of the finger flexor tendons and nerve gliding of the median nerve exercises are recommended for conservative management of symptoms related to CTS.[15] In the literature, a significant improvement was found in the Phalen and Tinel test results in the nerve gliding exercise groups.[16,17] In the present study, the provocation test results were better at the end of the exercise treatment.
Strength may be an important factor in limiting the cellular damage that occurs from repetitive motion and increasing muscular strength by exercise training can have a protective effect against injury such as carpal tunnel disease.[18] In Legg's study, participants were trained with the powerball three times a week for 4 weeks, and each session lasted for 5 min. Using the powerball showed an overall increase in grip strength, and the device might have possible benefits as a rehabilitative tool for the wrist and arm.[19] Similarly, in Randolph's study, a significant increase in strength was observed following 6 weeks of exercise training.[20] In the present study, the grip strength of all the patients significantly improved. As is known, patients with HD try to protect their hands with a fistula and rarely move their hands during dialysis treatment. Using the ball may also help prevent CTS. Thus, this exercise ball can be used as a conservative treatment in mild CTS before trying any other nonoperative treatment type as steroids injection and can take place in the current treatment type of mild CTS in patients with HD [Figure 1].
Figure 1.

Hand exercise with ball
Nerve and tendon gliding exercises can resolve symptoms by stretching the adhesions in the carpal canal, improving venous return from the nerve bundles, and reducing pressure inside the carpal tunnel. In Madenci et al.'s study, the symptom's severity score was decreased, and the functional capacity score was increased in splint and massage groups, being more significant in the massage group.[21] Akalın et al. found that nerve and tendon gliding exercises were effective in decreasing the severity of symptoms and making hand function better in patients with CTS.[17] Baker and Livengood found that symptom severity and functional status scores were higher for participants who had surgery than participants who did not have surgery.[22] Similar to the literature, in this study, the participants had significantly decreased CTS symptoms and improved functional status. The results show, in treating CTS, starting with alternative treatment before surgical intervention is a rational approach.
Nerve conduction studies have been used to assess nerve compression for >30 years, and the most frequently used parameters are median sensory and motor distal latencies.[23] Field et al. found no statistically significant difference between nerve conduction velocity measures in participants who received 15 min massage therapy.[24] Keskin et al. found that at the 3rd and 6th months, the nerve and tendon gliding exercise group had a significant improvement in median motor nerve distal latency.[25] In this study, there was a significant decrease between the baseline and 3-month motor amplitude values, but there was a significant increase in the baseline and 1-month sensory amplitude values. CTS follows a progressive process. However, during this study, except for median motor distal amplitude, no symptom worsened.
Conclusion
This study evaluated the efficacy of hand and finger exercises performed with a ball in decreasing the symptoms of CTS in patients with HD who used the ball for 30 s to 1 min two times/day. This exercise treatment demonstrated no absolute contraindications, significant decrease in CTS symptoms, and improvement in functional status of patients with HD. The strengths of this study were reliable and valid outcome measures. As identified with the follow-up results of this study, the ball exercise treatment can be used as a conservative treatment for mild CTS. The additional benefits of this treatment are being self-administered, low cost, and practical. These are the advantages of this exercise to prefer before other alternative treatments.
Limitations
This study results were related only to patients with HD and mild-to-moderate CTS. Thus, these results cannot be generalized to other sample groups and severe CTS.
Financial support and sponsorship
The present study was supported by the Research Fund of Istanbul University. Project No. 13001.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We thank to neurologist N.G. for electrodiagnostic examinations during the study and thank all HD centers for giving permission and their patients for including in the study.
References
- 1.Aroori S, Spence RA. Carpal tunnel syndrome. Ulster Med J. 2008;77:6–17. [PMC free article] [PubMed] [Google Scholar]
- 2.Fung BK, Chan KY, Lam LY, Cheung SY, Choy NK, Chu KW, et al. Study of wrist posture, loading and repetitive motion as risk factors for developing carpal tunnel syndrome. Hand Surg. 2007;12:13–8. doi: 10.1142/S0218810407003341. [DOI] [PubMed] [Google Scholar]
- 3.Otsubo S, Kimata N, Okutsu I, Oshikawa K, Ueda S, Sugimoto H, et al. Characteristics of dialysis-related amyloidosis in patients on haemodialysis therapy for more than 30 years. Nephrol Dial Transplant. 2009;24:1593–8. doi: 10.1093/ndt/gfn706. [DOI] [PubMed] [Google Scholar]
- 4.Al-Homrany MA, Khan MR, Adzaku F, Harding MG. Carpal tunnel syndrome in haemodialysis patients: Early detection by electroneurophysiological studies. Nephrology. 2001;6:259–62. [Google Scholar]
- 5.Kang HJ, Koh IH, Lee WY, Choi YR, Hahn SB. Does carpal tunnel release provide long-term relief in patients with hemodialysis-associated carpal tunnel syndrome? Clin Orthop Relat Res. 2012;470:2561–5. doi: 10.1007/s11999-012-2309-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Walker JA. Management of patients with carpal tunnel syndrome. Nurs Stand. 2010;24:44–8. doi: 10.7748/ns2010.01.24.19.44.c7447. [DOI] [PubMed] [Google Scholar]
- 7.Atroshi I, Larsson GU, Ornstein E, Hofer M, Johnsson R, Ranstam J. Outcomes of endoscopic surgery compared with open surgery for carpal tunnel syndrome among employed patients: Randomised controlled trial. BMJ. 2006;332:1473. doi: 10.1136/bmj.38863.632789.1F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS); 2008. American Academy of Orthopaedic Surgeons and American Academy of Orthopaedic Surgeons. Clinical Practice Guideline on the Treatment of Carpal Tunnel Syndrome; pp. 1–33. [Google Scholar]
- 9.Seradge H, Bear C, Bithell D. Preventing carpal tunnel syndrome and cumulative trauma disorder: Effect of carpal tunnel decompression excercises: An Oklahoma experience. J Okla State Med Assoc. 2000;93:150–3. [PubMed] [Google Scholar]
- 10.MacDermid JC, Wessel J. Clinical diagnosis of carpal tunnel syndrome: A systematic review. J Hand Ther. 2004;17:309–19. doi: 10.1197/j.jht.2004.02.015. [DOI] [PubMed] [Google Scholar]
- 11.Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH, et al. Aself-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993;75:1585–92. doi: 10.2106/00004623-199311000-00002. [DOI] [PubMed] [Google Scholar]
- 12.Shechtman O, Gestewitz L, Kimble C. Reliability and validity of the DynEx dynamometer. J Hand Ther. 2005;18:339–47. doi: 10.1197/j.jht.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 13.Aygül R, Ulvi H, Kotan D, Kuyucu M, Demir R. Sensitivities of conventional and new electrophysiological techniques in carpal tunnel syndrome and their relationship to body mass index. J Brachial Plex Peripher Nerve Inj. 2009;4:12. doi: 10.1186/1749-7221-4-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schoenhuber R, Capone L, Gentile R, Pentore R. Carpal Tunnel Syndrome. 1st ed. Berlin Heidelberg: Springer; 2007. Neurophysiological assessment of carpal tunnel syndrome; pp. 69–74. [Google Scholar]
- 15.Michlovitz SL. Conservative interventions for carpal tunnel syndrome. J Orthop Sports Phys Ther. 2004;34:589–600. doi: 10.2519/jospt.2004.34.10.589. [DOI] [PubMed] [Google Scholar]
- 16.Pinar L, Enhos A, Ada S, Güngör N. Can we use nerve gliding exercises in women with carpal tunnel syndrome? Adv Ther. 2005;22:467–75. doi: 10.1007/BF02849867. [DOI] [PubMed] [Google Scholar]
- 17.Akalin E, El O, Peker O, Senocak O, Tamci S, Gülbahar S, et al. Treatment of carpal tunnel syndrome with nerve and tendon gliding exercises. Am J Phys Med Rehabil. 2002;81:108–13. doi: 10.1097/00002060-200202000-00006. [DOI] [PubMed] [Google Scholar]
- 18.McArdle WD, Katch FL, Katch VL. Exercise physciology: From par to present. In: Lupash E, editor. Essentials of Exercise Physiology. 1st ed. Philadelphia: Lippincott Williams and Wilkins; 2006. pp. 3–37. [Google Scholar]
- 19.Legg JP. The Effect of Powerball on Grip Strenght. Johannesburg University, Master's Thesis. 2008:40–7. [Google Scholar]
- 20.Randolph JK. A Comparison of Flexion and Extension Exercises in Workers at Risk for Developing Cumulative Trauma Disorder. University of Cincinnati; Doctoral Dissertation. 2000:63–72. [Google Scholar]
- 21.Madenci E, Altindag O, Koca I, Yilmaz M, Gur A. Reliability and efficacy of the new massage technique on the treatment in the patients with carpal tunnel syndrome. Rheumatol Int. 2012;32:3171–9. doi: 10.1007/s00296-011-2149-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Baker NA, Livengood HM. Symptom severity and conservative treatment for carpal tunnel syndrome in association with eventual carpal tunnel release. J Hand Surg Am. 2014;39:1792–8. doi: 10.1016/j.jhsa.2014.04.034. [DOI] [PubMed] [Google Scholar]
- 23.Jablecki CK, Andary MT, Floeter MK, Miller RG, Quartly CA, Vennix MJ, et al. Practice parameter: Electrodiagnostic studies in carpal tunnel syndrome. Report of the American Association of Electrodiagnostic Medicine, American Academy of Neurology, and the American Academy of Physical Medicine and Rehabilitation. Neurology. 2002;58:1589–92. doi: 10.1212/wnl.58.11.1589. [DOI] [PubMed] [Google Scholar]
- 24.Field T, Diego M, Cullen C, Hartshorn K, Gruskin A, Hernandez-Reif M, et al. Carpal tunnel syndrome symptoms are lessened following massage therapy. J Bodyw Mov Ther. 2004;8:9–14. [Google Scholar]
- 25.Keskin D, Uçan H, Akbulut L, Tanyolaç Ö, Aktekin C, Yaǧcı İ, et al. Effectiveness of Nerve and Tendon Gliding Exercises Following Open Carpal Tunnel Release. Türk Fiz Tıp Rehab Derg. 2008;11:15–20. [Google Scholar]