

Abstract
Background:
Though Sushruta Samhita is considered as the chief surgical treatise, Maharshi Sushruta has also emphasized on the preventive and curative aspects of diet. Dwadasha Ashana Pravichara is one of the unique concepts of Sushruta Samhita which can be considered as the root of diet therapy. In Dwadasha Ashana Pravichara, diet pattern is described for both healthy and diseased people.
Aim:
This study aimed to assess the effect of Ekakala Bhojana in Agnimandya patients.
Materials and Methods:
Patients fulfilling the criteria of selection were selected for the present study and were divided into two groups using simple random sampling method. Patients were treated for 10 days. The patients in Group A were treated with Trikatu tablet and those in Group B were given Ekakala Bhojana and placebo tablet. Effect of therapy was assessed on the basis of Abhyavaharana and Jarana Shakti.
Results:
Group B (Ekakala Bhojana) shows better results than Group A in the parameters of Abhyavaharana and Jarana Shakti except in Udgarashuddhi. Group B (65.19%) shows better result in Ahara shakti than that of Group A (55.76%).
Conclusion:
Agnimadya may be treated at primary level without the use of any medicine and only by reducing frequency of meal to Ekakala Bhojana.
Keywords: Agnimandya, Dwadasha Ashana Pravichara, Ekakala Bhojana
Introduction
Sushruta Samhita has described Dwadasha Ashana Pravichara in Swasthavritta Adhyaya of Uttaratantra, which is the major contribution in the field of dietetics.[1] There are 12 different kinds of dietary patterns which are helpful in different disease conditions and in healthy state too. Ekakala Bhojana is one among them, which means meal once in a day.[2] Acharya had suggested this dietetic regimen in persons having weak Agni (digestive fire).
According to ayurvedic philosophy, Agni is said to be responsible for Bala (strength), Varna (complexion), and Sukhayu (healthy life). All these depend on Agni and by properly maintaining Agni, one can get long and healthy life.[3] Mandagni is considered as root cause for most of the diseases.[4] Loss of function or malfunctioning can be considered as Agnimandya. Weakened Agni cannot make enough nutritive Rasa Dhatu which provides nutrition for subsequent Dhatu and the person gets easily diseased. Agnimandya may occur as a symptom or a disease itself and may provide background for further disease progression. If Agni is in normal physiology, the body is maintained in homeostasis and if the condition of the Agni is abnormal, the person may have to face pathological or diseased condition. Hence, efforts are to be taken to maintain the normal condition of Agni in human body.
Many diets, dietetic regimens and simple medicines are found which helps in maintaining the normal state of Agni with minimum efforts. Trikatu, a group of three drugs, i.e., Shunthi (Zingiber officinale Rosc.), Maricha (Piper nigrum Linn.) and Pippali (Piper longum Linn.), is one among the mostly used medicines for Deepana purpose.[5] Hence, Trikatu which is the best Deepana drug was used as standard group in the present study. Till date, no studies have been carried out to evaluate the effect of Ekakala Bhojana in Agnimandya conditions. Keeping these facts in mind, the present study was selected to evaluate the effect of dietetic regimen in patients of Agnimandya.
Materials and Methods
Source of data
Individuals attending the outpatient department and inpatient department (IPD) of the Department of Basic Principles, fulfilling the criteria of selection, were selected for the present study. A special proforma was prepared as per Ayurvedic guidelines to assess the effect of therapy.
Inclusion criteria
Patients suffering from classical signs and symptoms of Agnimandya
Patients having age between 25 and 50 years
Chronicity not more than 1 month.
Exclusion criteria
Patients having age <25 years and >50 years
Patients suffering from any major systemic diseases such as diabetes, heart disease and hypertension
Pregnant women
Conditions where Trikatu or Ekakala bhojana is contraindicated.
Investigations
To rule out any other existing pathology, hematological investigation (routine), liver function test and fasting blood sugar, postprandial blood sugar and urine (routine and microscopic) examination were carried out.
This project has been approved by Institutional Ethics Committee vide its letter No. PGT/7-A/2012-2013/1964, dated: 21/09/2012. This trial was also registered in Clinical Trial Registry of India (CTRI), Reg. no. CTRI/2013/10/004059 (trial registered retrospectively on 14/10/2013).
Drug and posology
The patients fulfilling the criteria were divided into two groups.
The patients in Group A were treated with Trikatu tablet 500 mg 2 tablets with lukewarm water at Pragbhakta Kala (before meal) for 10 days.
Group B patients were treated with Ekakala Bhojana and placebo tablet 500 mg 2 tablets with lukewarm water at Pragbhakta Kala (before meal) for 10 days. Patients were advised to take diet only one time per day, preferably only lunch. Patients were instructed not to take any food or drink (except water/tea/coffee) other than lunch. A majority of patients were admitted in the IPD of institutional hospital and light (midday) diet was provided (milk was restricted).
An assessment was made on Abhyavaharana Shakti (food intake capacity) and Jarana Shakti (digestion capacity) before and after treatment. The scoring was given to each criterion ranging from 0 to 3. The following criteria were made to assess the effect of therapy.
Statistical analysis
The obtained data, on the basis of the observation, were subjected to statistical analysis in terms of mean, standard deviation, and standard error. The Student's t-test conceded at a level of P > 0.05 (insignificant), P < 0.05 and P < 0.01 (significant), and P < 0.001 (highly significant) for the final results.
Results and Observations
In the present study consisting of fourty patients, maximum patients, i.e., 40% were in 31–40 years age group while 30% of patients were from both 25–30 and 41–50 years age group. Most of the patients (i.e. 52.5%) were males and 30% of patients were having self-business. Out of 47.5% female patients, 40% were housewives. Most of the patients were having vegetarian diet (80%) and maximum (92.5%) patients were Hindu by caste.
The symptoms of Agnimandya observed in more than 50% of patients were Udaragaurava 95% (heaviness in abdomen), Kshudhamandya 60% (lack of appetite), and Shirogaurava 52.5% (heaviness in head), while 47.5% patients had Udarashoola (abdominal pain), 40% had Gatrasadana (malaise) and 37.5% patients had both Shirahshoola (headache) and Udgarabahulya (excessive eructation).
In all parameters of Abhyavaharana Shakti (quantity of food and quality and frequency of meal), Group B had better result than Group A. Statistically highly significant result was found in Group B in all parameters of Abhyavaharana Shakti, while in Group A, statistically insignificant result was found in frequency [Tables 1–3]. Overall improvement in Abhyavaharana Shakti in Group A was 46.81% and in Group B it was 63.73%, which is statistically highly significant [Table 4].
Table 1.
Effect of therapy on Abhyavaharana Shakti in Group A
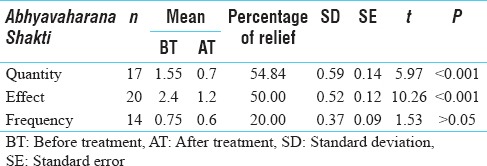
Table 3.
Comparative effect of therapy on Abhyavaharana Shakti
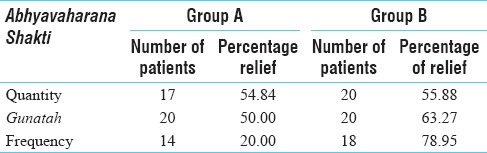
Table 4.
Total effect of therapy on Abhyavaharana Shakti of forty patients
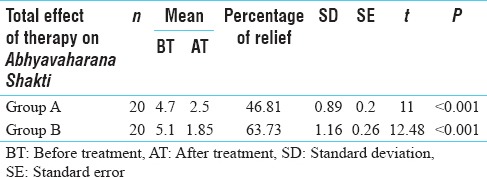
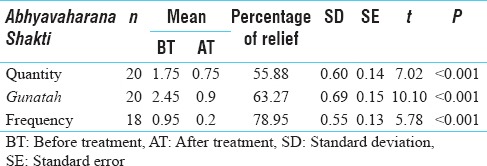
Table 2.
Effect of therapy on Abhyavaharana Shakti in Group B
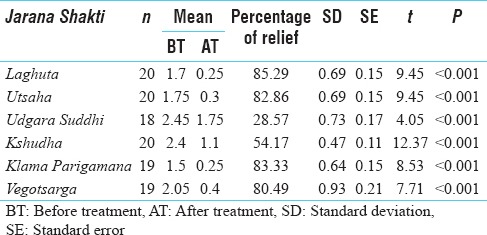
In all parameters of Jarana Shakti (Laghuta, Utsaha, Udgara Shuddhi, Kshudha, Klama Parigamanad and Vegotsarga), both the groups had highly significant result, but percentage wise, Group B had better result except in Udgarashuddhi [Tables 5–7]. Overall, improvement in Jarana Shakti was 59.32% in Group A and 65.82% in Group B. Statistically highly significant result was found in both the groups [Table 8].
Table 5.
Effect of therapy on Jarana Shakti in Group A
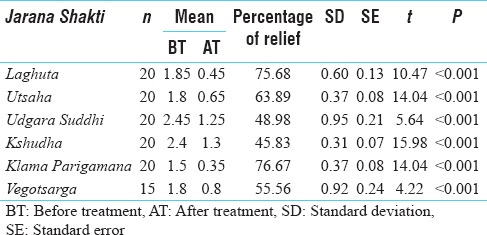
Table 7.
Comparative effect of therapy on Jarana Shakti
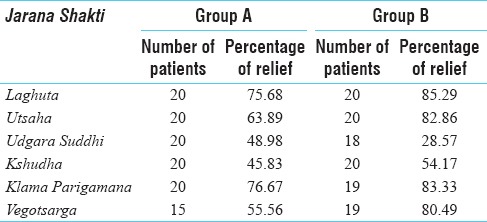
Table 8.
Total effect of therapy on Jarana Shakti of forty patients

Table 6.
Effect of therapy on Jarana Shakti in Group B
The total effect of therapy in Ahara Shakti shows that both the groups have highly significant result. Better improvement (65.19%) was found in Group B than Group A (55.76%) [Table 9].
Table 9.
Overall effect of therapy on forty patients

Complete remission was found in none of the patients in both the groups. Marked improvement was found in 20% of patients in Group B and 10% of patients in Group A. Moderate improvement was found in 75% of patients in Group B and 60% of patients in Group A. Mild improvement was found in 30% of patients in Group A and 5% of patients in Group B [Table 10].
Table 10.
Total effect of therapy

Discussion
As per the study, 40% of the patients of Agnimandya were between 31 and 40 years of age. This is the age group of Pitta predominance. Moreover, the other causative factors of Agnimandya are also found commonly during this age group such as stress regarding job security, financial constraints, Viruddhahara and family problem so that they might be not following the proper diet regulations. Viruddhahara, Ratrijagarana and other irregularities are also common in this age group. Thus, the population of this age generally does not follow the correct dietetic and behavioral regimens which eventually impair the status of their Agni. Persons having self-business (30%) may be prone to the disease because of their habits of Akala Bhojana (meal at improper time) and Adhyashana (intake of food before digestion of prior meal), street food, irregularity in diet, hurriedness in taking meal, lack of exercise, stress, tension, etc., Housewives (40%) are performing the duties due to their responsibility toward family and thus they are careless about their own health status. They are irregular in their diet and are more prone to emotional factors which are the etiological factors for Agnimandya.
It was reported that 55% of the total patients were taking Madhura Rasa, predominantly Ahara. Madhura Rasa causes Agnidaurbalya (weakness of digestive power) and Anannabhilasha (aversion to food).[6] Nearly 47.5% of the patients were taking Ushna-Tikshna Pradhana Ahara, 45% were taking Snigdha Pradhana and 40% were taking Guru Pradhana Ahara. Atiushna-Tikshna Ahara causes Drava Gunayukta Pitta Prakopa and Atisnigdha and Atiguru Ahara takes long time to digest and increases Kapha which also causes Agnimandya. Maximum, i.e., 82.5% of patients were having the habit of Amatrashana (improper quantity of food). The quantity of the food determines the stimulation of Agni.[7] It was revealed that 82.5%, 75% and 45% of the patients were having the habit of Adhayshana, Vishamashana, and Viruddhahara respectively. These dietary patterns are responsible for many diseases.[8] Nearly 55% of patients had the habit of more water intake. More water intake is again a causative factor for Agnimandya.[9] Around 77.5%, 72.5%, and 62.5% of patients had the habit of water intake after meal, at sleeping time and in the morning respectively and 45% of patients had the habit of excessive sleep. Almost 65% and 62.5% of patients had the habit of Ratrijagarana (night awakening) and Diwasvapna (day sleep) respectively. It shows that Swapnaviparyaya is one of the important causes found for Agnimandya in the study as elaborated in classics.[9] Nearly 15% of patients were found with Ati Mutrapravritti (polyuria) due to Ama formation which is sequel of Agnimandya. It was found that 62.5% of patients had unsatisfactory Mala Pravritti, while 50% and 40% patients had Durgandhita and Pichhila Mala Pravritti respectively, which suggests that food is incompletely digested by weakened Agni.
Effect of therapy on Abhyavaharana Shakti
In Group A, after administration of Trikatu, the quantity of food consumption was increased by 54.84%, symptoms after consumption of Guru and Snigdha Ahara were decreased by 50% and frequency of food intake was increased by 20%. In quantity and appearance of symptoms after consumption of Guru and Snigdha Ahara, result was highly significant. In frequency, result was insignificant. Overall, improvement in Abhyavaharana Shakti in Group A was 46.81% which is highly significant. As Agni is stimulated by Deepana Karma of Trikatu, frequency and quantity were increased and it is able to bear the Apachara Sevana.
In Group B, Ekakala Bhojana with placebo, the quantity of food consumption was increased by 55.88%, symptoms after consumption of Guru and Snigdha Ahara were decreased by 63.27% while the frequency of food intake was increased by 78.95%. Here, improvement in frequency of Abhyavaharana Shakti is in sense of intake of meal at appropriate time. All the parameters of Abhyavahaarana Shakti in Group B showed highly statistically significant result. Overall, improvement in Abhyavahaarana Shakti in Group B was 63.73% which is statistically highly significant. In Ekakala Bhojana, less quantity of food and reduced frequency of meal result in the proper digestion of meal. Hence, the power of Agni is increased and eventually quantity and frequency were increased. As Agni becomes powerful, it can able to tolerate Apachara Sevana.
Effect of therapy on Jarana Shakti
Laghuta (lightness) was increased by 85.29% in Group B and 75.68% in Group A. Statistically both groups showed highly significant result. As less amount of Laghu Ahara was given in Ekakala Bhojana, it was easily digested and symptoms of Atimatrashana were relieved.
Utsaha (energeticfeel with enthusiasm) was increased by 82.86% in Group B while in Group A, Utsaha was increased by 63.89%. Statistically both groups showed highly significant result. As less amount of food was taken in Ekakala Bhojana, it was easily digested and patients had no symptoms such as Alasya.
Udgarashuddhi (clear eructation) was increased by 48.98% in Group A and 28.57% in Group B. Statistically both groups showed highly significant result. It may be due to Katu Rasa of Trikatu and Pachana of Ama. Udgarshuddhi indicates complete digestion of Ama. In Group B, it may need prolonged treatment in chronic cases.
Kshudha was increased by 54.17% in Group B and 45.83% in Group A. Highly significant result was found in both the groups. It may be due to Deepana Karma of Trikatu in Group A. In Group B, it was increased due to Laghu Ahara which is easy to digest and Agnisandhukshanakara. Decreased frequency also gives time for proper digestion of food by Agni. The best way to judge that Agni is back in action is one feels hungry again at appropriate time.
Klama Parigamana was increased by 83.33% in Group B and 76.67% in Group A. Statistically it was found highly significant in both groups. It may be due to Deepana Karma of Trikatu in Group A and reduced frequency and easy digestion of less amount of food taken in Group B.
In Vegotsarga, better improvement was found in Group B (80.49%) and the result was found in the same symptom of Group A (55.56%). Statistically highly significant result was found in both groups. It may be due to Agnideepana and Vatanulomana effect of Trikatu and Ekakala Bhojana.
Probable mode of action
Trikatu is having Katu Rasa, Katu Vipaka, and Ushna Veerya along with Deepana Karma. It alleviates Vata-Kapha Dosha. Kapha is the main Dosha in Agnimandya and it is pacified by Trikatu. Katu Rasa also acts as a Deepana drug and causes Pachana by Ushna Veerya.
Ekakala Bhojana works as a medicine for Agnimandya by modification in regular diet in its frequency, quantity and quality. As Mandagni is unable to digest even small quantity of food, it needs much time for digestion. By giving Ekakala Bhojana, enough time is given to the Agni for complete digestion. Time is one of the important factors for Ahara Parinamakara Bhava. Though all the Aharaparinamakara Bhava works properly, if enough time is not given to Agni, food cannot be digested properly and produces undigested or intermediate products called as Ama. The rest is given to the Agni by skipping one-time meal and thus Ama is being digested in the absence of food by Agni. As Ama is digested, Agni becomes strong and stable that can digest food taken in regular amount. In addition to that, in Ekakala bhojana, amount is also reduced which Agni can digest easily. Less amount of food takes less time for digestion by Agni. Laghu Ahara was given in this group qualitatively. Agni is stimulated by Laghu Ahara by its Agnisandhukshanakara Swabhava as Laghu Ahara takes less time to get digested.
Conclusion
Maharshi Sushruta has described a key of dietetics under the heading of “Dwadasha Ashana Pravichara.” Agnimadya may be treated at primary level without use of any medicine and only by reducing the frequency of meal. By prescribing one-time meal, organs of digestive system get some rest and they can digest one-time light meal. Group B (Ekakala Bhojana) shows better results than Group A in the parameters of Abhyavaharana and Jarana Shakti except in Udgarashuddhi. Group B shows better result in Ahara shakti than Group A.
Financial support and sponsorship
This study was financially supported by IPGT and RA, Gujarat Ayurved University, Jamnagar, Gujarat, India.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Acharya YT, editor. Sushruta Samhita of Sushruta, Uttartantra. Ch. 64, Ver. 56. Varanasi: Chaukhambha Surabharati Prakashan; 2014. p. 812. [Google Scholar]
- 2.Acharya YT, editor. Sushruta Samhita of Sushruta, Uttartantra. Ch. 64, Ver. 62. Varanasi: Chaukhambha Surabharati Prakashan; 2014. p. 812. [Google Scholar]
- 3.Acharya YT, editor. Charaka Samhita of Agnivesha, Chikitsa Sthana. Reprint Edition. Ch. 15, Ver. 3. Varanasi: Chaukhambha Prakashana; 2009. p. 512. [Google Scholar]
- 4.Harishastri P, editor. Ashtanga Hridaya of Vagbhata, Nidana Sthana. Reprint. 9th Edition. Varanasi: Chaukhamba Orientalia; 2005. p. 513. Ch. 12, Ver. 1. [Google Scholar]
- 5.Acharya YT, editor. Varanasi: Chaukhambha Surabharati Prakashan; 2014. Sushruta Samhita of Sushruta, Sutra Sthana. Ch. 38, Ver. 58-59; p. 168. [Google Scholar]
- 6.Acharya YT, editor. Varanasi: Chaukhambha Prakashana; 2009. Charaka Samhita of Agnivesha, Sutra Sthana. Reprint Edition. Ch. 26, Ver. 43; p. 144. [Google Scholar]
- 7.Acharya YT, editor. Varanasi: Chaukhambha Prakashana; 2009. Charaka Samhita of Agnivesha, Chikitsa Sthana. Reprint Edition. Ch. 15, Ver. 211 ; p. 524. [Google Scholar]
- 8.Acharya YT, editor. Varanasi: Chaukhambha Prakashana; 2009. Charaka Samhita of Agnivesha, Chikitsa Sthana. Reprint Edition. Ch. 15, Ver. 237; p. 525. [Google Scholar]
- 9.Acharya YT, editor. Varanasi: Chaukhambha Orientalia; 2009. Sushruta Samhita of Sushruta, Sutra Sthana. Reprint Edition. Ch. 46, Ver. 500; p. 250. [Google Scholar]