

Abstract
Purpose
To produce a physician and scientific workforce capable of delivering high quality, culturally competent health care and research, academic medical centers must assess their capacity for diversity and inclusion and respond to identified opportunities. Thus, the Diversity Engagement Survey (DES) is presented as a diagnostic and benchmarking tool.
Method
The 22-item DES connects workforce engagement theory with inclusion and diversity constructs. Face and content validity were established based on decades of previous work to promote institutional diversity. The survey was pilot tested at a single academic medical center and subsequently administered at 13 additional academic medical centers. Cronbach alphas assessed internal consistency and Confirmatory Factor Analysis (CFA) established construct validity. Criterion validity was assessed by observed separation in scores for groups traditionally recognized to have less workforce engagement.
Results
The sample consisted of 13,694 individuals at 14 medical schools from across the U.S. who responded to the survey administered between 2011– 2012. The Cronbach alphas for inclusion and engagement factors (range: 0.68 to 0.85), CFA fit indices, and item correlations with latent constructs, indicated an acceptable model fit and that questions measured the intended concepts. DES scores clearly distinguished higher and lower performing institutions. The DES detected important disparities for black, women, and those who did not have heterosexual orientation.
Conclusions
This study demonstrated that the DES is a reliable and valid instrument for internal assessment and evaluation or external benchmarking of institutional progress in building inclusion and engagement.
Persistent health disparities, changing population demographics, and more insured patients under the Affordable Care Act, make graduating a physician and scientific workforce prepared to provide high quality, culturally competent health care more challenging for medical schools.1 Therefore, it is imperative for institutions to assess their organizational capacity for diversity and inclusion and respond effectively to insights gained.2 Scholars and practitioners have made strides in creating metrics related to diversity and inclusion interventions such as pipeline programs, internships, mentoring programs, equal opportunity plans, diversity councils, and affinity networks. Institutions have administered climate and culture surveys, which have been used to identify differences in the workplace perceptions between various demographic groups within the institution. However, beyond the compositional diversity and workforce profiles focused on protected legal categories such as race/ethnicity, gender and disability, the question still remains—How do we actually measure the capacity to fully include and engage all members of the institution?
The Diversity Engagement Survey (DES) was created by the authors to measure how well academic medical centers are responding to the diversity of its community. As a measure of the academic environment through the lens of diversity and inclusion, the DES provides data on an institution’s level of active engagement by its members, its inclusive characteristics, and the degree to which diverse groups experience inclusion.
This article discusses the development and psychometric properties of the DES, which we propose as a tool for diagnosis, for guiding institutional improvement, and for benchmarking of academic medical centers.
Method
The development of the DES
The factors that undergird the DES emerged from years of study of the diversity, inclusion and engagement literature and applied diversity management. Previous iterations of the instrument were used with 12 organizations (six corporations, four hospital systems, one government agency and one social service organization). These previous iterations were very useful in evaluating perspectives about diversity among individuals at participating institutions. However, these instruments were not as effective in providing diagnostic data and strategic direction for future interventions. To support such an objective, we recognized the need to focus on how the cultural conditions of an institution are influenced by the interplay of engagement and inclusion.
Conceptual underpinnings
Unlike culture or climate or general purpose engagement surveys, which are widely used in academic medical settings for assessing individual perceptions of her or his own psychosocial experiences within an institution, the DES reveals the aspects of culture and social dynamics related to inclusion and engagement that have been most strongly related to productivity and employee retention.3,4 Within the DES framework, diversity is conceptualized as embracing all aspects of human differences and is viewed as a core value that is embodied by inclusiveness, mutual respect and awareness of multiple perspectives.5 Inclusion is conceptualized as a set of social processes that influence an individual’s access to information, sense of belonging and job security, as well as social support received from others.6,7 Without an institutional culture that supports the inclusion of differences in perspectives, life experience and knowledge that individuals bring to the institution, the full potential of diversity cannot be realized.2
Engaging every member of the institution is the foundation upon which a truly inclusive academic medical center is built. Successful employee engagement is derived from meeting the basic intellectual and emotional needs of workers.8-12 Engagement results from conditions that foster a shared sense of vision/purpose of the organization as well as camaraderie, and appreciation of employees’ contribution to the institution. Vision and purpose provides employees with a compelling reason to contribute to the organization’s mission. Camaraderie gives the employee a sense of belonging and provides them with an opportunity to reach out personally and connect to those around them. Appreciation recognizes contributions and values what each individual brings to the organization as a person. These are conditions for building inclusion within a diverse workforce as well as encouraging people to bring their full creative and innovative talents into the workplace.10,13, 14
The DES
The authors delineated those behaviors that would exemplify an inclusive academic medical center by grounding the work of the revised survey in diversity, inclusion and engagement literature and applied diversity management. The behaviors that described an inclusive environment and employee experiences that resulted in engagement coalesced into eight inclusion factors that formed the frame work for developing the DES:
Common Purpose: individual experiences a connection to the mission, vision and values of the organization;
Trust: individual has confidence that the policies, practices, and procedures of the organization will allow them to bring their best and full self to work;
Appreciation of Individual Attributes: individual is valued and can successfully navigate the organizational structure in their expressed group identity;
Sense of Belonging: individual experiences their social group identity being connected and accepted in the organization;
Access to Opportunity: individual is able to find and utilize support for their professional development and advancement;
Equitable Reward and Recognition: individual perceives the organization as having equitable compensation practices and non-financial incentives;
Cultural Competence: individual believes the institution has the capacity to make creative use of its diverse workforce in a way that meets business goals and enhances performance; and,
Respect: individual experiences a culture of civility and positive regard for diverse perspectives and ways of knowing.
The authors proposed survey items derived from a review of literature and their own experience in the field relative to the framework factors. The final DES consisted of twenty-two items chosen to reflect the eight domains of inclusion and engagement. Each item was created to capture the essence of the relationship between the institution and the employee rather than capturing the employee’s perception about how they and other members who share their group identity experience institutional practices. All items were written in first person and phrased positively. One final open-ended question (“If you wish, please provide additional comments on the diversity and inclusion efforts”) was offered to provide the respondents the opportunity to express any concerns, insights, or experiences related to their institutional context.
All responses on the 22-item instrument were scored on a 5-point Likert scale (5=Strongly agree to 1=Strongly disagree). Respondents were also given the opportunity to indicate if they were unable to evaluate any particular item. Because of the small number of items, any significant concerns about participant acquiescence bias were dismissed.
In addition, the DES collects characteristics of the respondents and their environment that may be useful in interpreting findings about diversity and inclusion:
Internal dimensions: race, ethnicity, age, gender, sexual orientation, physical ability;
External dimensions: religion, work experience, languages spoken;
Organizational dimensions: management status, functional level/classification, division/department, unit/group, work location, seniority.
Pilot testing and survey implementation
Face and content validity of the initial survey was assessed and improved through a review panel consisting of representative respondents at the home medical institution of one of the authors. The survey was piloted at an academic medical center in March 2011. After the pilot, an invitation to participate in the survey benchmarking process was sent through AAMC and the Group on Diversity and Inclusion (GDI) to all member institutions. The survey was subsequently administered to 13 additional academic medical centers. The participating academic medical centers were offered the instrument at no cost to their institution and were provided access to their survey results in aggregate form with the understanding that their results would be used to validate the instrument and create benchmark data. Data were collected and compiled by an external provider of survey management services to researchers.
The Institutional Review Board of the University of Massachusetts Medical School provided an exemption waiver for the study in February 2011. The survey was implemented in a voluntary, anonymous manner to all employees including faculty, staff, and administrators as well as students. Completion of the survey constituted consent. No incentives were provided for participation.
Statistical analysis
All quantitative analyses were performed using SAS 9.3 (SAS Institute Inc., Cary, NC) and Stata 12 (StataCorp LP, College Station Texas). Demographic characteristics of the participants were summarized. Based on the development process described above, face and content validity of the instrument were established prior to pilot testing of the instrument.
Internal consistency
Internal consistency reliability, a commonly used tool in psychometric evaluation, is an indicator of how well different items measure the same concept.15 We measured the internal consistency of the eight inclusion and engagement factors by calculating Cronbach alphas. Traditionally, Cronbach alpha values of 0.70 and above are deemed acceptable.
Construct validity
Construct validity is a measure of how meaningful an instrument is in actual use.15 More specifically, construct validity is conveyed when a measure captures what it is intended to represent. In other words, with high construct validity, the measure will behave according to a specified conceptual model. Based on the expected mapping of items to inclusion and engagement factors, we performed confirmatory factor analysis (CFA) via structural equation modeling to investigate construct validity, and examine the dimensionality of the instrument. We selected two representative fit indices, comparative fit index (CFI)16 and the standardized root mean square residual (SRMR)17, to assess model fit. CFI is an index that ranges in value from 0 to 1, with values greater than 0.90 considered an indicator of a good fitting model.17 The SRMR is an absolute measure of fit and is defined as the standardized difference between the observed and predicted correlation; models with a SRMR value less than or equal to 0.08 are considered good.17
We also examined the ability of our instrument to distinguish between high and lower performing schools and between the experiences of demographic groups. We first calculated a mean for each factor by institution and also a separate grand mean DES score for each institution. Next, we created a graphic display for each factor that arrayed mean institutional scores in ascending order. This display provided a visual method to examine the ability of the DES to distinguish between high and low performing institutions. Next, we conducted a cluster analysis based on the grand mean DES score for each institution to determine whether patterns observed graphically resulted in different statistical clusters of schools. Cluster analysis is a set of techniques designed to place objects into groups, suggested by the data, such that an object in a given cluster is more like others in that same cluster than objects in another cluster.18 We examined tree plots to determine the appropriate number of clusters. Using a complete linkage approach, we determined a school’s cluster membership based on the grand mean DES.
We also sought to demonstrate the instrument’s usefulness in understanding specific disparities within a given institution. As one possible example of this type of analysis, we first calculated differences in mean question scores for blacks and whites within each institution. Next, we ranked each academic medical center separately on the black respondents’ DES scores (ordered from highest to lowest) and the observed disparity (white score – black score) (ordered from lowest to highest) and calculated a Spearman correlation for the two rankings. A separate analyses was performed for each question. This graphical and statistical analysis was repeated using the grand average of all DES questions for black and white respondents at each institution.
Criterion validity
As a final step in assessing the utility of the DES we examined criterion validity, a measure of how well a construct predicts an outcome based on information from other variables.15 Here, we examined differences in DES scores based on key respondent characteristics suggested by the literature, such as race/ethnicity, gender, and sexual orientation.
Results
Broad representation across each region of the country was obtained through the 13,694 respondents to the survey. The average response rate across the 14 institutions was 26.7% (SD=9.5) and ranged from 11% to 46% (one institution did not provide the total number of possible respondents). Approximately 66% of respondents were female, and most were white (75%). Most respondents reported heterosexual orientation (87%). Duration of employment at the respondent’s current medical school was equally distributed between those less than 5 years (50%) and those 5 years or more (50%).
Internal consistency
The DES Cronbach alpha’s for the inclusion and engagement factors ranged from 0.68 to 0.85 (Table 2). With the exception of one factor which was marginal (Common Purpose: Cronbach alpha=0.68), factors demonstrated acceptable levels of internal consistency reliability.
Table 2.
Confirmatory Factor Loadings, and Cronbach Alphas for Diversity Engagement Survey Items
| Engagement and Inclusion Factor | Item | Confirmatory Factor Loadings | Cronbach Alpha |
|---|---|---|---|
| Common Purpose | 4 | 0.57 | 0.68 |
| 17 | 0.76 | ||
| Access to Opportunity | 5 | 0.71 | 0.77 |
| 9 | 0.76 | ||
| Equitable Reward and Recognition | 10 | 0.79 | 0.77 |
| 16 | 0.74 | ||
| Cultural Competence | 7 | 0.7 | 0.81 |
| 11 | 0.76 | ||
| 15 | 0.74 | ||
| 20 | 0.64 | ||
| Trust | 1 | 0.76 | 0.85 |
| 13 | 0.81 | ||
| 19 | 0.75 | ||
| Sense of Belonging | 6 | 0.75 | 0.70 |
| 14 | 0.45 | ||
| 21 | 0.68 | ||
| Appreciation of Individual Attributes | 3 | 0.81 | 0.81 |
| 8 | 0.66 | ||
| 22 | 0.8 | ||
| Respect | 2 | 0.81 | 0.83 |
| 12 | 0.73 | ||
| 18 | 0.82 | ||
| Overall | 0.96 | ||
Construct validity
Confirmatory factor analysis resulted in a CFI of 0.917 and a SRMR of 0.038 (Figure 1). Both indices indicate an acceptable model fit and support the mapping of items to inclusion and engagement factors. An examination of item correlations with the latent constructs from CFA indicated that in general all items correlated well with the constructs they were intended to measure with only three items (Questions 4, 14 and 20) having slightly lower correlations than desired (Figure 1). CFA results also revealed satisfactory loadings for all the items (Table 2). Similar to the results found in the item correlations and latent constructs, Questions 14 and 4 had slightly lower factor loadings however, they were still within the threshold of acceptability (loading scores > 0.4).
Figure 1.
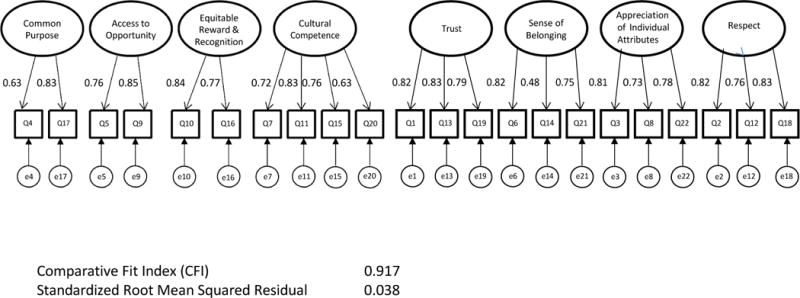
Confirmatory Factor Analysis: The Diversity Engagement Survey
All coefficients significant at p<0.001
The graphical displays of the mean factor scores clearly separated high and low performing institutions (Figure 2). The more formal cluster analysis based on the grand mean DES scores yielded three distinct clusters, which accounted for 98% of the variation in the eigenvalues. Figure 2 reveals that there is a high degree of correspondence between the formal cluster analysis based on the grand mean DES and the graphical rankings of institutional performance on each factor.
Figure 2.
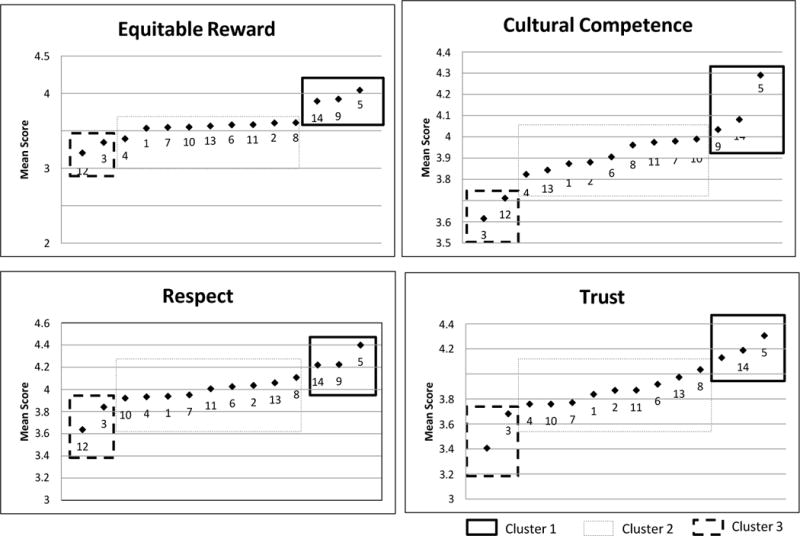
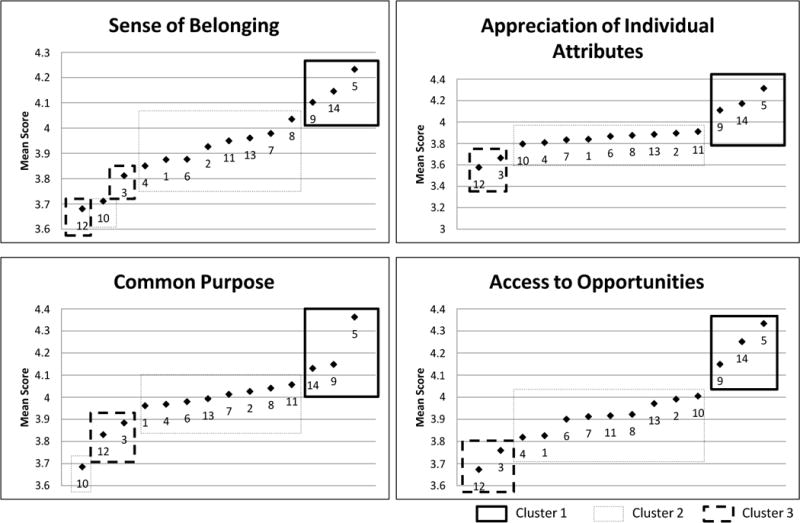
Each point represents a single institution. Cluster analysis was based on grand mean DES score for each institution.
Mean Scores and Cluster Membership of Selected DES Factors
We also found that greater disparity between black and white respondents at the institutional level was strongly correlated with lower black respondent scores. In fact, Table 4 reveals that Spearman correlations for institutional rankings based on disparities and institutional rankings based on mean black scores ranged from 0.70 to 0.95 and were statistically significant for all questions except 4 and 14. Figure 3 depicts similar findings based on the analysis for the mean of all questions. This figure also demonstrates great variability in both observed disparities and mean scores for blacks. For only two schools, disparities “favored” blacks.
Table 4.
Correlation between Institutional Ranking based on Mean African American Score and Institutional Ranking based on Difference in Mean Score for African American and White Respondents to the Diversity Engagement Survey
| Item | Spearman Correlation | 95% Confidence Interval |
|---|---|---|
| Q1 | 0.80 | (0.47, 0.93) |
| Q2 | 0.77 | (0.40, 0.92) |
| Q3 | 0.80 | (0.46, 0.93) |
| Q4 | 0.47 | (−0.08, 0.80) |
| Q5 | 0.74 | (0.34, 0.91) |
| Q6 | 0.95 | (0.85, 0.98) |
| Q7 | 0.74 | (0.35, 0.91) |
| Q8 | 0.75 | (0.36, 0.92) |
| Q9 | 0.82 | (0.52, 0.94) |
| Q10 | 0.76 | (0.39, 0.92) |
| Q11 | 0.83 | (0.54, 0.95) |
| Q12 | 0.89 | (0.68, 0.96) |
| Q13 | 0.82 | (0.50, 0.94) |
| Q14 | 0.63 | (0.15, 0.87) |
| Q15 | 0.74 | (0.34, 0.91) |
| Q16 | 0.88 | (0.64, 0.96) |
| Q17 | 0.70 | (0.26, 0.90) |
| Q18 | 0.75 | (0.37, 0.92) |
| Q19 | 0.82 | (0.50, 0.94) |
| Q20 | 0.80 | (0.47, 0.93) |
| Q21 | 0.74 | (0.35, 0.91) |
| Q22 | 0.88 | (0.66, 0.96) |
Figure 3.
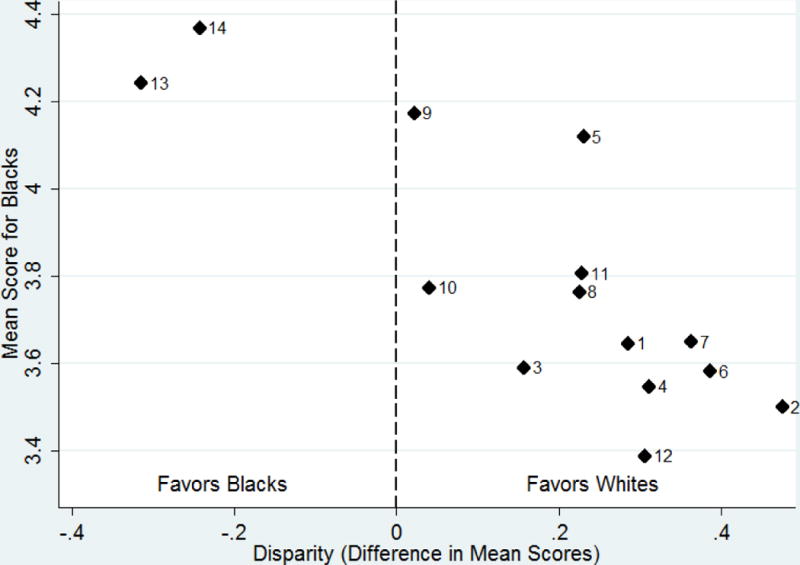
Analysis is at school level. Labels indicate specific schools. Pearson ρ = 0.80.
Relation of Black vs. White Disparity in DES Score to Mean DES Score for African Americans
Criterion validity
Analysis of the responses to the survey by demographic group revealed that blacks, and Hispanic participants had lower mean inclusion scores than whites. Women had lower scores than men (Table 3). Participants who self-identified as LGBT had lower mean inclusion scores than heterosexuals. This pattern persisted when analyses were restricted to respondents from higher performing institutions (schools found to belong to the high group by cluster analysis) (Results not shown).
Table 3.
Association of Diversity Engagement Survey Factors and Selected Respondent Characteristics
| Characteristic | Common Purpose
|
Access to Opportunity
|
||
|---|---|---|---|---|
| Mean (SD) | Significant Group Differencesa | Mean (SD) | Significant Group Differencesa | |
| Gender | ||||
| FemaleA | 3.98 (0.81) | A v. B | 3.88 (0.97) | A v. B |
| MaleB | 4.08 (0.84) | 3.97 (0.97) | ||
| Race/Ethnicity | ||||
| AsianA | 4.09 (0.79) | A v. | 4.06 (0.86) | A v. |
| Black/African AmericanB | 3.89 (0.88) | (B,C,D, E); | 3.75 (1.06) | (B,C,D,E); |
| Hispanic/LatinoC | 3.95 (0.90) | B v. E; | 3.79 (1.03) | B v. E; |
| OtherD | 3.86 (0.90) | C v. E; | 3.72 (1.14) | C v. E; |
| WhiteE | 4.03 (0.80) | D v. E | 3.93 (0.95) | D v. E |
| Sexual Orientation | ||||
| LGBTQA | 3.83 (0.92) | 3.81 (0.98) | ||
| HeterosexualB | 4.03 (0.81) | A v. B; | 3.93 (0.97) | A v. (B,C); |
| Missing/Refused to AnswerC | 3.80 (1.09) | B v. C | 3.54 (1.22) | B v. C |
|
| ||||
| Equitable Reward
|
Cultural Competency
|
|||
| Characteristic | Mean (SD) | Significant Group Differencesa | Mean (SD) | Significant Group Differencesa |
|
| ||||
| Gender | ||||
| FemaleA | 3.47 (1.05) | A v. B | (0.73) 3.86 | A v. B |
| MaleB | 3.67 (1.08) | 3.97 (0.76) | ||
| Race/Ethnicity | ||||
| AsianA | 3.79 (1.02) | A v. | 4.01 (0.75) | A v. |
| Black/African AmericanB | 3.34 (1.11) | (B,C,D,E); | 3.67 (0.83) | (B,C,D,E); |
| Hispanic/LatinoC | 3.43 (1.13) | B v. E; | 3.79 (0.85) | B v. (C,E); |
| OtherD | 3.30 (1.22) | C v. (D,E); | 3.71 (0.87) | C v. E; |
| WhiteE | 3.55 (1.04) | D v. E | 3.93 (0.71) | D v. E |
| Sexual Orientation | ||||
| LGBTQA | 3.35 (1.12) | 3.71 (0.81) | ||
| HeterosexualB | 3.56 (1.06) | A v. B; | 3.92 (0.73) | A v. B; |
| Missing/Refused to AnswerC | 3.25 (1.19) | B v. C | 3.68 (0.99) | B v. C |
|
| ||||
| Trust
|
Sense of Belonging
|
|||
| Characteristic | Mean (SD) | Significant Group Differencesa | Mean (SD) | Significant Group Differencesa |
|
| ||||
| Gender | ||||
| FemaleA | 3.77 (0.90) | A v. B | 3.88 (0.76) | A v. B |
| MaleB | 4.00 (0.88) | 3.99 (0.80) | ||
| Race/Ethnicity | ||||
| AsianA | 4.05 (0.79) | A v. | 4.00 (0.72) | A v. |
| Black/African AmericanB | 3.57 (0.95) | (B,C,D,E); | 3.77 (0.78) | (B,C,D,E); |
| Hispanic/LatinoC | 3.68 (1.00) | B v. (C,E); | 3.80 (0.83) | B v. E; |
| OtherD | 3.58 (1.07) | C v. E; | 3.73 (0.91) | C v. E; |
| WhiteE | 3.88 (0.87) | D v. E | 3.94 (0.76) | D v. E |
| Sexual Orientation | ||||
| LGBTQA | 3.60 (1.01) | 3.75 (0.84) | ||
| HeterosexualB | 3.87 (0.88) | A v. B; | 3.94 (0.77) | A v. B; |
| Missing/Refused to AnswerC | 3.65 (1.14) | B v. C | 3.72 (1.02) | B v. C |
|
| ||||
| Appreciation of Attributes
|
Respect
|
|||
| Characteristic | Mean (SD) | Significant Group Differencesa | Mean (SD) | Significant Group Differencesa |
|
| ||||
| Gender | ||||
| FemaleA | 3.83 (0.82) | A v. B | 3.93 (0.77) | A v. B |
| MaleB | 3.94 (0.87) | 4.09 (0.78) | ||
| Race/Ethnicity | ||||
| AsianA | 4.02 (0.78) | A v. | 4.12 (0.73) | A v. |
| Black/African AmericanB | 3.73 (0.87) | (B,C,D,E); | 3.75 (0.82) | (B,C,D,E); |
| Hispanic/LatinoC | 3.76 (0.92) | B v. E; | 3.88 (0.86) | B v. (C,E); |
| OtherD | 3.65 (1.00) | C v. (D,E); | 3.74 (0.95) | C v. (D,E); |
| WhiteE | 3.88 (0.82) | D v. E | 4.01 (0.74) | D v. E |
| Sexual Orientation | ||||
| LGBTQA | 3.67 (0.92) | 3.76 (0.89) | ||
| HeterosexualB | 3.89 (0.83) | A v. B; | 4.00 (0.76) | A v. B; |
| Missing/Refused to AnswerC | 3.64 (1.06) | B v. C | 3.74 (1.07) | B v. C |
Overall p-value significant at the P<0.001 level. Group difference significance estimated using least squares means and adjust for multiple testing. All listed differences are significant at least at the P<0.05 level. As an example of interpretation: for Race/Ethnicity, A v. (B, C, D, E) would indicate that people who self-identify as Asian are significantly different from those who self- identify as Black, Hispanic/Latino, Other race, or White.
Discussion
Our findings suggest that the DES produces useful, reliable, and valid measurements of key phenomena essential to the integration of diversity in academic medical centers. Additionally, the DES lends itself to both composite and subgroup analysis, each serving complementary yet distinct functions. The overall composite scores support ranking and benchmarking whereas subgroup analysis allow focused investigation about root causes that may be used in improvement plans. For example, if both the baseline and subgroup scores are equally low, changes in organization-wide policy may be needed. On the other hand, if the baseline scores are high but the subgroup scores are low, a policy targeting the subgroup would be appropriate.
Overall, the Cronbach Alpha results indicate that the DES is a reliable instrument. One possible explanation for the marginally low Cronbach Alpha of the Common Purpose factor may be violation of the essential tau equivalence assumption,19 which is suggested because the observed variances of the two questions comprising this factor are significantly different. (Data are not shown.) However, violation of this assumption usually leads to underestimation of the alpha coefficient, so it is reasonable to assume that the reported coefficient represents a lower bound for the true value. Because the entire survey has considerable face validity based on existing literature and vetting with the review panel, we have chosen to retain this factor in the survey. Nonetheless, we will continue to monitor this factor closely as the survey is rolled out to additional medical centers.
Additionally, we demonstrated both construct and criterion validity. Fit indices from the confirmatory factor analysis were acceptable indicating appropriate model fit. Consistent with prior research,20-24 we found that blacks, Hispanic, female and LGBT respondents provided less favorable responses to the survey than males, or whites regardless of gender. We also found that the DES consistently separated respondent institutions into three groupings of mean cluster scores supporting the instrument’s promise as a benchmarking tool to measure the progress of diversity interventions among academic medicine institutions.
The within-institutional analysis revealed large variation in disparities for black and white respondents, suggesting the importance of future study to determine how institutional characteristics, culture, and programming are related to observed disparities. The within- institutional analysis also suggests that when there is a disparity between blacks and whites, that difference occurs because blacks are reporting at a lower level than whites. We also demonstrated that high performing schools generally had higher scores for blacks and lower disparity between blacks and whites.
It should be noted that our sample is not necessarily representative of the entire population of academic medical centers in the United States. For example, institutions that are experiencing diversity challenges or those who have been particularly active in promoting and integrating diversity may have selected to participate. However, concern about selection bias is somewhat mitigated because a significant number of institutions clustered in the middle range of scores. Nonetheless, because of concern about selection bias, we did not examine the relation between DES scores and institutional characteristics. Such studies will be appropriate as larger, representative institutional samples become available. In addition, in-depth case studies of selected high performing and low performing institutions might yield findings to critically inform future interventions.
Conclusion
To build institutional capacity for diversity, institutions must start with an understanding of the extent to which various groups feel included and engaged.25 The DES provides a way of measuring the conditions to which the institutional culture fosters inclusion and engagement. As a diagnostic tool it allows organizations to assess the institution’s inclusion efforts and develop a strategy for achieving its diversity goals. As a benchmarking tool, the DES distinguishes institutions in their process towards inclusion. Overall it supports academic medical centers to assess and build their institutional capacity to adapt and innovate during this time of great transformation across all domains of healthcare and academic medicine.
Table 1.
Diversity Engagement Survey Items Mapped to Engagement and Inclusion Factors
| Engagement and Inclusion Factor | Item | Item Description |
|---|---|---|
| Common Purpose | 4 | I feel that my work or studies contribute to the mission of the institution. |
| 17 | I feel connected to the vision, mission and values of this institution. | |
| Access to Opportunity | 5 | This last year, I have had opportunities at work/school to develop professionally. |
| 9 | There is someone at work/school who encourages my development. | |
| Equitable Reward and Recognition | 10 | I receive recognition and praise for my good work similar to others who do good work at this institution. |
| 16 | In my institution, I am confident that my accomplishments are compensated similar to others who have achieved their goals. | |
| Cultural Competence | 7 | In this institution, I have opportunities to work successfully in settings with diverse colleagues. |
| 11 | I believe my institution manages diversity effectively. | |
| 15 | In my institution, I receive support for working with diverse groups and working in cross-cultural situations. | |
| 20 | In this institution, there are opportunities for me to engage in service and community outreach. | |
| Trust | 1 | I trust my institution to be fair to all employees and students. |
| 13 | If I raised a concern about discrimination, I am confident my institution would do what is right. | |
| 19 | I believe that in my institution harassment is not tolerated. | |
| Sense of Belonging | 6 | At work/school, my opinions matter. |
| 14 | I consider at least one of my co-workers or fellow students to be a trusted friend. | |
| 21 | I feel that I am an integral part of my department or school. | |
| Appreciation of individual Attributes | 3 | I am valued as an individual by my institution. |
| 8 | Someone at work/school seems to care about me as an individual. | |
| 22 | The culture of my institution is accepting of people with different ideas. | |
| Respect | 2 | The leadership of my institution is committed to treating people respectfully. |
| 12 | In my institution, I experience respect among individuals and groups with various cultural differences. | |
| 18 | I believe that my institution reflects a culture of civility. |
Acknowledgments
None
Funding/Support: Research in the publication was partially supported by the UMASS Center for Health Equity Intervention Research (CHEIR) (NIH Award # P60MD006912) and the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR000161. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Other disclosures: None
Ethical approval: Deemed Exempt, UMMS Institutional Review Board, February 25, 2011, Reference number 14148
Disclaimer: None
Previous presentations:
AAMC DES Webinars, March 2013 and March 2014
AAMC Roundtable on Organizational Inclusion, Washington D.C. June 2013
Annual GDI/GFA Conference, August 2012
Contributor Information
Dr. Sharina D. Person, Associate Professor, Department of Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, MA.
Dr. C. Greer Jordan, Associate Vice Chancellor, Diversity and Inclusion and Assistant Professor, Graduate School of Nursing, Psychiatry and Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, MA.
Dr. Jeroan J. Allison, Associate Vice Provost for Health Disparities Research and Vice Chair and Professor, Department of Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, MA.
Dr. Lisa M. Fink Ogawa, Clinical Assistant Professor and Director, Quality and Safety Scholarship, The University of Kansas Medical Center School of Nursing, Kansas City, KS.
Dr. Laura Castillo-Page, Senior Director, Diversity Policy and Programs and Organizational Capacity Building Portfolio, Association of American Medical Colleges, Washington DC.
Sarah Conrad, Senior Research Analyst, Association of American Medical Colleges, Washington DC.
Dr. Marc A. Nivet, Chief Diversity Officer Association of American Medical Colleges, Washington DC.
Dr. Deborah L. Plummer, Vice Chancellor, Diversity and Inclusion and Professor, Departments of Psychiatry, Quantitative Health Sciences, and Nursing, University of Massachusetts Medical School, Worcester, MA.
References
- 1.Kocher R, Emmanuel EJ, DeParle NM. The affordable care act and the future of clinical medicine: The opportunities and challenges. Ann Intern Med. 2010;135:536–539. doi: 10.7326/0003-4819-153-8-201010190-00274. [DOI] [PubMed] [Google Scholar]
- 2.Ely RJ, Thomas DA. Cultural diversity at work: The effects of diversity perspectives on work group processes and outcomes. Adm Sci Q. 2001;46:229–262. [Google Scholar]
- 3.Cooke RA, Szumal JL. Measuring normative beliefs and shared behavioral expectations in organizations: The reliability and validity of the organizational culture inventory. Psychol Rep. 1993;72:1299–1330. [Google Scholar]
- 4.Mor Barak ME, Cherin DA, Berkman S. Organizational and personal dimensions in diversity climate: Ethnic and gender differences in employee perceptions. J Appl Behav Sci. 1998;34:82–104. [Google Scholar]
- 5.AAMC Group on Diversity and Inclusion. Definitions. https://www.aamc.org/members/gdi/about/. Accessed January 2, 2014.
- 6.Hope Pelled L, Ledford GE, Mohrman SA. Demographic dissimilarity and workplace inclusion. J of Manag Studies. 1999;36(7):1013–1031. [Google Scholar]
- 7.Schein EH. Organizational Culture and Leadership. San Francisco: Jossey-Bass; 1992. [Google Scholar]
- 8.Buckingham M, Coffman C. First Break all the Rules: What the World’s Greatest Managers do Differently. New York, NY: Simon & Schuster; 1999. [Google Scholar]
- 9.Kahn WA. Physiological conditions of personal engagement and disengagement at work. Acad Manag J. 1990;33:692–724. [Google Scholar]
- 10.Colan L. Engaging the Hearts and Minds of all your Employees: How to Ignite Passionate Performance for Better Business Results. New York, NY: McGraw-Hill; 2008. [Google Scholar]
- 11.Harter JK, Schmidt FL, Keyes CL. Well-being in the workplace and its relationship to business outcomes: A review of the Gallup studies. In: Keyes LM, editor. Flourishing: Positive Psychology and the Life Well-lived. Washington, DC: American Psychological Association; 2003. [Google Scholar]
- 12.Volpone SD, Avery DR. Linkages between racioethnicity, appraisal reactions and employee engagement. J Appl Soc Psychol. 2012;42:252–270. [Google Scholar]
- 13.Davidson MN, Ferdman BM. Diversity and inclusion: What difference does it make? Ind Org Psychol. 2001;39(2):36–38. [Google Scholar]
- 14.Cox T. A Strategy for Capturing the Power of Diversity. San Francisco, CA: Jossey-Bass; 2001. Creating The Multicultural Organization. [Google Scholar]
- 15.Litwin MS. How to Assess and Interpret Survey Psychometrics. 2nd. Vol. 8. Thousand Oaks, CA: Sage Publications; 2003. The survey kit series. [Google Scholar]
- 16.Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- 17.Hu L, Bentler PM. Cutoff criteria for fit indices in covariance structure analysis: Convention criteria versus new alternatives. Struct Equ Modeling. 1999;6:1–55. [Google Scholar]
- 18.Everitt BS, Landau S, Leese M, Stahl D. Cluster Analysis. 5th. New York: Wiley & Sons; 2011. [Google Scholar]
- 19.Tavakol M, Dennick R. Making sense of Cronbach’s Alpha. Intern J of Med Educ. 2001;2:53–55. doi: 10.5116/ijme.4dfb.8dfd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Assessing the academic work environment for science and engineering and social science faculty at the University of Michigan in 2006: Gender, race, and discipline in department and university related climate factors. UM ADVANCE Program. 2008 Website. http://www.advance.rackham.umich.edu/ADV-FacultyClimate-Rpt2-final.pdf. Accessed January 2, 2014.
- 21.Bilimoria D, Liang X. Routledge Studies in Management, Organizations and Society. Florence, KY: Routledge; 2012. Gender Equity in Science and Engineering: Advancing Change in Higher Education. [Google Scholar]
- 22.Bilimoria D, Stewart AJ. “Don’t ask, don’t tell”: The academic climate for lesbian, gay, bisexual, and transgender faculty in science and engineering. NWSA J. 2009;21(2):85–103. [Google Scholar]
- 23.Liang X, Bilimoria D. The representation and experience of women faculty in STEM fields. In: Burke RJ, Mattis MC, editors. Women and Minorities in Science, Technology, Engineering, and Mathematics: Upping the Numbers. 2007. p. 317. [Google Scholar]
- 24.Nivet MA. Commentary: Diversity 3.0: A necessary systems upgrade. Acad Med. 2011;86:1487–1489. doi: 10.1097/ACM.0b013e3182351f79. [DOI] [PubMed] [Google Scholar]