

Abstract
Importance
Most studies on opsoclonus-myoclonus syndrome (OMS) in adults are based on small case series before the era of neuronal cell surface antibody discovery.
Objective
To report the clinical and immunological features of idiopathic OMS (l-OMS) and paraneoplastic OMS (P-OMS), the occurrence of antibodies to cell surface antigens, and the discovery of a novel cell surface epitope.
Design Setting and Participants
Retrospective cohort study and laboratory investigations of 114 adult patients with OMS at a center for autoimmune neurological disorders done between January 2013 and September 2015.
Main Outcomes and Measures
Review of clinical records. Immunohistochemistry on rat brain and cultured neurons as well as cell-based assays were used to identify known autoantibodies. Immunoprecipitation and mass spectrometry were used to characterize novel antigens.
Results
Of the 114 patients (62 [54%] female; median age, 45 years; interquartile range, 32-60 years), 45 (39%) had P-OMS and 69 (61%) had l-OMS. In patients with P-OMS, the associated tumors included lung cancer (n = 19), breast cancer (n = 10), other cancers (n = 5), and ovarian teratoma (n = 8); 3 additional patients without detectable cancer were considered to have P-OMS because they had positive results for onconeuronal antibodies. Patients with l-OMS, compared with those who had P-OMS, were younger (median age, 38 [interquartile range, 31-50] vs 54 [interquartile range, 45-65] years; P < .001), presented more often with prodromal symptoms or active infection (33% vs 13%; P = .02), less frequently had encephalopathy (10% vs 29%; P = .01), and had better outcome (defined by a modified Rankin Scale score ≤2 at last visit; 84% vs 39%; P < .001) with fewer relapses (7% vs 24%; P = .04). Onconeuronal antibodies occurred in 13 patients (11%), mostly Ri/ANNA2 antibodies, which were detected in 7 of 10 patients (70%) with breast cancer. Neuronal surface antibodies were identified in 12 patients (11%), mainly glycine receptor antibodies (9 cases), which predominated in P-OMS with lung cancer (21% vs 5% in patients with OMS without lung cancer; P = .02); however, a similar frequency of glycine receptor antibodies was found in patients with lung cancer without OMS (13 of 65 patients [20%]). A novel cell surface epitope, human natural killer 1 (HNK-1), was the target of the antibodies in 3 patients with lung cancer and P-OMS.
Conclusions and Relevance
Patients with l-OMS responded better to treatment and had fewer relapses than those with P-OMS. Older age and encephalopathy, significantly associated with P-OMS, are clinical clues suggesting an underlying tumor. Glycine receptor antibodies occur frequently in P-OMS with lung cancer, but the sensitivity and specificity are low. The HNK-1 epitope is a novel epitope in a subset of patients with P-OMS and lung cancer.
Opsoclonus-myoclonus syndrome (OMS) is characterized by the combination of opsoclonus and arrhythmic action myoclonus that predominantly involves trunk and limbs usually accompanied by axial ataxia and dysarthria.1 The 2 most common causes of OMS are paraneoplastic and idiopathic,2,3 but the clinical features, types of tumors, and other comorbidities are different in children and adults. The current study examines these in adults.4
Several clinical and laboratory findings suggest that paraneoplastic OMS (P-OMS) and idiopathic OMS (I-OMS) are immune mediated.5 The symptom presentation is usually acute or subacute, the presence of pleocytosis is common, and patients often respond to immunotherapy. Autopsy studies may show mild perivascular lymphocytic cuffs but rarely demonstrate neuronal degeneration or extensive T-cell infiltrates, suggesting that the disorder could be mediated by antibodies rather than cytotoxic T-cell mechanisms.6,7
To our knowledge, with the exception of Ri/ANNA2 antibodies in patients with OMS and breast cancer, the search for other antibodies specific for OMS has not revealed a common biomarker of the disease.8,9 Most of these studies were done before the discovery of antibodies to neuronal cell surface proteins that currently characterize many types of autoimmune encephalitis.10 Therefore, a systematic analysis of these antibodies in adult OMS has not been done. Recently, antibodies to dendritic surface antigens were detected in 10% of patients with adult and pediatric OMS but the target antigen was not identified.11 In the current study, we examine a large series of adult patients with P-OMS or I-OMS to define clinical and immunological subtypes of OMS, including possible associations with neuronal cell surface antibodies, and to describe a novel paraneoplastic epitope.
Methods
Patients
One hundred fourteen patients with OMS whose serum and cerebrospinal fluid (CSF) samples were sent for antibody testing to the laboratories of Hospital Clínic, Barcelona, Spain, or the University of Pennsylvania, Philadelphia, between January 1995 and December 2014 were included in the study, which was conducted between January 2013 and September 2015. Samples from the University of Pennsylvania used in a recent study were not included.11 Inclusion criteria were the following: (1) aged 18 years or older; (2) adequate clinical information; (3) paraneoplastic, idiopathic, or infectious causes of OMS, and exclusion of structural, toxic, and metabolic causes; and (4) serum or CSF sample available for antibody testing. Clinical information was obtained by us or provided by the referring physicians through a written questionnaire, telephone interviews, or review of medical records. The OMS was considered P-OMS when a tumor was diagnosed within 5 years of onset of the neurological symptoms or when onconeuronal antibodies were identified.12
Written informed consent for the storage and use of samples for research was obtained from patients or representative family members. The study was approved by the institutional review boards of the University of Pennsylvania and Hospital Clínic, Barcelona.
Detection of Antineuronal Antibodies and Screening for Novel Cell Surface Autoantigens
All serum and CSF samples (70 paired samples, 39 serum samples, and 5 CSF samples) were examined for onconeural antibodies (Hu, Yo, Ri, CRMP5, amphiphysin, Ma2, Tr, and Zic4), glutamic acid decarboxylase (GAD), and cell surface antibodies (N-methyl-d-aspartate receptor [NMDAR], α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor [AMPAR], γ-aminobutyric acid type A receptor [GABAAR], γ-aminobutyric acid type B receptor [GABABR], glycine receptor [GlyR], contactin-associated protein 2 [CASPR2], leucine-rich glioma-inactivated protein 1 [LGI1], di-peptidyl-peptidase-like protein-6 [DPPX], metabotropic glutamate receptor 1 [mGluRl], and metabotropic glutamate receptor 5 [mGluR5]) using previously reported techniques.13-17 Samples were also examined for IgG and IgM antibodies to unknown cell surface antigens using a combination of techniques (tissue immunohistochemistry, cell-based assays, cultured live neurons) and the novel autoantigens precipitated, as reported.13,14 All techniques are explained in detail in the eAppendix in the Supplement.
To determine the relevance of GlyR antibodies in patients with OMS, serum samples of 254 controls (30 healthy individuals, 20 with neurodegenerative disorders, 55 with multiple sclerosis, 55 with autoimmune encephalitis with antibodies against surface antigens, 65 with lung cancer, and 29 with paraneoplastic neurological syndromes [PNSs] other than OMS associated with lung cancer) were used as controls. Human natural killer 1 (HNK-1) antibodies were investigated by immunohistochemistry (eAppendix in the Supplement) in the CSF samples of 20 patients with lung cancer and PNSs other than OMS.
Statistical Analysis
Demographic information and clinical and immunological features comparing P-OMS and I-OMS were analyzed with Fisher exact test, χ2 test, or Mann-Whitney U test when appropriate. Outcome analysis was only considered in patients with at least 3 months of follow-up and was assessed with the modified Rankin Scale (mRS).15 Patients were considered to have a good outcome if the mRS score at the last follow-up was 0 to 2 and a poor outcome if the mRS score was higher than 2. Factors influencing outcome were assessed by univariable binary logistic regression (eTable 1 in the Supplement). Factors associated with a poor outcome (P < .10) were included in a multivariate binary logistic regression model and approached by forward stepwise procedure; variables were considered independent when they remained statistically significant. Odds ratio with 95% confidence interval was used to measure the effect of independent variables. The 95% confidence interval for sensitivity and specificity of Ri antibodies for the diagnostic assessment of breast cancer was determined with the Wilson procedure. Stata version 13.1 statistical software (StataCorp LP) was used for the analyses.
Results
Clinical Features
One hundred fourteen adults with OMS (62 female [54%]; median age, 45 years; interquartile range [IQR], 32-60 years) fulfilled the study criteria. Forty-five patients (39%) had P-OMS and 69 (61%) had l-OMS. Patients with P-OMS included 19 (5 women) with lung cancer (13 with small cell lung cancer [SCLC] and 6 with non-SCLC), 10 with breast cancer, 8 with ovarian teratoma, and 5 men with other cancer types (1 patient each: testicular seminoma, stomach, thymus, kidney, and oropharyngeal carcinoma). Three additional patients without detectable cancer were considered to have P-OMS because they had positive results for onconeuronal antibodies (Ri, CRMP5, or Ma2). Symptoms of OMS preceded the diagnosis of the rumor in 29 of 42 patients (69%), with no differences among tumor types. Among the 13 patients whose tumor was diagnosed before onset of OMS, 4 developed the symptoms soon after tumor removal or biopsy, and another 3 developed the symptoms during chemotherapy. Onconeuronal antibodies were identified in 13 patients (11%) (Ri, 8; Ma2,3; Zic4,1; and CRMP5, 1). Seven of 10 patients (70%) with breast cancer harbored Ri antibodies (sensitivity, 70%; 95% CI, 40-89; specificity, 99%; 95% CI, 95-100). Other cancer types associated with onconeuronal antibodies were lung cancer (2 of 19 patients [11%]: 1 had Ma2 and the other Zic4 antibodies) and stomach cancer (1 patient with Ma2). The Table shows the clinical features of patients with I-OMS compared with those with P-OMS. Patients with I-OMS were younger than those with P-OMS (median age, 38 [IQR, 31-50] vs 54 [45-65] years; P < .001); however, the P-OMS group showed a bimodal age distribution: the group with ovarian teratoma was younger (median age, 23 years; IQR, 22-30 years) than those with I-OMS (P = .003), whereas the group with other tumors was older (median age, 60 years; IQR, 46-66 years; P < .001). Prodromal symptoms suggestive of viral infections or history of infection or of recent vaccinations were more frequent in patients with I-OMS (33% vs 13%; P = .02). Six patients with I-OMS, but none with P-OMS, had a confirmed active infection (4 with human immunodeficiency virus [HIV], 1 with hepatitis C virus, and 1 with tuberculosis). Acute vertigo with vomiting and/or gait instability was the most common symptom presentation in I-OMS or P-OMS, often leading to an initial misdiagnosis of peripheral vertigo. However, while patients with I-OMS were more likely than those with P-OMS to present with isolated vertigo (68% vs 49%; P = .04), patients with P-OMS more frequently had coexisting or early development of encephalopathy (29% vs 10%; P = .01) and other symptoms, such as cranial nerve palsy (16% vs 5%; P = .02) (Table).
Table. Clinical Features of Patients With P-OM5 and l-OMS.
| Characteristic | No.(%) | P Value | |
|---|---|---|---|
| P-OMS (n = 45) | I-OMS (n = 69) | ||
| Age, median (IQR), y | 54 (45-65)a | 38 (31-50) | <.001 |
| Female | 24 (53) | 38 (55) | .86 |
| Prodromal and/or infection | 6 (13) | 23 (33) | .02 |
| Autoimmune background | 3 (7) | 11 (16) | .14 |
| Presenting symptoms | |||
| Acute vertigo | 22 (49) | 47 (68) | .04 |
| Subacute ataxia or myoclonus | 11 (24) | 8 (12) | .07 |
| Other symptomsb | 12 (27) | 14 (20) | .43 |
| Additional symptoms at any time | |||
| Encephalopathy | 13 (29) | 7 (10) | .01 |
| Cranial nerve palsy | 7 (16) | 4 (5) | .02 |
| Severe behavioral changes | 6 (13) | 4 (6) | .16 |
| CSF studies (n = 90) | (n = 34) | (n = 56) | |
| Abnormal | 24(71) | 42 (75) | .65 |
| WBC count >5 μL | 16 (47) | 34 (61) | .21 |
| Protein >45 mg/dL | 14 (41) | 18 (32) | .38 |
| Follow-up, median (IQR), mo (n = 81) | (n = 38) | (n = 43) | |
| Duration, median (IQR), mo | 14 (6-27) | 20 (8-45) | .36 |
| Poor outcome, mRS score >2c | 23 (61) | 7 (16) | <.001 |
| QMS relapse | 9 (24) | 3 (7) | .04 |
Abbreviations: CSF, cerebrospinal fluid; l-OMS, idiopathic opsoclonus-myoclonus syndrome; IQR, interquartile range: mRS, Modified Rankin Scale; OMS, opsoclonus-myoclonus syndrome: P-OMS, paraneoplastic opsoclonus-myodonus syndrome: WBC, white blood cell.
SI conversion factor: To convert WBC count to ×109 per liter, multiply by 0.001.
Including 8 patients with ovarian teratoma who were much younger (median age, 23 years; IQR, 22-30 years).
Other symptoms at presentation included 8 patients with abnormal behavior, 7 with encephalopathy, 5 with cranial nerve palsy, 3 with lower limb bilateral weakness, and 1 each with lower limb radiculopathic pain, cognitive deficits, and insomnia.
Only patients with detailed information about treatment and follow-up longer than 3 months.
Detailed information regarding treatment and outcome was available for 81 patients (71%): 70 (86%) received immunotherapy and 11 (14%) did not. Among the 70 patients treated with immunotherapy, 27 (39%) received steroids, 10 (14%) received intravenous immunoglobulin (IVIg), 24 (34%) received steroids and IVIg, and 9 (13%) received steroids, IVIg, and plasma exchange. Six of these 70 patients also were treated with azathioprine (n = 4), rituximab (n = 1), or rituximab and mycophenolate mofetil (n = 1). At the last follow-up (median, 17 months; IQR, 6-33 months), 51 of 81 patients (63%) had a good outcome (36 complete or almost complete recovery [mRS score ≤2]) and 30 (37%) had a poor outcome (10 had an mRS score ≥3, 11 had an mRS score of 4 or 5, and 9 died). In multivariate analysis, independent factors significantly associated with a poor outcome adjusted by time of follow-up were being older than 40 years (odds ratio = 8.6; 95% CI, 1.9-38.4) and paraneoplastic origin (odds ratio = 6.9; 95% CI, 2.0-23.7). Twelve of 81 patients (15%) developed relapsing OMS; relapsing symptoms were more frequent in patients with P-OMS than in those with I-OMS (24% vs 7%; P = .04).
Antibodies to Known Neuronal Surface Antigens
Antibodies to known cell surface antigens were identified in the serum or CSF of 12 patients (11%), including 9 with antibodies to GlyR, 1 with antibodies to GABABR, 1 with antibodies to NMDAR, and 1 with antibodies to DPPX. The 2 patients with GABABR or NMDAR antibodies were young women (in their mid-30s) who developed typical OMS; the patient with GARABR antibodies was previously described.16 The patient with NMDAR antibodies was found to have an ovarian teratoma and fully recovered after tumor removal and administration of IVIg, and steroids. The patient with DDPX antibodies was a man in his late 50s who during 1 year developed weight loss (22 kg), dizziness, ataxia, diplopia, tremor, opsoclonus, myoclonus, and downbeat nystagmus. He also had insomnia, major depressive symptoms, and mild cognitive deficits. Findings on magnetic resonance imaging of the brain and cervical spine as well as electroencephalography were normal. He received oral steroids without symptom improvement.
Among the 9 patients (8%) with GlyR antibodies (7 in serum, 1 in CSF, and 1 in both), 6 had cancer (4 had lung cancer, 1 had breast cancer, and 1 had testicular seminoma); 3 of the 9 patients with GlyR antibodies had coexisting onconeural antibodies (Ri, Zic4, and Ma2). Overall, GlyR antibodies were more frequently detected in patients with OMS and lung cancer (4 of 19 patients [21%]) vs patients with OMS without lung cancer (5 of 95 patients [5%]) (P = .02). However, patients with lung cancer without OMS (13 of 65 patients [20%]) or with other PNSs (3 of 29 patients [10%]) also frequently had GlyR antibodies (P = .45). Of the 160 controls without cancer, 8 (5%) had GlyR antibodies (4 with multiple sclerosis and 4 with classic anti-NMDAR encephalitis).
No patients with OMS had GABAAR antibodies. The 2 previously described patients with these antibodies17 were not included because the clinical and outcome information was very limited.
Antibodies to Novel Neuronal Surface Antigens
Studies on rat brain sections and live hippocampal neurons identified 7 patients with antibodies against novel neuronal cell surface antigens. In 4 patients, the antibodies were of the IgG class (3 had I-OMS and 1 had OMS with ovarian teratoma) and immunoprecipitation studies did not reveal the antigen. In the other 3 patients (2 with non-SCLC and 1 with SCLC, 2 of them with coexisting GAD antibodies) without monoclonal gammopathy or neuropathy, IgM antibodies in brain sections had an immunoreactivity identical to that observed with a commercial monoclonal antibody (Sigma-Aldrich) against the glycosylated HNK-1 epitope or the serum of patients with neuropathy, monoclonal gammopathy, and IgM antibodies against myelin-associated glycoprotein (MAG), a protein that contains the HNK-1 epitope (Figure 1).18 The same results were obtained in immunoblots of an enriched extract of human myelin proteins (Figure 2). The specific HNK-1 reactivity of the 3 patients with IgM antibodies was confirmed in cultured live hippocampal neurons, which showed remarkable colocalization with the reactivity of the monoclonal HNK-1 antibody (Figure 3). Furthermore, immunoprecipitation studies using a mixed pool of CSF from the 3 patients consistently isolated sequences of glutamate receptor 2 (GluR2), a subunit of AMPAR known to contain the glycosylated HNK-1 epitope (20 peptides of GluR2 sequence, 21% of protein coverage; eFigure in the Supplement; Figure 4).20 These findings reveal a subset of patients with P-OMS and antibodies targeting proteins with the HNK-1 epitope. None of the 20 controls with SCLC without OMS had CSF IgM HNK-1 antibodies.
Figure 1. Immunostaining Results on Frozen Sections of Rat Brain.
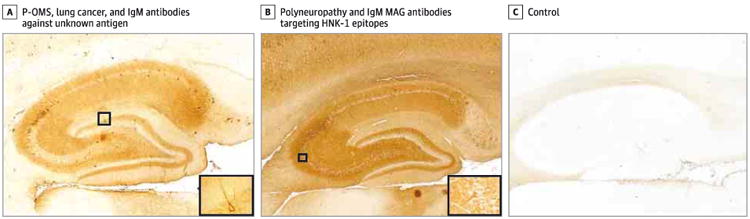
A-C. Immunoreactivity developed with standard avidin-biotin immunoperoxidase technique. A, Cerebrospinal fluid immunoreactivity from 1 of the 3 patients with paraneoplastic opsoclonus-myoclonus syndrome (P-OMS), lung cancer, and IgM antibodies against an unknown antigen (original magnification ×40). Inset, Higher-magnification image (original magnification ×400). B, This pattern of immunostaining was similar to that seen in patients with polyneuropathy and IgM myelin-associated glycoprotein (MAG) antibodies targeting glycosylated human natural killer 1 (HNK-1) epitopes. Note the high similarity in the staining surrounding the neuronaI celI bodies and a long proximal dendrites of large neurons (original magnification ×40). Inset, Higher-magnification image (original magnification ×400). C. The absence of reactivity in the cerebrospinal fluid of a control (original magnification ×40).
Figure 2. Immunoblot Results.
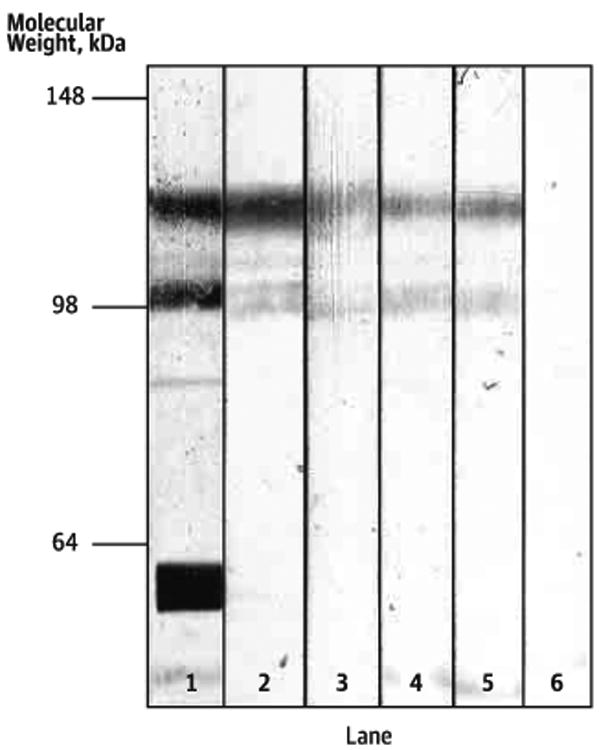
Immunoblot of human myelin proteins probed with serum of a patient with IgM myelin-associated glycoprotein antibodies and neuropathy (lane 1), a commercial antibody against human natural killer 1 (HNK-1) (lane 2), and the cerebrospinal fluid of our 3 patients with paraneoplastic opsoclonus-myoclonus syndrome and lung cancer (lanes 3-5). Note that all patient and commercial antibodies reacted with bands of similar molecular weight that are not shown by the negative control sample (lane 6).
Figure 3. Immunofluorescence Results.
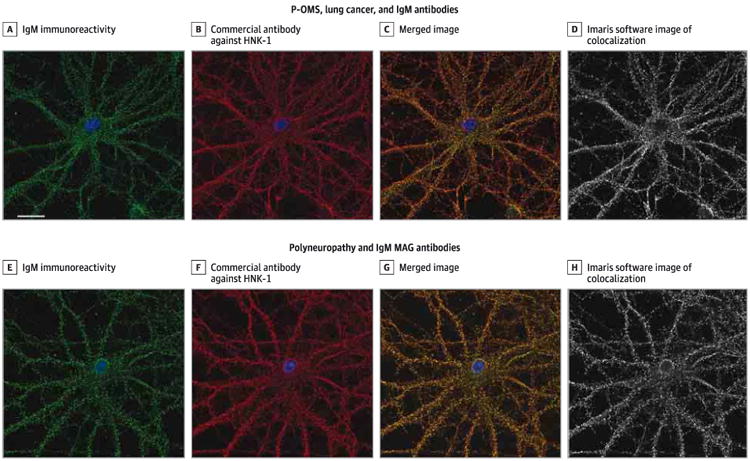
Immunofluorescence on live hippocampal neurons incubated with the cerebrospinal fluid of 1 of the 3 patients with paraneoplastic opsoclonus-myoclonus syndrome (P-OMS), lung cancer, and IgM antibodies (A-D) and the serum of a patient with polyneuropathy and IgM myelin-associated glycoprotein (MAG) antibodies (EH). The punctate IgM immunoreactivity of die 2 patients (A and E) colocalized with die reactivity of a commercial antibody against human natural killer 1 (HNK-1) (B and F), shown in the merged images (C and G); a high degree of colocalization was confirmed by Imaris software (Mander coefficient = 0.8 for both fluorescent channels; the coefficient ranges from 0.0 [no colocalization] to 1.0 [full colocalization]19) (D and H) (scale bar = 20 μrn).
Figure 4. Immunoblot Results of the Immunoprecipitated Proteins.
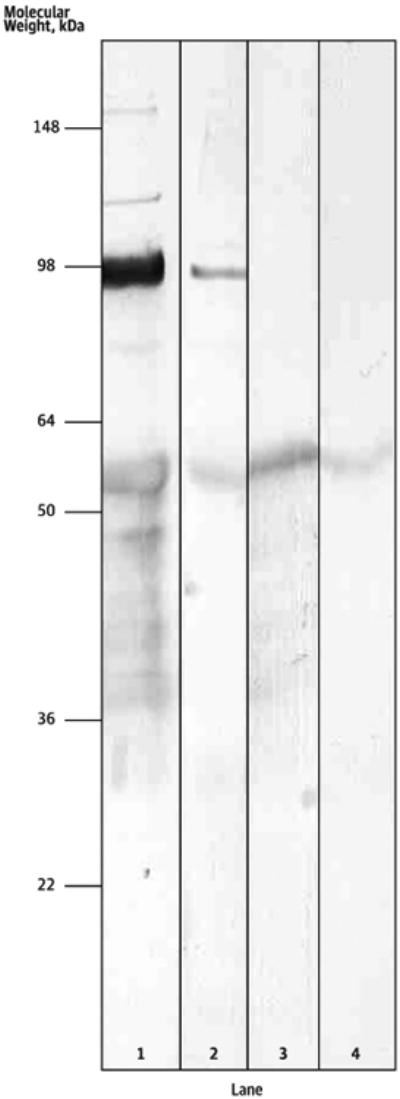
To determine whether the immunoprecipitated antigen was the glutamate receptor 2 (GluR2) subunit, immunoblots of neuronal proteins precipitated with cerebrospinal fluid from patients with paraneoplastic opsoclonus-myoclonus syndrome and IgM human natural killer 1 antibodies were probed with commercial antibodies against the GluR2 subunit of α-amino-3-hydroxy-5-methyl-4-isoxazolepropionicacid receptor (AMPAR) (lane 1) and a monoclonal human natural killer 1 antibody (lane 2). Both antibodies recognize a similar band in tine 98-kDa range consistent with GluR2. This band was not observed in immunoblots of neuronal proteins precipitated with a control's cerebrospinal fluid probed with the same antibodies against GluR2 (lane 3) and human natural killer 1 (lane 4).
Discussion
Our study represents the largest series, to our knowledge, of adult patients with OMS. The current findings along with those of previous studies2,3,21-23 have several practical implications for the diagnosis and management of patients with this disorder. First, once toxic, metabolic, and structural causes of OMS are ruled out,1 the most important indicator of paraneoplastic OMS is the patient's age. For adult patients younger than 40 years, the probability of an underlying tumor other than ovarian teratoma23 is very low, suggesting that aggressive or periodic investigations for an occult cancer and the use of extensive panels of paraneoplastic antibodies are not necessary (with the exception of Ri antibodies in middle-aged women). Second, P-OMS should be considered in older patients who develop encephalopathy or symptoms beyond the classic picture of OMS. The current series confirms that lung cancer, particularly SCLC, is the most frequently involved tumor, followed by breast and gynecological cancers.2,3 Third, whereas Ri/ANNA2 antibodies are good predictors of P-OMS related to breast cancer, other paraneoplastic antibodies are rare or not consistently found in P-OMS.2,3,9 In the present study, GlyR antibodies occurred in 21% of patients with lung cancer-related P-OMS, but the sensitivity and specificity were not robust enough to suggest the use of these antibodies as biomarkers of P-OMS. Fourth, compared with I-OMS, patients with P-OMS had more relapses and worse outcome, confirming our findings in a smaller previous series of patients.2 These results emphasize the need for tumor treatment and up-front use of more aggressive immunotherapies such as rituximab or intravenous cyclophosphamide to treat P-OMS.
In adults younger than 40 years, the most likely cause of OMS is idiopathic or parainfectious, both of which have a better prognosis than P-OMS or than OMS in children.24,25 First-line immunotherapies, such as steroids, IVIg, or plasma exchange, are associated with good outcome in most of these patients who usually receive 1 or several types of symptomatic therapy (topiramate,26 gabapentin,27 or benzodiazepines28; not investigated in the current study). Antineuronal antibodies are usually negative, although a few exceptions have been reported (summarized in eTable 2 in the Supplement).29-31 In this age group, it is important to exclude an underlying ovarian teratoma or HIV infection,23,32 which in the current series occurred in 12 of 70 patients younger than 40 years (17%). Patients with ovarian teratoma frequently develop additional symptoms, such as dysautonomia, behavioral change, or drowsiness, and results of testing for NMDAR antibodies are almost always negative.23 Although we identified a patient with OMS, ovarian teratoma, and NMDAR antibodies, the 3 previously reported cases (one of them a young child) with OMS and NMDAR antibodies had typical symptoms of anti-NMDAR encephalitis.33-35 Also, OMS may be the initial manifestation of HIV infection or may occur during immune reconstitution at the onset of antiretroviral therapy.36,37 There are no clinical features characteristic of HlV-related OMS; therefore, a high degree of awareness is needed for not missing this diagnosis.32,38,39
Glycine receptor antibodies were more frequent in P-OMS (mainly associated with SCLC) than in other forms of OMS. This finding is interesting because glycine is the neurotransmitter of omnipause neurons in the paramedian pontine reticular formation that exert a tonic inhibition of saccadic burst neurons.40,41 These antibodies were initially detected in patients with progressive encephalomyelitis with rigidity and myoclonus.42 Symptoms of progressive encephalomyelitis with rigidity and myoclonus, like those of OMS, are believed to result from a disturbance of the inhibitory (glycine/GABAergic) circuits, which would be altered by GlyR antibodies.42 However, GlyR antibodies were not found in a previous report that studied 4 patients with I-OMS.43 The presence of GlyR antibodies in our patients was unlikely related to OMS. Indeed, these antibodies have been reported (mainly in serum) in subgroups of patients with optic neuritis,44 GAD antibody-associated stiff person syndrome or cerebellar ataxia,45 and multiple sclerosis,44 suggesting that in some patients they may reflect a non-syndrome-specific immune activation, or propensity to autoimmunity. An alternative explanation is that GlyR antibodies may reflect the presence of a tumor; this is supported by a similar frequency of these antibodies in patients with SCLC without OMS or with other PNSs, and the expression of the α1 subunit of the GlyR in SCLC cell lines.46
We detected IgM antibodies against the carbohydrate epitope HNK-1 in the CSF of 3 patients with P-OMS and lung cancer. The HNK-1 epitope is the main target epitope of IgM antibodies against MAG in patients with neuropathy and IgM monoclonal gammopathy18 and, to our knowledge, HNK-1 has not been previously reported as an autoantigen in other neurological disorders. This epitope has been previously reported in membrane proteins of cell lines and biopsies of SCLC.47,48 In brain, HNK-1 is present not only in MAG but also in several proteins such as cell adhesion molecules, tenascins, and integrins widely present in the brain.49,50 These proteins as well as the HNK-1-containing GluR2 subunit of AMPAR, which was precipitated with the CSF of our patients, are involved in synaptic plasticity and a variety of neuronal functions.20
Conclusions
Our findings show that OMS in adults is the common manifestation of different disorders associated with distinct comorbidities (cancer, teratoma, idiopathic, inflammation, infection) and a variety of paraneoplastic and cell surface autoantibodies that were collectively detected in only 19% of the patients (10 patients with onconeural antibodies, 9 with antibodies to known cell surface antigens, and 3 with both types of antibodies). Future studies aiming to identify immunological mechanisms in OMS should focus on methods different from those used in autoimmune encephalitis and cell surface antigens. Although unknown antibodies may still be involved, as shown here in 3 patients, an impairment of synaptic signaling by other mechanisms, perhaps circulating inflammatory molecules, should be considered. Electrophysiological assessment of neuronal cultures or acute slices of brain exposed to patients' serum or CSF may shed light on the type of molecular targets involved. Meanwhile, the clinical profile of OMS suggests an immune-mediated pathogenesis. Immunotherapy should be considered despite the fact that no antibody markers are identified in most patients.
Supplementary Material
Key Points.
Question
Are there clinical clues or antibody biomarkers that differentiate idiopathic from paraneoplastic opsoclonus-myoclonus syndrome (OMS)?
Results
In this cohort study, older age and encephalopathy were significantly associated with paraneoplastic OMS, and paraneoplastic OMS and being older than 40 years were independently associated with poor outcome. Neuronal surface antibodies were identified in 12 patients (11%), mainly glycine receptor antibodies, which predominated in paraneoplastic OMS with lung cancer.
Meaning
Patients with idiopathic OMS had better outcomes than those with paraneoplastic OMS.
Acknowledgments
Funding/Support: This work was supported in part by grants FIS12/00611 (Drs Bataller and Graus). FIS 14/00203 (Dr Dalmau), CM14/00081 (Dr Armangué), and CD14/00155 (Dr Martínez-Hernández) from Institute de Salud Carlos III, grant RO1NS077851 from the National Institutes of Health (Dr Dalmau), and Fundació CELLEX (Dr Dalmau). Dr Dalmau is supported by a research grant from Euroimmun.
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Footnotes
Author Contributions: Drs Armangué and Sabater contributed equally to this work. Dr Graus had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Armangué, Sabater, Bataller, Dalmau, Graus.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Armangué, Dalmau, Graus.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Armangué.
Obtained funding: Armangué, Martínez-Hernández, Bataller, Dalmau, Graus.
Administrative, technical, or material support: Planagumà. Dalmau.
Study supervision: Bataller, Dalmau, Graus.
Additional Contributions: We thank all the physicians who have contributed by providing clinical information of their patients, and we thank all the patients for their generous contribution to research. Mercè Alba, BS, Esther Aguilar, BS, and Eva Caballero, BS, Institut d'lnvestigació Biomèdica August Pi i Sunyer, Barcelona, Spain, provided technical support; they received no compensation.
Conflict of Interest Disclosures: Dr Dalmau reported receiving royalties from patents for the use of Ma2 and NMDAR and from intellectual property for the use of GABABR. DPPX, and GABAAR as diagnostic tests. No other disclosures were reported.
References
- 1.Caviness JN, Forsyth PA, Layton DD, McPhee TJ. The movement disorder of adult opsoclonus. Mov Disord. 1995;10(1):22–27. doi: 10.1002/mds.870100106. [DOI] [PubMed] [Google Scholar]
- 2.Bataller L, Graus F, Saiz A, Vilchez JJ Spanish Opsoclonus-Myoclonus Study Group. Clinical outcome in adult onset idiopathic or paraneoplastic opsoclonus-myoclonus. Brain. 2001;124(pt 2):437–443. doi: 10.1093/brain/124.2.437. [DOI] [PubMed] [Google Scholar]
- 3.Klaas JP, Ahlskog JE, Pittock SJ, et al. Adult-onset opsoclonus-myoclonus syndrome. Arch Neurol. 2012;69(12):1598–1607. doi: 10.1001/archneurol.2012.1173. [DOI] [PubMed] [Google Scholar]
- 4.Pike M. Opsoclonus-myoclonus syndrome. Handb Clin Neurol. 2013;112:1209–1211. doi: 10.1016/B978-0-444-52910-7.00042-8. [DOI] [PubMed] [Google Scholar]
- 5.Pranzatelli MR. The immunopharmacology of the opsoclonus-myoclonus syndrome. Clin Neuropharmacol. 1996;19(1):1–47. doi: 10.1097/00002826-199619010-00001. [DOI] [PubMed] [Google Scholar]
- 6.Ridley A, Kennard C, Scholtz CL, Biittner-Ennever JA, Summers B, Turnbull A. Omnipause neurons in two cases of opsoclonus associated with oat cell carcinoma of the lung. Brain. 1987;110(pt6):1699–1709. doi: 10.1093/brain/110.6.1699. [DOI] [PubMed] [Google Scholar]
- 7.Young CA, MacKenzie JM, Chadwick DW, Williams IR. Opsoclonus-myoclonus syndrome: an autopsy study of three cases. Eur J Med. 1993;2(4):239–241. [PubMed] [Google Scholar]
- 8.Bataller L, Rosenfeld MR, Graus F, Vilchez JJ, Cheung NK, Dalmau J. Autoantigen diversity in the opsoclonus-myoclonus syndrome. Ann Neurol. 2003;53(3):347–353. doi: 10.1002/ana.10462. [DOI] [PubMed] [Google Scholar]
- 9.Luque FA, Furneaux HM, Ferziger R, et al. Anti-Ri: an antibody associated with paraneoplastic opsoclonus and breast cancer. Ann Neurol. 1991;29(3):241–251. doi: 10.1002/ana.410290303. [DOI] [PubMed] [Google Scholar]
- 10.Leypoldt F, Armangue T, Dalmau J. Autoimmune encephalopathies. Ann N Y Acad Sci. 2015;1338:94–114. doi: 10.1111/nyas.12553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Panzer JA, Anand R, Dalmau J, Lynch DR. Antibodies to dendritic neuronal surface antigens in opsoclonus myoclonus ataxia syndrome. J Neuroimmunol. 2015;286:86–92. doi: 10.1016/j.jneuroim.2015.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Graus F, Delattre JY, Antoine JC, et al. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry. 2004;75(8):1135–1140. doi: 10.1136/jnnp.2003.034447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dalmau J, Lancaster E. Martinez-Hernandez E, Rosenfeld MR, Balice-Gordon R. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol. 2011;10(1):63–74. doi: 10.1016/S1474-4422(10)70253-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lancaster E, Lai M, Peng X, et al. Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen. Lancet Neurol. 2010;9(1):67–76. doi: 10.1016/S1474-4422(09)70324-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19(5):604–607. doi: 10.1161/01.str.19.5.604. [DOI] [PubMed] [Google Scholar]
- 16.DeFelipe-Mimbrera A, Masjuan J, Corral Í, Villar LM, Graus F, García-Barragán N. Opsoclonus-myoclonus syndrome and limbic encephalitis associated with GABAB receptor antibodies in CSF. J Neuro mmuno. 2014(1-2):272. 91–93. doi: 10.1016/j.jneuroim.2014.04.009. [DOI] [PubMed] [Google Scholar]
- 17.Petit-Pedrol M, Armangue T, Peng X, et al. Encephalitis with refractory seizures, status epilepticus, and antibodies to the GABAA receptor: a case series, characterisation of the antigen, and analysis of the effects of antibodies. Lancet Neurol. 2014;13(3):276–286. doi: 10.1016/S1474-4422(13)70299-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ilyas AA, Quarles RH, Macintosh TD, et al. IgM in a human neuropathy related to paraproteinemia binds to a carbohydrate determinant in the myelin-associated glycoprotein and to a ganglioside. Proc Nat Mcad Sci USA. 1984;81(4):1225–1229. doi: 10.1073/pnas.81.4.1225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McDonald JH, Dunn KW. Statistical tests for measures of colocalization in biological microscopy. J Microsc. 2013;252(3):295–302. doi: 10.1111/jmi.12093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Takeuchi Y, Morise J, Morita I, Takematsu H, Oka S. Role of site-specific N-glycans expressed on GluA2 in the regulation of cell surface expression of AMPA-type glutamate receptors. PLoS One. 2015;10(8):e0135644. doi: 10.1371/journal.pone.0135644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Anderson NE, Budde-Steffen C, Rosenblum MK, et al. Opsoclonus, myoclonus, ataxia, and encephalopathy in adults with cancer: a distinct paraneoplastic syndrome. Medicine (Baltimore) 1988;67(2):100–109. doi: 10.1097/00005792-198803000-00003. [DOI] [PubMed] [Google Scholar]
- 22.Digre KB. Opsoclonus in adults: report of three cases and review of the literature. Arch Neurol. 1986;43(11):1165–1175. doi: 10.1001/archneur.1986.00520110055016. [DOI] [PubMed] [Google Scholar]
- 23.Armangue T, Titulaer MJ, Sabater L, et al. A novel treatment-responsive encephalitis with frequent opsoclonus and teratoma. Ann Neurol. 2014;75(3):435–441. doi: 10.1002/ana.23917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Matthay KK, Blaes F, Hero B, et al. Opsoclonus myoclonus syndrome in neuroblastoma: a report from a workshop on the dancing eyes syndrome at the advances in neuroblastoma meeting in Genoa, Italy, 2004. Cancer Lett. 2005;228(1-2):275–282. doi: 10.1016/j.canlet.2005.01.051. [DOI] [PubMed] [Google Scholar]
- 25.De Grandis E, Parodi S, Conte M, et al. Long-term follow-up of neuroblastoma-associated opsoclonus-myoclonus-ataxia syndrome. Neuropediatrics. 2009;40(3):103–111. doi: 10.1055/s-0029-1237723. [DOI] [PubMed] [Google Scholar]
- 26.Fernandes TD, Bazan R, Betting LE, da Rocha FC. Topiramate effect in opsoclonus-myoclonus-ataxia syndrome. Arch Neurol. 2012;69(1):133. doi: 10.1001/archneurol.2011.717. [DOI] [PubMed] [Google Scholar]
- 27.Moretti R, Torre P, Antonello RM, Nasuelli D, Cazzato G. Opsoclonus-myoclonus syndrome: gabapentin as a new therapeutic proposal. Eur J Neurol. 2000;7(4):455–456. doi: 10.1046/j.1468-1331.2000.00091.x. [DOI] [PubMed] [Google Scholar]
- 28.Bartos A. Effective high-dose clonazepam treatment in two patients with opsoclonus and myoclonus: GABAergic hypothesis. Eur Neurol. 2006;56(4):240–242. doi: 10.1159/000096494. [DOI] [PubMed] [Google Scholar]
- 29.Ariño H, Hoftberger R, Gresa-Arribas N, et al. Paraneoplastic neurological syndromes and glutamic acid decarboxylase antibodies. JAMA Neurol. 2015;72(8):874–881. doi: 10.1001/jamaneurol.2015.0749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Candler PM, Dale RC, Griffin S, et al. Post-streptococcal opsoclonus-myoclonus syndrome associated with anti-neuroleukin antibodies. J Neurol Neurosurg Psychiatry. 2006;77(4):507–512. doi: 10.1136/jnnp.2005.078105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Morales-Briceño H, Rodríguez-Violante M, Cervantes-Arriaga A, Irani SR, Lees AJ, Silveira-Moriyama L. Opsoclonus myoclonus syndrome associated with GQlb antibodies. Mov Disord. 2012;27(13):1615–1616. doi: 10.1002/mds.25169. [DOI] [PubMed] [Google Scholar]
- 32.Scott KM, Parker F, Heckmann JM. Opsoclonus-myoclonus syndrome and HIV-infection. J Neuro Sci. 2009;284(1-2):192–195. doi: 10.1016/j.jns.2009.04.026. [DOI] [PubMed] [Google Scholar]
- 33.Smith JH, Dhamija R, Moseley BD, et al. N-methyl-D-aspartate receptor autoimmune encephalitis presenting with opsoclonus-myoclonus: treatment response to plasmapheresis. Arch Neurol. 2011;68(8):1069–1072. doi: 10.1001/archneurol.2011.166. [DOI] [PubMed] [Google Scholar]
- 34.Kurian M, Lalive PH, Dalmau JO, Horvath J. Opsoclonus-myoclonus syndrome in anti-N-methyl-D-aspartate receptor encephalitis. Arch Neurol. 2010;67(1):118–121. doi: 10.1001/archneurol.2009.299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Player B, Harmelink M, Bordini B, Weisgerber M, Girolami M, Croix M. Pediatric opsoclonus-myoclonus-ataxia syndrome associated with anti-N-methyl-D-aspartate receptor encephalitis. Pediatr Neurol. 2015;53(5):456–458. doi: 10.1016/j.pediatrneurol.2015.07.010. [DOI] [PubMed] [Google Scholar]
- 36.van Toorn R, Rabie H, Warwick JM. Opsoclonus-myoclonus in an HIV-infected child on antiretroviral therapy: possible immune reconstitution inflammatory syndrome. Eur J Paediatr Neurol. 2005;9(6):423–426. doi: 10.1016/j.ejpn.2005.06.007. [DOI] [PubMed] [Google Scholar]
- 37.Kanjanasut N, Phanthumchinda K, Bhidayasiri R. HIV-related opsoclonus-myoclonus-ataxia syndrome: report on two cases. Clin Neurol Neurosurg. 2010;112(7):572–574. doi: 10.1016/j.clineuro.2010.03.024. [DOI] [PubMed] [Google Scholar]
- 38.Ayarza A, Parisi V, Altclas J, et al. Opsoclonus-myoclonus-ataxia syndrome and HIV seroconversion. J Neurol. 2009;256(6):1024–1025. doi: 10.1007/s00415-009-5046-1. [DOI] [PubMed] [Google Scholar]
- 39.Wiersinga WJ, Prins JM, van de Beek D. Therapy-resistant opsoclonus-myoclonus syndrome secondary to HIV-1 infection. Clin Infect Dis. 2012;54(3):447–448. doi: 10.1093/cid/cir711. [DOI] [PubMed] [Google Scholar]
- 40.Lynch JW. Native glycine receptor subtypes and their physiological roles. Neuropharmacology. 2009;56(1):303–309. doi: 10.1016/j.neuropharm.2008.07.034. [DOI] [PubMed] [Google Scholar]
- 41.Horn AK, Büttner-Ennever JA, Wahle P, Reichenberger I. Neurotransmitter profile of saccadic omnipause neurons in nucleus raphe interpositus. J Neurosci. 1994;14(4):2032–2046. doi: 10.1523/JNEUROSCI.14-04-02032.1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Carvajal-González A, Leite Ml, Waters P, et al. Glycine receptor antibodies in PERM and related syndromes: characteristics, clinical features and outcomes. Brain. 2014;137(pt 8):2178–2192. doi: 10.1093/brain/awu142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.lizuka T, Leite Ml, Lang B, et al. Glycine receptor antibodies are detected in progressive encephalomyelitis with rigidity and myoclonus (PERM) but not in saccadic oscillations. J Neurol. 2012;259(8):1566–1573. doi: 10.1007/s00415-011-6377-2. [DOI] [PubMed] [Google Scholar]
- 44.Martinez-Hernandez E, Sepulveda M, Rostásy K, et al. Antibodies to aquaporin 4, myelin-oligodendrocyte glycoprotein, and the glycine receptor α1 subunit in patients with isolated optic neuritis. JAMA Neurol. 2015;72(2):187–193. doi: 10.1001/jamaneurol.2014.3602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ariño H, Gresa-Arribas N, Blanco Y, et al. Cerebellar ataxia and glutamic acid decarboxylase antibodies: immunologic profile and long-term effect of immunotherapy. JAMA Neurol. 2014;71(8):1009–1016. doi: 10.1001/jamaneurol.2014.1011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gurrola-Diaz C, Lacroix J, Dihlmann S, Becker CM, von Knebel Doeberitz M. Reduced expression of the neuron restrictive silencer factor permits transcription of glycine receptor alpha1 subunit in small-cell lung cancer cells. Oncogene. 2003;22(36):5636–5645. doi: 10.1038/sj.onc.1206790. [DOI] [PubMed] [Google Scholar]
- 47.Hozumi I, Sato S, Tunoda H, et al. Shared carbohydrate antigenic determinant between the myelin-associated glycoprotein (MAG) and lung cancers: an immunohistochemical study by an anti-MAG IgM monoclonal antibody. J Neuroimmunol. 1987;15(2):147–157. doi: 10.1016/0165-5728(87)90089-0. [DOI] [PubMed] [Google Scholar]
- 48.Willison HJ, Minna JD, Brady RO, Quarles RH. Glycoconjugates in nervous tissue and small cell lung cancer share immunologically cross-reactive carbohydrate determinants. J Neuroimmunol. 1986;10(4):353–365. doi: 10.1016/S0165-5728(86)90018-4. [DOI] [PubMed] [Google Scholar]
- 49.Matà S, Ambrosini S, Mello T, Lolli F, Minciacchi D. Anti-myelin associated glycoprotein antibodies recognize HNK-1 epitope on CNS. J Neuroimmunol. 2011;236(1-2):99–105. doi: 10.1016/j.jneuroim.2011.05.002. [DOI] [PubMed] [Google Scholar]
- 50.Kizuka Y, Oka S. Regulated expression and neural functions of human natural killer-1 (HNK-1) carbohydrate. Cell Mot Life Sci. 2012;69(24):4135–4147. doi: 10.1007/s00018-012-1036-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.