

Abstract
Purpose of Review
This review examines recent literature on injury epidemiology and prevention in the sport of baseball from youth to professional levels.
Recent Findings
Overuse is the predominant mechanism of injury in youth baseball players. Newer stretching and exercise protocols may help prevent these injuries. At the professional level, however, overuse has not been proven to correlate with increased injury incidence, but pitch counts are still monitored. There continues to be a rise in operations performed for baseball-related injuries, including ulnar collateral ligament (UCL) reconstruction, particularly in younger athletes. As the level of play increases, there is significant loss of participation due to injuries, such as the UCL in the upper extremity and the hamstrings in the lower extremity.
Summary
Baseball is a widely popular sport, which has led to a focus on injury epidemiology and prevention. While the majority of research regarding baseball injuries focuses on pitchers, fielders and catchers are also at risk. In an attempt to decrease non-contact injuries in the upper and lower extremities, stretching and strengthening exercises are vitally important. Because injury profiles demonstrate significant variability from youth to professional baseball, unique prevention strategies are likely necessary at each level. More research is needed to develop and validate appropriately targeted injury prevention programs.
Keywords: Baseball injuries, Injury prevention, Ulnar collateral ligament, Overuse, Professional, Youth
Introduction
Every year, approximately three million children play baseball in the USA [1]. Many of these kids continue to play through their adolescent and high school years. Approximately 25,000 athletes compete each year in National Collegiate Association of America (NCAA) baseball at the collegiate level [2]. A select few of these end up playing minor or major league baseball. This high level of sports participation by the population creates a large role for health care providers in the care of the injured baseball players. It is extremely important for these providers to have a thorough understanding of the sports-specific injuries that effect baseball athletes.
Recently, there has been an increased scientific interest in baseball injury epidemiology and prevention. This increased interest is no surprise given the amount of youth involvement and increased push for young athletes to focus on a single sport year-round. In addition, major league baseball is a 36 billion-dollar business, and each franchise has an understandably strong interest in the health of its players [3]. Examples of well-known baseball-specific injuries are Little League elbow (in youth throwers) and medial ulnar collateral ligament (MUCL) injury, better known as a “Tommy John” injury. Both of these can result in significant loss of participation time. A MUCL injury, for example, results in an average of 17.1 months out of competition at the professional level [4•].
The available literature regarding injuries is highly variable depending on the age of the athletes. For example, the most robust research on injury epidemiology exists at the professional level while the majority of literature on injury prevention research has been conducted for the youth population. The primary purposes of this review are to summarize the current literature on baseball injury epidemiology, review prevention strategies, and provide suggestions for future research efforts. Special attention will be paid to injuries based on levels of play such as follows: youth, high school, college, and professional baseball.
Youth
Though baseball is a relatively safe sport for children, overuse and throwing injuries remain a significant problem, particularly among pre-adolescent and adolescent pitchers. Many traumatic injuries, such as on-field collisions, base-running injuries, baseball impact injuries, and concussions, may be unavoidable during gameplay but can be reduced by protective equipment. Prevention and safety strategies for young players continue to be researched in order to best ensure long-term, injury-free participation in the sport.
Epidemiology
For the purpose of this paper, youth injuries have been divided into overuse and non-overuse injuries. Young baseball players, particularly pitchers, are prone to overuse injuries such as Little League elbow and shoulder. Unfortunately, we know that these young athletes often play with pain. Up to 74% of youth baseball players (ages 8–18) report some degree of arm pain while throwing, and almost a quarter (23%) report injury histories [5] consistent with overuse [6•].
Five percent of youth pitchers will suffer a serious elbow or shoulder injury within 10 years, and pitching volume is the strongest known predictor of injury [7]. A survey of 754 youth pitchers (9–18 years old) revealed that a significant portion have engaged in non-recommended activities according to recent guidelines published by the American Sports Medicine Institute [5]. More than 43% pitched on consecutive days, 31% pitched on multiple teams with overlapping seasons, and 19% pitched multiple games per day, resulting in an increased risk of pitching-related arm pain. Arm pain related to pitching is indicative of overuse, and these pitchers are likely at increased risk of real injury to the elbow and shoulder [8]. What is more concerning are the results of a survey by Makhni et al., in which 46% of youth respondents said they were encouraged on at least one occasion to keep playing despite having arm pain [6•].
Prevention
Overuse, arm fatigue, high pitch velocity, participation in showcases, and traveling baseball are all associated with increased risk for injury [9, 10]. Another potential risk factor is early physical maturity [11]. Players that are bigger and stronger are usually overrepresented in key positions such as pitcher, where overuse injuries are more common. Pitchers who also play catcher seem to be at increased risk, likely due to the increased number of throws during the season.
Whether or not to allow skeletally immature players to throw breaking balls remains controversial. Historically, experts recommended that boys refrain from throwing breaking pitches due to the theory that the physis and UCL insertion cannot safely withstand the forces placed on the elbow while throwing a curveball. Existing clinical, epidemiologic, and biomechanical data does not support this claim; however, many leading clinicians and organizations have discouraged curveballs before skeletal maturity [7]. Dun et al. and Nissen et al. found that although increased forearm supination is required to throw a curveball, elbow varus torque is actually significantly less than with throwing a fastball in both adolescent and high school pitchers [12, 13]. Similarly, there are lower moments on the shoulder and elbow while throwing a curveball [13].
A newer study by Oliver et al. evaluated the pitching mechanics of youth baseball pitchers with the use of surface electromyography [14•]. Examining mechanics and muscle activation in the pelvis, torso, and upper extremity, they found no differences in mechanics of pitchers throwing fastballs, change-ups, and curveballs. Essentially, they reported that pitchers obtain the spin needed for a curveball from their grip, not by altering their arm slot or upper extremity mechanics, indicating that throwing a curveball is no more dangerous than other pitches [14•].
Despite the adoption of safety guidelines, pitch count recommendations, and increased media coverage on injury prevention for youth baseball players, injuries in this age group do not seem to be decreasing. There remains a lack of knowledge of safe throwing practices and compliance with safety recommendations, both in players and in coaches. For example, in a survey of 98 youth baseball players, ages 4 to 16, 63% of respondents disagreed with the statement “The more you throw, the more likely you are to get an injury.” A majority of respondents also reported that they would continue playing if they experienced an injury or had a sore arm during a game (64 and 61%, respectively) [15]. Clearly, further dissemination of this information is needed.
The role of the parent is crucial as well. When a child complains of arm pain, the parents and coaches must act in the best interest of the child. This includes a period of avoidance of throwing activities and management with ice, NSAIDs, and stretching. They should also be evaluated by a sports medicine physician. While not participating in throwing activities, they should perform general conditioning and core strength exercises [16].
Based on data from numerous studies evaluating biomechanics and throwing injuries, young pitchers should first learn proper fastball mechanics and consistency in their motions. Players should not pitch competitively more than 8 months per year, and they should follow pitch count limits and recommended day offs. Coaches should avoid the use of radar guns when possible, particularly in practices, as this may be correlated with increased risk of injury [7, 17].
Recently, Sakata et al. performed a prospective cohort study including 305 youth baseball players aged 8–11, evaluating a novel stretching and strengthening protocol called the Yokohama Baseball-9 (YKB-9). It includes nine stretching (Fig. 1) and strengthening (Fig. 2) exercises. The 10-s long stretches are designed to improve posture and range of motion (ROM) of the elbow, shoulder, and hip. The strength exercises focus on rotator cuff, scapular function, posture, and lower extremity balance. Players who participated in the YKB-9 had approximately 50% fewer medial elbow injuries over the course of a 12-month follow-up period [18•].
Fig. 1.
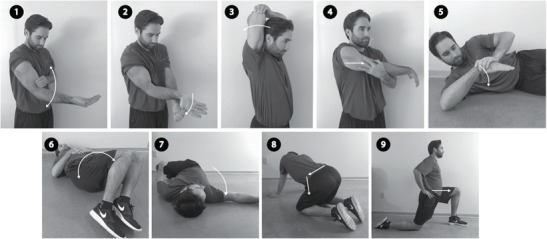
Nine stretching exercises as described in the Yokohama Baseball-9 protocol
Fig. 2.
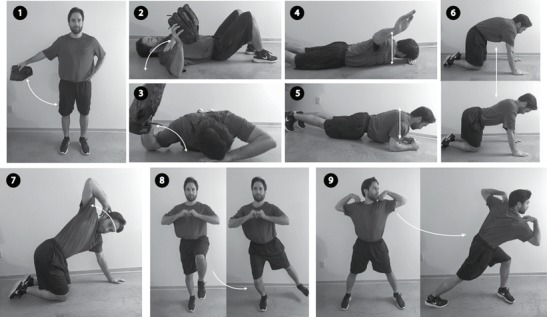
Nine strength exercises as described in the Yokohama Baseball-9 protocol
In terms of non-overuse injuries, most prevention is provided by protective/adaptive equipment, but teaching of proper fielding, batting, and base-running techniques should also be incorporated. Face guards lower the risk of facial and dental trauma and are increasingly accepted in lower levels of play [19, 20]. Softer “safety” baseballs reduce contusions but may increase the risk of eye injury due to deforming characteristics [19]. Breakaway bases reduce injuries associated with sliding, such as foot and ankle sprains and fractures [21, 22].
Overall, good mechanics combined with common sense practices, awareness of pitch counts, pre-activity stretching and strengthening, avoidance of fatigue, and use of the aforementioned protective equipment likely remain the best measures to prevent injuries in the young baseball player. Moving forward, future efforts should be directed at better informing players, parents, and coaches of recommended pitch limits, and the fact that any player who is experiencing pain should not continue to play until they are pain free.
High School
Baseball remains popular among high school students as well, with approximately 500,000 participants across the USA. It is the fourth most participated sport in high school, behind football, track, and basketball [23]. As with youth baseball athletes, high school athletes are at risk for overuse and traumatic injuries. Injuries in high school players tend to be more severe compared to youth players, as evidenced by the increased rate of surgery [24].
Epidemiology
Injuries in high school baseball players occur at approximately 1 injury per 1000 practices or competitions [25]. Overuse injuries commonly involve the shoulder and elbow. Shoulder injuries occur around 1.39–1.72 per 10,000 athlete-exposures (AEs), with muscle strains being most common [26, 27]. Juniors and seniors sustain a majority (69%) of shoulder injuries compared to freshmen and sophomores, as they are participating in a higher level of competition and playing in more games. Pitchers account for the largest proportion of shoulder injuries (38%). Approximately 10% of shoulder injuries require surgery and three-quarters of them are among pitchers [26].
Elbow injuries are less frequent at 0.86 per 10,000 AEs and most often involve ligamentous sprains (42.7%) [27]. The rate of elbow operations in young athletes has significantly risen over the last couple of decades. Some orthopedic practices have seen a sixfold increase in the number of elbow surgeries performed on high school pitchers from 2000 to 2004 compared to 1994–1999 [24] with approximately 13% of ulnar collateral ligament reconstructions being performed on high school players [28].
Fourteen percent of high school baseball injuries result in time loss from participation (sitting out greater than 1 day) [29]. Although most athletes get back to playing in less than a week, approximately 10% will miss an entire season due to their injury [27, 30].
Catastrophic injuries such as commotio cordis and traumatic brain are fortunately very rare in the sport of baseball. Of the 128 cases of commotio cordis reported in the USA over a 20-year period, however, approximately 40% were caused by a thrown or batted baseball [31]. Of the major high school sports, baseball has the lowest risk of traumatic brain injury at 0.05 per 1000 AEs [20].
Prevention
Many of the preventative measures in youth baseball apply to high school baseball as well, including pitch count limits, strengthening and stretching programs, use of protective gear, and continuation of proper mechanics.
Given that 12% of baseball injuries in high school occur to the head and face, many clinicians would recommend use of helmets with face shields or at least mouth guards for batters [20, 30]. Pitchers and infielders may also benefit from using mouth guards.
Players should be vigilant in stretching to maintain flexibility of both upper and lower extremities before and during the season. There seems to be a correlation between tightness in the quadriceps, hamstring, and shoulder internal rotators and shoulder and elbow pain. Core strength and stability is likely also important for injury prevention and high performance [32]. The YKB-9 stretching and strengthening program seems to drastically reduce medial elbow injuries in adolescents and is likely translatable to the high school athlete as well [18•].
College
There is paucity of literature regarding collegiate baseball injury epidemiology and prevention. Even though there is a significant amount of professional baseball players being drafted out of high school, college baseball remains the gateway to the majors so the lack of research is surprising. The National Collegiate Athletic Association (NCAA) consists of three divisions with Division 1 being the most competitive, and there are approximately 25,000 collegiate baseball players each year [2]. Although the majority of these players will not end up playing professionally, an understanding of the epidemiology and prevention of college baseball injuries are important to avoid future morbidity.
Epidemiology
McFarland et al. first conducted a prospective epidemiologic study evaluating injury incidence at a single Division 1 institution [33]. Over a 3-year period, the overall incidence of injuries was 5.83 per 1000 athlete-exposures (AEs). They found that upper extremity injuries accounted for 58% of all injuries. The shoulder was the most commonly injured body part and typically resulted in around a week of lost participation time. They defined a severe injury as those resulting in 21 or more days of lost participation. Twenty-five percent of all injuries were considered severe. The most common injuries were characterized as strains (23%), sprains (19%), and contusions (17%). In contrast to this study, other studies have found sliding injuries to be common [34, 35]. A more recent epidemiologic study by Dick et al. [35] reported on 16 years of NCAA injury surveillance data. They found injury rates to be three times higher in games compared to those in practice. The game injury rate was 5.78 per 1000 AEs, which is very similar to that found in the aforementioned study [33]. The most common player positions to incur injury were base runners (23.7%), pitchers (20.9%), and batters (15.3%). As expected, upper extremity injuries accounted for the majority of reported injuries. It was somewhat surprising though that upper leg and ankle injuries were more common than shoulder injuries in game play. Shoulder injuries were more common in practice. The majority of injuries incurred during games were the result of contact, whereas 63.9% of practice injuries were non-contact. The nature of contact injuries in baseball have been described as occurring as a result of base-running, base-sliding, ball-contact, bat-contact, and player-player contact [33–36]. Dick et al. defined a severe injury as those resulting in ten or more days of lost participation and found 25% of all injuries to be severe [35]. Although rare, clinicians must also be aware of the potential for fatal and non-fatal catastrophic injuries in collegiate baseball. Boden et al. [37] reported the catastrophic injury rate to be 1.7 per 100,000 baseball players and the fatal catastrophic injury rate to be 0.86 per 100,000 baseball players during a 21-year period.
Prevention
Injuries were found to be most common in pre-season and early season practices and games, respectively. This is a testament to the importance of off-season conditioning and progression of pre-season workout intensity [35]. There is a lack of injury prevention literature specific to collegiate baseball; however, many of the youth injury prevention principles still apply. Interestingly, pitch type has not been suggestive of increased risk of injury for college pitchers although change-ups do demonstrate the lowest kinetic demand and may be safest [24]. Prevention strategies should focus on upper and lower extremity strengthening, proper throwing mechanics, avoiding overuse, stretching exercises, avoiding collisions, and proper utilization of protective gear [38–40]. As many of these strategies are drawn from the youth and professional levels, more research is needed into specific college baseball preventative measures.
Professional
There is an increasing amount of literature regarding injury epidemiology and prevention in minor (MiLB) and major league baseball (MLB). Major league baseball is considered one of the most popular sports in the USA and its popularity is only increasing. In 2017, the average MLB team was said to be worth $1.54 billion, an increase of 19% since 2016 [41]. Injuries to professional baseball players that result in placement on the disabled list result in major monetary loss to MLB franchises [4•]. Given these facts, it is not surprising that there is a significant amount of interest in evaluating what injuries occur most and how to prevent them.
Epidemiology
Over the years, there has been a steady increase in professional baseball injuries as first reported by Conte et al. [42]. Posner et al. [43] reported a 37% increase in injuries between the years on 2005 and 2008. This more recent study found the incidence of injury resulting in placement on the disabled list to be 3.61 per 1000 athlete exposures. This is rather high considering it does not include injuries that did not require an assignment to the disabled list, which is common for injuries resulting in less than 15 days out of play. At this level, injuries to pitchers continue to increase significantly more than other positions [43–45]. Posner et al. [43] found 34% higher injury rate among pitchers compared to fielders. Overall, upper extremity injuries accounted for 51.4% of all injuries. Lower extremity injuries were much more common in fielders than pitchers. Common lower extremity injuries include those to the hamstrings [46]. Dahm et al. [47] reported the knee injury rate across MiLB and MLB to be 1.2 per 1000 AEs. Conte et al. [4•] performed the most recent evaluation of MLB injury data and found that overall injury rates increased between 1998 and 2015. They found shoulder and elbow injuries to be the leading cause of lost participation time. Interestingly, the rate of elbow injuries increased while shoulder injuries decreased during the study period. Injuries involving the medial ulnar collateral ligament (MUCL) are of particular interest. Their incidence has been found to increase significantly, and it has been reported that between 25 and 33% of all MLB pitchers have had an MUCL reconstruction surgery at some point during their baseball careers [4•, 44, 45, 48]. Research has also been conducted to further characterize other clinically relevant injuries such as abdominal oblique injuries, lumbar spine injuries, and sliding-related injuries [49–51].
Prevention
Similar to that found in collegiate baseball, early season injuries are more common in professional baseball [43]. This attests to the importance of off-season fitness and gradual increase in early season workout intensity. There is again a limited amount of literature demonstrating proven injury preventing measures in professional baseball. With a knowledge of known risk factors for injury, one can reasonably predict strategies that will prove to be injury preventing. Wilk et al. [52] demonstrated that deficits in shoulder rotation and flexion were associated with increased risk of elbow injury in professional pitchers. In a subsequent study, Wilk et al. [53] found that decreased shoulder external rotation was predictive of shoulder injuries in pitchers. Similarly, Camp et al. [54] demonstrated increased rates of elbow injuries in pitchers who demonstrated decreased shoulder flexion and external rotation during a pre-season physical examination. Given this knowledge, many exercises such as the sleeper stretch and others have been developed to improve upper extremity flexibility and range of motion [38] (Figs. 1 and 2). Increased total cumulative work has been shown to increase risk of injury in youth baseball players, but this has not as reliably been demonstrated in professionals [9, 55].
In recent years, MLB pitchers have demonstrated gradually increasing mean fastball velocities from 90.9 in 2008 to 93.3 in 2017 [56]. Several recent articles have studied the potential causes of the rising elbow UCL tears in professional baseball [57•, 58, 59]. Chalmers et al. [57•] showed that peak velocity was an independent predictor of UCL reconstruction status. They also found that increased mean velocity was a statistically significant secondary predictor. It has been well documented that increased velocity and arm speed has a direct relationship to increase valgus torque on the UCL [60, 61]. Keller et al. [59] demonstrated that throwing a higher percentage of fastball (over 48%) was also a risk factor. Although the relationship between velocity and injury risk is well established, velocity is critical to the athletic success for most pitchers. Accordingly, asking them to decrease their throwing velocity is not likely a practical injury prevention strategy.
There have been several strength and conditioning programs that are designed for high school, college, and professional pitchers alike to increase their velocity. One of the most common and popular strategies in modern throwing regimens is utilization of weighted baseballs [62]. These programs have pitchers throwing balls that are under or over weighted compared to the normal 5-oz baseball. The balls range from 4 to 32 oz. Although this has been shown to increase velocity, there is concern that these programs could directly result in injury or that the increased velocity may place the pitcher at increased risk for injury. More studies are necessary to determine how these programs should be optimized in order to maximally improve performance without increasing the risk for injury.
Although injuries to the upper extremities are important and tend to garner the most attention in baseball, lower extremity injuries can also result in significant loss of participation time. In 2011 alone, 268 hamstring strains occurred in professional baseball, and these resulted in an average of 24 lost days of participation per injury [46]. Prevention of these injuries is important and the use of Nordic or eccentric hamstring exercises have been shown to decrease the incidence of hamstring injuries in professional soccer players [63] (Fig. 3). Seagrave et al. [64•] found that a strengthening program including these same eccentric hamstring exercises instituted in professional baseball resulted in a decreased incidence of hamstring injuries and less days missed due to injury in one organization.
Fig. 3.

Eccentric hamstring exercises have been shown to prevent hamstring injuries
An awareness of the risk of contact injuries in professional baseball is also important. These tend to effect fielders and catchers more than pitchers. Rules have been developed to help decrease the rate of these contact events. Ultimately, more research is needed to develop more proven preventative measures.
Conclusion
Baseball is a finesse sport that is ubiquitously popular among all age groups. Given its popularity, a large majority of our population has either played baseball or is a fan. Professional baseball is a multibillion-dollar business, and franchises have an understandably sizable interest in the health of their players. Injury prevention in youth baseball is largely aimed at avoiding overuse and this holds true up to the highest levels. Prevention of collisions and upper extremity stretching and range of motion exercises are thought to be useful. Although there is an increasing scientific interest into baseball injury epidemiology and prevention, more research is needed on this topic.
Compliance with Ethical Standards
Conflict of Interest
All authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Injuries in Overhead Athletes
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.Manager D. How many kids play baseball in the world? [Available from: https://www.dugoutmanager.com/how-many-kids-are-playing-baseball-in-the-world/.
- 2.Web HSB. Probability of playing college and professional baseball [Available from: http://www.hsbaseballweb.com/probability.htm.
- 3.Ozanian M. Forbes-MLB teams worth $36 billion as team values hit record $1.2 billion average [Available from: http://www.thesportsadvisorygroup.com/resource-library/business-of-sports/forbes-mlb-teams-worth-36-billion-as-team-values-hit-record-1-2-billion-average/.
- 4.Conte S, Camp CL, Dines JS. Injury trends in Major League Baseball over 18 seasons: 1998–2015. Am J Orthop (Belle Mead NJ) 2016;45(3):116–123. [PubMed] [Google Scholar]
- 5.Position statement for adolescent baseball pitchers 2013 [Available from: http://www.asmi.org/research.php?page=research§ion=positionStatement.
- 6.• Makhni EC, Morrow ZS, Luchetti TJ, Mishra-Kalyani PS, Gualtieri AP, Lee RW, et al. Arm pain in youth baseball players: a survey of healthy players. Am J Sports Med. 2015;43(1):41–6. Though guidelines and recommendations are in place to prevent youth overuse injuries, adherence to them remains an issue for players and coaches. A recent study by Makhni et al. found that 46% of youth respondents said they were encouraged on at least one occasion to keep playing despite having arm pain. This is clearly a problem, as throwing-related arm pain is indicative of possible injury, and management involves cessation of throwing. It is imperative that adults, including coaches and parents, act in the interest of the athlete and not pressure them into continuation of potentially destructive activity. 10.1177/0363546514555506. [DOI] [PubMed]
- 7.Fleisig GS, Andrews JR. Prevention of elbow injuries in youth baseball pitchers. Sports Health. 2012;4(5):419–424. doi: 10.1177/1941738112454828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang J, Mann BJ, Guettler JH, Dugas JR, Irrgang JJ, Fleisig GS, Albright JP. Risk-prone pitching activities and injuries in youth baseball: findings from a national sample. Am J Sports Med. 2014;42(6):1456–1463. doi: 10.1177/0363546514524699. [DOI] [PubMed] [Google Scholar]
- 9.Fleisig GS, Andrews JR, Cutter GR, Weber A, Loftice J, McMichael C, Hassell N, Lyman S. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39(2):253–257. doi: 10.1177/0363546510384224. [DOI] [PubMed] [Google Scholar]
- 10.Olsen SJ, 2nd, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34(6):905–912. doi: 10.1177/0363546505284188. [DOI] [PubMed] [Google Scholar]
- 11.Matthys SP, Vaeyens R, Coelho ESMJ, Lenoir M, Philippaerts R. The contribution of growth and maturation in the functional capacity and skill performance of male adolescent handball players. Int J Sports Med. 2012;33(7):543–549. doi: 10.1055/s-0031-1298000. [DOI] [PubMed] [Google Scholar]
- 12.Dun S, Loftice J, Fleisig GS, Kingsley D, Andrews JR. A biomechanical comparison of youth baseball pitches: is the curveball potentially harmful? Am J Sports Med. 2008;36(4):686–692. doi: 10.1177/0363546507310074. [DOI] [PubMed] [Google Scholar]
- 13.Nissen CW, Westwell M, Ounpuu S, Patel M, Solomito M, Tate J. A biomechanical comparison of the fastball and curveball in adolescent baseball pitchers. Am J Sports Med. 2009;37(8):1492–1498. doi: 10.1177/0363546509333264. [DOI] [PubMed] [Google Scholar]
- 14.• Oliver GD, Plummer H, Henning L, Saper M, Glimer G, Brambeck A, et al. Effects of a simulated game on upper extremity pitching mechanics and muscle activations among various pitch types in youth baseball pitchers. J Pediatr Orthop. 2017. Whether or not young athletes should throw breaking balls prior to skeletal maturity has been a controversial topic over the years. This recent biomechanical study in youth athletes throwing various breaking and non-breaking pitches demonstrated no significant difference in arm slot position or muscle activation in the pelvis, torso, and upper extremity. This lends support to the argument that throwing a breaking ball is no more dangerous than throwing other pitches. [DOI] [PubMed]
- 15.Bohne C, George SZ, Zeppieri G., Jr Knowledge of injury prevention and prevalence of risk factors for throwing injuries in a sample of youth baseball players. Int J Sports Phys Ther. 2015;10(4):464–475. [PMC free article] [PubMed] [Google Scholar]
- 16.Benjamin HJ, Briner WW., Jr Little league elbow. Clin J Sport Med. 2005;15(1):37–40. doi: 10.1097/00042752-200501000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Fleisig GS, Weber A, Hassell N, Andrews JR. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep. 2009;8(5):250–254. doi: 10.1249/JSR.0b013e3181b7ee5f. [DOI] [PubMed] [Google Scholar]
- 18.• Sakata J, Nakamura E, Suzuki T, Suzukawa M, Akaike A, Shimizu K, et al. Efficacy of a prevention program for medial elbow injuries in youth baseball players. Am J Sports Med. 2017:363546517738003. This prospective randomized trial of a unique stretching and strengthening protocol demonstrated a significant decrease in medial elbow injuries in adolescent baseball players. The exercises also improved dominant side total range of shoulder rotation, non-dominant side hip internal rotation, bilateral shoulder internal rotation deficit, dominant side lower trapezius muscle strength, and the thoracic kyphosis angle. This appears to be the first prospective study of its kind. The Yokohama Baseball-9, or similar exercises, could be incorporated into pre-game and pre-practice routines.
- 19.Marshall SW, Mueller FO, Kirby DP, Yang J. Evaluation of safety balls and faceguards for prevention of injuries in youth baseball. JAMA. 2003;289(5):568–574. doi: 10.1001/jama.289.5.568. [DOI] [PubMed] [Google Scholar]
- 20.Powell JW, Barber-Foss KD. Traumatic brain injury in high school athletes. JAMA. 1999;282(10):958–963. doi: 10.1001/jama.282.10.958. [DOI] [PubMed] [Google Scholar]
- 21.Lyman S, Fleisig GS. Baseball injuries. Med Sport Sci. 2005;49:9–30. doi: 10.1159/000085340. [DOI] [PubMed] [Google Scholar]
- 22.Janda DH, Bir C, Kedroske B. A comparison of standard vs. breakaway bases: an analysis of a preventative intervention for softball and baseball foot and ankle injuries. Foot Ankle Int. 2001;22(10):810–816. doi: 10.1177/107110070102201006. [DOI] [PubMed] [Google Scholar]
- 23.NFHS. National Federation of State High Schools Association Available from: www.nfhs.org.
- 24.Fleisig GS, Kingsley DS, Loftice JW, Dinnen KP, Ranganathan R, Dun S, Escamilla RF, Andrews JR. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am J Sports Med. 2006;34(3):423–430. doi: 10.1177/0363546505280431. [DOI] [PubMed] [Google Scholar]
- 25.Knowles SB, Marshall SW, Bowling JM, Loomis D, Millikan R, Yang J, Weaver NL, Kalsbeek W, Mueller FO. A prospective study of injury incidence among North Carolina high school athletes. Am J Epidemiol. 2006;164(12):1209–1221. doi: 10.1093/aje/kwj337. [DOI] [PubMed] [Google Scholar]
- 26.Krajnik S, Fogarty KJ, Yard EE, Comstock RD. Shoulder injuries in US high school baseball and softball athletes, 2005–2008. Pediatrics. 2010;125(3):497–501. doi: 10.1542/peds.2009-0961. [DOI] [PubMed] [Google Scholar]
- 27.Saper MG, Pierpoint LA, Liu W, Comstock RD, Polousky JD, Andrews JR. Epidemiology of shoulder and elbow injuries among United States high school baseball players: school years 2005-2006 Through 2014-2015. Am J Sports Med. 2017:363546517734172. [DOI] [PubMed]
- 28.Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med. 2004;32(5):1158–1164. doi: 10.1177/0363546503262166. [DOI] [PubMed] [Google Scholar]
- 29.Kerr ZY, Roos KG, Djoko A, Dompier TP, Marshall SW. Rankings of high school sports injury rates differ based on time loss assessments. Clin J Sport Med. 2017;27(6):548–551. doi: 10.1097/JSM.0000000000000405. [DOI] [PubMed] [Google Scholar]
- 30.Collins CL, Comstock RD. Epidemiological features of high school baseball injuries in the United States, 2005–2007. Pediatrics. 2008;121(6):1181–1187. doi: 10.1542/peds.2007-2572. [DOI] [PubMed] [Google Scholar]
- 31.Maron BJ, Gohman TE, Kyle SB, Estes NA, 3rd, Link MS. Clinical profile and spectrum of commotio cordis. JAMA. 2002;287(9):1142–1146. doi: 10.1001/jama.287.9.1142. [DOI] [PubMed] [Google Scholar]
- 32.Endo Y, Sakamoto M. Correlation of shoulder and elbow injuries with muscle tightness, core stability, and balance by longitudinal measurements in junior high school baseball players. J Phys Ther Sci. 2014;26(5):689–693. doi: 10.1589/jpts.26.689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McFarland EG, Wasik M. Epidemiology of collegiate baseball injuries. Clin J Sport Med. 1998;8(1):10–13. doi: 10.1097/00042752-199801000-00003. [DOI] [PubMed] [Google Scholar]
- 34.Centers for Disease C. Prevention. Sliding-associated injuries in college and professional baseball—1990–1991. MMWR Morb Mortal Wkly Rep. 1993;42(12): 223, 229–30. [PubMed]
- 35.Dick R, Sauers EL, Agel J, Keuter G, Marshall SW, McCarty K, McFarland E. Descriptive epidemiology of collegiate men's baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):183–193. [PMC free article] [PubMed] [Google Scholar]
- 36.Nicholls RL, Elliott BC, Miller K. Impact injuries in baseball: prevalence, aetiology and the role of equipment performance. Sports Med. 2004;34(1):17–25. doi: 10.2165/00007256-200434010-00003. [DOI] [PubMed] [Google Scholar]
- 37.Boden BP, Tacchetti R, Mueller FO. Catastrophic injuries in high school and college baseball players. Am J Sports Med. 2004;32(5):1189–1196. doi: 10.1177/0363546503262161. [DOI] [PubMed] [Google Scholar]
- 38.Wilk KE, Hooks TR, Macrina LC. The modified sleeper stretch and modified cross-body stretch to increase shoulder internal rotation range of motion in the overhead throwing athlete. J Orthop Sports Phys Ther. 2013;43(12):891–894. doi: 10.2519/jospt.2013.4990. [DOI] [PubMed] [Google Scholar]
- 39.Laudner KG, Sipes RC, Wilson JT. The acute effects of sleeper stretches on shoulder range of motion. J Athl Train. 2008;43(4):359–363. doi: 10.4085/1062-6050-43.4.359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McClure P, Balaicuis J, Heiland D, Broersma ME, Thorndike CK, Wood A. A randomized controlled comparison of stretching procedures for posterior shoulder tightness. J Orthop Sports Phys Ther. 2007;37(3):108–114. doi: 10.2519/jospt.2007.2337. [DOI] [PubMed] [Google Scholar]
- 41.Ozanian M. Baseball team values 2017 https://www.forbes.com/sites/mikeozanian/2017/04/11/baseball-team-values-2017/#5d11a8332451.
- 42.Conte S, Requa RK, Garrick JG. Disability days in major league baseball. Am J Sports Med. 2001;29(4):431–436. doi: 10.1177/03635465010290040801. [DOI] [PubMed] [Google Scholar]
- 43.Posner M, Cameron KL, Wolf JM, Belmont PJ, Jr, Owens BD. Epidemiology of Major League Baseball injuries. Am J Sports Med. 2011;39(8):1676–1680. doi: 10.1177/0363546511411700. [DOI] [PubMed] [Google Scholar]
- 44.Conte SA, Fleisig GS, Dines JS, Wilk KE, Aune KT, Patterson-Flynn N, ElAttrache N. Prevalence of ulnar collateral ligament surgery in professional baseball players. Am J Sports Med. 2015;43(7):1764–1769. doi: 10.1177/0363546515580792. [DOI] [PubMed] [Google Scholar]
- 45.Erickson BJ, Gupta AK, Harris JD, Bush-Joseph C, Bach BR, Abrams GD, San Juan AM, Cole BJ, Romeo AA. Rate of return to pitching and performance after Tommy John surgery in Major League Baseball pitchers. Am J Sports Med. 2014;42(3):536–543. doi: 10.1177/0363546513510890. [DOI] [PubMed] [Google Scholar]
- 46.Ahmad CS, Dick RW, Snell E, Kenney ND, Curriero FC, Pollack K, Albright JP, Mandelbaum BR. Major and minor league baseball hamstring injuries: epidemiologic findings from the Major League Baseball Injury Surveillance System. Am J Sports Med. 2014;42(6):1464–1470. doi: 10.1177/0363546514529083. [DOI] [PubMed] [Google Scholar]
- 47.Dahm DL, Curriero FC, Camp CL, Brophy RH, Leo T, Meister K, Paletta GA, Steubs JA, Mandelbaum BR, Pollack KM. Epidemiology and impact of knee injuries in major and minor league baseball players. Am J Orthop (Belle Mead NJ). 2016;45(3):E54–E62. [PubMed] [Google Scholar]
- 48.Erickson BJ, Chalmers PN, Bush-Joseph CA, Romeo AA. Predicting and preventing injury in Major League Baseball. Am J Orthop (Belle Mead NJ). 2016;45(3):152–156. [PubMed] [Google Scholar]
- 49.Camp CL, Conte S, Cohen SB, Thompson M, J DA, Nguyen JT, et al. Epidemiology and impact of abdominal oblique injuries in major and minor league baseball. Orthop J Sports Med. 2017;5(3):2325967117694025. doi: 10.1177/2325967117694025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Camp CL, Conti MS, Sgroi T, Cammisa FP, Dines JS. Epidemiology, treatment, and prevention of lumbar spine injuries in major league baseball players. Am J Orthop (Belle Mead NJ) 2016;45(3):137–143. [PubMed] [Google Scholar]
- 51.Camp CL, Curriero FC, Pollack KM, Mayer SW, Spiker AM, D'Angelo J, et al. The epidemiology and effect of sliding injuries in major and minor league baseball players. Am J Sports Med. 2017;45(10):2372–2378. doi: 10.1177/0363546517704835. [DOI] [PubMed] [Google Scholar]
- 52.Wilk KE, Macrina LC, Fleisig GS, Aune KT, Porterfield RA, Harker P, Evans TJ, Andrews JR. Deficits in glenohumeral passive range of motion increase risk of elbow injury in professional baseball pitchers: a prospective study. Am J Sports Med. 2014;42(9):2075–2081. doi: 10.1177/0363546514538391. [DOI] [PubMed] [Google Scholar]
- 53.Wilk KE, Macrina LC, Fleisig GS, Aune KT, Porterfield RA, Harker P, Evans TJ, Andrews JR. Deficits in glenohumeral passive range of motion increase risk of shoulder injury in professional baseball pitchers: a prospective study. Am J Sports Med. 2015;43(10):2379–2385. doi: 10.1177/0363546515594380. [DOI] [PubMed] [Google Scholar]
- 54.Camp CL, Zajac JM, Pearson DB, Sinatro AM, Spiker AM, Werner BC, Altchek DW, Coleman SH, Dines JS. Decreased shoulder external rotation and flexion are greater predictors of injury than internal rotation deficits: analysis of 132 pitcher-seasons in professional baseball. Arthroscopy. 2017;33(9):1629–1636. doi: 10.1016/j.arthro.2017.03.025. [DOI] [PubMed] [Google Scholar]
- 55.Karakolis T, Bhan S, Crotin RL. An inferential and descriptive statistical examination of the relationship between cumulative work metrics and injury in Major League Baseball pitchers. J Strength Cond Res. 2013;27(8):2113–2118. doi: 10.1519/JSC.0b013e3182785059. [DOI] [PubMed] [Google Scholar]
- 56.About All These Velocity Spikes | FanGraphs Baseball [Available from: https://www.fangraphs.com/blogs/about-all-these-velocity-spikes/.
- 57.Chalmers PN, Erickson BJ, Ball B, Romeo AA, Verma NN. Fastball pitch velocity helps predict ulnar collateral ligament reconstruction in major league baseball pitchers. Am J Sports Med. 2016;44(8):2130–2135. doi: 10.1177/0363546516634305. [DOI] [PubMed] [Google Scholar]
- 58.Whiteside D, Martini DN, Lepley AS, Zernicke RF, Goulet GC. Predictors of ulnar collateral ligament reconstruction in major league baseball pitchers. Am J Sports Med. 2016;44(9):2202–2209. doi: 10.1177/0363546516643812. [DOI] [PubMed] [Google Scholar]
- 59.Keller RA, Marshall NE, Guest JM, Okoroha KR, Jung EK, Moutzouros V. Major league baseball pitch velocity and pitch type associated with risk of ulnar collateral ligament injury. J Shoulder Elb Surg. 2016;25(4):671–675. doi: 10.1016/j.jse.2015.12.027. [DOI] [PubMed] [Google Scholar]
- 60.Anz AW, Bushnell BD, Griffin LP, Noonan TJ, Torry MR, Hawkins RJ. Correlation of torque and elbow injury in professional baseball pitchers. Am J Sports Med. 2010;38(7):1368–1374. doi: 10.1177/0363546510363402. [DOI] [PubMed] [Google Scholar]
- 61.Camp CL, Tubbs TG, Fleisig GS, Dines JS, Dines DM, Altchek DW, Dowling B. The relationship of throwing arm mechanics and elbow varus torque: within-subject variation for professional baseball pitchers across 82,000 throws. Am J Sports Med. 2017;45(13):3030–3035. doi: 10.1177/0363546517719047. [DOI] [PubMed] [Google Scholar]
- 62.Fleisig GS, Diffendaffer AZ, Aune KT, Ivey B, Laughlin WA. Biomechanical analysis of weighted-ball exercises for baseball pitchers. Sports Health. 2017;9(3):210–215. doi: 10.1177/1941738116679816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Petersen J, Thorborg K, Nielsen MB, Budtz-Jorgensen E, Holmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39(11):2296–2303. doi: 10.1177/0363546511419277. [DOI] [PubMed] [Google Scholar]
- 64.• Seagrave RA 3rd, Perez L, McQueeney S, Toby EB, Key V, Nelson JD. Preventive effects of eccentric training on acute hamstring muscle injury in professional baseball. Orthop J Sports Med. 2014;2(6):2325967114535351. This study demonstrated a decreased incidence of hamstring injuries in a single professional baseball franchise when eccentric or Nordic hamstring strengthening exercises were implemented. This led to decreased loss of participation time as well. 10.1177/2325967114535351. [DOI] [PMC free article] [PubMed]