

Abstract
Anorectal malformation are common congenital problems occurring in 1 in 5,000 births and have a spectrum of anatomical presentations, requiring individualized treatments for the newborn, sophisticated approaches to the definitive reconstruction, and management of long-term treatments and outcomes. Associated anomalies related to the cardiac, renal, gynecologic, orthopedic, spinal, and sacral systems impact care and prognosis. Long-term results are good provided there is an accurate anatomical reconstruction and a focus on maximizing of functional results.
Keywords: anorectal malformation, imperforate anus, cloaca, pediatric fecal incontinence
Anorectal malformations (ARMs) occur in approximately 1 out of every 5,000 births and are slightly more common in males, 1 2 with a 1% risk for a family to have a second child with an ARM. 3 4 A rectourethral fistula is most common in males and a rectovestibular fistula in females. Having no fistula at all is rare (5% of patients) and is associated with Down's syndrome. 5 Cloaca, in the past, was considered a rare defect, whereas rectovaginal fistula was reported commonly, but the converse is true, as cloacas comprise the third most common defect in females (after vestibular and perineal fistulas). A true congenital rectovaginal fistula is rare, occurring in less than 1% of cases. 6 An incorrect diagnosis in such a case leads to surgery in which only the rectal component is repaired, leaving the patient with a persistent urogenital sinus. 7
The Wingspread classification (1984), which described malformations as low, intermediate, and high, does not help predict the type of surgery required or the clinical outcome, and therefore, the Krickenbeck classification (2005) ( Table 1 ), which is based on precise anatomical abnormalities, is much more valuable. 8 While the complexity of the malformation plays a role in long-term results, data on reliable outcomes remain elusive. With consistent assessment of the sacrum and spine, the potential for continence can be better predicted (referred to as the ARM Continence Index). Patients must have a detailed clinical examination to accurately diagnose the malformation so that they can receive the correct treatment in the newborn period.
Table 1. Krickenbeck classification.
| Major clinical groups |
| Perineal (cutaneous) fistula |
| Rectourethral fistula |
| Prostatic |
| Bulbar |
| Rectovesical fistula |
| Vestibular fistula |
| Cloaca |
| ARM with no fistula |
| Anal stenosis |
| Rare variants |
| Pouch colon atresia/stenosis |
| Rectal atresia/stenosis |
| Rectovaginal fistula |
| H-type fistula |
| Others |
Abbreviation: ARM, anorectal malformation.
Anorectal malformations are not usually diagnosed on prenatal ultrasound, but markers of a cloacal malformation exist, including intrapelvic or abdominal cysts as well as hydronephrosis, 9 and sonographic markers of VACTERL (vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities) abnormalities (single kidney, hydronephrosis, absent radius, and absent sacrum) may alert the clinician to look more carefully for an ARM.
In the newborn, assessment to make an anatomical diagnosis and a review of associated anomalies are the key goals. 10 A careful perineal inspection gives clues to the type of malformation present. It is important to not make any decisions regarding the surgical management before 24 hours of life because significant intraluminal pressure is required for the meconium to be forced through a fistulous tract, which helps to establish the diagnosis. If meconium is seen exiting the perineal skin, a rectoperineal fistula is present. If there is meconium in the urine, a rectourethral fistula is present. Radiological evaluations done prior to 24 hours may be misleading, as the rectum will be incorrectly diagnosed as very high. If the neonate has signs of a rectoperineal fistula, primary surgery in the form of an anoplasty, without a diverting colostomy, can be performed then or in the first few months of age ( Fig. 1 ).
Fig. 1.
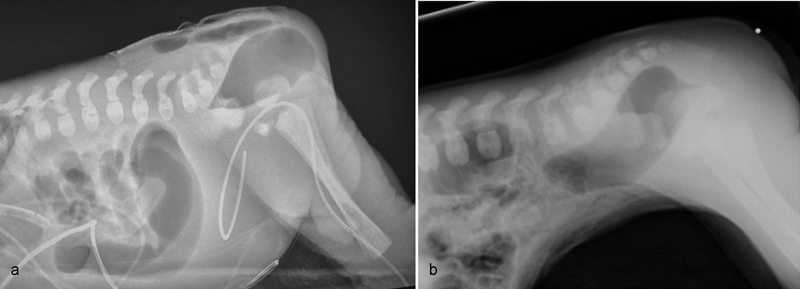
Cross-table lateral film in two newborns. ( a ) In a reachable rectum, a newborn anoplasty can be performed. ( b ) In a distant rectum, a colostomy is required.
During the first 24 hours of life, the neonate should receive intravenous fluids, antibiotics, and nasogastric decompression and be evaluated for associated defects, which include cardiac malformations, esophageal atresia, and renal anomalies. 10 The lumbar spine and the sacrum should be reviewed radiographically (X-ray and spinal ultrasound, magnetic resonance imaging [MRI] if needed) to look for spinal and sacral abnormalities. 11 12 Ultrasonography of the abdomen and pelvis will evaluate for hydronephrosis, and specifically in females, a hydrocolpos, which is a vagina dilated with urine and mucous. 13
Depending on the patient's overall condition and the experience of the surgeon, patients with perineal and vestibular fistulae can be treated with either a primary repair or dilation of the fistula and delayed repair, 14 or a colostomy can be performed at the same time as the repair.
After 24 hours, if there is no evidence of a fistula, a cross-table lateral radiograph with the patient in prone position can show air in the rectum located below the coccyx, in which case a posterior sagittal anorectoplasty (PSARP) can be performed, or rectal gas that does not extend beyond the coccyx, in which case a colostomy should be performed ( Fig. 1 ). The colostomy allows for a distal colostogram, a valuable study to define the specific anatomy and relationships of the rectum to the urinary tract ( Figs. 2 and 3 ). A PSARP can then be performed 2 to 3 months later. Rectourethral fistulae usually present with signs of meconium in the urine, and a colostomy in the newborn period should be performed. Then, after a high pressure distal colostogram, definitive reconstruction can be performed. Similarly, cloacal malformations are best managed with a colostomy and further imaging to clarify the anatomy done prior to repair. A vaginostomy is needed if a hydrocolpos is present.
Fig. 2.
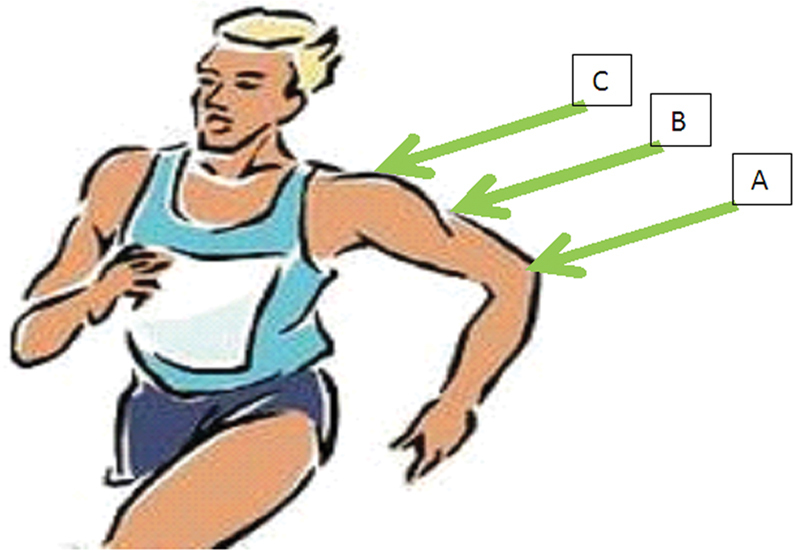
Male anomalies: ( A ) rectobulbar fistula, ( B ) rectoprostatic fistula, and ( C ) recto–bladder neck fistula based on the insertion of the distal rectum into the urethra, mapped like an “elbow.”
Fig. 3.
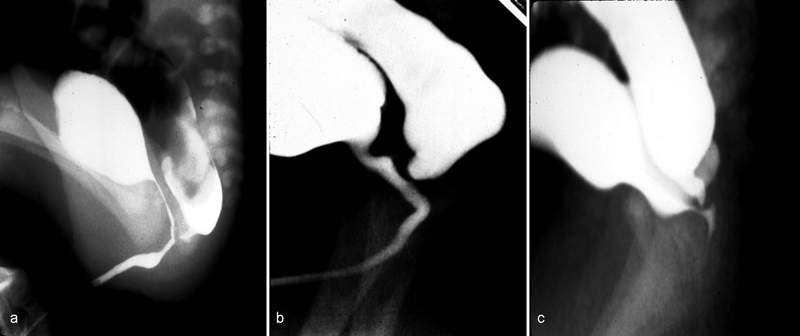
( a - c ) Distal colostogram demonstrating a rectobulbar fistula, done with adequate pressure.
Associated abnormalities are a source of major morbidity in patients with ARMs. While cardiac, esophageal, and some severe renal abnormalities may pose an immediate threat to life and may complicate anesthesia for these infants, it is the underlying spinal 15 16 17 and long-term urological abnormalities 18 19 that are the source of greatest morbidity and often are underrecognized. Missed tethered cord can have negative implications for bowel, bladder, and ambulatory function. Underlying renal and urological abnormalities pose a threat to long-term renal health.
Newborn Management
Fig. 4 depicts the initial management. Screening for associated malformations should be concluded within the first 24 hours, and then the child should be carefully reexamined to define the type of ARM.
Fig. 4.

Proximal sigmoid divided colostomy with mucous fistula.
Newborn Female
In a female, the following questions should be asked. How many orifices are present? If three are present, is the anal orifice correctly located within the muscle complex (defined by an area of hyperpigmentation)? Is the anal opening of adequate size (a Hegar size 12 at birth is normal)? Is there an adequate perineal body?
While it is vital to not miss an ARM, many babies are incorrectly diagnosed with an “anteriorly misplaced anus” that are in fact normal, the anal opening is properly centered in the sphincters and no surgery is needed. In female patients, one needs to decide if one is dealing with a perineal fistula, a vestibular fistula, a cloaca, a no fistula defect, or with some rare or complex malformation. In a male, the observation records whether there is a perineal fistula, no fistula, or, most commonly, a rectourethral fistula. Decisions regarding surgical management in the newborn period are led by this initial assessment.
Newborns (male or female) with a perineal fistula or females with a vestibular fistula, provided they have no severe comorbidities, can be managed with an anoplasty or PSARP, respectively, without the need for a colostomy. If there is a single perineal orifice, the diagnosis of a cloaca should be made, and treatment is with a divided proximal sigmoid colostomy. Due to the high incidence of associated urological malformations, an evaluation including abdominal and pelvic ultrasonography to look for hydronephrosis and hydrocolpos is mandatory. If hydrocolpos is present, it should be adequately drained at the same time as the colostomy formation, which in almost all cases helps to resolve the hydronephrosis.
Newborn Male
In male patients, the key to successful management is a thorough examination of the perineum at 24 hours. If an open fistula or other signs of meconium on the perineum is present, a diagnosis of rectoperineal fistula is made, and a primary anoplasty in the newborn period can be performed. The anterior rectal dissection must avoid injuring the urethra and should always be performed with a urethral catheter in place. Evidence of meconium in the urine confirms the diagnosis of a rectourethral fistula, and the patient requires a colostomy.
Newborns of either gender rarely may have a blind-ending rectum and no fistula, which occurs in less than 5% of infants and is associated with Down's syndrome. In such a case, a cross-table film is useful to decide whether to operate primarily through a posterior sagittal incision or to perform a colostomy ( Fig. 1 ). The use of a colostomy in this situation is always a reasonable option, especially in the setting of associated abnormalities.
Performing the definitive repair early in life allows for less time with a stoma, easier anal dilations (because the infant is smaller), and the possibility that placing the rectum in the right location early may lead to improved acquired sensation. 20 The potential advantages of early definitive surgery without a protective stoma 21 22 23 24 must be weighed against the possible perineal complications of not being diverted, which may have negative long-term implications on the child's continence potential. 5 The colostomy also allows for a distal colostogram, which, when performed correctly, gives the surgeon vital information as to where the rectum will be found ( Fig. 2 ) and helps the surgeon safely perform the operation without injuring other structures and by using the best approach, either posterior sagittal alone or laparoscopic-assisted. The colostogram is performed under pressure and must overcome the muscle tone of the pelvic floor ( Fig. 3 ). Any colostogram in which the rectum is flattened along the pubococcygeal line has not been performed with enough pressure and will not show the accurate anatomical information.
If a colostomy is required as the initial surgical procedure, a divided proximal sigmoid colostomy is ideal. It should be completely diverting, provide both bowel decompression and protection for the final reconstruction, and have a mucous fistula that can be used for the distal colostogram ( Fig. 4 ).
Fig. 5.

Posterior sagittal incision revealing distal rectum, which must now be dissected off of the posterior urethra.
Fig. 6.
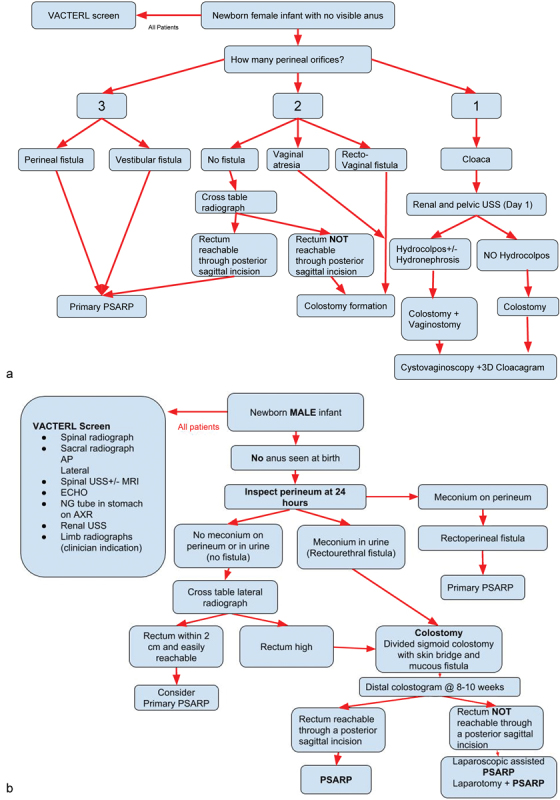
Flow diagram. ( a ) Female anorectal malformations (ARMs). ( b ) Male ARM.
The upper sigmoid divided colostomy has clear advantages over a right or transverse colostomy. The length of the defunctionalized colon needs to be a relatively short to prevent urine absorption and acidosis through a rectourethral fistula, but long enough to allow the distal rectum to be pulled through. The ideal location is just at the point where the proximal sigmoid comes off the left retroperitoneum. Loop colostomies are disadvantageous as they can permit the passage of stool from the proximal stoma into the distal bowel, potentially leading to urinary tract infections, distal rectal pouch dilation, stool impaction, and more severe constipation later in life. Also, colostomy prolapse is more frequent in loop stomas. The most common error in colostomy formation is when it is opened too distally in the rectosigmoid and therefore interferes with mobilization of the rectum during the reconstruction.
The proximal colon is unlikely to prolapse when placed in the correct part of the colon as it is tethered by the left retroperitoneum. The distal colon still has a prolapse potential, which can be reduced by making the mucous fistula small and flat ( Fig. 4 ). In cloacas, it is critical to perform the divided sigmoid colostomy with as much redundant distal rectosigmoid colon as possible to allow for the subsequent pull-through and possible vaginal replacement if needed ( Fig. 4 ).
Prior to the colostomy in a newborn with a cloacal malformation, an ultrasound of the pelvis looking for hydrocolpos is required, which, if present, should be drained at the same time as the colostomy procedure with a pigtail catheter. Because a significant number of these patients have two hemivaginas, the surgeon must be certain that both hemivaginas are drained, and in such a case, a vaginovaginostomy in the vaginal septum through an incision in the dome can be created to drain both hemivaginas with one catheter. At times, the hydrocolpos is so large that it may produce respiratory distress and reach above the umbilicus. In such a case, it is preferable to perform a formal cutaneous vaginostomy that does not require a tube. The hydrocolpos compresses the trigone and therefore the distal ureters and this causes hydronephrosis. Effective drainage of the hydrocolpos allows for decompression of the urological system in most instances. A vesicostomy would not solve this problem. Perineal drainage, if reliable and reproducible, can also be performed. Rarely, if the common channel is very narrow and does not allow the bladder to drain, the neonate may require an additional vesicostomy or suprapubic cystostomy to decompress the bladder. The timing of the definitive repair is largely dependent on the child's general condition and associated abnormalities, but usually can be performed sometime between 3 and 12 months of age.
Definitive Repair
Posterior Sagittal Anorectoplasty
To perform the anorectal reconstruction, 25 the patient is placed in the prone position with the pelvis raised and the operating table in Trendelenburg's position. An electrical stimulator is used to map the sphincter before and during the operation. The length of the incision varies with how much exposure is needed to safely repair the specific malformation. Thus, a perineal fistula requires a minimal posterior sagittal incision (2 cm), whereas higher defects may require a full posterior sagittal incision that runs from the lower sacrum toward the base of the scrotum in the male or to the single perineal orifice in a female with a cloacal malformation. The incision includes the skin and subcutaneous tissue and separates the parasagittal fibers, muscle complex, and levator muscles in the midline. In lower defects (perineal and vestibular), the incision separates only the parasagittal fibers and the muscle complex in the midline. The levator muscle is not seen. Once the sphincter mechanism has been divided, the key step is the separation of the rectum from the urogenital structures. In perineal and vestibular fistulas, the rectum is immediately visible and multiple silk sutures are placed on the rectum to apply uniform traction to facilitate the safe separation from adjacent structures. Even in these more minor malformations, care must be taken to separate the rectum completely from its anterior attachments to either the urethra or vagina. Failure to do this will leave the anoplasty under tension and is the cause of many failed repairs. 7 Once fully mobilized in the correct plane, the rectum should be placed in the middle of the muscle complex, which is accurately mapped with an electrical stimulator. Interrupted long-term absorbable sutures are used to repair the perineal body. The posterior edge of the muscle complex is tacked to the posterior rectal wall. Thus, the posterior muscle complex surrounds the rectum and helps prevent rectal prolapse. 26 The parasagittal fibers are then reapproximated, the posterior incision is closed, and an anoplasty is performed to complete the repair.
The repair of a rectourethral fistula in a male has many similar principles but several fundamental differences. A urinary catheter must be inserted at the start of the procedure, and a Coude tip catheter helps to prevent inadvertent insertion into the rectal fistula. First, the rectum is located through the posterior sagittal incision. Prior to starting the procedure, the surgeon should know exactly where to expect to find the rectum. The importance, therefore, of an accurate distal colostogram to avoid injuries to adjacent structures cannot be overstated. 27 In the case of a bulbar urethral fistula, the rectum will lie just beneath the levator muscles, and in the case of a prostatic urethral fistula ( Fig. 2 ), it will lie much higher, under the coccyx. Once the parasagittal fibers, muscle complex, and levators are opened, the surgeon should attempt to find the rectum, and once it is confidently identified, it should be mobilized laterally and posteriorly. Then, with silk traction sutures in place, the rectum should be opened in the midline. Multiple stitches are then placed on the edges of the rectum as it is opened in an inferior direction, precisely in the midline. The fistula is then identified, and a line of silk sutures placed proximal to the fistula. The common wall between the rectum and the urethra is then carefully separated. This initial 1- to 2-mm separation should be performed in a submucosal rectal plane to prevent a urethral injury. The dissection is facilitated by completing the lateral dissection of the rectum, prior to attempting the anterior plane. Once the rectum is completely separated from the urethra, the site of the fistula can be closed with long-term absorbable sutures, and the rectum can be further mobilized to allow for a tension-free anoplasty.
Laparoscopic-Assisted Anorectoplasty
Approximately 90% of defects in males can be repaired through a posterior sagittal approach only. It is only in rectourethral (bladder neck) fistulas or high prostatic fistulas that one has to approach the rectum through the abdominal cavity either with laparoscopy 28 29 30 or laparotomy. The repair is always performed with a urethral catheter in place. In patients with bladder neck fistulae, the rectum is separated from the urethra through the abdomen laparoscopically (or open) and the fistula is closed. In these defects, the rectum enters the urethra at a right angle. Once the rectum is freed and sufficient length is achieved, a limited posterior sagittal incision can be used to split the muscle complex accurately. This can be performed in the supine position with the legs lifted up. The levator muscles are opened sufficiently and the rectum is passed through the pelvic floor and repaired in the standard manner, with tacking of the posterior rectal wall to the posterior edge of the muscle complex. In lower anomalies such as rectourethral (bulbar) fistulae, there is a long common wall between the rectum and urethra that makes the dissection from an abdominal approach extremely difficult, and a posterior sagittal only approach is easier and safer.
Imperforate Anus without Fistula
In these cases, the blind end of the rectum is usually located at the level of the bulbar urethra and is easily reachable from the posterior sagittal approach. The rectum must be carefully separated from the urethra because the two structures share a common wall, even though no fistula is present. The rest of the repair is performed like that for the rectourethral fistula defect.
Rectal Atresia and Rectal Stenosis
The approach to these malformations is also posterior sagittal. The upper rectal pouch is opened and the distal anal canal is split in the posterior midline. An end-to-end anastomosis is performed under direct visualization leaving the dentate line intact. 31 If a presacral mass (which occurs in 30% of these patients) is identified on preoperative MRI, 32 it is removed with presacral dissection at the same time unless it is connected to the dural elements, in which case the neurosurgical part is performed separately.
Cloacal Malformations
The definitive repair of cloacal malformations has its own spectrum of complexity. 33 First, a cystoscopy, vaginoscopy, and cloacagram should be performed during a separate anesthetic after the newborn period; this is key for surgical planning. At this examination, the length of the common channel and the length of the urethra from the common channel to the bladder neck are determined, as well as the genital anatomy, the presence of a vaginal septum, the numbers and patency of cervices, and size and height of the vagina. The position of the rectum must be carefully checked to see whether it can be reached from a posterior sagittal incision or will require a laparotomy or laparoscopy.
The repair of cloacal malformations with a less than 3-cm common channel can be performed through a posterior sagittal approach alone, usually using a total urogenital mobilization technique. Long common-channel cloacas are less predictable and commonly involve nuances in anatomical variation. They frequently require vaginal replacement and reconstructive urological expertise and are ideally treated in a specialized center.
Cloacas with a Common Channel Shorter Than 3 cm
The incision extends from the lower sacrum down to the single perineal orifice, and the sphincter mechanism is separated in the midline. The first structure usually found is the rectum; however, many anatomical variations may be encountered. The rectum is opened in the midline, silk sutures are placed along the edges of the posterior rectal wall, and the rectum is mobilized. The entire common channel is exposed, which allows confirmation of its length under direct vision. Separation of the rectum from the vagina is accomplished in the same way as that for a rectovestibular fistula.
Once the rectum has been completely separated from the vagina, the total urogenital mobilization brings the vagina and urethra to the perineum as a unit. The urogenital sinus is then divided just below the clitoris, and the anterior aspect is dissected full thickness from the pubic symphysis. At the upper edge of the pubis, fibrous, avascular bands called the suspensory ligaments of the urethra are divided while applying traction to the urogenital sinus sutures, gaining 2 to 3 cm of length. Lateral and posterior dissection of the urogenital sinus will provide an additional 0.5 to 1.0 cm of length, allowing for a complete urogenital mobilization. The common channel is then divided up to the urethral orifice, which creates two lateral flaps that become the new labia. Both the urethral meatus and the vaginal introitus can then be anastomosed to the perineum in the appropriate positions. The urethra is sutured to the mucosal edge below the clitoris, and the vaginal edges are sutured to the skin. The limits of the rectal sphincter are electrically determined, and the perineal body is reconstructed, bringing together the anterior limits of the sphincter, with the rectum placed within the margins of the sphincter.
Cloacas with a Common Channel Longer Than 3 cm
When endoscopy shows that the patient has a long common channel, the surgeon must be prepared to face a significant technical challenge. The patient is prepped so that the entire lower body is accessible because it is likely that the patient will require a laparotomy after initial exploration by the posterior sagittal approach. The principles of this repair and the decision-making based on the anatomy are extremely important, and these cases should be repaired in a pediatric colorectal center with collaborative support from reconstructive urology and gynecology. The decision to perform a total urogenital mobilization on a patient with a common channel greater than 3 cm must be carefully weighed, and should be based on the length of the urethra and on the likelihood of getting the urethra to the perineum. If the urethra (meaning the distance from the urethral orifice to the bladder neck) is short (<1.5 cm), then a total urogenital mobilization should not be attempted, as the urethra will not be long enough to provide any sort of urinary continence. With a total urogenital mobilization, the anterior urethra is dissected, and if at that point the surgeon realizes that the urogenital tracts must be separated, both the anterior and posterior urethra will have been mobilized, and the chances of housing a long-term functional urethra with this sort of dissection is low. Thus, in such a situation, the surgeon should instead leave the common channel intact and separate the vagina from the common channel, and then close this vaginourethal connection. Thus, the common channel becomes the urethra. The vagina is then mobilized as a separate unit.
To start the case, the separates the muscle complex and levators, and the rectum and vagina are identified and mobilized. The common channel is left untouched. If the rectum is found from this approach, it should be mobilized free from the vagina. If no rectum is identified but the vagina is found, then the separation of the urogenital tract should be started in the posterior sagittal position as this will greatly facilitate this separation once the surgeon is in the abdomen dissecting from above. To complete this maneuver, a midline laparotomy is recommended. If the ureters enter near the intended dissection, the bladder should be opened in the midline and ureteral catheters should be placed to protect them. The ureters run through the common wall between the vagina and bladder, and the ureteral stents allow for their identification during the difficult dissection of vaginas from the bladder neck. Once separated, the posterior common channel (in the area of the bladder neck) is repaired.
There are certain circumstances in which the mobilized urogenital complex in a total urogenital mobilization can be delivered up into the abdomen, and this allows for enough dissection to get it to reach. The decision on whether the urogenital complex should be mobilized or separated is ideally made prior to beginning of the total urogenital mobilization.
The presence of a common channel longer than 5 cm means that the total urogenital mobilization from below will definitely not be enough to repair the malformation. Therefore, in this scenario, it is again advisable to leave the common channel intact for use as the urethra and separate the vagina from it. The common channel will in most cases eventually be used for intermittent catheterization, but some patients will be able to spontaneously void.
Vaginal Procedures
In many patients, the vagina cannot be mobilized sufficiently in order for it to reach the perineum, and specific maneuvers are required to deliver an intact genital tract to the perineum. The choice of how to do this is based on the patient's anatomical findings. The vaginal switch and vaginal replacement with the rectum, colon, or small bowel all need to be within the repertoire of the team attempting to repair a patient with a complex malformation. 33
Postoperative Management and Colostomy Closure
Postoperatively, most patients have an uneventful course. Pain control is generally easy for the posterior sagittal incision and harder for those who have undergone a laparotomy. After cloaca repair, with a total urogenital mobilization, the urinary catheter remains for 14 to 28 days postoperatively until the perineum is no longer swollen, and the patient can be recatheterized, if necessary. In very complex malformations, as with a bladder neck or urethral reconstruction, a suprapubic tube or vesicostomy is advised. A silicon circle stent through the urethral repair and exiting the lower abdomen also helps. The two ends of the stent are then tied together to prevent dislodgement; it can be left in for up to 3 months and does not cause bladder spasms like other indwelling catheters with a balloon. The circle stent is generally removed after approximately 6 to 8 weeks when a cystoscopy is performed to check healing of the urethral reconstruction. At this point, an assessment for the need for intermittent catheterization is made. In male patients with repaired rectourethral fistulae, the urinary catheter is left for 7 days. If the catheter becomes dislodged, the patient often can void without difficulty and does not require replacement of the catheter. Most patients are discharged 2 days after posterior sagittal repair, and after 3 to 5 days if laparoscopy or laparotomy was needed if they have a diverting colostomy.
Anal dilatations are started 2 weeks after the repair to avoid a skin-level stricture with a dilator that fits easily into the anus. Dilations are performed twice daily by the parents at home, and the size of the dilator is increased weekly until the rectum reaches the desired size, based on the patient's age ( Table 2 ). Once this desired size is reached, the colostomy can be closed. The dilations can be tapered once there is no longer resistance with insertion of the final dilator, over the subsequent 3 to 4 months. Significant anal strictures occur in cases in which the blood supply of the distal rectum is insufficient, or when the anoplasty is performed under tension. Skin level (1–2 mm) strictures occur in some cases that do not undergo recommended dilations.
Table 2. Size of the dilator according to age.
| Age | Size of the Hegar dilator |
|---|---|
| 1–4 mo | 12 |
| 4–12 mo | 13 |
| 8–12 mo | 14 |
| 1–3 y | 15 |
| 3–12 y | 16 |
| >12 y | 17 |
After the colostomy is closed, the patient may have multiple bowel movements and can develop perineal excoriation. A constipating diet may be helpful in the treatment of this problem. After several weeks though, the number of bowel movements decreases, and a majority of patients will develop constipation and usually need laxatives. After a few months, the patient develops a more consistent pattern of bowel movements. A good prognosis can usually be predicted in a patient who has one to three discreet, well-formed bowel movements per day, remains clean between bowel movements, and shows evidence of feeling or pushing during bowel movements. This type of patient can usually be toilet-trained. A patient with multiple bowel movements or one who passes stool constantly without showing any signs of sensation or pushing usually has a poor functional prognosis. Of course, the quality of the patient's spine and sacrum factor into this prediction.
Patients with cloacal repairs should have a cystoscopy at the time of their colostomy closure and their ability to spontaneously void needs to be closely monitored. Approximately 20% of patients with a cloacal malformation and a common channel shorter than 3 cm require intermittent catheterization to empty their bladder. Patients with common channels longer than 3 cm require intermittent catheterization 80% of the time. 33 A kidney and bladder ultrasound can assess whether the patient is capable of spontaneous bladder emptying, and this should be performed 2 to 3 weeks after the catheter is removed and should be repeated every several months. If the patient cannot pass urine or does not empty the bladder satisfactorily, intermittent catheterization will need to be started. “Good voiding” without confirmation of bladder emptying or the absence of urinary tract infections is not enough to assure the clinician that the kidneys are safe. Good bladder emptying confirmed by ultrasound, absence of hydronephrosis, and confirmation of good renal function (glomerular filtration rate and cystatin C) are key factors to follow, ideally in collaboration with pediatric urology. 34 35
Most patients with a cloaca have a large flaccid bladder that does not empty completely and they usually have a competent bladder neck. This combination makes them ideal candidates for intermittent catheterization, which can keep them completely dry between catheterizations. Exceptions do exist, which should be managed on an individual basis, and these may ultimately require bladder neck closure/tightening and continent urinary diversion.
Fecal Continence after Repair of an Anorectal Malformation
Fecal continence depends on the following three factors:
Voluntary muscle structures : the levators, muscle complex, and parasagittal fibers in patients with ARMs have different degrees of hypodevelopment, affecting voluntary bowel control.
Anorectal sensation : the voluntary muscles can be used only when the patient feels that it is necessary to use them, and this exquisite sensation in normal individuals resides in the anal canal. Except for patients with rectal atresia and stenosis, patients with ARMs are born without an anal canal, and therefore sensation does not exist or is rudimentary. Distention of the rectum, however, can be felt in many of these patients, provided the rectum has been located accurately within the muscle structures. This sensation (proprioception) appears to be felt when there is a stretching of the muscles. The most important clinical implication of this is that liquid or soft stool cannot be detected well. Thus, to achieve some degree of sensation and bowel control, the patient must be able to (or helped to) form solid stool.
Bowel motility : the main factor that initiates emptying of the rectosigmoid is an involuntary peristaltic contraction that is helped by a Valsalva maneuver. Most patients with an ARM have a disturbance of this mechanism. Patients who have undergone a PSARP or any other type of sacroperineal approach, in which the most distal part of the bowel was preserved often have an over efficient rectal reservoir (megarectum), the main clinical manifestation of this is constipation, which seems to be more severe in patients with lower defects. 36 The dilated rectosigmoid has normal ganglion cells so the constipation is not due to Hirschsprung disease, but behaves like it is hypomotility. The overflow fecal incontinence based on rectosigmoid constipation in patients with good potential for bowel control can be managed with an appropriate dose of stimulant laxatives. Those with a poor sacrum, poor muscles, and thus with minimal potential for bowel control are treated with a daily enema. 5 Those patients treated with older techniques in which the most distal part of the bowel was resected (abdominoperineal pull-through) 37 have no rectal reservoir and, depending on the amount of colon resected, may have loose stools. In these cases, bowel management consisting of a daily enema, a constipating diet, and medications to slow down the colonic motility may be needed.
Long-Term Outcomes
There appear to be three factors that affect the outcomes in these patients. (1) The type of malformation, (2) sacral development or lack thereof as suggested by the sacral ratio, and (3) spinal abnormalities all have an influence of the potential for bowel control. The interaction between these three (the ARM continence index) and their individual contribution is the subject of ongoing prospective research.
Cloacal malformations represent their own spectrum of defects and should be subclassified on the basis of potential for both bowel and urinary control, as well as gynecological function. 38 The length of the common channel seems to be the most important prognostic factor, as is the ultimate length of the urethra after repair, and as for all ARM patients, the status of the sacrum and the spine.
Complications
There are several complications related to the operative repair of ARMs. Wound infection, dehiscence, and strictures are all initial postoperative problems. 39 Many complications are related to excessive tension or inadequate blood supply of mobilized structures. Mislocation of the anoplasty outside of the sphincter complex and injury to adjacent structures such as the vas deferens, seminal vesicles, ecoptic ureters, or urethra are also seen. Constipation is the most common functional disorder observed in patients who undergo a PSARP, occurring most frequently in those with the best prognosis for bowel control. 36 Patients with a poor prognosis, such as those with bladder neck fistula, conversely, have a low incidence of constipation and a high rate of incontinence. 5
Some patients develop a megarectum for various reasons related to inherent ectasia, type of or time with colonic diversion, or inadequate cleaning of the distal colon at the time of colostomy formation. These patients require proactive, aggressive treatment of constipation after colostomy closure to avoid future problems. Rectal prolapse occurs on occasion, is more prevalent in higher malformations with poor sphincters, and is worsened by postoperative constipation. 26 Finally, transient femoral nerve palsy can occur as a consequence of excessive pressure on the groin while in the prone position, a problem which can be avoided by adequate cushioning.
Specific to cloacal repairs, urethrovaginal fistulas had been the most common and feared complication prior to the introduction of the total urogenital mobilization technique. 33 In cases in which vaginal mobilization and separation from the neourethra result in opposing suture lines, 90-degree rotation of the vagina can decrease the incidence of a postoperative fistula. These suture lines can be protected further with use of a vascularized ischiorectal fat pad, similar to the technique described to protect suture lines of other types in complex repairs. 40 Fibrosis and stenosis of the vagina can develop and are caused by ischemia and excess tension. 41 Many patients with ARMs have stooling issues for which a comprehensive bowel program is required to achieve the best results. 42
References
- 1.Stephens F D, Smith E eds. Chicago, IL: Year Book Medical; 1971. Incidence, frequency of types, etiology. In: Anorectal Malformations in Children; pp. 160–171. [Google Scholar]
- 2.Santulli T V. The treatment of imperforate anus and associated fistulas. Surg Gynecol Obstet. 1952;95(05):601–614. [PubMed] [Google Scholar]
- 3.Falcone R A, Jr, Levitt M A, Peña A, Bates M.Increased heritability of certain types of anorectal malformations J Pediatr Surg 20074201124–127., discussion 127–128 [DOI] [PubMed] [Google Scholar]
- 4.Mundt E, Bates M D. Genetics of Hirschsprung disease and anorectal malformations. Semin Pediatr Surg. 2010;19(02):107–117. doi: 10.1053/j.sempedsurg.2009.11.015. [DOI] [PubMed] [Google Scholar]
- 5.Levitt M A, Peña A. Anorectal malformations. Orphanet J Rare Dis. 2007;2:33. doi: 10.1186/1750-1172-2-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosen N G, Hong A R, Soffer S Z, Rodriguez G, Peña A.Rectovaginal fistula: a common diagnostic error with significant consequences in girls with anorectal malformations J Pediatr Surg 20023707961–965., discussion 961–965 [DOI] [PubMed] [Google Scholar]
- 7.Levitt M A, Peña A. New York, NY: Humana Press; 2008. Reoperative surgery for anorectal malformations. IN: Reoperative Pediatric Surgery; pp. 311–326. [Google Scholar]
- 8.Holschneider A, Hutson J, Peña A et al. Preliminary report on the International Conference for the Development of Standards for the Treatment of Anorectal Malformations. J Pediatr Surg. 2005;40(10):1521–1526. doi: 10.1016/j.jpedsurg.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 9.Livingston J, Elicevik M, Crombleholme T, Peña A, Levitt M. Prenatal diagnosis of persistent cloaca: A 10 year review. Am J Obstet Gynecol. 2006;195(06):S63. doi: 10.7863/jum.2012.31.3.403. [DOI] [PubMed] [Google Scholar]
- 10.Shaul D B, Harrison E A. Classification of anorectal malformations--initial approach, diagnostic tests, and colostomy. Semin Pediatr Surg. 1997;6(04):187–195. [PubMed] [Google Scholar]
- 11.Bui C J, Tubbs R S, Oakes W J. Tethered cord syndrome in children: a review. Neurosurg Focus. 2007;23(02):E2. doi: 10.3171/foc.2007.23.2.2. [DOI] [PubMed] [Google Scholar]
- 12.Daszkiewicz P, Barszcz S, Roszkowski M, Maryniak A. Tethered cord syndrome in children - impact of surgical treatment on functional neurological and urological outcome. Neurol Neurochir Pol. 2007;41(05):427–435. [PubMed] [Google Scholar]
- 13.Levitt M A, Peña A. Pitfalls in the management of newborn cloacas. Pediatr Surg Int. 2005;21(04):264–269. doi: 10.1007/s00383-005-1380-2. [DOI] [PubMed] [Google Scholar]
- 14.Upadhyaya V D, Gopal S C, Gupta D K, Gangopadhyaya A N, Sharma S P, Kumar V. Single stage repair of anovestibular fistula in neonate. Pediatr Surg Int. 2007;23(08):737–740. doi: 10.1007/s00383-007-1965-z. [DOI] [PubMed] [Google Scholar]
- 15.Selden N R.Occult tethered cord syndrome: the case for surgery J Neurosurg 2006104(5, Suppl):302–304. [DOI] [PubMed] [Google Scholar]
- 16.Drake J M.Occult tethered cord syndrome: not an indication for surgery J Neurosurg 2006104(5, Suppl):305–308. [DOI] [PubMed] [Google Scholar]
- 17.Kuo M-F, Tsai Y, Hsu W-M, Chen R-S, Tu Y-K, Wang H-S.Tethered spinal cord and VACTERL association J Neurosurg 2007106(3, Suppl):201–204. [DOI] [PubMed] [Google Scholar]
- 18.Belman A B, King L R. Urinary tract abnormalities associated with imperforate anus. J Urol. 1972;108(05):823–824. doi: 10.1016/s0022-5347(17)60879-6. [DOI] [PubMed] [Google Scholar]
- 19.Hoekstra W J, Scholtmeijer R J, Molenaar J C, Schreeve R H, Schroeder F H. Urogenital tract abnormalities associated with congenital anorectal anomalies. J Urol. 1983;130(05):962–963. doi: 10.1016/s0022-5347(17)51597-9. [DOI] [PubMed] [Google Scholar]
- 20.Freeman N V, Burge D M, Soar J S, Sedgwick E M. Anal evoked potentials. Z Kinderchir. 1980;31:22–30. [Google Scholar]
- 21.Menon P, Rao K L. Primary anorectoplasty in females with common anorectal malformations without colostomy. J Pediatr Surg. 2007;42(06):1103–1106. doi: 10.1016/j.jpedsurg.2007.01.056. [DOI] [PubMed] [Google Scholar]
- 22.Albanese C T, Jennings R W, Lopoo J B, Bratton B J, Harrison M R. One-stage correction of high imperforate anus in the male neonate. J Pediatr Surg. 1999;34(05):834–836. doi: 10.1016/s0022-3468(99)90382-2. [DOI] [PubMed] [Google Scholar]
- 23.Moore T C. Advantages of performing the sagittal anoplasty operation for imperforate anus at birth. J Pediatr Surg. 1990;25(02):276–277. doi: 10.1016/0022-3468(90)90440-k. [DOI] [PubMed] [Google Scholar]
- 24.Vick L R, Gosche J R, Boulanger S C, Islam S. Primary laparoscopic repair of high imperforate anus in neonatal males. J Pediatr Surg. 2007;42(11):1877–1881. doi: 10.1016/j.jpedsurg.2007.07.014. [DOI] [PubMed] [Google Scholar]
- 25.Peña A, Devries P A. Posterior sagittal anorectoplasty: important technical considerations and new applications. J Pediatr Surg. 1982;17(06):796–811. doi: 10.1016/s0022-3468(82)80448-x. [DOI] [PubMed] [Google Scholar]
- 26.Belizon A, Levitt M, Shoshany G, Rodriguez G, Peña A. Rectal prolapse following posterior sagittal anorectoplasty for anorectal malformations. J Pediatr Surg. 2005;40(01):192–196. doi: 10.1016/j.jpedsurg.2004.09.035. [DOI] [PubMed] [Google Scholar]
- 27.Hong A R, Acuña M F, Peña A, Chaves L, Rodriguez G. Urologic injuries associated with repair of anorectal malformations in male patients. J Pediatr Surg. 2002;37(03):339–344. doi: 10.1053/jpsu.2002.30810. [DOI] [PubMed] [Google Scholar]
- 28.Georgeson K E, Inge T H, Albanese C T.Laparoscopically assisted anorectal pull-through for high imperforate anus--a new technique J Pediatr Surg 20003506927–930., discussion 930–931 [DOI] [PubMed] [Google Scholar]
- 29.Georgeson K E. Midterm follow-up study of high-type imperforate anus after laparoscopically assisted anorectoplasty. Yearbook of Surgery. 2007;2007:287–288. doi: 10.1016/j.jpedsurg.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 30.Sydorak R M, Albanese C T. Laparoscopic repair of high imperforate anus. Semin Pediatr Surg. 2002;11(04):217–225. doi: 10.1053/spsu.2002.35358. [DOI] [PubMed] [Google Scholar]
- 31.Hamrick M, Eradi B, Bischoff A, Louden E, Peña A, Levitt M. Rectal atresia and stenosis: unique anorectal malformations. J Pediatr Surg. 2012;47(06):1280–1284. doi: 10.1016/j.jpedsurg.2012.03.036. [DOI] [PubMed] [Google Scholar]
- 32.Lee S-C, Chun Y-S, Jung S-E, Park K-W, Kim W-K. Currarino triad: anorectal malformation, sacral bony abnormality, and presacral mass--a review of 11 cases. J Pediatr Surg. 1997;32(01):58–61. doi: 10.1016/s0022-3468(97)90094-4. [DOI] [PubMed] [Google Scholar]
- 33.Levitt M A, Peña A. Cloacal malformations: lessons learned from 490 cases. Semin Pediatr Surg. 2010;19(02):128–138. doi: 10.1053/j.sempedsurg.2009.11.012. [DOI] [PubMed] [Google Scholar]
- 34.Boemers T M. Neurogenic bladder in infants born with anorectal malformations: comparison with spinal and urologic status. J Pediatr Surg. 1999;34(12):1889–1890. doi: 10.1016/s0022-3468(99)90343-3. [DOI] [PubMed] [Google Scholar]
- 35.Boemers T M, de Jong T P, van Gool J D, Bax K M. Urologic problems in anorectal malformations. Part 2: functional urologic sequelae. J Pediatr Surg. 1996;31(05):634–637. doi: 10.1016/s0022-3468(96)90663-6. [DOI] [PubMed] [Google Scholar]
- 36.Levitt M A, Kant A, Peña A. The morbidity of constipation in patients with anorectal malformations. J Pediatr Surg. 2010;45(06):1228–1233. doi: 10.1016/j.jpedsurg.2010.02.096. [DOI] [PubMed] [Google Scholar]
- 37.Kiesewetter W B. Imperforate anus: II. The rationale and technic of the sacroabdominoperineal operation. J Pediatr Surg. 1967;2:106–110. [Google Scholar]
- 38.Breech L. Gynecologic concerns in patients with anorectal malformations. Semin Pediatr Surg. 2010;19(02):139–145. doi: 10.1053/j.sempedsurg.2009.11.019. [DOI] [PubMed] [Google Scholar]
- 39.Peña A, Grasshoff S, Levitt M. Reoperations in anorectal malformations. J Pediatr Surg. 2007;42(02):318–325. doi: 10.1016/j.jpedsurg.2006.10.034. [DOI] [PubMed] [Google Scholar]
- 40.Levitt M A, King S K, Bischoff A, Alam S, Gonzalez G, Pena A. The Gonzalez hernia revisited: use of the ischiorectal fat pad to aid in the repair of rectovaginal and rectourethral fistulae. J Pediatr Surg. 2014;49(08):1308–1310. doi: 10.1016/j.jpedsurg.2013.10.020. [DOI] [PubMed] [Google Scholar]
- 41.Teich S, Caniano D A. New York, NY: Springer Science & Business Media; 2008. Reoperative Pediatric Surgery. [Google Scholar]
- 42.Levitt M A, Peña A. Pediatric fecal incontinence: a surgeon's perspective. Pediatr Rev. 2010;31(03):91–101. doi: 10.1542/pir.31-3-91. [DOI] [PubMed] [Google Scholar]