

Abstract
Background
Hybrid therapy is a promising first-line regimen for Helicobacter pylori (H. pylori) eradication. We evaluated a hybrid therapy, assessing the impact of antibiotic resistance on eradication outcome.
Methods
This was a prospective study that included 155 treatment-naïve patients diagnosed with H. pylori infection by positive CLO-test, confirmed with histology and/or culture. The hybrid therapy consisted of 40 mg esomeprazole and 1 g amoxicillin for 14 days, with the addition of 500 mg clarithromycin and 500 mg metronidazole for the final 7 days (all b.i.d.). Eradication was defined by negative 13C-urea breath test or histology.
Results
The eradication rates were 85.8% (133/155; 95% confidence interval [CI] 79.4-90.5%) by intention-to-treat and 90.2% (129/143; 95%CI 84.1-94.2%) by per-protocol analysis in a setting of high antibiotic resistance (clarithromycin 25.9%, metronidazole 31.1%, dual resistance 8.9%). Adverse events occurred in 29.7% and 1.3% discontinued treatment because of adverse events. Adherence >90% was achieved in 96.6%. The eradication rate in patients with dual clarithromycin/metronidazole resistance (50%) was markedly lower compared to those with single clarithromycin resistance (91.4%), single metronidazole resistance (90.5%) or dual susceptibility (97.8%). Dual resistance was the only factor to correlate with the failure of hybrid therapy (odds ratio 14.4, 95%CI 3.8-54.9, P=0.0003).
Conclusions
Hybrid therapy is an effective and safe first-line regimen in populations with relatively high rates of antibiotic resistance. However, dual clarithromycin/metronidazole resistance may significantly compromise its efficacy.
Keywords: Helicobacter pylori, hybrid therapy, antibiotic resistance, clarithromycin, metronidazole, dual resistance
Introduction
As a result of rising antibiotic resistance, the eradication rate of Helicobacter pylori (H. pylori) using standard triple therapies is unacceptably low (<80%) in most countries [1]. Therefore, bismuth-based and non-bismuth quadruple first-line options have been proposed, aiming to overcome increasing clarithromycin resistance [2,3]. A rational approach is to use a clarithromycin-free regimen (i.e., bismuth-based quadruple therapy). Nevertheless, non-bismuth quadruple therapies are the only realistic approach in countries where bismuth salts and/or tetracycline are not available [4]. An example is Greece, a country with high prevalence of resistance to clarithromycin (>27%) and metronidazole (>40%) [5-7]. Until recently, the sequential and concomitant regimens have been the competing non-bismuth quadruple treatments, with several studies assessing their efficacy, safety, and compliance rates. Finally, the 2015 Maastricht V/Florence consensus favored the use of concomitant (over sequential) therapy, by virtue of its better efficacy against antibiotic-resistant H. pylori strains supported by head-to-head trials [8,9].
Since 2011, the armamentarium of non-bismuth quadruple treatments has further expanded. This was due to the addition of an innovative 14-day, two-step regimen that functionally combines the concomitant and sequential treatments (i.e., hybrid therapy) [10]. It comprises a proton pump inhibitor (PPI) and amoxicillin for 14 days, adding clarithromycin and a nitroimidazole as a quadruple therapy for the final 7 days [2,10]. Compared to a concomitant treatment of same duration (14 days), the hybrid regimen is characterized by a lower pill burden. This could be associated with potential advantages, including a lower cost of eradication but also improved safety, convenience and better compliance. In the original pilot study, hybrid therapy produced outstanding cure rates, yielding 97% in intention to treat (ITT) and 99% in per protocol (PP) analysis [10]. However, this study was conducted in a setting (Taiwan) with low clarithromycin resistance. Thus, further validation is warranted for hybrid therapy, providing concrete evidence of its efficacy in geographical and/or national areas harboring different patterns of antimicrobial resistance [11]. To date, only a limited number of studies have evaluated hybrid therapy in a high-resistance setting, and even fewer provided pretreatment susceptibility data. Therefore, this prospective open-label trial was aimed to determine the clinical efficacy and safety of the hybrid regimen in treatment-naïve patients in Greece. The impact of H. pylori resistance to clarithromycin and metronidazole on the efficacy of hybrid therapy was also evaluated.
Patients and methods
Study design and participants
This was a prospective, open-label, dual-center study for the treatment of patients with H. pylori infection. The study was conducted from January 2015 to March 2016 in the Gastroenterology Departments of the Athens Medical, Paleo Faliron General Hospital (Athens, Greece) and the General Hospital of Rhodes (Rhodes, Greece). Consecutive patients with dyspepsia who were referred and scheduled for upper endoscopy were prospectively enrolled. Eligible patients were those aged 18 years, diagnosed with H. pylori infection by rapid urease test confirmed with gastric histology and/or culture. The following were exclusion criteria: a history of previous H. pylori eradication treatment; allergies to the medications used; treatment during the preceding two months with antibiotics, bismuth preparations or non-steroid anti-inflammatory drugs, and in the preceding two weeks with PPIs; previous esophageal or gastric surgery; serious systemic disease; pregnancy or lactation. For eligible patients, the demographic data, body mass index (BMI), history of smoking and alcohol consumption, and the endoscopic findings were all recorded.
The study protocol was in accordance with the principles of the Declaration of Helsinki and was approved by the local Ethics Committee of the participating hospitals. Written informed consent was obtained from all patients prior to their enrollment in the study.
Treatment and procedures
All eligible patients were assigned to receive a hybrid regimen consisting of 40 mg esomeprazole and 1 g amoxicillin for 14 days, with the addition of 500 mg clarithromycin and 500 mg metronidazole for the final 7 days, all twice daily. A 13C-urea breath test (Helicobacter Test INFAI®, INFAI GmbH, Cologne, Germany) was performed 8-12 weeks after completion of treatment and a negative test result was considered indicative of successful H. pylori eradication. For patients who required a follow-up endoscopy because of gastric ulcer, histological evaluation of gastric biopsies (two from the corpus and two from the antrum) was the diagnostic test.
Treatment-related side-effects were investigated by means of a structured questionnaire, immediately after therapy was completed. Patients were asked to grade the severity of each side-effect as follows: a) mild: transient and well tolerated; b) moderate: causing discomfort and partially interfering with common everyday activities; c) severe: causing considerable interference with the patient’s activities, possibly incapacitating or life-threatening. Drug compliance was determined by counting unused medication. For this purpose, any tablet that was not consumed was brought back to the clinic for pill count. Patients’ adherence to therapy was defined as poor if <90% of the prescribed medication was taken. Biopsy specimens were cultured according to previously described methods and antibiotic susceptibility was determined by Etest® (AB Biodisk, Solna, Sweden) [5,7]. H. pylori strains with MICs of >1 μg/mL, >0.5 μg/mL and >8 μg/mL were considered to be resistant to clarithromycin, amoxicillin and metronidazole, respectively. Culture and antibiotic susceptibility testing procedures were centralized and performed by blinded personnel at the Laboratory of Medical Microbiology of the Hellenic Pasteur Institute (Athens, Greece).
Statistical analysis
The primary outcome was eradication of H. pylori infection. In the ITT analysis, data from all included patients were calculated and patients who did not complete the study were counted as treatment failures. PP analysis excluded patients who violated the study protocol or who were noncompliant with the prescribed treatment. Secondary outcomes were compliance and side effects.
Categorical variables are expressed as percentages, while continuous variables are expressed as means with standard deviation. The chi-square test or the Fisher’s exact test were used to compare categorical data, as appropriate. The eradication rates and their 95% confidence intervals (CI) were calculated.
Univariate analysis was performed to evaluate factors affecting the eradication efficacy of hybrid therapy. A multivariate regression analysis was planned, including variables with statistical significance (P<0.1) on univariate analysis. The magnitude of the effect is described as odds ratio (OR) with 95%CI. SPSS version 24 for Macintosh (IBM SPSS, Chicago, IL, USA) was used for statistical analyses and a two-sided P-value of <0.05 was regarded as statistically significant.
Results
Patient data and antibiotic resistance rates
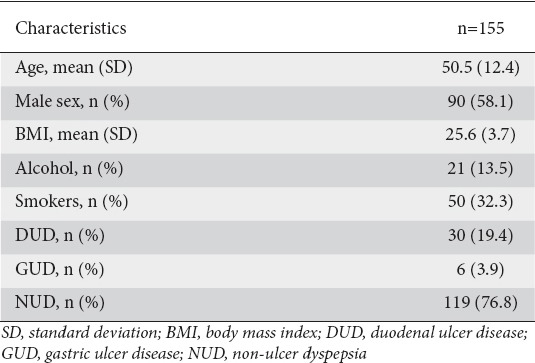
The study flow chart is shown in Fig. 1. A total of 343 patients were initially screened for eligibility and 188 were excluded. Thus, 155 patients were finally included in the study; their baseline characteristics are shown in Table 1. H. pylori culture and sensitivity test were successfully carried out in 135/155 (87.1%) patients. The rates of H. pylori strains with single resistance to clarithromycin, metronidazole and amoxicillin were 35/135 (25.9%), 42/135 (31.1%) and 0/135 (0%), respectively, whereas dual clarithromycin/metronidazole resistance was detected in 12/135 (8.9%).
Figure 1.
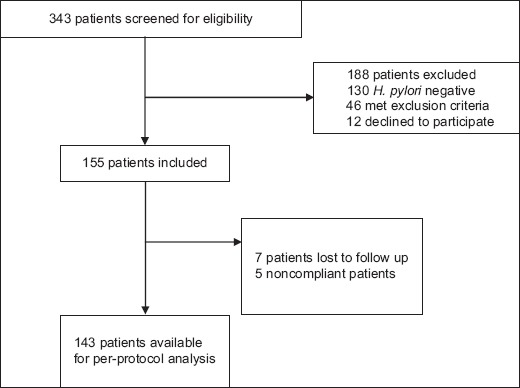
Flowchart of the patients in the study
H. pylori, Helicobacter pylori.
Table 1.
Clinical and demographic characteristics of the treated population
Side effects and adherence
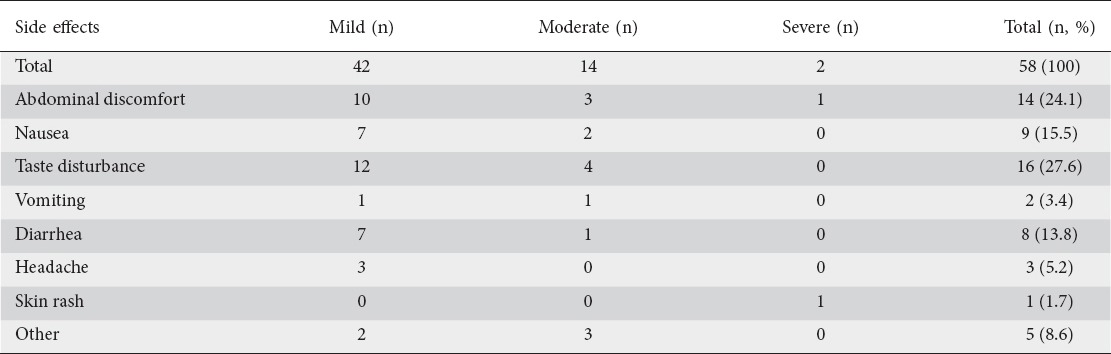
One hundred fifty-five patients were included in the trial, but a total of seven patients were lost to follow up (Fig. 1). Among the 148 patients who returned for follow up, a total of 58 adverse events were noted in 44 (29.7%) patients. The proportion and severity of adverse events is shown in Table 2. Overall, 2 of the 148 patients (1.3%) specified severe adverse events as the reason for treatment interruption. One patient discontinued treatment on day 11 because of abdominal discomfort; however, H. pylori was successfully eradicated, as indicated by the negative breath test on final follow up. However, the other patient, who interrupted treatment on day 3 because of an allergic skin rash, failed to eradicate the pathogen. Overall, 96.6% (143/148) of the patients took more than 90% of the total medication prescribed. Adherence to therapy, defined as the total percentage of tablets taken, was 98.3% (95%CI 98.1-98.5%).
Table 2.
Adverse events resulting from eradication therapy
Eradication efficacy and associated factors
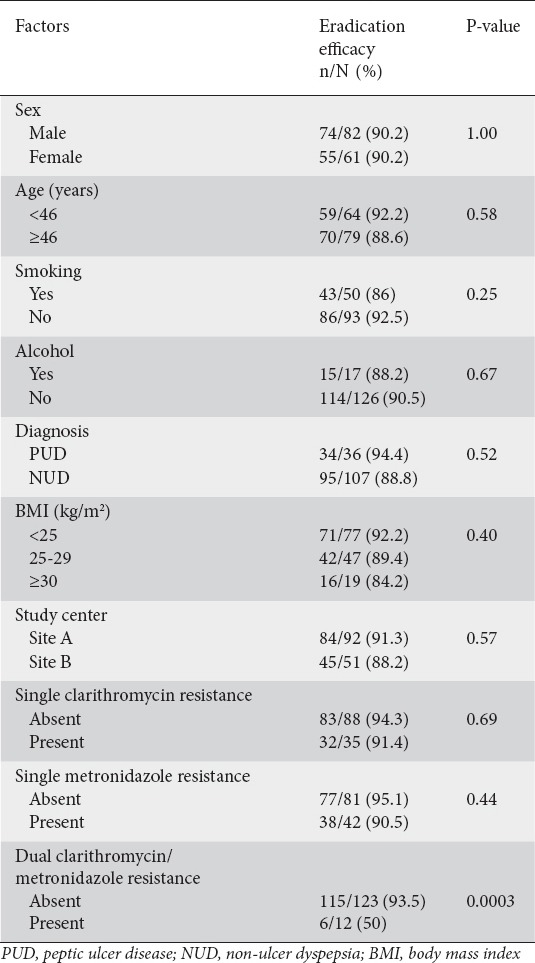
Overall, eradication rates were 85.8% (133/155; 95%CI 79.4-90.5%) and 90.2% (129/143; 95%CI 84.1-94.2%) respectively, in the ITT and PP analyses. No differences in the eradication rates were found between the clarithromycin-resistant and -sensitive strains (91.4% [32/35] vs. 94.3% [83/88], P=0.69), or between the metronidazole-resistant and -sensitive strains (90.5% [38/42] vs. 95.1% [77/81], P=0.44). However, dual clarithromycin-metronidazole resistance was associated with a significantly lower eradication rate (50% [6/12]) compared with single clarithromycin resistance (91.4% [32/35], P=0.005), single metronidazole resistance (90.5% [38/42], P=0.005) and dual susceptibility (97.8% [45/46], P=0.0001). By univariate analysis (Table 3), the following variables were not associated with H. pylori eradication: sex, age, BMI, history of smoking and alcohol consumption, indication for eradication (peptic ulcer disease vs. non-ulcer dyspepsia), study center, and single clarithromycin or metronidazole resistance. The presence of dual clarithromycin/metronidazole resistance was the only factor associated with the failure of hybrid therapy (OR 14.4, 95%CI 3.8-54.9, P=0.0003).
Table 3.
Factors affecting the eradication efficacy (per protocol) of hybrid therapy as determined by univariate analysis
Discussion
Six years after it was first proposed, our understanding of hybrid therapy remains limited. Available evidence from 12 studies (2009-2015) has indeed shown a wide variation in the eradication rates, ranging from 77.6-97.4% in ITT and from 82.6-99.1% in PP analysis [12]. These heterogeneous results underscore the need for cautious interpretation of data pertaining to different regions and populations, which are likely to reflect different backgrounds of antibiotic resistance. To date, only a few studies evaluating hybrid therapy provided susceptibility data, mostly from regions with low-to-moderate clarithromycin resistance [10,13]. Moreover, the subpopulations tested were inherently small, thus raising the possibility of selection bias. This prospective trial, involving 155 patients from two hospitals located in two geographically distinct areas of Greece, indicates that hybrid therapy is a valuable (PP eradication: 90.2%) treatment option that is safe and well-tolerated by most patients. This was achieved in the face of high (>15%) clarithromycin, but acceptable (<9%) dual clarithromycin/metronidazole resistance, documented by extensive analysis of susceptibility data (n=135) [8]. To our knowledge, this is the first evaluation of hybrid therapy in Greece and represents the largest European series of antibiotic-resistant H. pylori strains treated with hybrid therapy.
We determined that the efficacy of hybrid therapy is markedly decreased by dual clarithromycin/metronidazole resistance. This premise has been also corroborated in previous studies that evaluated sequential and concomitant regimens [5,7,14,15]. Therefore, all non-bismuth quadruple therapies appear to be influenced by dual resistance, though not to the same extent. Rates of dual resistance >5%, >9% and >15% have been proposed as the thresholds associated with unacceptable performance (<90% cure rate) for sequential, hybrid and concomitant regimens, respectively [16]. Overall, our experience appears to support this notion, indicating that both the 10-day concomitant and 14-day hybrid therapies, but not the sequential therapy, are acceptable first-line regimens in Greece, a country with a >5% but <9% prevalence of dual clarithromycin/metronidazole resistance [5,7,17,18]. A head-to-head comparison between the 10-day concomitant and 14-day hybrid regimens would be useful to clarify the optimal first-line regimen in Greece. However, assuming they prove to be equally effective, the lower pill burden (80 tablets for 10-day concomitant; 84 tablets for 14-day hybrid) and less complex administration would favor the 10-day concomitant therapy. Crucially, shortening the duration of hybrid therapy (to 10 or 12 days) may be realistic in regions of moderate-to-low resistance [13]. However, this may be unfeasible in high-resistance settings, as shown by an Iranian randomized study comparing 14- and 10-day hybrid therapies (PP eradication: 92.8% and 83.8% respectively) [19]. Likewise, prolonged (14 days) exposure to amoxicillin is the key for improved eradication with hybrid therapy. Accordingly, prolonging the duration of sequential therapy (in which amoxicillin is discontinued at mid-point) does not seem to provide any substantial benefit [20]. To date, a single study from China recorded such a large dataset (n=135) of antibiotic susceptibility before hybrid therapy [21]. In sharp contrast to our data, hybrid therapy was shown to perform unsatisfactorily (ITT: 77%, PP: 86%), an unsurprising finding considering that the burden of antibiotic resistance was disproportionately higher (clarithromycin 44.9%, metronidazole 67.3%, dual 33.3%). Interestingly, the deleterious impact of dual resistance appears to be more prominent in the European as compared to the Asian population (efficacy against dual-resistant H. pylori strains: 70.2% in the Chinese study vs. 50% in present series) [21]. In keeping with this observation, only one out of three dual-resistant H. pylori strains was successfully eradicated in a Spanish/Italian study [22]. Clearly, a number of potential confounders may play a role, including racial and genetic background, differences in the metabolism of PPIs, and the nature of the underlying disease. Furthermore, variations in the type of PPI and nitroimidazole may affect the eradication outcome. Notably, tinidazole, which is known to possess a longer half-life compared to metronidazole, was used in the Chinese study. With regard to acid suppression, we used high-dose (40 mg b.i.d.) esomeprazole, a new-generation PPI that has been reported to be metabolized irrespective of the cytochrome P450 (CYP) 2C19 status [23]. In contrast, standard-dose (20 mg b.i.d.) omeprazole was used in the Chinese study, justified by the lower prevalence of rapid metabolizers among the Asian population [24]. Clearly, both studies address the same effect (i.e., detrimental impact of dual resistance on hybrid therapy). However, they addressed different settings of antibiotic resistance and distinct populations that were likely to reflect different magnitudes of this same phenomenon. Thus, rather than contrasting, the two studies should be viewed as complementary.
As sequential therapy, hybrid therapy has been devised to decrease pill burden (compared to concomitant therapy) with no efficacy cost, relying on sequential administration. It has been postulated that pretreatment with amoxicillin could markedly reduce the bacterial load and prevent the development of bacterial efflux channels [25], increasing the susceptibility of the organisms during the second phase of treatment [26]. Nevertheless, the concept of sequential administration has been seriously challenged by studies showing that “reverse hybrid” and “reverse sequential” regimens perform equally well [27,28]. Indeed, in a recent Taiwanese trial, reverse hybrid therapy was highly effective (95.7% by PP analysis) and superior to standard triple therapy [27].
In keeping with our findings, previous studies evaluating hybrid therapy reported consistently good compliance and safety [10,13,19,29-33]. A Spanish/Italian study determined that the overall rate of adverse effects of hybrid therapy was lower than that of concomitant therapy [22]. Likewise, the rate of discontinued medication was lower in a Korean study [31]. However, in both studies the differences were of borderline significance (P=0.05 and P=0.051, respectively). Overall, based on updated meta-analyses, hybrid therapy appears to display slightly better compliance and safety than concomitant therapy [12,34]. However, whether this difference may be clinically relevant, particularly regarding a routine practice setting, merits further assessment.
The present trial is not free of limitations. Firstly, by design, this was an open-label, non-controlled study, precluding conclusions on the comparative efficacy and safety of hybrid therapy. Secondly, the antimicrobial susceptibility of H. pylori was determined using the E-test, which tends to overestimate metronidazole resistance, although in a previous study this was not associated with any change in the overall metronidazole resistance pattern [7]. Thirdly, CYP2C19 polymorphisms were not evaluated. However, we expect the impact, if any, to be minimal, as the metabolism of esomeprazole has been reported to be independent of CYP2C19 status [35].
In conclusion, hybrid therapy achieved an H. pylori cure rate of 90.2% (PP) in a setting with high resistance to clarithromycin and metronidazole. Dual clarithromycin and metronidazole resistance plays a key role in the treatment failure of hybrid therapy. Further studies providing susceptibility data are warranted to better define the position of hybrid therapy in the armamentarium of current first-line regimens for H. pylori eradication.
Summary Box.
What is already known:
Because of rising antibiotic resistance, Helicobacter pylori (H. pylori) eradication rate with standard triple therapies is unacceptably low (<80%) in most countries
Hybrid therapy is an innovative 14-day, two-step, non-bismuth quadruple regimen, which functionally combines the concomitant and sequential treatments
To date, only a limited number of studies have evaluated hybrid therapy in a high-resistance setting, and even fewer provided pretreatment susceptibility data
What the new findings are:
This is the largest, to date, European series of antibiotic-resistant H. pylori strains treated with hybrid therapy
Hybrid therapy is an effective (PP cure rate: 90.2%) and safe first-line regimen for H. pylori eradication in populations with relatively high antibiotic resistance rates
Dual clarithromycin and metronidazole resistance plays a key role in the treatment failure of hybrid therapy
Biography
Athens Medical, Paleo Faliron Hospital, Athens; General Hospital of Rhodes; Hellenic Pasteur Institute, Athens, Greece
Footnotes
Conflict of interest: None
References
- 1.Papastergiou V, Georgopoulos SD, Karatapanis S. Treatment ofHelicobacter pyloriinfection:meeting the challenge of antimicrobial resistance. World J Gastroenterol. 2014;20:9898–9911. doi: 10.3748/wjg.v20.i29.9898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Georgopoulos SD, Papastergiou V, Karatapanis S. Current options for the treatment ofHelicobacter pylori. Expert Opin Pharmacother. 2013;14:211–223. doi: 10.1517/14656566.2013.763926. [DOI] [PubMed] [Google Scholar]
- 3.Papastergiou V, Georgopoulos SD, Karatapanis S. Treatment ofHelicobacter pyloriinfection:past, present and future. World J Gastrointest Pathophysiol. 2014;5:392–399. doi: 10.4291/wjgp.v5.i4.392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Georgopoulos SD, Papastergiou V, Karatapanis S. Helicobacter pylorieradication therapies in the era of increasing antibiotic resistance:a paradigm shift to improved efficacy. Gastroenterol Res Pract. 2012;2012:757926. doi: 10.1155/2012/757926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Georgopoulos SD, Xirouchakis E, Martinez-Gonzales B, et al. Randomized clinical trial comparing ten day concomitant and sequential therapies forHelicobacter pylorieradication in a high clarithromycin resistance area. Eur J Intern Med. 2016;32:84–90. doi: 10.1016/j.ejim.2016.04.011. [DOI] [PubMed] [Google Scholar]
- 6.Karamanolis GP, Daikos GL, Xouris D, Goukos D, Delladetsima I, Ladas SD. The evolution ofHelicobacter pyloriantibiotics resistance over 10 years in Greece. Digestion. 2014;90:229–231. doi: 10.1159/000369898. [DOI] [PubMed] [Google Scholar]
- 7.Georgopoulos SD, Xirouchakis E, Martinez-Gonzalez B, et al. Clinical evaluation of a ten-day regimen with esomeprazole, metronidazole, amoxicillin, and clarithromycin for the eradication ofHelicobacter pyloriin a high clarithromycin resistance area. Helicobacter. 2013;18:459–467. doi: 10.1111/hel.12062. [DOI] [PubMed] [Google Scholar]
- 8.Malfertheiner P, Megraud F, O'Morain CA, et al. EuropeanHelicobacterand Microbiota Study Group and Consensus panel. Management ofHelicobacter pyloriinfection-the Maastricht V/Florence Consensus Report. Gut. 2017;66:6–30. doi: 10.1136/gutjnl-2016-312288. [DOI] [PubMed] [Google Scholar]
- 9.Georgopoulos SD, Xirouchakis E. Which regimens should be used and which rejected for the treatment ofHelicobacter pylori? Am J Gastroenterol. 2017;112:1168–1169. doi: 10.1038/ajg.2017.90. [DOI] [PubMed] [Google Scholar]
- 10.Hsu PI, Wu DC, Wu JY, Graham DY. Modified sequentialHelicobacter pyloritherapy:proton pump inhibitor and amoxicillin for 14 days with clarithromycin and metronidazole added as a quadruple (hybrid) therapy for the final 7 days. Helicobacter. 2011;16:139–145. doi: 10.1111/j.1523-5378.2011.00828.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liatsos C, Georgopoulos SD. Helicobacter pyloribest treatment approach:should a national consensus be the best consensus? Ann Gastroenterol. 2017;30:704–706. doi: 10.20524/aog.2017.0183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Song ZQ, Liu J, Zhou LY. Hybrid therapy regimen forHelicobacter pylorieradication. Chin Med J (Engl) 2016;129:992–999. doi: 10.4103/0366-6999.179803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wu JY, Hsu PI, Wu DC, Graham DY, Wang WM. Feasibility of shortening 14-day hybrid therapy while maintaining an excellentHelicobacter pylorieradication rate. Helicobacter. 2014;19:207–213. doi: 10.1111/hel.12113. [DOI] [PubMed] [Google Scholar]
- 14.Zhou L, Zhang J, Chen M, et al. A comparative study of sequential therapy and standard triple therapy forHelicobacter pyloriinfection:a randomized multicenter trial. Am J Gastroenterol. 2014;109:535–541. doi: 10.1038/ajg.2014.26. [DOI] [PubMed] [Google Scholar]
- 15.Georgopoulos SD, Xirouchakis E, Mentis A. Is there a nonbismuth quadruple therapy that can reliably overcome bacterial resistance? Gastroenterology. 2013;145:1496–1497. doi: 10.1053/j.gastro.2013.07.054. [DOI] [PubMed] [Google Scholar]
- 16.Graham DY, Lee YC, Wu MS. RationalHelicobacter pyloritherapy:evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014;12:177–186. e3. doi: 10.1016/j.cgh.2013.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Georgopoulos S, Papastergiou V, Xirouchakis E, et al. Nonbismuth quadruple “concomitant” therapy versus standard triple therapy, both of the duration of 10 days, for first-lineH. pylorieradication:a randomized trial. J Clin Gastroenterol. 2013;47:228–232. doi: 10.1097/MCG.0b013e31826015b0. [DOI] [PubMed] [Google Scholar]
- 18.Georgopoulos S, Papastergiou V, Xirouchakis E, et al. Evaluation of a four-drug, three-antibiotic, nonbismuth-containing “concomitant” therapy as first-lineHelicobacter pylorieradication regimen in Greece. Helicobacter. 2012;17:49–53. doi: 10.1111/j.1523-5378.2011.00911.x. [DOI] [PubMed] [Google Scholar]
- 19.Metanat HA, Valizadeh SM, Fakheri H, et al. Comparison between 10- and 14-day hybrid regimens forHelicobacter pylorieradication:a randomized clinical trial. Helicobacter. 2015;20:299–304. doi: 10.1111/hel.12202. [DOI] [PubMed] [Google Scholar]
- 20.Hsu PI, Wu DC, Wu JY, Graham DY. Is there a benefit to extending the duration ofHelicobacter pylorisequential therapy to 14 days? Helicobacter. 2011;16:146–152. doi: 10.1111/j.1523-5378.2011.00829.x. [DOI] [PubMed] [Google Scholar]
- 21.Song Z, Zhou L, Zhang J, He L, Bai P, Xue Y. Hybrid therapy as first-line regimen forHelicobacter pylorieradication in populations with high antibiotic resistance rates. Helicobacter. 2016;21:382–388. doi: 10.1111/hel.12294. [DOI] [PubMed] [Google Scholar]
- 22.Molina-Infante J, Romano M, Fernandez-Bermejo M, et al. Optimized nonbismuth quadruple therapies cure most patients withHelicobacter pyloriinfection in populations with high rates of antibiotic resistance. Gastroenterology. 2013;145:121–128. doi: 10.1053/j.gastro.2013.03.050. [DOI] [PubMed] [Google Scholar]
- 23.Georgopoulos SD, Papastergiou V, Karatapanis S. Treatment ofHelicobacter pyloriinfection:optimization strategies in a high resistance era. Expert Opin Pharmacother. 2015;16:2307–2317. doi: 10.1517/14656566.2015.1084503. [DOI] [PubMed] [Google Scholar]
- 24.Bertilsson L, Lou YQ, Du YL, et al. Pronounced differences between native Chinese and Swedish populations in the polymorphic hydroxylations of debrisoquin and S-mephenytoin. Clin Pharmacol Ther. 1992;51:388–397. doi: 10.1038/clpt.1992.38. [DOI] [PubMed] [Google Scholar]
- 25.Webber MA, Piddock LJ. The importance of efflux pumps in bacterial antibiotic resistance. J Antimicrob Chemother. 2003;51:9–11. doi: 10.1093/jac/dkg050. [DOI] [PubMed] [Google Scholar]
- 26.Zullo A, Rinaldi V, Winn S, et al. A new highly effective short-term therapy schedule forHelicobacter pylorieradication. Aliment Pharmacol Ther. 2000;14:715–718. doi: 10.1046/j.1365-2036.2000.00766.x. [DOI] [PubMed] [Google Scholar]
- 27.Hsu PI, Kao SS, Wu DC, et al. Taiwan Acid-Related Disease Study Group. A randomized controlled study comparing reverse hybrid therapy and standard triple therapy forHelicobacter pyloriinfection. Medicine (Baltimore) 2015;94:e2104. doi: 10.1097/MD.0000000000002104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tsay FW, Wu DC, Kao SS, et al. Reverse sequential therapy achieves a similar eradication rate as standard sequential therapy forHelicobacter pylorieradication:a randomized controlled trial. Helicobacter. 2015;20:71–77. doi: 10.1111/hel.12176. [DOI] [PubMed] [Google Scholar]
- 29.Cuadrado-Lavín A, Salcines-Caviedes JR, Diaz-Perez A, et al. First-line eradication rates comparing two shortened non-bismuth quadruple regimens againstHelicobacter pylori:an open-label, randomized, multicentre clinical trial. J Antimicrob Chemother. 2015;70:2376–2381. doi: 10.1093/jac/dkv089. [DOI] [PubMed] [Google Scholar]
- 30.De Francesco V, Hassan C, Ridola L, Giorgio F, Ierardi E, Zullo A. Sequential, concomitant and hybrid first-line therapies forHelicobacter pylorieradication:a prospective randomized study. J Med Microbiol. 2014;63:748–752. doi: 10.1099/jmm.0.072322-0. [DOI] [PubMed] [Google Scholar]
- 31.Heo J, Jeon SW, Jung JT, et al. Daegu-Gyeongbuk Gastrointestinal Study Group. Concomitant and hybrid therapy forHelicobacter pyloriinfection:A randomized clinical trial. J Gastroenterol Hepatol. 2015;30:1361–1366. doi: 10.1111/jgh.12983. [DOI] [PubMed] [Google Scholar]
- 32.Oh DH, Lee DH, Kang KK, et al. Efficacy of hybrid therapy as first-line regimen forHelicobacter pyloriinfection compared with sequential therapy. J Gastroenterol Hepatol. 2014;29:1171–1176. doi: 10.1111/jgh.12518. [DOI] [PubMed] [Google Scholar]
- 33.Sardarian H, Fakheri H, Hosseini V, Taghvaei T, Maleki I, Mokhtare M. Comparison of hybrid and sequential therapies forHelicobacter pylorieradication in Iran:a prospective randomized trial. Helicobacter. 2013;18:129–134. doi: 10.1111/hel.12017. [DOI] [PubMed] [Google Scholar]
- 34.Song ZQ, Zhou LY. Hybrid, sequential and concomitant therapies forHelicobacter pylorieradication:A systematic review and meta-analysis. World J Gastroenterol. 2016;22:4766–4775. doi: 10.3748/wjg.v22.i19.4766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tang HL, Li Y, Hu YF, Xie HG, Zhai SD. Effects of CYP2C19 loss-of-function variants on the eradication ofH. pyloriinfection in patients treated with proton pump inhibitor-based triple therapy regimens:a meta-analysis of randomized clinical trials. PLoS One. 2013;8:e62162. doi: 10.1371/journal.pone.0062162. [DOI] [PMC free article] [PubMed] [Google Scholar]