

Abstract
An ectopic thyroid gland may be present in any location along the path of migration from the foramen caecum to the mediastinum. The most common locations for an ectopic thyroid are the lingual thyroid followed by median cervical cysts. An ectopic thyroid in the submandibular region is extremely rare. We present the case of a 44-year-old patient with ectopic thyroid tissue in submandibular space and a review of the literature related to it.
Keywords: Thyroid gland, Thyroid dysgenesis, Tomography, Thyroid scan, Tomography, Thyroid function tests, Submandibular
The thyroid gland normally appears as a midline diverticulum between the first and second branchial arches in the third to fourth week of embryogenic development. This diverticulum develops between the hypobranchial eminence, which forms the posterior third of the tongue, and the tuberculum impar, which is responsible for the development of the anterior two-thirds of the tongue. The bilobed diverticulum, which is the median anlage, descends caudally as the embryo grows and fuses with lateral anlages that arise from ultimobranchial bodies to form the complete gland.1
By means of a stalk, the thyroid anlage remains connected to the pharyngeal pouch along the midline. This stalk ‘thyroglossal duct’ involutes and atrophies by the seventh to eighth week of embryonic life. The thyroid meanwhile continues to migrate caudally in the midline, passing anteriorly to the hyoid and laryngeal cartilages, and finally rests anterior to the trachea at the level of the second and third tracheal rings. Any arrest or abnormality in this pathway of descent will lead to ectopia.
Case history
A 44-year-old male presented in our department with a history of swelling in the right submandibular region for the past 15 years that was slowly progressive in nature. The patient was operated on 18 years earlier for a similar swelling but no details were available related to that. A clinical examination identified a mass in the right submandibular triangle of the neck measuring 8cm x 5cm in size and firm in consistency.
The rest of the examination including a clinical endoscopic examination was normal. A fine needle aspiration (FNA) of the submandibular mass was suggestive of a pleomorphic adenoma. Ultrasonography of the neck revealed a large hyperechoic mass in the submandibular area with an absent right thyroid lobe and isthmus and an atrophic left lobe. Computed tomography (CT) of the neck confirmed a right submandibular mass of 5.5cm x 5cm in size extending into sublingual space with no submandibular gland seen separately (Fig 1). The mass showed an intense post-contrast enhancement and dilated peripheral vascular channels with another small (1cm) enhancing focus seen in the left sublingual space. The thyroid was found to be absent with an atrophic left submandibular gland. All blood tests were normal, including thyroid function tests. A radioisotope thyroid scan revealed an increased uptake in the right submandibular region, indicating functional thyroid tissue in the mass.
Figure 1.

Computed tomography depicting a mass in the right submandibular region
Surgery was planned while bearing in mind that a large swelling was increasing in size and FNA was suggestive of a pleomorphic adenoma (Fig 2). After obtaining consent for postoperative hypothyroidism, surgery was performed. The excision of the mass with right submandibular node clearance was done while preserving the hypoglossal and lingual nerves and keeping the floor of the mouth intact. The dissection was confined to the submandibular triangle only and the submandibular gland could not be identified separately from the mass.
Figure 2.
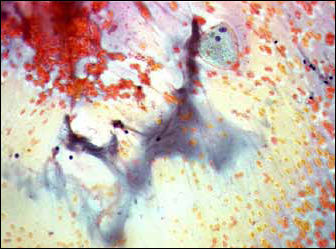
Fine needle aspiration histology suggestive of a salivary gland tumour
Pathological diagnosis
Histological examination of the submandibular mass identified a 7cm x 7cm x 4.5cm lobulated mass separated by septa and cystic spaces, and marked with specks of calcification (Fig 3). The findings were consistent with ectopic thyroid tissue with changes of adenomatous goitre.
Figure 3.
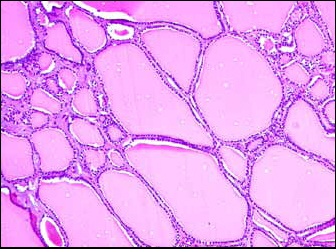
Final histology in favour of thyroid tissue with an adenomatous goitre
Following surgery, no intraoral bulge was palpated. A radioactive iodine uptake test showed <2% uptake at the operative site, indicating that the excised submandibular was the only functioning thyroid tissue in the body. The patient was started on oral thyroxine.
Discussion
Ectopic thyroid tissue is defined as thyroid tissue not located anterolaterally to the second, third and fourth tracheal rings.2 An ectopic thyroid is a rare phenomenon that may be found in any position along the thyroglossal track resulting from an abnormality in the normal descent of the thyroid along the midline in the neck. In 1869 Hickman was the first to report a lingual thyroid3 and since then many reports describing several ectopic locations for thyroid tissue have been published. The prevalence of an ectopic thyroid is reported to be 1 in 100,000–300,000 in the normal population and the male to female ratio is approximately 1:4.4 Ectopic thyroid tissue along the thyroglossal duct tract has been reported to have an incidence proportion of 7–10% of normal populations in different series.5,6 In 70% of the cases, the ectopic thyroid tissue is the only functional tissue described.7
The ectopic thyroid may rest anywhere along the path of migration from the foramen caecum to the mediastinum (Table 1). It is most commonly found as a lingual thyroid, which accounts for 90% of the reported cases in the literature. The other sites described include the mediastinum, lung, porta hepatis, duodenum, oesophagus, heart, breast and intratrachea etc.8 One very rare location for ectopic thyroid tissue as a mass is the submandibular region. Thyroid migration is associated with FOXE1 mutation in mouse models but to date no gene has been implicated for human ectopic thyroids.9
Table 1.
Location of ectopic thyroid glands
| Lingual thyroid |
| Intralingual thyroid |
| Thyroglossal duct cyst |
| Intratracheal position |
| Mediastinum |
Ectopic thyroid tissue as a submandibular mass can be explained in three ways: displacement during embryonic development (true lateral aberrant thyroid), metastasis of a thyroid carcinoma (lateral aberrant thyroid) or implantation of tissue during surgical procedures on a normally located thyroid.
It was previously believed that an ectopic submandibular location of thyroid tissue was due to the failure of descent of the lateral anlage or ‘ultimobranchial bodies’ in the neck but Radkowski et al10 and Morgan et al11 both proposed that thyroglossal duct cysts can be displaced from the midline. Laterally displaced ectopic thyroid tissue is more likely related to this phenomenon.
Very few cases of an ectopic thyroid in the submandibular region have been described in the literature (Table 2), with no clear guidelines regarding its diagnostic workup and management issues. We recommend that, prior to deciding on surgical excision, one must carry out investigations such as FNA of the mass, thyroid function tests, thyroid scans and imaging. FNA can be of vital importance considering that the majority of lateral ectopic thyroid cases represent metastatic disease from a primary thyroid carcinoma. Imaging studies such as CT or ultrasonography help in determining anatomical variants and can guide operative intervention. An iodine-131 or technetium-99m scan is recommended for looking for functional thyroid tissue before deciding on surgery.
Table 2.
Various case reports of an ectopic thyroid gland in the submandibular region
| Author and publication | Age of patient | Sex | Location of thyroid tissue | Histopathology |
| Helidonis et al J laryngol Otol 1980 |
30 | F | left submandibular and submental | Diffuse colloid goitre |
| Rubenfeld et al Arch Otolaryngol Head Neck Surg 1988 |
28 | F | Right cervical and submental | Normal thyroid |
| Aguirre et al Oral Surg Oral Med Oral Pathol 1991 |
47 | F | left submandibular | Colloid goitre |
| Alsop et al J Oral Pathol 1986 |
61 | M | Right submandibular and lingual thyroid | Signet ring follicular adenoma |
| Sambola-Cabrer et al Head Neck 1996 |
35 | F | Submandibular with normal thyroid | Fine needle aspiration: normal thyroid |
| Morgan et al J laryngol Otol 1995 |
50 | F | Right submandibular and lingual thyroid | Adenomatous hyperplasia |
| Sironi et al Clin Nucl Med 1996 |
45 | F | Bilateral submandibular | No surgery |
| kumar et al Clin Nuclear Med 2001 |
12 | M | left submandibular | Fine needle aspiration: colloid goitre |
| Gin et al Endocr Pathol 1998 |
29 | F | Right submandibular with normal thyroid | Clear cell follicular adenoma |
| Babazade et al J Oral Sci 2009 |
29 | F | Right submandibular | Thyroid tissue |
| Huang et al Head Neck 2007 |
71 | F | Right submandibular with normal thyroid | Ectopic thyroid tissue with goitrous change |
The indications for surgery in an ectopic thyroid include the generally symptomatic patient, risk of malignancy, presence of other thyroid tissue and cosmetic deformity. Surgery can be offered safely with postoperative thyroid hormone replacement therapy. However, patients can also simply be observed if there is no risk of developing a malignancy and the ectopic thyroid tissue is the only functional tissue in the body.
Conclusions
Ectopic submandibular thyroid tissue is extremely rare and poses both diagnostic and treatment problems. Before surgical excision of the ectopic thyroid, it is necessary to ensure that normal, well functioning thyroid tissue is present. Scintigraphy plays an important role in these conditions and the decision to excise should be taken only after a careful and complete pre-surgical workup of the patient.
References
- 1.Mansberger AR Jr, Wei JP. Surgical embryology and anatomy of the thyroid and parathyroid glands. Surg Clin North Am 1993; 73: 727–746. [DOI] [PubMed] [Google Scholar]
- 2.Damiano A, Glickman AB, Rubin JS, Cohen AF. Ectopic thyroid tissue presenting as a midline neck mass. Int J Pediatr Otorhinolaryngol 1996; 34: 141–148. [DOI] [PubMed] [Google Scholar]
- 3.Hickman W. Congenital tumor of the base of the tongue, pressing down the epiglottis on the larynx and causing death by suffocation sixteen hours after birth. Trans Pathol Soc Lond 1869; 20: 160–161. [Google Scholar]
- 4.Williams ED, Toyn CE, Harach HR. The ultimobranchial gland and congenital thyroid abnormalities in man. J Pathol 1989; 159: 135–141. [DOI] [PubMed] [Google Scholar]
- 5.Ellis PD, van Nostrand AW. The applied anatomy of thyroglossal tract remnants. Laryngoscope 1977; 87: 765–770. [DOI] [PubMed] [Google Scholar]
- 6.Sauk JJ., Jr Ectopic lingual thyroid. J Pathol 1970; 102: 239–243. [DOI] [PubMed] [Google Scholar]
- 7.Williams JD, Sclafani AP, Slupchinskij O, Douge C. Evaluation and management of the lingual thyroid gland. Ann Otol Rhinol Laryngol 1996; 105: 312–316. [DOI] [PubMed] [Google Scholar]
- 8.Feller KU, Mavros A, Gaertner HJ. Ectopic submandibular thyroid tissue with a coexisting active and normally located thyroid gland: case report and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 90: 618–623. [DOI] [PubMed] [Google Scholar]
- 9.De Felice M, Di Lauro R. Thyroid development and its disorders: genetics and molecular mechanisms. Endocr Rev 2004; 25: 722–746. [DOI] [PubMed] [Google Scholar]
- 10.Radkowski D, Arnold J, Healy GB et al. Thyroglossal duct remnants. Preoperative evaluation and management. Arch Otolaryngol Head Neck Surg 1991; 117: 1,378–1,381. [DOI] [PubMed] [Google Scholar]
- 11.Morgan NJ, Emberton P, Barton RP. The importance of thyroid scanning in neck lumps – a case report of ectopic tissue in the right submandibular region. J Laryngol Otol 1995; 109: 674–676. [DOI] [PubMed] [Google Scholar]