

Abstract
Situs inversus is a rare congenital anomaly that has reportedly been associated with caecal volvulus. We describe a case of partial situs inversus complicated by intestinal obstruction secondary to three simultaneously occurring volvuli of the stomach, caecum and sigmoid colon. To our knowledge, this is the first documented case in the literature of multiple, simultaneously occurring volvuli.
Keywords: Volvulus, Multiple volvulus, Triple vovulus, Bowel obstruction, Situs inversus, Colorectal surgery, Colon, Gastric
Case history
A 64-year-old man presented to the emergency department with a 3-day history of abdominal distension and constipation. He was unresponsive and hypothermic but otherwise haemodynamically stable. He had presented one month prior to this with similar obstructive symptoms and had been treated successfully with phosphate enemas for suspected faecal impaction. He required full-time nursing care due to severe vascular dementia but had no other medical issues of note.
Examination findings included a grossly distended abdomen and scrotum with surgical emphysema across the abdomen, pelvis and scrotum. Digital rectal examination showed a short mucosal prolapse, an empty rectum and crepitus on palpation of the bowel wall.
Laboratory tests demonstrated a metabolic acidosis with renal impairment and ongoing inflammation (Table 1). An erect chest x-ray and abdominal x-ray showed a left sided pneumoperitoneum with subcutaneous emphysema (Fig 1) associated with distended small and large bowel loops, suggestive of perforation (Fig 2).
Table 1.
Laboratory test results
| Blood sample | Venous blood gas | ||
| Sodium | 143mmol/l (high) | pH | 7.315 |
| Potassium | 4.9mmol/l | pCO2 | 3.18kPa |
| Urea | 12.2mmol/l (high) | pO2 | 3.42kPa |
| Creatinine | 208ìmol/l (high) | Lactate | 3.1mmol/l |
| C-reactive protein | 33mg/l (high) | HCO3 | 12.3mmol/l |
| Haemoglobin | 10.9g/dl (low) | Base excess | -14.1mmol/l |
| White blood count | 9.5 × 109/l | ||
| Platelet count | 447 × 109/l | ||
Figure 1.

Semi erect chest x-ray showing gastric volvulus (A), caecal volvulus (B), levocardia (C) and liver on left side of abdomen (D)
Figure 2.
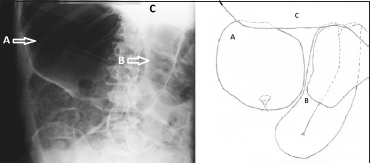
Abdominal x-ray showing gastric volvulus (A), caecal volvulus (B) and liver (c)
Considering the clinical picture and the patient’s comorbidities, it was decided that operative intervention was inappropriate. The patient was made comfortable and passed away in the following hours.
A postmortem examination was carried out. Findings revealed that although all the thoracic structures maintained their normal orientation, the entire upper abdominal visceral organs were located on the opposite side to the expected anatomical position, suggestive of a partial situs inversus. Astonishingly, the postmortem also reported three separate distended volvuli. The stomach was markedly distended and had undergone a 180º twist along a transverse axis, consistent with gastric volvulus. The terminal ileum, caecum and proximal colon were also distended and had undergone a 360º twist, consistent with caecal volvulus, and the sigmoid colon was also distended with another 180º volvulus. No perforation was identified. The examiner concluded that this was death due to natural causes as a result of the multiple volvuli.
On retrospective review of the x-rays, a consultant radiologist noted the abnormal position of the liver, indicating a situs anomaly. He also reported that the bowel patterns may have been suggestive of gastric and caecal volvuli had a diagnosis of situs inversus been suspected previously.
This case is of particular interest as it represents the first documented case of multiple simultaneous gastric and colonic volvuli in the literature. This is of clinical relevance because it highlights the well documented diagnostic pitfalls of situs inversus. In addition, it proves that multiple volvuli can occur simultaneously, which should be considered when managing sigmoid volvulus by sigmoidoscopy and air insufflation. This method fails to directly visualise the abdominal contents and may therefore miss more proximal volvuli.
Literature review
Situs inversus totalis is a rare anomaly in which all the internal viscera are located on the opposite side of the body to their expected location. The documented incidence of complete situs inversus in the literature ranges from 1:35,000 to 1:1,400.1 A rarer anomaly is that of partial situs inversus, in which only isolated parts of the internal viscera are malpositioned. Both anomalies are associated with developmental anomalies of the cardiac and abdominal viscera, and frequently present soon after birth with cardiac compromise or intestinal obstruction.2 A higher incidence of such complications is noted in cases of partial situs inversus. Infrequently, such complications manifest late and present in adult life.
Situs inversus is associated with an increased propensity of the bowel to twist due to the abnormal mobility of bowel segments caused by the improper developmental fusion of the mesentery to the posterior abdominal wall.1,3 Volvulus refers to a situation in which twisting of the bowel around itself or the stalk of mesentery causes an obstruction. This can occur in all mobile segments of bowel attached to a mesentery. If untreated, this may lead to strangulation or perforation with fatal peritonitis. Isolated volvulus is a common associated complication of situs inversus that has been well reported in the literature. However, volvulus characteristically occurs in isolation and, as far as we are aware, it has not been reported in multiple locations simultaneously, even in those patients with an increased propensity such as those with situs inversus.
Figure 3.
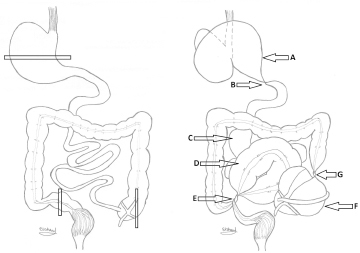
Schematic representation of situs inversus and pattern of volvuli observed at postmortem examination. Left: situs inversus of abdominal viscera. Bars represent axes of rotation. Right: Volvuli observed in this case: dilated gastric volvulus (A), 180º twist (B), dilated small bowel (C), dilated sigmoid volvulus (D), 360º twist (E), caecal volvulus (F) and 360º twist (G)
On x-ray a reflected cardiac shadow, gastric bubble or, as in our case, a liver may suggest a situs anomaly is present although these findings cannot establish the true extent of the anomaly when they occur in isolation. If such findings are found in patients presenting with obstruction, volvuli must always be actively excluded.
The treatment of volvulus depends on the clinical scenario. If strangulation is present, bowel resection is mandatory. In the absence of strangulation, more conservative measures can be adopted. Endoscopic detorsion is frequently attempted for sigmoid volvulus but can also be attempted for gastric volvulus although it is rarely successful (overall success rate 12.5%). More frequently, formal laparotomy and manual detorsion is carried out, usually followed by fixation to prevent recurrence. Procedures in which compromised bowel is resected have significantly lower recurrence rates and avoid reperfusion injuries.1,3–5
Conclusions
We report the first documented case of multiple, simultaneous volvuli of the stomach, caecum and sigmoid colon. This is of particular clinical interest as it is a condition that could lead to significant morbidity if not suspected in patients who are initially managed conservatively for volvuli. This occurred incidentally in a rare patient with partial situs inversus, reminding readers of the known association between situs inversus and volvulus.
References
- 1.Onder A, Okur N, Bülbüloğlu E, Yüzbas¸ioğllu MF. Cecal volvulus in situs inversus totalis accompanied with pancreatic malrotation. Diagn Interv Radiol 2009; 15: 188–192. [PubMed] [Google Scholar]
- 2.Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics 2002; 22: 1,439–1,456. [DOI] [PubMed] [Google Scholar]
- 3.Ringer PH, Killam AR, Davis BA. Situs inversus viscerum associated with intermittent midgut volvulus. South Med J 1982; 75: 620–623. [DOI] [PubMed] [Google Scholar]
- 4.Majeski J. Operative therapy for cecal volvulus combining resection with colopexy. Am J Surg 2005; 189: 211–213. [DOI] [PubMed] [Google Scholar]
- 5.Madiba TE, Thomson SR. The management of cecal volvulus. Dis Colon Rectum 2002; 45: 264–267. [DOI] [PubMed] [Google Scholar]