

Abstract
We describe explosive combustion of a gas filled peritoneum from a handheld electrosurgery electrode used to enter the abdomen. The pneumoperitoneum was due to small bowel perforation and peritonitis had been established for at least two days. No injury was caused to either the patient or medical staff. This rare occurrence has only been described once before. Surgeons should be aware of the possible combustion of bowel gas, whether on opening bowel or the peritoneum after bowel perforation.
Keywords: Pneumoperitoneum, Electrosurgery, Peritonitis
Surgical explosions in the abdomen are rare. Combustion of this nature requires a fuel, an ignition source and may be potentiated by the presence of high dose oxygen.1 Electro-surgery is the most common energy source used in general surgery. However, it is also a potent ignition source. Surgical fires and explosions have been described with electrosurgery using fuels such as alcohol-based skin preparations,2 plastic endoluminal tubes,3 intracolonic gas4 and, rarely, free peritoneal gas following bowel perforation.1 Significant complications or death can ensue as a result of such fires or explosions and surgeons should be aware of these hazards.
Case history
A 41-year-old woman presented to the emergency surgical team with peritonitis. She had been admitted two weeks earlier under a medical team with abdominal pain, diarrhoea and electrolyte disturbances. The cause for this initial presentation remains unknown despite extensive investigation. Two days prior to referral she developed worsening abdominal pain and abdominal distension. An erect plain chest x-ray demonstrated free intraperitoneal air (Fig 1) and she was scheduled for a laparotomy. A midline incision was made using a handheld electrosurgical blade dividing all layers in turn using the device. On dividing the peritoneum, there was an explosion. There appeared to be no injury to either the patient or the medical team as a result of the explosion. The laparotomy demonstrated two small bowel perforations, a grossly contaminated peritoneal cavity, a large volume of pus and small bowel enteral fluid.
Figure 1.
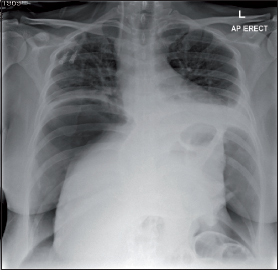
Erect plain chest x-ray demonstrating the presence of free intra-abdominal gas
Discussion
Flammable gases are produced at all levels of the gastrointestinal tract. Hydrogen and methane are the most common flammable gases produced in the bowel. Their proportions will vary with diet, digestion and metabolism.5 Bowel preparation of the colon with mannitol or lactulose is associated with an increase in combustible gas, resulting in explosions during colonic resection caused by electrosurgery.6
Oxygen concentrations in the normal gastrointestinal tract decrease from 10% in the stomach to 5% in the colon and combustible bowel gas will not ignite in less than 5% oxygen. However, during general anaesthesia with supplemental oxygen the concentration of the oxygen in the bowel increases.5 This applies to nitrous oxide as well, which may also aid combustion.7
In our case the most likely fuel causing the explosion on entering the peritoneum was free intraperitoneal bowel gas, ignited by the handheld electrosurgery device. We have found only one similar report.1 Unlike our case, there were extensive intra-abdominal injuries sustained secondary to the explosion. Several case reports have described the ignition of intracolonic gas on directly entering the colon using handheld diathermy.4,8,9 Because of this risk, many surgeons avoid using electrosurgery in this particular situation. We recommend that on entering a peritoneum in which there is free gas, electrosurgery should be avoided and scissors or a scalpel should be used instead.
References
- 1.Dhebri AR, Afify SE. Free gas in the peritoneal cavity: the final hazard of diathermy. Postgrad Med J 2002; 78: 496–497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Briscoe CE, Hill DW, Payne JP. Inflammable antiseptics and theatre fires. Br J Surg 1976; 63: 981–983. [DOI] [PubMed] [Google Scholar]
- 3.Baur DA, Butler RC. Electrocautery-ignited endotracheal tube fire: case report. Br J Oral Maxillofac Surg 1999; 37: 142–143. [DOI] [PubMed] [Google Scholar]
- 4.Shinagawa N, Mizuno H, Shibata Y et al. . Gas explosion during diathermy colotomy. Br J Surg 1985; 72: 306. [DOI] [PubMed] [Google Scholar]
- 5.MacDonald AG. A short history of fires and explosions caused by anaesthetic agents. Br J Anaesth 1994; 72: 710–722. [DOI] [PubMed] [Google Scholar]
- 6.Zanoni CE, Bergamini C, Bertoncini M et al. . Whole-gut lavage for surgery. A case of intraoperative colonic explosion after administration of mannitol. Dis Colon Rectum 1982; 25: 580–581. [DOI] [PubMed] [Google Scholar]
- 7.Robinson JS, Thompson JM, Wood AW. Letter: Laparoscopy explosion hazards with nitrous oxide. BMJ 1975; 3: 764–765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.De Wilt JH, Borel Rinkes IH, Brouwer KJ. Gas explosion during colonic surgery. J R Coll Surg Edinb 1996; 41: 419. [PubMed] [Google Scholar]
- 9.Gross E, Jurim O, Krausz M. Diathermy-induced gas explosion in the intestinal tract. Harefuah 1992; 123: 12–13, 71–72. [PubMed] [Google Scholar]