

Sir,
Ultrasound-guided erector spinae plane (US-ESP) block is a novel analgesic technique, in which local anaesthetic is injected into fascial plane deep to erector spinae muscle. It is possible to block the dorsal and ventral rami of the spinal nerve depending on the level of injection and amount of local anaesthetic injected. The drug spreads in craniocaudal fashion over several levels as the erector spinae fascia extends from nuchal fascia cranially to the sacrum caudally.[1] Forero et al. recently described US-ESP block for thoracic neuropathic pain.[2] This block could be effective in both acute post-operative thoracic and abdominal surgeries and also neuropathic pain in these regions.[3] We report here a series of 5 cases, in which this block was used for post-operative analgesia in patients undergoing modified radical mastectomy. We selected 5 patients of the American Society of Anesthesiologists grade 1 or 2 between age group 35 and 50 years posted for either left or right modified radical mastectomy (MRM). All the patients gave written informed consent for the procedure. Patients were given US-ESP block followed by general anaesthesia. With patients in sitting position depending on the surgical side, left- or right-sided ESP block was given using a high-frequency linear US transducer (Fujifilm Sonosite, Bothwell, USA). The probe was placed in longitudinal orientation lateral to the thoracic fifth spinous process. Then, trapezius, rhomboideus major and erector spinae were identified from the surface [Figure 1]. We deposited 25 ml 0.25% bupivacaine into interfascial plane between rhomboideus major and erector spinae muscle [Figure 1]. After checking for sensory dermatome from 2nd thoracic vertebrae to 8th thoracic vertebrae, general anaesthesia was given to the patient. The intraoperative course was uneventful, and post-operative period, no additional analgesic was given. All the patients were followed post-operatively for 8 h, in which every 2 h pain was rated on 11-point rating by Numerical Rating Scale, patients were asked to circle the number between 0 and 10 (0 no pain and 10 worst pain). Four out of 5 patients had the pain score between 2 and 4 at different time intervals and they did not require any additional analgesia [Table 1]. One patient had pain score 6 when assessed at 4th h and was given rescue analgesia post-operatively [Table 1]. Thus, the results demonstrated that the US-ESP block was able to block the ventral rami of required thoracic spinal nerves providing good pain relief. Compared to paravertebral block (due to close proximity to pleura) and epidural (proximity to spinal cord), this may be considerably safer. Further, MRM involves pectoral muscles supplied by brachial plexus. Hence, any nociceptive input from the brachial plexus may be spared by epidural blocks. As ESP block involves an unhindered craniocaudal spread, and thus may effectively decrease such pain. Further, haemodynamic fluctuations associated with epidural analgesia are not common with ESP blocks. We present this case series to throw light on this useful technique. However, further controlled clinical trials are needed to validate our initial observations.
Figure 1.
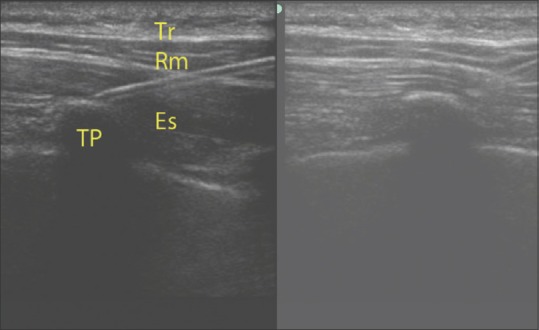
Localisation of the space and drug injection. (Tr-Trapezius, Rm- Rhomboideus major, Er- Erector spinae, TP- Transverse Process)
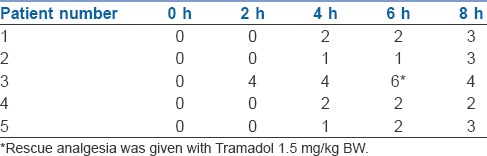
Table 1.
Numerical pain score rating at different time intervals post-operatively
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: Anatomy, function and clinical considerations. J Anat. 2012;221:507–36. doi: 10.1111/j.1469-7580.2012.01511.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: A Novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–7. doi: 10.1097/AAP.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 3.Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: A Report of 3 cases. Reg Anesth Pain Med. 2017;42:372–6. doi: 10.1097/AAP.0000000000000581. [DOI] [PubMed] [Google Scholar]