

Abstract
Age differences in decision-making are of theoretical interest and have important practical implications, but relevant lines of work are distributed across multiple disciplines and often lack integration.
The present review proposes an overarching conceptual framework with the aim of connecting disjointed aspects of this field of research.
The framework builds on process models of decision-making and specifies potential mechanisms behind age effects as well as relevant moderators including task characteristics and contextual factors.
After summarizing the extant literature for each aspect of the framework, compensatory mechanisms and ecological fit among different components of the model are considered.
Implications for real-life decision making, remaining research gaps and directions for future research are discussed.
As population aging extends beyond industrialized nations (https://esa.un.org/unpd/wpp), a better understanding of age differences in decision-making is gaining in importance. Older adults not only make up a growing part of the world’s population, but the societal changes and scientific advances that precipitated population aging further emphasize individual choice. Biomedical breakthroughs have reduced early life mortality from acute diseases, and thus, more people live long enough to develop chronic conditions that require ongoing management (https://cdc.gov). With growing efforts to empower patients (Diefenbach, Miller-Halegoua, & Bowen, 2016), older patients are now more engaged in their medical choices than ever before. Moreover, as active life spans are lengthening, traditional models of retirement are becoming obsolete and older adults are faced with momentous choices about phased retirement, late life career changes, and the management of various sources of retirement income (https://census.gov). Of course, an aging workforce also raises questions about older employees’ ability to make sound choices in occupational settings.
In response, a growing body of research has examined age differences in decision-making (for an overview see Hess, Strough, & Löckenhoff, 2015). However, compared to other areas of the gerontological literature, empirical evidence in this field is relatively disjointed and distributed across multiple disciplines. This makes it difficult to identify broad trends, reconcile seemingly contradictory results, and – most importantly – derive directions for future research and concrete pathways for intervention. The present review builds on previous efforts (e.g., Mata et al., 2012; Peters, Dieckmann, & Weller, 2011; Sanfey & Hastie, 2000) to propose a conceptual framework that integrates different lines of research within the aging and decision-making literature (Figure 1). At its core, the framework builds on process approaches (Einhorn, 1970; Slovic, Fischhoff, & Lichtenstein, 1977; Cox, Granbois, & Summers, 1983) which consider decision-making as a multi-step, recursive process in which people’s evaluations of a given outcome feed into their approach to future decisions.
Figure 1.
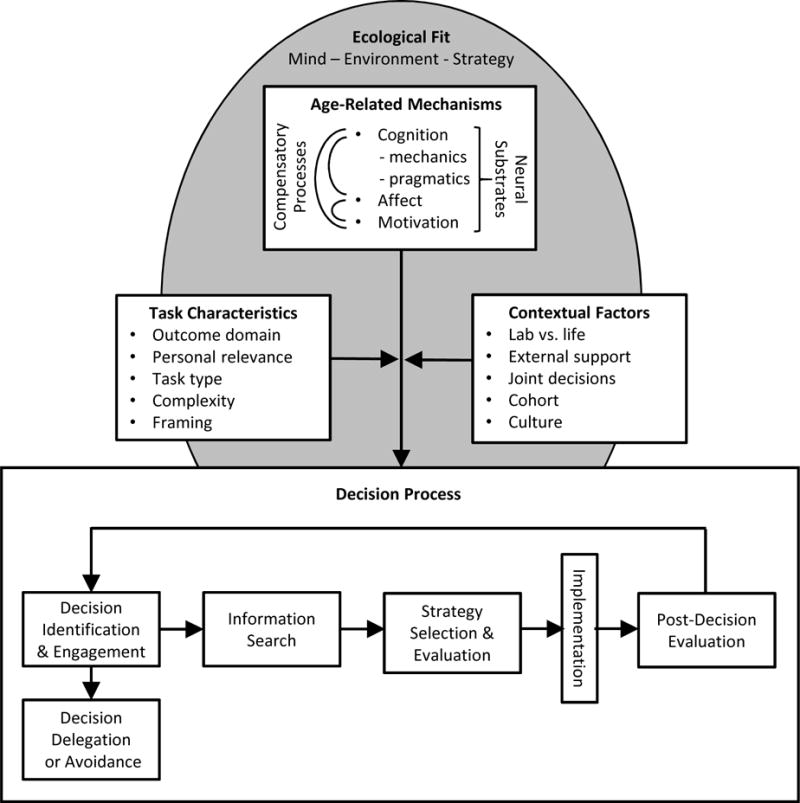
Conceptual framework for mapping age differences in decision making
Regarding potential mechanisms, the framework differentiates among cognitive, affective, and motivational factors along with their underlying neural substrates. In line with dual-process models of decision-making (Peters et al., 2011) this framework acknowledges that the balance between analytical/deliberative and experiential/affect-rich processes may shift with age as decrements in some areas are compensated by others.
Further, following the ecological rationality framework (Mata et al., 2012), age-related changes in decision-making capacities and strategies should not be evaluated in isolation but considered in terms of their relative fit with the structure and contingencies of the surrounding environment. To capture the role of such factors, Figure 1 differentiates between task characteristics (e.g., outcome domain, task type) and contextual factors (e.g., lab vs. life, culture) and highlights the importance of overarching ecological fit.
In the following sections, I consider empirical evidence for each component of this framework, beginning with age differences in specific steps of the decision process and then turning to underlying mechanisms and potential moderators. A comprehensive review of the literature is of course beyond the scope of this brief review. Instead I highlight key papers within each area exemplifying both convergent streams of evidence and apparent contradictions with the goal of reconciling disparate findings and identifying research gaps.
Age Differences in Steps of the Decision Process
Contemporary views of decision-making propose a multi-step, recursive process (Figure 1, bottom) in which each higher-order step entails lower-level choices. Consider ‘Jane’, who is purchasing a new car. First, she identifies the need for a decision to be made (e.g., her old car is starting to show signs of wear) and she chooses to select a new one. Alternatively, she may avoid the decision by postponing her purchase or asking a trusted friend to choose a car for her. Next, Jane begins to search for relevant information and makes decisions on what sources of information to consider (e.g., advertisements, reviews) and when to stop the search. She then employs strategies for evaluating the available information. She may consider one car at a time or compare specific features across several cars at once and she must manage trade-offs between immediate and long-term outcomes (e.g., purchase price vs. maintenance fees) and weigh potential risks (e.g., safety ratings). The process culminates in decision implementation – the actual purchase of the car – followed by post-decision evaluation based on subjective criteria (e.g., driving experience) or objective criteria (e.g., fuel economy). These evaluations, in turn, inform Jane’s future car purchases.
This is, of course, an idealized model. Realistic choices may skip or condense steps and relegate lower-level choices to automatic preferences rather than conscious processing. Laboratory tasks, in turn, tend to isolate specific elements such as information search, strategy selection, temporal trade-offs, or risk taking. Nonetheless, a process approach proves useful in capturing broad trends in aging and decision-making as noticeable age differences found at each step along the way.
For starters, older adults are less likely than their younger counterparts to engage in decision-making in the first place and often bypass the entire process through choice delegation, deferral, or avoidance (Finucane et al., 2002). This tendency appears in both hypothetical laboratory tasks (Chen, Ma, & Pethtel, 2011) and realistic choices (Löckenhoff, Hsiao, Kim, & Swarts, 2016).
Once engaged with a decision, older adults’ information search tends to be less exhaustive than that of younger adults. They prefer to choose among fewer options (Reed, Mikels, & Löckenhoff, 2013), review fewer pieces of information, and often make their decisions more quickly (Mata & Nunes, 2010). Older age is also associated with a preference for personally relevant information (Hess, Queen, & Ennis, 2013), but reduced sensitivity to the sources of information (Cansino et al., 2013).
Once information has been acquired, it needs to be evaluated. In this phase, age differences are seen in both the weight assigned to different characteristics and the strategies used to trade them off against each other. In general, older decision makers favor strategies that are less complex and systematic (Mata, Schooler, & Rieskamp, 2007). For instance, when information is presented in a table, younger adults tend to use alternative-based strategies that trade-off different characteristics within a given option whereas older adults tend to use attribute-based strategies that compare a single characteristic across options (Johnson, 1990). Older adults are also more likely to use heuristic strategies such as satisficing (i.e., choosing the first alternative that meets a given standard, Bruine de Bruin, Parker, & Strough, 2016) and they tend to draw more on their prior experiences and emotional responses than their younger counterparts (Peters et al., 2011, although see Delaney, Strough, Parker, & Bruine de Bruin, 2015). Targeted streams of research have examined how the weighing of specific characteristics varies with age. For instance, studies examining trade-offs between immediate and delayed outcomes suggest that older age is associated with reduced sensitivity for temporal delays (for a review see Löckenhoff & Rutt, 2015). Research on age differences in risk-taking, in turn, indicates that older decision makers are somewhat less willing to take risks than their younger counterparts (Mamerow, Frey, & Mata, 2016), although this pattern is more prominent when trading off risk against certainty as compared to trading off two risky options (Mather et al., 2012; Pachur et al., 2017). However, within each of these research streams, there is significant heterogeneity across domains and paradigms, indicating a role of moderating factors to which we return below.
The eventual implementation of a decision is followed by post-decisional evaluation. From a subjective point of view, there is converging evidence that older adults consider their past choices more favorably than younger adults: They report higher post-decisional satisfaction (Löckenhoff & Carstensen, 2008) and lower regret (Brassen, Gamer, Peters, Gluth, & Buchel, 2012). This has raised concerns that older adults may be less able to learn from poor decisions, especially when outcomes are ambiguous (e.g., Delpero et al., 2015). Thus, the feedback loop to incorporate past decision outcomes into future choices may be less pronounced with age.
Research on objective decision quality, in turn, is surprisingly equivocal. In part, this is due to difficulties in defining the ‘best choice’ in realistic decision scenarios. In health-care settings, for example, the optimal course of action may vary depending on age and physical health of the patient (Löckenhoff et al., 2016). However, even standardized scenarios show significant heterogeneity, which suggests that age differences in decision quality depend on the specific types of processing required. In the following section, we consider such mechanisms in more detail.
Potential Mechanisms behind Age Effects
Cognition
Age differences in cognitive abilities have long been considered as the primary factor behind age-related variations in decision strategies and outcomes (e.g., Sanfey & Hastie, 2000). Over the decades, however, the field has shifted from a one-sided emphasis on age-related limitations towards a more differentiated understanding. Perhaps most importantly, one must distinguish between steep cognitive decrements associated with dementia and terminal decline (Gerstorf, Ram, Hoppmann, Willis, & Schaie, 2011), which severely limit decision-making abilities and more subtle effects of healthy aging (Salthouse, 2010), which are the focus of the present review. Within this realm, one may further differentiate between deliberative, resource-intensive processes associated with acquiring and manipulating novel information (i.e., cognitive mechanics or fluid intelligence) and experience-based, intuitive processes that govern much of our everyday functioning (i.e., cognitive pragmatics or crystallized intelligence, Peters et al., 2011).
With regard to cognitive mechanics, decades of research have documented significant age-related declines in processing speed and working memory (Salthouse, 2010) which may impose limits on pre-decisional information-gathering and impair strategies that require multiple simultaneous comparisons. Moreover, age decrements in inhibition (Butler & Zacks, 2006) may increase the intrusion of task-irrelevant information and bias decision-makers towards default responses. More broadly, limitations in executive functioning may hinder the strategic allocation of resources across different components of a task (Salthouse, 2010). In combination, these effects are likely to impair older adults’ performance in complex decision scenarios, especially if time is limited and relevant/irrelevant information is intermingled. In some contexts, however, decrements in deliberate processing may benefit decision quality. Limited working memory, for example, may facilitate the identification of certain associations (Healey & Hasher, 2009), although support for this ‘deficit attenuation hypothesis’ is limited to specific task contexts.
Research on cognitive pragmatics, in turn, has documented that experience-based skills and generalized world knowledge continue to accumulate over the life span and remain largely intact during healthy aging (Salthouse, 2010). Thus, older adults may be able to maintain sound decision-making by drawing on domain-specific knowledge and expertise (Li et al., 2015). Moreover, as decision-makers become experts in an area, they shift from analytical, exhaustive decision styles to heuristic, rule-based styles that entail a lower cognitive load (Reyna & Brainerd, 2011; Pachur & Marinello, 2013). In combination, leveraging prior experience and utilizing heuristic strategies are likely to benefit older adults’ decision quality (Queen, Hess, Ennis, Dowd, & Grühn, 2012). There are, however, some important caveats. The benefits of crystallized knowledge are most relevant in familiar scenarios, and because of age decrements in source memory (Cansino et al., 2013), older decision makers may not always be sure whether a given piece of information is applicable to a certain context. Some knowledge domains, such as health-care contexts, also experience rapid knowledge turnover, which may render some aspects of prior knowledge obsolete. Further, although heuristic approaches economize cognitive effort, they can give rise to systematic biases (Strough, Karns, & Schlosnagle, 2011). It is therefore reassuring to note that older adults do not apply heuristics indiscriminately. Instead, age effects vary across types of heuristics and appear to be driven by factors beyond cognitive aging including emotional and motivational constructs (Strough et al., 2011).
Emotion
Dual process models of decision-making acknowledge that any decision that is worth making hinges not only on ‘cold’ cognitive reasoning but also on ‘hot’ emotional aspects (Peters et al., 2011). The latter can be further differentiated into incidental affect (i.e., decision-independent mood states) and integral affect (i.e., affective responses to decision alternatives). Some decisions may also elicit trade-off aversion which is associated with challenging aspects of the decision process itself, rather than specific decision outcomes (Luce, 2005). Optimal choices require decision-makers to balance ‘hot’ and ‘cold’ reasoning and downregulate incidental affect and trade-off aversion to focus on integral affect.
Research on emotional aging suggests that – in some respects – older adults may be better prepared for these challenges than their younger counterparts. Mental health and emotional well-being remain fairly stable in healthy aging (Ong & Löckenhoff, 2016), and emotion-regulatory strategies show an age-related shift from response-focused strategies that downregulate aversive emotions after they occur to antecedent-focused strategies that proactively avoid them (Urry & Gross, 2010). Affective forecasting, the ability to anticipate one’s future emotions, is also well preserved, and emotionally salient task content appears to be selectively spared from age-related cognitive decrements in fluid cognition (Isaacowitz & Livingstone, 2015). These trends in emotional aging may boost older adults’ decision quality. Positive mood, for example, facilitates the downregulation of task-irrelevant affect and fosters creativity (Isen & Labroo, 2003), and accurate affective forecasting may forestall short-sighted decisions and limit post-decisional regret (Brassen et al, 2012). Moreover, older adults may utilize the so-called ‘affect heuristic’ and leverage the integral affect elicited by different decision options to augment more deliberative forms of processing (Mikels et al., 2010).
However, the age-related emphasis on emotions also raises concerns about potential biases. Numerous studies have documented an age-related preference for positive over negative material, and this ‘positivity effect’ (Reed & Carstensen, 2012) extends to the decision process (Löckenhoff & Carstensen, 2008; Pachur et al., 2017). Conceivably, this could limit older adults’ consideration of negatively valenced characteristics that are nonetheless crucial to many choices and lead them to evaluate their past choices as overly positive which could forestall future learning.
To appreciate the influence of emotional aging on decision-making, a better understanding of the underlying mechanisms is required (for a review see Mikels, Reed, Hardy, & Löckenhoff, 2014). Although some have suggested that the positivity effect is due to cognitive limitations, older adults with high cognitive functioning are actually more, not less likely to show the effect (Mather & Knight, 2005). Moreover, there is evidence for age-associated changes in motivational priorities that allow older adults to flexibly adjust decision-making strategies based on priorities and task demands (Mikels et al., 2014).
Motivation
Life span theory (Baltes, Lindenberger, & Staudinger, 1998), a prominent meta-theoretical perspective on adult development, notes that later life is characterized by a preponderance of losses over gains. As a result, motivational priorities are thought to shift with age from promotion and growth towards maintenance and loss prevention (Freund, Hennecke, & Mustafić, 2012). Moreover, older adults appear to reorient from an emphasis on outcomes (which may be increasingly out of reach in later life) towards the processes or means of goal pursuit (Freund et al., 2012). In the context of decision-making, the proposed shift from promotion to prevention maps well onto the age-related tendency to prefer certainty over risk (Mather et al., 2012). A greater focus on decision processing (as opposed to outcomes), may also explain why older adults are more sensitive to emotionally challenging trade-offs (Chen et al., 2011).
Life-span theory further proposes that older adults maintain high functioning by engaging in selective optimization with compensation (SOC), a process by which individuals select personally relevant areas of functioning and optimize them through targeted allocation of resources while compensating for age-related losses in other areas (Baltes et al., 1998). Consistent with processes of selection and optimization, older adults were found to expend greater effort in judgment and reasoning tasks when personal relevance is high (Hess et al., 2013). The age-related tendency towards decision delegation (Finucane et al., 2002), in turn, may reflect compensatory processes for non-essential types of decisions.
Beyond age-related losses, shifts in time horizons may affect decision-making as well (for a review see Löckenhoff & Rutt, 2015). According to socioemotional selectivity theory (SST, Carstensen, 2006), limitations in time perspective lead to a reallocation of goal priorities from future-oriented goals such as information seeking and network building to present-oriented goals aimed at strengthening social ties and savoring the present moment. In the context of decision-making, limitations in future horizons have been linked to a prioritization of positive information (Löckenhoff & Carstensen, 2008) and lower susceptibility towards certain decision biases such as the sunk cost fallacy (Strough, Schlosnagle, Karns, Lemaster, & Pichayayothin, 2014). Older age is also linked to a greater sense of continuity with past and future selves, which may account for age-related improvements in affective forecasting and the reduced tendency to discount future outcomes (Löckenhoff & Rutt, 2017).
Neural substrates
Taken together, research on the mechanisms behind age differences in decision-making paints a complex picture in which changes in deliberative and experiential resources interact with affective and motivational factors. Over the last two decades, rapid advances in imaging techniques have begun to yield insights into the neurobiological bases of such effects.
Mirroring trends in behavioral research, inquiries into the neural substrates of age differences in decision-making branched out from an initial focus on medial temporal and lateral regions, implicated in cognitive processes such as attention and memory aging, to prefrontal regions associated with executive functioning, frontostriatal pathways associated with the processing of rewards, and limbic regions associated with affective processing, to highlight just a few recent advances (Hess et al., 2015). Figure 1 reflects these developments by acknowledging the role of neural substrates not just for cognition but also for affect and motivation.
These inquiries have offered critical new insights, such as evidence for age-related variations in the neural representation of rewards (Samanez-Larkin & Knutson, 2015). However, our understanding of the neurobiological substrates of age differences in decision-making still remains much more advanced with regard to cognitive components as compared to motivational and affective factors. To date, little is known about the neural signatures behind active compensatory processes such as SOC and the age-related shifts towards heuristic, affect-rich, and experiential processing that are implicated by behavioral findings. To map such dynamics, we need to move beyond the present focus on specific brain regions towards age-related changes in decision-relevant brain networks (e.g., dorsal attention and frontoparietal control networks) as well as the coupling across different networks (Turner & Spreng, 2015). In conducting this work, it will be critical to control for relevant task characteristics and contextual factors that were found to moderate age differences in decision-making.
Moderating Factors
Task Characteristics
Perhaps the most ‘consistent’ finding about aging and decision-making is the dependence of age patterns on specific task characteristics. Typically, age differences are attenuated for scenarios that are high in personal relevance, most likely because – consistent with the SOC framework – older adults are more willing to expend effort in such scenarios (Hess et al., 2013).
Age effects also vary across domains. For instance, older adults tend to be more patient than younger adults in waiting for delayed outcomes in the monetary domain (Löckenhoff & Rutt, 2015), but less patient in the health and interpersonal domain (Seaman et al., 2016). This age-related emphasis on health and social contact is consistent with SST (Carstensen, 2006) which proposes that limitations in future time lead older adults to optimize well-being in the present moment. In some cases, personal relevance and decision domains may also interact with each other. English and Carstensen (2015) for example, found that the age-related positivity effect in pre-decisional information search was attenuated in the health domain relative to the consumer and interpersonal domain, but only among older adults in poor health for whom the stakes were higher.
Even within a given domain, decision outcomes depend on the degree of fit among aging minds, strategy use, and task characteristics (see Figure 1). Consistent with age decrements in fluid cognitive resources, for example, age effects are more pronounced for task components with higher computational demands and time pressure (Mata et al., 2007). Further, consistent with age trends in motivation, responses to task frames vary by age with older adults showing greater sensitivity to frames that emphasize positive over negative information, gains over losses, and emotional meaning in the present over preparation for a distant future (for a review see Strough, de Bruin, & Peters, 2015). Such findings highlight the importance of judicious research practices to track relevant task characteristics and examine their relative consequences for younger and older decision-makers.
Contextual Factors
Beyond task characteristics, a comprehensive understanding of aging and decision-making must acknowledge the role of context. A broad distinction can be drawn between laboratory versus real-life contexts. Although laboratory studies are important because they allow for the systematic manipulation of task characteristics and the thorough tracking of mechanisms, they tend to rely on hypothetical outcomes that are not likely to elicit maximum effort from resource-constrained older adults (Hess et al., 2015). Realistic settings, in turn, involve consequential outcomes, but their richness makes them challenging to study. Moreover, the predominant choices that people face may vary across the life span, and – aside from rare cases where decisions can be studied ‘in action’ – research on real-life decisions often relies on self-reports that may be subject to age-related positivity effects or memory biases.
Real-life decisions are also more likely to be embedded in a social context. The degree of other’s involvement can be mapped along a continuum ranging from fully autonomous choices to joint decisions incorporating advice from others to full delegation of a choice to another person (Sharma et al., 2011). As noted previously, evidence suggests that younger adults’ decisions are closer to the autonomous end of this continuum whereas older adults show a tendency towards delegation. In part, this may reflect attempts to regulate decision-related affect or manage limited cognitive resources. However, at least in the medical domain, older patients may also be discouraged by physicians and other stakeholders from taking an active role (Löckenhoff et al., 2016). Confidants and family members play a key role in older adults’ choices as well, and the age-related emphasis on emotionally meaningful relationships (Carstensen, 2006) may make older adults particularly responsive to the wishes of close others. To date, systematic research on dyadic choices among aging couples or among adult children and their aging parents is missing and further research is required before general conclusions can be drawn (for a review see Queen, Berg, & Lowrance, 2015).
More broadly, research on aging and decision-making would benefit from a systematic consideration of historical context and cohort differences. Because the field has relied predominantly on cross-sectional designs, it can be difficult to disentangle the effects of birth cohort and chronological age. In the healthcare domain, for instance, pre-WWII cohorts were socialized to defer to physician’s authority, whereas baby boomers and their offspring emphasize active involvement and individual choice (Diefenbach et al., 2016). As the medical field shifts towards shared decision-making, the passive stance among current cohorts of older patients may not extend to future generations.
Finally, the field needs to consider the role of cultural context. Culturally shared beliefs about aging often take the form of generalized stereotypes that neglect individual variations and do not accurately reflect reality. Although there is some degree of cross-cultural variation, older adults around the world are perceived to have lower physical and cognitive resources than younger adults (Löckenhoff et al., 2009). Culture also determines what kinds of behavior are seen as ‘appropriate’ for older adults within a given society (Löckenhoff et al., 2009). In combination, cultural norms and aging stereotypes may affect decision-making: First, they may skew older adults’ decision preferences towards options seen as age-appropriate (e.g., in healthcare or consumer choices). Second, the implicit activation of negative age stereotypes may interfere with older adults’ cognitive performance by drawing resources away from the task at hand, an effect known as “stereotype threat” (Lamont, Swift, & Abrams, 2015). Finally, aging stereotypes among collaborators in the decision process may inhibit effective communication and lead to a disregard of older adults’ input (Löckenhoff et al., 2016).
Conclusion
Taken together, this review reveals a complex picture highlighting both strengths and weaknesses of older decision makers and implicating a host of mechanisms that likely contribute to age-related variations in people’s choices. Importantly, such mechanisms may manifest themselves in different ways along the decision-making process and they may interact with each other to amplify or attenuate each other’s consequences. A key dynamic involves age decrements in core decision-making resources (e.g, fluid cognitive processing), compensatory processes (as described by the SOC framework and other motivational accounts), and life-long growth in areas such as experience and emotional processing. Furthermore, the size and direction of age effects depends on the presence of moderating factors as well as the specific context in which a decision is made. The proposed conceptual frameworks (Figure 1) captures key elements in this rich body of work, outlines their relation to each other, and thus sets the stage for evaluating the adaptive fit among mind, environment, and strategy, as outlined in the ecological rationality perspective (Mata et al., 2012).
Of course, the inherent breadth of this framework goes well beyond the scope of being implemented in a single study. Instead, it is meant to encourage researchers to situate their lines of work within the broader context of the field in order to identify related work, consider alternative mechanisms, and at least control (if not experimentally manipulate) relevant task characteristics and contextual factors. The benefits of an integrative approach are exemplified in recent work by Pachur et al. (2017) which disentangled cognitive and motivational factors during age differences in risky choice and found that the relative role of these factors varied for the gain versus loss domains, thus reconciling some of the apparent discrepancies in the prior literature.
Mapping existing research and theories onto this framework will also facilitate the identification of research gaps. Regarding the decision process, for example, much is known about age differences in information search and strategy selection, whereas decision identification and engagement, post-decisional evaluation, and learning during sequential choices are relatively poorly understood. Similarly, with regard to outcome domains, there is a disproportionate emphasis on hypothetical monetary, health, and consumer choices with a relative neglect for other domains, most notably interpersonal choices. Ultimately, the framework encourages the development of more integrative theoretical accounts that span across multiple components and mechanisms to obtain a differentiated understanding of how we shift (or maintain!) our approach to life’s choices as we age.
Acknowledgments
Preparation of this article was supported, in part, by the Edward R. Roybal Centers for Translation of the Behavioral and Social Sciences of Aging (P30AG022845).
References
- Baltes PB, Lindenberger U, Staudinger UM. Life-span theory in developmental psychology. In: Damon W, Lerner RM, Damon W, Lerner RM, editors. Handbook of child psychology: Theoretical models of human development. 5th. Vol. 1. Hoboken, NJ, US: John Wiley & Sons Inc.; 1998. pp. 1029–1143. [Google Scholar]
- Brassen S, Gamer M, Peters J, Gluth S, Buchel C. Don’t Look Back in Anger! Responsiveness to Missed Chances in Successful and Nonsuccessful Aging. Science. 2012;336(6081):612–614. doi: 10.1126/science.1217516. [DOI] [PubMed] [Google Scholar]
- Bruine de Bruin W, Parker AM, Strough J. Choosing to be happy? Age differences in ‘maximizing’ decision strategies and experienced emotional well-being. Psychology and Aging. 2016;31(3):295–300. doi: 10.1037/pag0000073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler KM, Zacks RT. Age deficits in the control of prepotent responses: Evidence for an inhibitory decline. Psychology and Aging. 2006;21(3):638–643. doi: 10.1037/0882-7974.21.3.638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cansino S, Estrada-Manilla C, Hernández-Ramos E, Martínez-Galindo JG, Torres-Trejo F, Gómez-Fernández T, Rodríguez-Ortiz MD. The rate of source memory decline across the adult life span. Developmental Psychology. 2013;49(5):973–985. doi: 10.1037/a0028894. [DOI] [PubMed] [Google Scholar]
- Carstensen LL. The influence of a sense of time on human development. Science. 2006;312(5782):1913–1915. doi: 10.1126/science.1127488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen YW, Ma XD, Pethtel O. Age Differences in Trade-Off Decisions: Older Adults Prefer Choice Deferral. Psychology and Aging. 2011;26(2):269–273. doi: 10.1037/a0021582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox A, Granbois DH, Summers J. Planning, search, certainty and satisfaction among durables buyers: a longitudinal study. Advances in Consumer Research. 1983;10:394–399. [Google Scholar]
- Delaney R, Strough J, Parker AM, Bruine de Bruin W. Variations in decision-making profiles by age and gender: A cluster-analytic approach. Personality and Individual Differences. 2015;85:19–24. doi: 10.1016/j.paid.2015.04.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delpero C, Mioni G, Rubio JL, Juárez Ramos V, Gómez Milán E, Stablum F. Decision-making and feedback sensitivity: A comparison between older and younger adults. Journal of Cognitive Psychology. 2015;27(7):882–897. doi: 10.1080/20445911.2015.1036759. [DOI] [Google Scholar]
- Diefenbach MA, Miller-Halegoua S, Bowen D, editors. Handbook of health decision science. New York: Springer; 2016. [Google Scholar]
- Einhorn HJ. The use of non-linear, non-compensatory models in decision making. Psychological Bulletin. 1970;73(3):221–230. doi: 10.1037/h0028695. [DOI] [PubMed] [Google Scholar]
- English T, Carstensen LL. Does positivity operate when the stakes are high? Health status and decision making among older adults. Psychology and Aging. 2015;30(2):348–355. doi: 10.1037/a0039121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finucane ML, Slovic P, Hibbard JH, Peters E, Mertz CK, MacGregor DG. Aging and decision-making competence: An analysis of comprehension and consistency skills in older versus younger adults considering health-plan options. Journal of Behavioral Decision Making. 2002;15(2):141–164. doi: 10.1002/bdm.407. [DOI] [Google Scholar]
- Freund AM, Hennecke M, Mustafić M. On gains and losses, means and ends: Goal orientation and goal focus across adulthood. In: Ryan RM, Ryan RM, editors. The Oxford handbook of human motivation. New York, NY, US: Oxford University Press; 2012. pp. 280–300. [Google Scholar]
- Gerstorf D, Ram N, Hoppmann C, Willis SL, Schaie KW. Cohort differences in cognitive aging and terminal decline in the Seattle Longitudinal Study. Developmental Psychology. 2011;47(4):1026–1041. doi: 10.1037/a0023426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Healey MK, Hasher L. Limitations to the deficit attenuation hypothesis: Aging and decision making. Journal of Consumer Psychology. 2009;19(1):17–22. doi: 10.1016/j.jcps.2008.12.003. [DOI] [Google Scholar]
- Hess TM, Queen TL, Ennis GE. Age and self-relevance effects on information search during decision making. The Journals of Gerontology: Series B: Psychological Sciences and Social Sciences. 2013;68(5):703–711. doi: 10.1093/geronb/gbs108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hess TM, Strough J, Löckenhoff CE, editors. Aging and decision making: Empirical and applied perspectives. New York: Elsevier Academic Press; 2015. [Google Scholar]
- Isaacowitz DM, Livingstone K. Emotion in adulthood: What changes and why? In: Reynolds KJ, Branscombe NR, Reynolds KJ, Branscombe NR, editors. Psychology of change: Life contexts, experiences, and identities. New York, NY, US: Psychology Press; 2015. pp. 116–132. [Google Scholar]
- Isen AM, Labroo AA. Some ways in which positive affect facilitates decision making and judgment. In: Schneider SL, Shanteau J, editors. Emerging perspectives on judgment and decision research. New York, NY US: Cambridge University Press; 2003. pp. 365–393. [Google Scholar]
- Johnson MM. Age differences in decision making: A process methodology for examining strategic information processing. Journals of Gerontology. 1990;45(2):P75–P78. doi: 10.1093/geronj/45.2.p75. [DOI] [PubMed] [Google Scholar]
- Lamont RA, Swift HJ, Abrams D. A review and meta-analysis of age-based stereotype threat: Negative stereotypes, not facts, do the damage. Psychology and Aging. 2015;30(1):180–193. doi: 10.1037/a0038586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li Y, Gao J, Enkavi AZ, Zaval L, Weber EU, Johnson EJ. Sound credit scores and financial decisions despite cognitive aging. Proceedings of the National Academy of Sciences. 2015;112(1):65–69. doi: 10.1073/pnas.1413570112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Löckenhoff CE, Carstensen LL. Decision strategies in health care choices for self and others: Older but not younger adults make adjustments for the age of the decision target. Journals of Gerontology Series B-Psychological Sciences and Social Sciences. 2008;63(2):P106–P109. doi: 10.1093/geronb/63.2.p106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Löckenhoff CE, De Fruyt F, Terracciano A, McCrae RR, De Bolle M, Costa PT, Yik M. Perceptions of Aging Across 26 Cultures and Their Culture-Level Associates. Psychology and Aging. 2009;24(4):941–954. doi: 10.1037/a0016901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Löckenhoff CE, Hsiao C, Kim J, Swarts K. Adult age differences in health-related decision making: A primer. In: Diefenbach M, Miller-Halegoua S, Bowen D, editors. Handbook of health decision science. New York: Springer; 2016. pp. 157–170. [Google Scholar]
- Löckenhoff CE, Rutt JL. Age differences in time perception and their implications for decision making across the life span. In: Hess TM, Strough J, Löckenhoff CE, editors. Aging and decision making: Empirical and applied perspectives. London, UK: Academic Press/Elsevier; 2015. [Google Scholar]
- Löckenhoff CE, Rutt JL. Age Differences in Self-Continuity: Converging Evidence and Directions for Future Research. The Gerontologist. 2017;57(3):396–408. doi: 10.1093/geront/gnx010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luce MF. Decision making as coping. Health Psychology. 2005;24(4):S23–S28. doi: 10.1037/0278-6133.24.4.s23. [DOI] [PubMed] [Google Scholar]
- Mamerow L, Frey R, Mata R. Risk taking across the life span: A comparison of self-report and behavioral measures of risk taking. Psychology and Aging. 2016;31(7):711–723. doi: 10.1037/pag0000124. [DOI] [PubMed] [Google Scholar]
- Mata R, Nunes L. When less is enough: Cognitive aging, information search, and decision quality in consumer choice. Psychology and Aging. 2010;25(2):289–298. doi: 10.1037/a0017927. [DOI] [PubMed] [Google Scholar]
- Mata R, Pachur T, Von Helversen B, Hertwig R, Rieskamp J, Schooler JW. Ecological rationality: A framework for understanding and aiding the aging decision maker. Frontiers in neuroscience. 2012;6(19):1–6. doi: 10.3389/fnins.2012.00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mata R, Schooler LJ, Rieskamp J. The aging decision maker: Cognitive aging and the adaptive selection of decision strategies. Psychology and Aging. 2007;22(4):796–810. doi: 10.1037/0882-7974.22.4.796. [DOI] [PubMed] [Google Scholar]
- Mather M, Knight M. Goal-directed memory: The role of cognitive control in older adults’ emotional memory. Psychology and Aging. 2005;20(4):554–570. doi: 10.1037/0882-7974.20.4.554. [DOI] [PubMed] [Google Scholar]
- Mather M, Mazar N, Gorlick MA, Lighthall NR, Burgeno J, Schoeke A, Ariely D. Risk Preferences and Aging: The “Certainty Effect” in Older Adults’ Decision Making. Psychology and Aging. 2012;27(4):801–816. doi: 10.1037/a0030174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mikels JA, Löckenhoff CE, Maglio SJ, Carstensen LL, Goldstein MK, Garber A. Following Your Heart or Your Head: Focusing on Emotions Versus Information Differentially Influences the Decisions of Younger and Older Adults. Journal of Experimental Psychology-Applied. 2010;16(1):87–95. doi: 10.1037/a0018500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mikels JA, Reed AE, Hardy LN, Löckenhoff CE. Positive emotions across the adult life span. In: Tugade M, Shiota MN, Kirby L, editors. Handbook of Positive Emotions. New York: Guilford Press; 2014. pp. 256–272. [Google Scholar]
- Ong AD, Löckenhoff CE, editors. Emotion, aging, and health. Washington, DC: American Psychological Association; 2016. [Google Scholar]
- Pachur T, Marinello G. Expert intuitions: How to model the decision strategies of airport customs officers? Acta Psychologica. 2013;144(1):97–103. doi: 10.1016/j.actpsy.2013.05.003. [DOI] [PubMed] [Google Scholar]
- Pachur T, Mata R, Hertwig R. Who dares, who errs? Disentangling cognitive and motivational roots of age differences in decisions under risk. Psychological Science. 2017;28(4):504–518. doi: 10.1177/0956797616687729. [DOI] [PubMed] [Google Scholar]
- Peters E, Dieckmann NF, Weller J. Age differences in complex decision making. In: Schaie KW, Willis SL, editors. Handbook of the psychology of aging. Elsevier; 2011. pp. 133–151. [Google Scholar]
- Queen TL, Berg CA, Lowrance W. A framework for decision making in couples across adulthood. In: Hess TM, Strough J, Löckenhoff CE, Hess TM, Strough J, Löckenhoff CE, editors. Aging and decision making: Empirical and applied perspectives. San Diego, CA, US: Elsevier Academic Press; 2015. pp. 371–392. [Google Scholar]
- Queen TL, Hess TM, Ennis GE, Dowd K, Grühn D. Information search and decision making: Effects of age and complexity on strategy use. Psychology and Aging. 2012;27(4):817–824. doi: 10.1037/a0028744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reed A, Mikels J, Löckenhoff CE. Preferences for choice across adulthood: Age trajectories and potential mechanisms. Psychology and Aging. 2013;28(3):625–632. doi: 10.1037/a0031399. [DOI] [PubMed] [Google Scholar]
- Reed AE, Carstensen LL. The theory behind the age-related positivity effect. Frontiers in psychology. 2012;3 doi: 10.3389/fpsyg.2012.00339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reyna VF, Brainerd CJ. Dual processes in decision making and developmental neuroscience: A fuzzy-trace model. Developmental Review. 2011;31(2-3):180–206. doi: 10.1016/j.dr.2011.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salthouse TA. Major issues in cognitive aging. Vol. 49. New York, NY US: Oxford University Press; 2010. [Google Scholar]
- Samanez-Larkin GR, Knutson B. Decision making in the ageing brain: Changes in affective and motivational circuits. Nature Reviews Neuroscience. 2015;16(5):278–289. doi: 10.1038/nrn3917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanfey AG, Hastie R. Judgment and decision making across the adult life span: A tutorial review of psychological research. In: Park DC, Schwarz N, editors. Cognitive aging: A primer. New York, NY US: Psychology Press; 2000. pp. 253–273. [Google Scholar]
- Seaman KL, Gorlick MA, Vekaria KM, Hsu M, Zald DH, Samanez-Larkin GR. Adult age differences in decision making across domains: Increased discounting of social and health-related rewards. Psychology and Aging. 2016;31(7):737–746. doi: 10.1037/pag0000131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharma RK, Hughes MT, Nolan MT, Tudor C, Kub J, Terry PB, Sulmasy DP. Family Understanding of Seriously-ill Patient Preferences for Family Involvement in Healthcare Decision Making. Journal of General Internal Medicine. 2011;26(8):881–886. doi: 10.1007/s11606-011-1717-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slovic P, Fischhoff B, Lichtenstein S. Behavioral decision theory. Annual Review of Psychology. 1977;28:1–39. [Google Scholar]
- Strough J, de Bruin WB, Peters E. New perspectives for motivating better decisions in older adults. Frontiers in psychology. 2015;6:783. doi: 10.3389/fpsyg.2015.00783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strough J, Karns TE, Schlosnagle L. Decision-making heuristics and biases across the life span. In: SamanezLarkin GR, editor. Decision Making over the Life Span. Vol. 1235. 2011. pp. 57–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strough J, Schlosnagle L, Karns T, Lemaster P, Pichayayothin N. No Time to Waste: Restricting Life-Span Temporal Horizons Decreases the Sunk-Cost Fallacy. Journal of Behavioral Decision Making. 2014;27(1):78–94. doi: 10.1002/bdm.1781. [DOI] [Google Scholar]
- Turner GR, Spreng RN. Prefrontal engagement and reduced default network suppression co-occur and are dynamically coupled in older adults: The default–executive coupling hypothesis of aging. Journal of Cognitive Neuroscience. 2015;27(12):2462–2476. doi: 10.1162/jocn_a_00869. [DOI] [PubMed] [Google Scholar]
- Urry HL, Gross JJ. Emotion regulation in older age. Current Directions in Psychological Science. 2010;19(6):352–357. doi: 10.1177/0963721410388395. [DOI] [Google Scholar]