

Abstract
Desmopressin increases endogenous factor VIII levels in hemophilia A. Large inter-individual variation in the response to desmopressin is observed. Patients with a lower baseline factor VIII activity tend to show a reduced response, therefore, desmopressin is less frequently used in moderate hemophilia A patients (baseline factor VIII activity 1-5 international units/deciliter), even though factor VIII levels may rise substantially in some of them. We aim to describe the response to desmopressin in moderate hemophilia A patients and to identify predictors. We selected data on 169 patients with moderate hemophilia from the multicenter Response to DDAVP In non-severe hemophilia A patients: in Search for dEterminants (RISE) cohort study. Adequate response to desmopressin was defined as a peak factor VIII level ≥ 30, and excellent response as ≥ 50 international units/deciliter after desmopressin administration. We used univariate and multiple linear regression techniques to analyze predictors of the peak factor VIII level. Response was considered adequate in 68 patients (40%), of whom 25 showed excellent response (15%). Intravenous administration, age, pre-desmopressin factor VIII activity and von Willebrand factor antigen, peak von Willebrand factor activity and desmopressin-induced rise in von Willebrand factor antigen were significant predictors of peak factor VIII level and explained 65% of the inter-individual variation. In 40% of moderate hemophilia A patients, desmopressin response was adequate, thus it is important not to with-hold this group of patients from desmopressin responsiveness. Among the six predictors that we identified for desmopressin-induced factor VIII rise, factor VIII activity and desmopressin-induced rise in von Willebrand factor antigen had the strongest effect.
Introduction
Hemophilia A (HA) is a hereditary clotting disease caused by mutations in the F8 gene, leading to a deficiency of clotting factor VIII (FVIII) that occurs in one out of 5,000 men. Patients are classified based on residual levels of FVIII activity (FVIII:C). Severe patients have no detectable FVIII:C, non-severe patients have some activity (moderate FVIII:C 1-5 and mild 6-40 IU/dL).
Severe and moderate HA patients are generally treated with FVIII concentrates, whereas most mild HA patients may be successfully treated with 1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP) for minor injuries or procedures. Using DDAVP, and thereby avoiding FVIII concentrates, has two important advantages: depending on the country, DDAVP is much cheaper than FVIII concentrate, and DDAVP does not carry the risk of inhibitor development associated with the use of exogenous (allogeneic) sources of FVIII present in concentrates.1–3
DDAVP is a synthetic vasopressin analogue and can be administered intravenously, subcutaneously or intranasally. The drug increases endogenous FVIII plasma concentrations by an average of three- to five-fold by inducing the release of von Willebrand factor (VWF), the carrier protein of FVIII, and the direct release of FVIII from Weibel-Palade bodies (WPBs) in endothelial cells.4,5 FVIII is primarily synthesized in liver sinusoidal endothelial cells.6 Extrahepatic FVIII is believed to be made by cells in the spleen, by lymphatic tissue, and especially by endothelial cells.7–11 The effect of DDAVP is dependent on the vasopressin type 2 receptor which is highly expressed in lung endothelial cells, but not in other populations of vascular endothelial cells.12 It is currently unknown from which sites FVIII and VWF are released upon DDAVP stimulation. Interestingly, liver transplantation in HA patients eliminates DDAVP response for FVIII but not for VWF, suggesting that extrahepatic FVIII synthesis may be necessary for DDAVP response.13
Large inter-individual variation in the response to DDAVP is observed. The variability of biological response within the same individual is smaller than between individuals.14 Although the relative increase in VWF and FVIII levels may be similar between non-severe HA patients, as moderates start at a much lower baseline FVIII:C, they may not reach a sufficient peak FVIII level to allow for treatment of minor procedures or trauma. Nevertheless, peak FVIII:C levels reaching 30 IU/dL may be clinically relevant for minor procedures or bleeding events.
Several single-center studies described DDAVP in moderate HA.15–22 A total of 21% of the moderate patients who were tested showed an increase of FVIII:C to at least 30 IU/dL and identified the following predictors of response: age, route of administration, blood group, disease severity, and F8 mutations.
However, these studies were hampered by small sample sizes and provided heterogeneous outcomes due to differences in patient characteristics and route of administration. Moreover, VWF was not studied as a potential determinant and the outcome variable which was principally studied was peak FVIII:C. In addition to the peak FVIII:C, the incremental response (proportional rise) may reveal important information on the biological mechanisms underlying DDAVP response, with possibly different predictors.
We aim to describe the response to DDAVP in moderate HA patients and to identify predictors in a large, international cohort of moderate HA patients. Our results show that DDAVP provides a valuable treatment option in a large proportion of patients with moderate HA.
Methods
Study population
We selected data on all 169 patients with moderate HA from the multicenter Response to DDAVP In non-severe hemophilia A patients: in Search for dEterminants (RISE) cohort study, consisting of 1,474 non-severe HA patients from 24 hemophilia treatment centers (Figure 1). The aim of the RISE project was to assess the predictive value of clinical and genetic factors on the DDAVP response in non-severe HA patients. This international retrospective cohort study includes all consecutive non-severe HA patients with DDAVP administration between 1980 and 2012.
Figure 1.

Patient selection of 169 moderate hemophilia A (HA) patients with 1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP) administration. The 169 patients are from 23 different hemophilia treatment centers. *Reason for treatment was unknown for one patient.
Participating centers (listed in the Online Supplementary Appendix) were located in Canada, Australia and ten European countries. The institutional review boards of all centers approved the study. Since this project involves retrospective data collection, all review boards indicated that informed consent was not required. This study was conducted in accordance with the Declaration of Helsinki.
Data collection
We collected demographic and clinical data from available medical records using a standardized electronic case report form. The following data on baseline characteristics were collected: date of birth, ethnicity, ABO blood group, family history of DDAVP response, F8 mutation (Human Genome Variation Society [HGVS] numbering was used), reason for DDAVP administration, lifetime lowest FVIII:C (one-stage clotting assay), pre-DDAVP FVIII:C, pre-DDAVP VWF antigen (VWF:Ag) and activity (VWF:Act), date of DDAVP response, DDAVP dose, Body Mass Index (BMI), inhibitor status, route of administration, FVIII:C/VWF:Ag/VWF:Act after DDAVP, and potential side effects. In cases where the patient was treated to prevent or stop bleeding, we also collected information on the reason for treatment, location and severity of bleeding and therapeutic response.
Patient selection
We selected patients from the RISE study with moderate disease severity. Patients were defined as moderate if one of the available FVIII:C measurements was 5 IU/dL or lower (lifetime lowest FVIII:C). In case of multiple DDAVP administrations, we selected the most recent DDAVP administration.
It is important to mention that 13 patients from Seary et al. and 17 patients from the study conducted by Stoof et al. with FVIII:C ≤5 IU/dL are also included in our population.15,16 We explored selection bias of our study population by comparing the RISE population to 357 moderate patients from the Intervention as a Goal in Hypertension Treatment (INternational Study on etiology of inhibitors in patients with a moderate or mild form of hemophilia A, influences of Immuno Genetic & Hemophilia Treatment factors ([INSIGHT]) study population that did not receive DDAVP.23 We compared: FVIII:C, inhibitors, cumulative exposure days to FVIII, date of birth, and age.
Definition of response
The main study outcome is the peak FVIII:C after DDAVP (in IU/dL). We classified peak response as none (<20), partial (20-29), complete (30-49) or excellent (≥50). With these classifications we were able to compare our findings to previously reported response rates. For further univariate analyses of the determinants of response, we compared patients with inadequate response to patients with at least a complete response.
Incremental response was calculated by dividing peak FVIII:C by pre-DDAVP FVIII:C. Data was collected on the therapeutic response, which is defined in Online Supplementary Table S1.
Statistical analyses
Summary statistics include frequencies and percentages for categorical variables and medians and interquartile ranges for continuous variables. An unpaired t-test and χ2 test were used to compare means between patients with inadequate response and at least a complete response. Furthermore, we used multiple linear regression to model relationships between potential explanatory variables and peak FVIII:C and incremental response in the patients tested for DDAVP responsiveness. Potential explanatory variables included in the model were: blood group, route of administration, dose, lifetime lowest FVIII:C, age, pre-DDAVP FVIII:C/VWF:Ag/VWF:Act, peak VWF:Ag/VWF:Act, and ΔVWF:Ag. ΔVWF:Ag was defined as peak VWF:Ag minus pre-DDAVP VWF:Ag. We restricted multivariate analyses to DDAVP test results as only nine patients were exclusively treated with DDAVP (Figure 1). We added pre-DDAVP FVIII:C times age as an interaction term to the model, as younger patients might have lower pre-DDAVP FVIII:C and VWF:Ag levels, and pre-DDAVP levels are known to affect the DDAVP response. A P-value <0.05 was considered statistically significant. Logistic transformation was used for variables that were not-normally distributed. Missing data were analyzed by Little’s missing completely at random (MCAR) test. If Little’s MCAR test P-value was not significant, missing data was imputed by multiple imputation.
Results
Baseline characteristics
Eleven percent of the source population (n=169) had moderate disease severity (Figure 1).
Table 1 shows the baseline characteristics and response rates of the 169 moderates with DDAVP. Administration was mostly intravenous (62%). Patients with subcutaneous versus intravenous administration were comparable, except for weight (mean 76 kg intravenous and 52 kg subcutaneous, P<0.001). In total, 99 patients (59%) were responsive to DDAVP (peak FVIII:C >20 IU/dL). The responses were excellent, complete and partial in 25 (15%), 43 (25%), and 31 (18%) patients, respectively. Table 2A displays the response rates per lowest lifetime FVIII and Table 2B shows the discrepencies between lowest lifetime FVIIII and pre-DDAVP FVIII. Further information on treatment outcomes is displayed in Online Supplemental Table S1.
Table 1.
Baseline characteristics and 1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP) response in moderate patients.
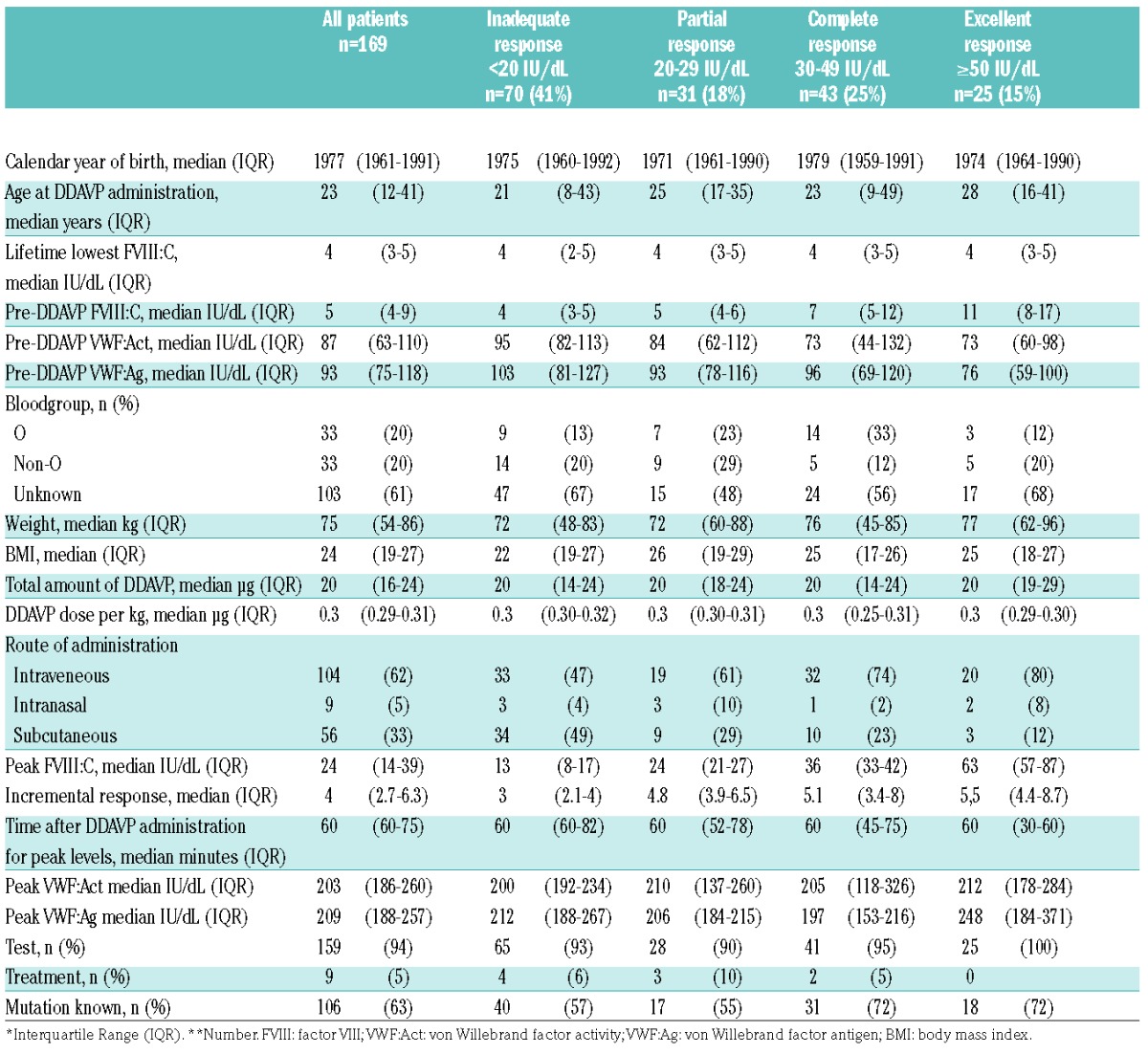
Table 2A.
Response rates per *Lowest lifetime factor VIII (FVIII:C).
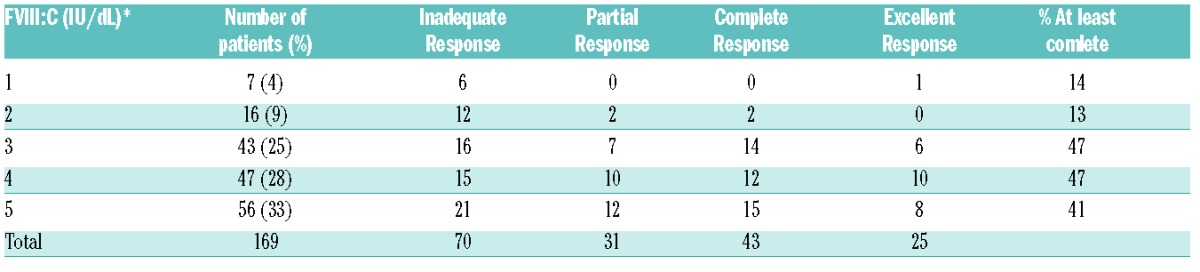
Table 2B.
Pre-1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP) factor VIII (FVIII:C) minus lowest lifetime FVIII:C, per response group.

To address selection bias, we compared moderates that received and did not receive DDAVP. The only characteristic that differed between the groups was lifetime lowest FVIII:C. This was higher in patients who received DDAVP (median 4 (interquartile range [IQR] 3-5) vs. 3 (IQR 3-4) IU/dL, P=0.002). Missing data are displayed in Online Supplementary Table S2.
Side effects
Where data was available, side effects were present in 3/119 cases. Three patients reported skin flushing and one patient had an abnormally low blood pressure (defined as <2SD for age) with an increased heart rate (>100/min) following DDAVP administration.
Univariate analyses of peak FVIII:C: no versus at least complete response
Complete and excellent responders had significantly higher pre-DDAVP FVIII:C (P<0.001) and a higher proportion of intravenous administration. Pre-DDAVP VWF showed a trend towards lower levels in excellent responders (Ag: P=0.06, Act: P=0.07). No differences were observed between the response groups for other characteristics.
Mutations
Genotype was known in 107 patients (63%). We identified 58 different mutations of which nine were present in at least three patients (Table 3, Figure 2). The Arg2169His mutation was most prevalent (n=21). Responses are scattered among the different mutation groups.
Table 3.
Mutations in at least three patients.

Figure 2.

Mutations and associated response to 1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP). All mutations were present in three patients, except for the Pro149Arg and Arg2169His mutation (n=6 and n=21, respectively). The size of the diagrams reflects the number of patients.
Multivariate analysis of peak FVIII:C and increment
The following predictors explain 65% (Adjusted R2=0.65) of the variation in peak FVIII:C: intravenous administration, pre-DDAVP FVIII:C and VWF:Ag, ΔVWF:Ag, peak VWF:Act and age (Table 4A).
Table 4A.
Multiple linear regression model of predictors of peak factor VIII (FVIII:C) explaining 65% of peak FVIII:C.
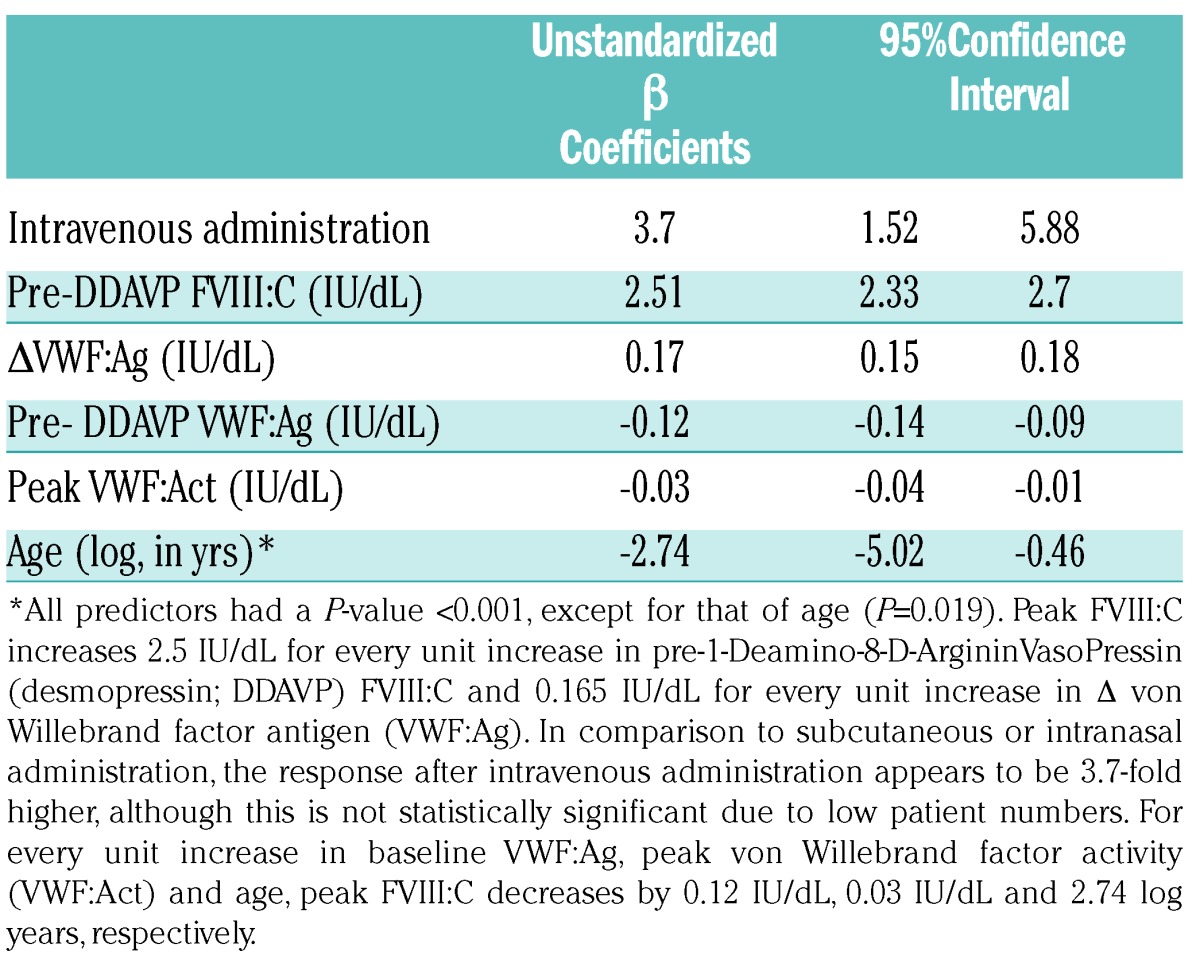
Both pre-FVIII:C and ΔVWF:Ag have strong effects; the peak FVIII:C increases by 2.5 IU/dL for every unit increase in pre-DDAVP FVIII:C, and by 0.165 IU/dL for every unit increase in ΔVWF:Ag (DDAVP induced rise of VWF:Ag). Peak FVIII:C increased with intravenous compared to subcutaneous and intranasal administration (β=3.7). Remarkably, for every unit increase in baseline VWF:Ag, peak FVIII:C decreases by 0.117 IU/dL.
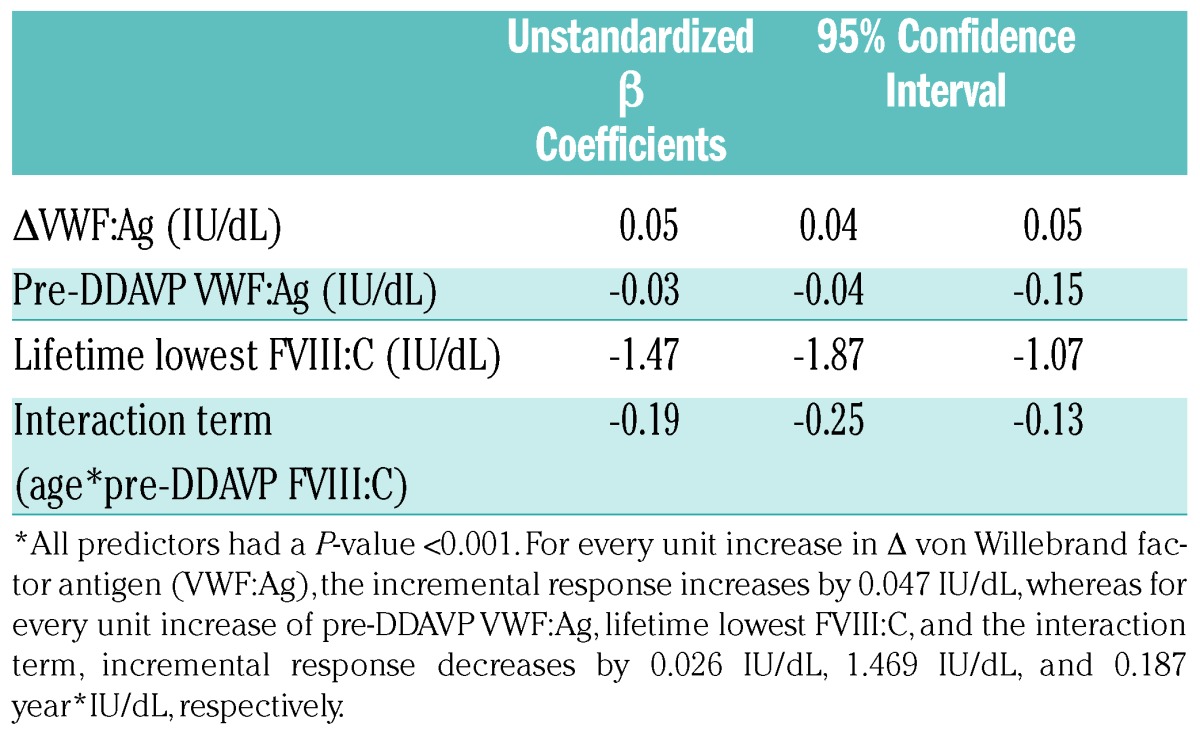
The incremental response of FVIII:C can be explained for 29% (Adjusted R2=0.29) by ΔVWF:Ag, pre-DDAVP VWF:Ag, lowest lifetime FVIII:C, and the interaction term age*pre-DDAVP FVIII:C (Table 4B). For every unit increase in Δ VWF:Ag, the incremental response increases by 0.047 IU/dL, whereas for every unit increase of pre-DDAVP VWF:Ag, lifetime lowest FVIII:C, the interaction term, the incremental response decreases by 0.026 IU/dL, 1.469 IU/dL, and 0.187 year*IU/dL, respectively.
Table 4B.
Multiple linear regression model of incremental response (peak factor VIII [FVIII:C]/pre-1-Deamino-8-D-ArgininVasoPressin [desmopressin; DDAVP] FVIII:C) explaining 29% of incremental response.
Discussion
Herein, we present DDAVP response rates and predictors in a large, international cohort of moderate HA patients. In total, 68 patients (40%) achieved a peak FVIII:C of at least 30 IU/dL, among these 25 responses were excellent (FVIII:C ≥ 50IU/dL).
We identified six predictors of peak FVIII:C, which, taken together, explain 65% of the variation in peak FVIII:C. The pre-DDAVP FVIII:C and DDAVP-induced rise in VWF:Ag were the most important. The incremental response could be explained for 29% by different predictors, other than for peak FVIII:C.
Response rates
Eight single-center studies previously reported DDAVP response rates in moderate HA patients and the characteristics of included patients (Table 5).15–22 The number of moderate patients in these studies varied from one to 17.
Table 5.
Previous studies on 1-Deamino-8-D-ArgininVasoPressin (desmopressin; DDAVP) response in moderate hemophilia A (HA) patients.
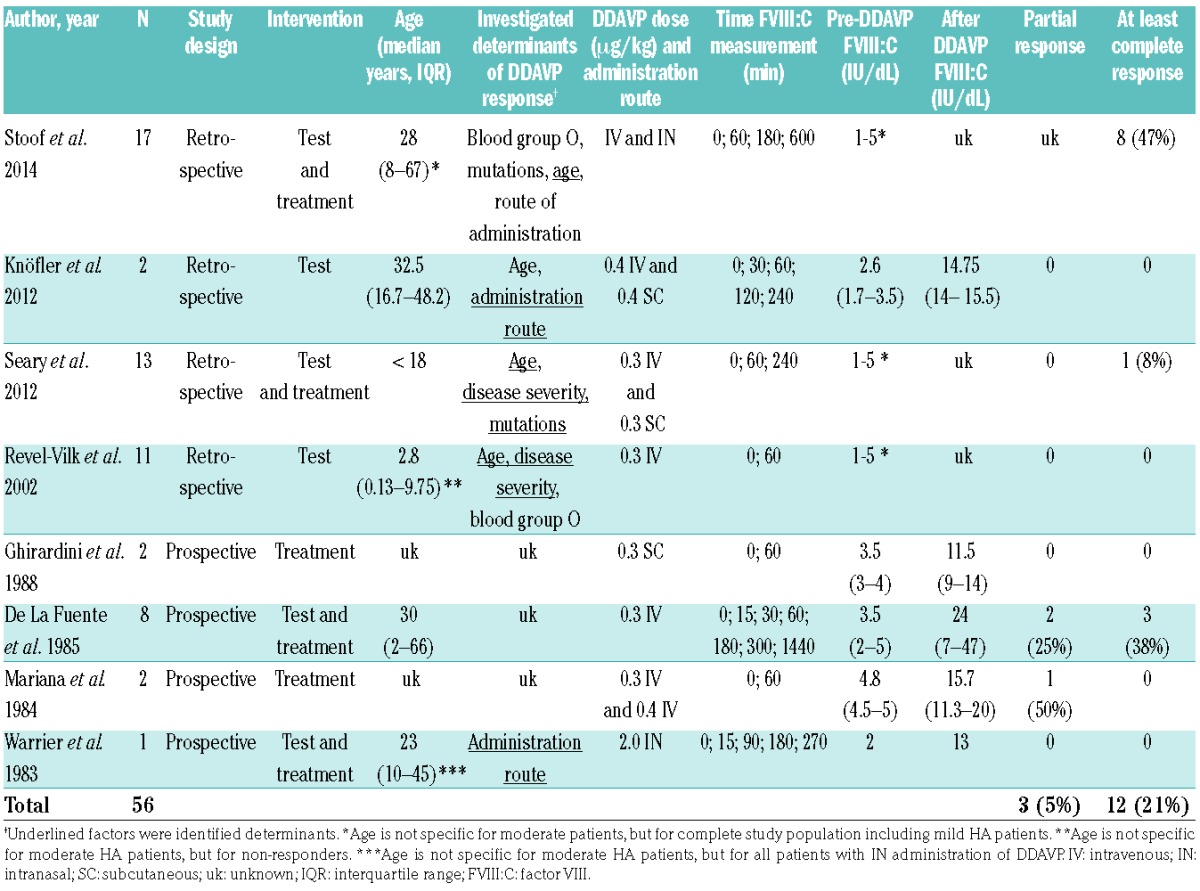
Taken together, a total of 12 out of 56 patients from the eight studies showed a response of at least 30 IU/dL after DDAVP administration (21%). The difference between the response rates that we report herein (40%) might be due to differences in selection, population characteristics and routes of administration.
Predictors of peak FVIII:C
We identified six predictors explaining 65% of the variation in peak FVIII:C.
Intravenous administration predicts higher peak FVIII:C compared to subcutaneous or intranasal administration in our cohort, as well as in other studies.17,24–31 However, it is unknown, as of yet, whether this difference is clinically relevant, and data on moderate patients are scarce. Subcutaneous administration is believed to be biologically equivalent to the intravenous route, but this is based on only one paper.32 The rate of subcutaneous absorption could affect either the FVIII:C peak or its timing. If there is a clinically relevant difference, then this effect might be more critical in moderate patients due to their lower baseline levels.
Our observation that higher pre-DDAVP FVIII:C predicts higher peak FVIII:C in moderate HA patients is supported by other studies.15,18
ΔVWF:Ag was the second strongest predictor of peak FVIII:C. In consistency with this finding, we identified lower pre-DDAVP VWF:Ag as a predictor of peak FVIII:C. We can only speculate on the biological mechanism explaining this observation. Potentially, the stronger increase in VWF provides more binding sites for FVIII released upon DDAVP administration. Some patients may have higher pre-DDAVP VWF:Ag due to stress. Stress is known to increase endogenous FVIII:C and VWF. Hence, patients may have already released some of their stored VWF due to stress, with with less potential for VWF to rise further with DDAVP. Finally, it is conceivable that some patients have a phenotype of “greedy” endothelium, whereby VWF stores (or storage compartments) are only depleted upon extra (DDAVP) stimulation. There is still more to learn about the exact sources and secretion of both FVIII and VWF upon DDAVP stimulation, and how they interact.
It is important to stress that ΔVWF:Ag is derived from a post hoc parameter (DDAVP-induced rise in VWF:Ag), and can therefore not be used by the clinician to predict response adequacy in advance.
We do not have an explanation for the lower peak VWF:Act which predicts a higher FVIII:C peak. This finding is inconsistent with the ΔVWF:Ag finding.
Our finding that younger age predicted higher peak FVIII:C in our cohort of moderate HA patients is inconsistent with the literature reporting moderate patients. Stoof et al. and Knöfler et al. did not find an effect of age on DDAVP response, which they both attribute to the fact that the age of their population was higher than in the studies of Seary et al. and Revel-Vilk et al. (Table 5).15–18 Both Seary et al. and Revel-Vilk et al. found that responders had a higher mean age compared to non-responders, however, they did not adjust for pre-DDAVP FVIII:C. Furthermore, their study was performed exclusively in children whereas our study focuses predominantly on adults (Table 5).15,18
Determinants of incremental response
We identified four predictors of the incremental response; ΔVWF:Ag, pre-DDAVP VWF:Ag and lifetime lowest FVIII:C levels increase the incremental response. Furthermore, a smaller product of the interaction term age*pre-DDAVP FVIII:C predicted a higher incremental response. The interaction term indicates that the effect of pre-DDAVP FVIII:C on the incremental change of FVIII following DDAVP varies for age, or that the effect of age on the incremental change of FVIII following DDAVP is altered by pre-DDAVP FVIII:C.
This is the first study which used incremental response as an outcome variable reflecting the biological mechanisms underlying DDAVP response. Unlike for peak FVIII:C, for incremental response the pre-DDAVP is not a predictor and lifetime lowest FVIII:C is inversely associated. This is most likely due to the reciprocal effect of higher pre-DDAVP FVIII:C on the relative increase, since it is the denominator of our outcome variable. There may be an effect of stress-induced increase of FVIII, depicted in Table 2B by a difference between lowest lifetime and pre-DDAVP FVIII:C. However, we did not adjust for age and mutation, as the effect of age on FVIII:C is dependent on mutation.33
The variation in the incremental response was explained for only 29% by the four identified predictors. This is less than the explained variation in peak response (65%). We believe that further analyses of different mutation groups might help to reveal the observed discrepancy in explained variance.
Mutation analysis
Two studies presented the DDAVP response for different mutations in non-severe patients.15,16 All moderate patients from these studies are also included in our cohort. Unexpectedly, we observed a discordance in DDAVP response among patients with the same mutation that was not due to differences in route of administration (Figure 2). Four mutations present in at least three patients were also identified in the INSIGHT cohort as high-risk mutations for inhibitor development (Arg550Cys, Arg612Cys, Arg2150His and Trp2248Cys HGVS numbering).23 As Figure 2 and Table 3 show, half of the patients with these mutations in our cohort showed at least a complete response to DDAVP. This is of clinical importance as these patients may be successfully treated with DDAVP in order to reduce hazardous exposure to FVIII concentrates.
Limitations and strengths
This large, international cohort study provides data on the response to DDAVP in moderate HA patients. Our study is unique owing to the large number of patients included, thus increasing the statistical power.
As lifetime lowest and pre-DDAVP FVIII:C was not measured in a standardized manner, this may have led to an overestimation of patients who were once classified as moderate, but who were not defined as moderate at the time of the DDAVP test. This can be seen in Table 1, where patients with complete and excellent responses have a higher pre-DDAVP FVIII:C irrespective of their lowest lifetime FVIII:C.
With respect to our outcome variables, it is important to state that the biological response is only a proxy of the clinical response to DDAVP. Additional data are warranted to establish when and to which extent desmopressin can be clinically used to treat patients with moderate HA.
As only 32% of the moderate patients from our source population were tested or treated with DDAVP, this might lead to an overestimation of patients with a good response. The proportion of moderate patients receiving DDAVP per hemophilia treatment center ranged from 19 to 50. Moderate patients who received DDAVP had higher lowest lifetime FVIII:C compared to those who did not. For these reasons, caution is needed when extrapolating these results to all moderate HA patients.
Although our study is unique in terms of its size, we still lacked the power to further analyze the effect of mutations on DDAVP response in moderate HA patients. As the F8 genotype is known to influence baseline FVIII:C, and thereby DDAVP response, the effect of mutations via baseline FVIII:C may contribute to clarifying 35% of the unexplained variation in peak FVIII:C levels.33
For further functional analyses of genotype, it would have been informative to have, in addition, the FVIII antigen (FVIII:Ag) levels. Castaman et al. demonstrated that the presence of a dysfunctional FVIII molecule (Antigen>Activity) per se does not prevent a response to DDAVP.34
Clinical significance and future studies
As illustrated in Table 5, the use of DDAVP for moderate HA patients in clinical practice has been limited to a few cases over the last 40 years, despite the fact that this drug has been available since 1977. The study herein evinces that 40% of the patients with moderate HA in our cohort have a clinical relevant response to DDAVP for mild bleeds/injuries. Moreover, half of the patients with high inhibitor risk mutations respond to DDAVP; for this reason, it is important to always assess such patients for DDAVP responsiveness. Doing so might lead to less exposure to FVIII concentrates, which reduces risk for inhibitor development, and realizes a reduction in costs.
In order to confirm our findings, future studies should focus on the prospective inclusion of moderate HA patients. Lastly, more data on mutations are needed in order to assess the effect of F8 missense mutations on DDAVP response in these patients.
Conclusion
In 40% of the administrations in moderate HA patients in our cohort, the use of DDAVP is adequate for treatment in case of minor bleeding or trauma; as such, it is important to consistently assess moderate patients for DDAVP responsiveness.
Furthermore, we identified six predictors of peak FVIII:C, which, taken together, explain 65% of the variation in peak FVIII:C. Pre-DDAVP FVIII:C levels and the patients’ ability to raise VWF levels are the essential predictors for response.
Supplementary Material
Acknowledgments
Romy van Spengen, medical student in the Academic Medical Center Amsterdam, helped to construct Table 5.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/103/3/550
Funding
This work was supported by the Access to Insight Grant from Novo Nordisk.
References
- 1.Fijnvandraat K, Cnossen MH, Leebeek FWG, Peters M. Diagnosis and management of haemophilia. BMJ. 2012;344(2707):1–5. [DOI] [PubMed] [Google Scholar]
- 2.Schramm W, Royal S, Kroner B, et al. Clinical outcomes and resource utilization associated with haemophilia care in Europe. Haemophilia. 2002;8(1):33–43. [DOI] [PubMed] [Google Scholar]
- 3.Mannucci P. Desmopressin (DDAVP) in the treatment of bleeding disorders: the first 20 years. Blood. 1997;90(7):2515–2521. [PubMed] [Google Scholar]
- 4.Mannucci P, Pareti F, Ruggeri Z, Capitanio A. DDAVP: a new pharmacological approach to the management of haemophilia and von Willebrand’s disease. Lancet. 1977;1(8017):869–872. [DOI] [PubMed] [Google Scholar]
- 5.Rosenberg JB, Greengard JS, Montgomery RR. Desmopressin (DDAVP) in the treatment of bleeding disorders: the first 20 years. Arterioscler Thromb Vasc Biol. 2000;20(12):2689–2695. [DOI] [PubMed] [Google Scholar]
- 6.Shanani T, Covens K, Lavend’homme R, et al. Human liver sinusoidal endothelial cells but not hepatocytes contain factor VIII. J Thromb Haemost. 2013;12(1):36–42. [DOI] [PubMed] [Google Scholar]
- 7.Groth CG, Hathaway WE, Gustafsson A, et al. Correction of coagulation in the hemophilic dog by transplantation of lymphatic tissue. Surgery. 1974;75(5):725–733. [PMC free article] [PubMed] [Google Scholar]
- 8.Norman JC, Covelli VH, Sise HS. Transplantation of the spleen: experimental cure of hemophilia. Surgery. 1968;64(1):1–14. [PubMed] [Google Scholar]
- 9.Jacquemin M, Neyrinck A, Hermanns MI, et al. FVIII production by human lung microvascular endothelial cells. Blood. 2006;108(2):515–517. [DOI] [PubMed] [Google Scholar]
- 10.Everett LA, Cleuren AC, Khoriaty RN, Ginsburg D. Murine coagulation factor VIII is synthesized in endothelial cells. Blood. 2014;123(24):3697–3705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fahs SA, Hille MT, Shi Q, Weiler H, Montgomery RR. A conditional knockout mouse model reveals endothelial cells as the principal and possibly exclusive source of plasma factor VIII. Blood. 2014;123(24):3706–3713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kaufmann JE, Oksche A, Wollheim CB, Günther G, Rosenthal W, Vischer UM. Vasopressin-induced von Willebrand factor secretion from endothelial cells involves V2 receptors and cAMP. J Clin Invest. 2000;106(1):107–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lamont PA, Ragni MV. Lack of desmopressin (DDAVP) response in men with hemophilia A following liver transplantation. J Thromb Haemost. 2005;3(10):2259–2263. [DOI] [PubMed] [Google Scholar]
- 14.Rodeghiero F, Castaman G, Di Bona E, Ruggeri M. Consistency of responses to repeated DDAVP infusions in patients with von Willebrand’s disease and hemophilia A. Blood. 1989;74(6):1997–2000. [PubMed] [Google Scholar]
- 15.Seary ME, Feldman D, Carcao MD. DDAVP responsiveness in children with mild or moderate haemophilia A correlates with age, endogenous FVIII:C level and with haemophilic genotype. Haemophilia. 2012;18(1):50–55. [DOI] [PubMed] [Google Scholar]
- 16.Stoof SCM, Sanders YV, Cnossen MH, de Maat MPM, Leebeek FWG, Kruip MJHA. Desmopressin response in hemophilia A patients with FVIII: C < 0.10 IU mL-1. J Thromb Haemost. 2014;12(1):110–112. [DOI] [PubMed] [Google Scholar]
- 17.Knöfler R, Koscielny J, Tauer JT, et al. Desmopressin testing in haemophilia A patients and carriers: Results of a multi centre survey. Hamostaseologie. 2012;32(4):271–275. [DOI] [PubMed] [Google Scholar]
- 18.Revel-Vilk S, Blanchette VS, Sparling C, Stain AM, Carcao MD. DDAVP challenge tests in boys with mild/moderate haemophilia A. Br J Haematol. 2002;117(4):947–951. [DOI] [PubMed] [Google Scholar]
- 19.Ghirardini A, Chistolini A, Tirindelli MC, Di Paolantonio T, Iacopino G, Marianio P. Clinical evaluation of subcutaneously administered DDAVP. Thromb Res. 1988;49(3):363–372. [DOI] [PubMed] [Google Scholar]
- 20.de la Fuente B, Kasper C, Rickles F, Hoyer L. Response of patients with mild and moderate hemophilia A and von Willebrand’s disease to treatment with desmopressin. Ann Intern Med. 1985;103(1):6–14. [DOI] [PubMed] [Google Scholar]
- 21.Mariana G, Ciavarella N, Mazzucconi M, et al. Evaluation of the effectiveness of DDAVP in surgery and in bleeding episodes in haemophilia and von Willebrand’s disease. A study on 43 patients. Clin Lab Haematol. 1984;6(3):229–238. [DOI] [PubMed] [Google Scholar]
- 22.Warrier AI, Lusher JM. DDAVP. A useful alternative to blood components in moderate hemophilia A and von Willebrand disease. J Pediatr. 1983;102(2):228–233. [DOI] [PubMed] [Google Scholar]
- 23.Eckhardt CL, Van Velzen AS, Peters M, et al. for the INSIGHT study group. Factor VIII gene (F8) mutation and risk of inhibitor development in nonsevere hemophilia A. Blood. 2013;122(11):1954–1962. [DOI] [PubMed] [Google Scholar]
- 24.Jacquemin M, Lavend’homme R, Benhida A, et al. A novel cause of mild/moderate hemophilia A: mutations scattered in the factor VIII C1 domain reduce factor VIII binding to von Willebrand factor. Blood. 2000;96(3):958–965. [PubMed] [Google Scholar]
- 25.Lethagen S, Harris S, Nilsson M. Intranasal desmopressin (DDAVP) by spray in mild hemophilia A and von Willebrand’s disease type I. Blut. 1990;60(3):187–191. [DOI] [PubMed] [Google Scholar]
- 26.Christolini A, Dragoni F, Ferrari A, et al. Intranasal DDAVP: biological and clinical evaluation in mild factor VIII deficiency. Pathophysiol Haemost Thromb. 1991;21(5):273–277. [DOI] [PubMed] [Google Scholar]
- 27.Rose EH, Aledort LM. Nasal spray desmopressin (DDAVP) for mild hemophilia A and von Willebrand disease. Ann Intern Med. 1991;114(7):563–568. [DOI] [PubMed] [Google Scholar]
- 28.Lethagen S, Egervall K, Berntorp E, Bengtsson B. The administration of desmopressin by nasal spray: a dose-determination study in patients with mild haemophilia A or von Willebrand’s disease. Haemophilia. 1995;1(2):97–102. [DOI] [PubMed] [Google Scholar]
- 29.Leissinger C, Becton D, Cornell C, Gill JC. High-dose DDAVP intranasal spray (Stimate) for the prevention and treatment of bleeding in patients with mild haemophilia A, mild or moderate type 1 von Willebrand disease and symptomatic carriers of haemophilia A. Haemophilia. 2001;7(3):258–266. [DOI] [PubMed] [Google Scholar]
- 30.Gill JC, Ottum M, Schwartz B. Evaluation of high concentration intranasal and intravenous desmopressin in pediatric patients with mild hemophilia A or mild-to-moderate type 1 von Willebrand disease. J Pediatr. 2002;140(5):595–599. [DOI] [PubMed] [Google Scholar]
- 31.Lethagen S, Ragnarson Tennvall G. Self-treatment with desmopressin intranasal spray in patients with bleeding disorders: Effect on bleeding symptoms and socioeconomic factors. Ann Hematol. 1993;66(5):257–260. [DOI] [PubMed] [Google Scholar]
- 32.Mannucci P, Vicente V, Alberca I, et al. Intravenous and subcutaneous administration of desmopressin (DDAVP) to hemophiliacs: pharmacokinetics and factor VIII responses. Thromb Haemost. 1987;58(4):1037–1039. [PubMed] [Google Scholar]
- 33.Loomans JI, van Velzen AS, Eckhardt CL, et al. Variation in baseline factor VIII concentration in a retrospective cohort of mild/moderate hemophilia A patients carrying identical F8 mutations. J Thromb Haemost. 2017;15(2):246–254. [DOI] [PubMed] [Google Scholar]
- 34.Castaman G, Mancuso ME, Giacomelli SH, et al. Molecular and phenotypic determinants of the response to desmopressin in adult patients with mild hemophilia A. J Thromb Haemost. 2009;7(11):1824–1831. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.