

Abstract
Objective
Corneal confocal microscopy (CCM), an in vivo ophthalmic imaging modality, is a noninvasive and objective imaging biomarker for identifying small nerve fiber damage. We have evaluated the diagnostic performance of previously established CCM parameters to a novel automated measure of corneal nerve complexity called the corneal nerve fiber fractal dimension (ACNFrD).
Methods
A total of 176 subjects (84 controls and 92 patients with type 1 diabetes) with and without diabetic sensorimotor polyneuropathy (DSPN) underwent CCM. Fractal dimension analysis was performed on CCM images using purpose-built corneal nerve analysis software, and compared with previously established manual and automated corneal nerve fiber measurements.
Results
Manual and automated subbasal corneal nerve fiber density (CNFD) (P < 0.0001), length (CNFL) (P < 0.0001), branch density (CNBD) (P < 0.05), and ACNFrD (P < 0.0001) were significantly reduced in patients with DSPN compared to patients without DSPN. The areas under the receiver operating characteristic curves for identifying DSPN were comparable: 0.77 for automated CNFD, 0.74 for automated CNFL, 0.69 for automated CNBD, and 0.74 for automated ACNFrD.
Conclusions
ACNFrD shows comparable diagnostic efficiency to identify diabetic patients with and without DSPN.
Keywords: corneal confocal microscopy, diabetic neuropathy, image segmentation, nerve fiber quantification
Diabetic sensorimotor polyneuropathy (DSPN) affects at least 50% of patients with diabetes.1 Earlier diagnosis and timely intervention to prevent progression to costly outcomes like foot ulceration could reduce not only morbidity but also mortality.2–4
DSPN can be quantified by assessing neuropathic symptoms and deficits, quantitative sensory testing, and neurophysiology.5 Neurophysiology is objective and reproducible and considered to be the most reliable method to confirm the diagnosis of DSPN, but it assesses only large nerve fiber damage, which may be preceded by small fiber damage.6,7 Small fiber dysfunction can be quantified by evaluating thermal thresholds,8 and small fiber pathology can be evaluated from a skin biopsy by deriving the intraepidermal nerve fiber density (IENFD).9–11 However, skin biopsy is invasive9 and therefore not easily amenable to repeat evaluation, and there are limited studies on the diagnostic reliability of IENFD in DSPN.12
Corneal confocal microscopy (CCM) can be used to image small nerve fiber damage. Previous studies13–18 have shown that corneal nerve loss can be detected in diabetic patients without diabetic neuropathy. This reflects the ability of CCM to capture early small fiber pathology, which cannot be detected using conventional tests such as diabetic neuropathic symptoms, deficits, and neurophysiology. This suggests that CCM may act as a surrogate endpoint for early DSPN.6,19–21 We have previously shown that CCM and IENFD correlate with each other14 and that the diagnostic ability of CCM is comparable to that of IENFD for the diagnosis of DSPN.18,22 In 2003, we originally established that quantification of subbasal corneal nerve fiber density (CNFD), corneal nerve branch density (CNBD), and corneal nerve fiber length (CNFL) was a reliable means to quantify corneal nerve damage and repair in diabetic neuropathy.13 Since then multiple studies have shown that these parameters also identify nerve fiber degeneration and repair in a range of peripheral neuropathies including amyloid neuropathy,23 Charcot-Marie-Tooth disease type 1A,24 chronic inflammatory demyelinating polyneuropathy,25,26 and human immunodeficiency virus (HIV)–induced sensory neuropathy,27 as well as central neurodegenerative conditions including motor neuron disease,28 Parkinson's disease,29 and multiple sclerosis.30,31 However, while corneal nerve fiber density, branch density, and length can quantify nerve fiber damage and repair, they cannot differentiate specific neurodegenerative conditions. We propose a novel metric of corneal nerve morphology, the fractal dimension (FD),32 to measure the spatial loss of nerve fibers, which may help to identify specific neurodegenerative conditions and augment the diagnosis of DSPN.
Methods
Study Subjects
This research adhered to the tenets of the Declaration of Helsinki and was approved by the North Manchester Research Ethics Committee. Age between 14 and 85 years and a history of type 1 diabetes were used as the inclusion criteria. Exclusion criteria were a positive history of malignancy, connective tissue or infectious disease, deficiency of vitamin B12 or folate, liver failure, chronic renal failure, active diabetic foot ulceration and family history of peripheral neuropathy, active ocular disease, and systemic disease known to affect the cornea other than diabetes or chronic corneal pathologies. Informed written consent was obtained from all participants. Ninety-two patients with type 1 diabetes mellitus and 84 age-matched controls were recruited for the study. All subjects were assessed for the presence and severity of DSPN based on the updated Toronto consensus criteria.33All participants underwent assessment of body mass index, glycated hemoglobin (HbA1c), total cholesterol, high-density lipoprotein cholesterol (HDL), triglycerides, and systolic and diastolic blood pressure.
Peripheral Neuropathy Assessment
Neurologic deficits (Neuropathy Disability score)34 and neuropathic symptoms (Diabetic Neuropathy Symptom score)35 were evaluated. Vibration perception threshold (VPT) was tested using a neurothesiometer (Horwell, Scientific Laboratory Supplies, Wilford, Nottingham, UK), and cold and warm thresholds were evaluated on the dorsolateral aspect of the left foot, using the TSA-II NeuroSensory Analyser (Medoc Ltd., Ramat-Yishai, Israel). Electrodiagnostic studies were performed using a Dantec Keypoint system (Dantec Dynamics Ltd, Bristol, UK) equipped with a DISA temperature regulator to keep limb temperature constantly between 32°C and 35°C. Sural sensory nerve conduction velocity (SSNCV), sural sensory nerve amplitude (SSNamp), peroneal motor nerve conduction velocity (PMNCV), and peroneal motor nerve amplitude (PMNamp) were assessed by a consultant neurophysiologist.
The Toronto Diabetic Neuropathy Expert Group33 recommendation was used to identify clinically detectable DSPN: (1) abnormal nerve conduction—a PMNCV of <42 m/s; (2) a symptom or sign of neuropathy, defined as one of the following: diabetic neuropathy symptom score of 1 or more out of 4 or neuropathy disability score of 3 or more out of 10.
Manual and Automated Corneal Nerve Quantification
CCM images were captured using the Heidelberg Retina Tomograph III Rostock Cornea Module (Heidelberg Engineering GmbH, Heidelberg, Germany),21,36 as shown in Figure 1. Each image is 384 × 384 pixels with a pixel size of 1.0417 μm. Six images of the subbasal nerve plexus from the right and left eyes were selected for analysis using purpose-written, proprietary software. CNFD (number of main fibers per mm2), CNFL (total length of main fibers and branches per mm2), and CNBD (number of branches per mm2)21,36 were quantified using manual (CCMetrics; M.A. Dabbah, Imaging Science, University of Manchester) and automated (ACCMetrics) software.19 The FD measurement is fully automated and consists of a nerve fiber detection step based on a machine-learning method37 (Fig. 1). As shown in Figure 1, most of the nerve fibers can be robustly detected, even with a noisy background, and a previous study has validated the utility of this method.37 The nerve fiber FD measures the structure complexity as a ratio of the change in detail to the change in scale.32 For the implementation of FD in this study, it is calculated using a box-counting method based on the detected nerve fibers from the CCM images.38 Different-sized boxes (size of 1 × 1, 2 × 2, 4 × 4…28 × 28) are used to check each pixel location in the image. If any part of the detected nerve fiber is within a box, the number of boxes for this particular size box increases by 1. A set of points can be plotted based on the number of boxes against the corresponding box sizes. A line is then fitted to these points using the least square method, where the slope of the line is the FD value. Intuitively, the slope of the line is larger when a larger number of small boxes are counted, indicating a more complicated structure. A high FD value corresponds to an evenly distributed complex nerve fiber structure that likely belongs to a healthy subject. In contrast, fewer distorted nerve fibers results in a lower FD value that may reflect abnormality. The automated corneal nerve fiber fractal dimension (ACNFrD) measurement is now included in our automated nerve fiber quantification software, which is freely available from a dedicated Web site via the University of Manchester portal.39 To assess the diagnostic ability of the standard corneal nerve metrics (CNFD, CNBD, CNFL) with ACNFrD for DSPN, we compared control subjects to diabetic subjects with and without DSPN.
Figure 1.
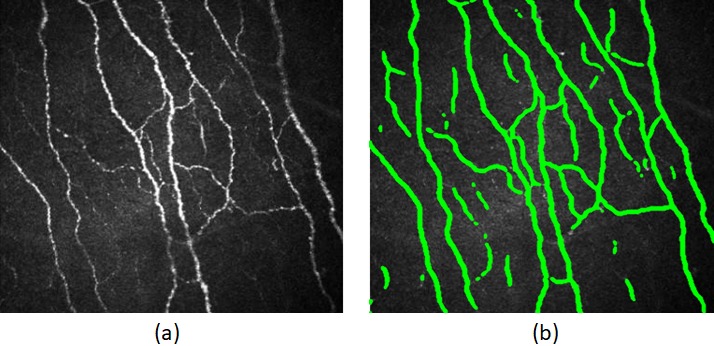
(a) Original CCM image. (b) Automatically detected nerve fibers.
Statistical Analysis
Statistical analysis and the receiver operating characteristic (ROC) curves were performed and generated using MATLAB (version R2012a, The MathWorks, Inc., Natick, MA, USA). One-way ANOVA (nonparametric Kruskal-Wallis) was used to evaluate within- and between-group differences (control versus no DSPN versus DSPN). A P < 0.05 was considered significant. Area under the ROC curve (AUC) values, 95% confidence intervals, and sensitivity/specificity both at the equal error rate point and at the threshold of 2 standard deviations below the mean of the control group were calculated and compared.40
Results
Demographic, Metabolic, and Anthropometric Assessment
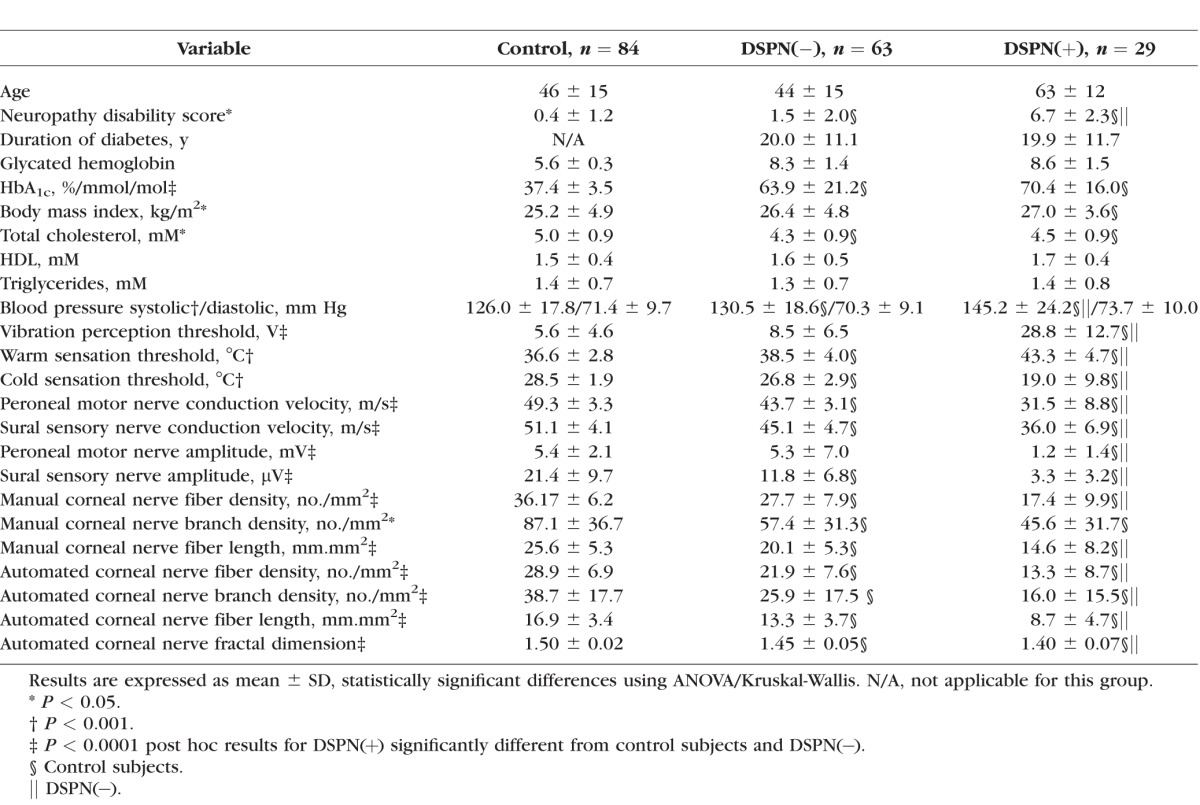
Demographic, anthropometric, and metabolic measurements in patients with diabetes and control subjects are summarized in Table 1. Age was comparable, but HbA1c was significantly higher in diabetic patients compared with control subjects, with no difference between patients with and without DSPN. Body mass index was significantly higher in diabetic patients with DSPN compared to controls. Total cholesterol was significantly lower in diabetic patients with and without DSPN, while HDL and triglycerides did not differ between groups. Systolic blood pressure was significantly higher in diabetic patients with and without DSPN, compared to control subjects.
Table 1.
Clinical Demographic Results and Neuropathy Assessment in Control Subjects and Type 1 Diabetic Patients Without (DSPN [−]) and With (DSPN [+]) Neuropathy
Neurologic Assessment
The neuropathy disability score was significantly higher in patients with DSPN compared to control subjects.
Quantitative Sensory Testing
The VPT was significantly higher in patients with DSPN compared to patients without DSPN and control subjects. Warm sensation threshold was significantly higher while cold sensation threshold was lower in patients with and without DSPN compared to control subjects.
Electrophysiology
PMNCV, SSNC, and SSNamp were significantly reduced in diabetic patients with and without DSPN compared to controls; PMNCV, SSMCV, PMNamp, and SSNamp were significantly reduced in diabetic patients with and without DSPN compared to controls and in diabetic patients with DSPN compared to patients without DSPN.
Manual CCM
MCNFD was significantly reduced in diabetic patients with (P < 0.0001) and without (P < 0.0001) DSPN compared to control subjects and was reduced in patients with DSPN compared to patients without DSPN (P < 0.0001) (Table 1). MCNBD was significantly reduced in diabetic patients with and without neuropathy (P < 0.0001) compared to control subjects. MCNFL was significantly reduced in diabetic patients with (P < 0.0001) and without (P < 0.0001) DSPN compared to control subjects and was reduced in diabetic patients with DSPN compared to patients without DSPN (P = 0.001).
Automated CCM
Automated corneal nerve fiber density (ACNFD), automated corneal nerve fiber length (ACNFL), and ACNFrD were all significantly reduced in diabetic patients with (P < 0.0001) and without (P < 0.0001) DSPN compared to control subjects and were further reduced in diabetic patients with DSPN compared to patients without DSPN (P < 0.0001). Automated corneal nerve branch density (ACNBD) was significantly reduced in diabetic patients with (P < 0.0001) and without (P < 0.0001) DSPN compared to control subjects and was reduced in diabetic patients with DSPN compared to patients without DSPN (P = 0.002). The box plots shown in Figure 2a indicate FD values decreasing significantly from the control group to the DSPN(−) group (P < 0.0001) and from the DSPN(−) group to the DSPN(+) group (P < 0.0001).
Figure 2.
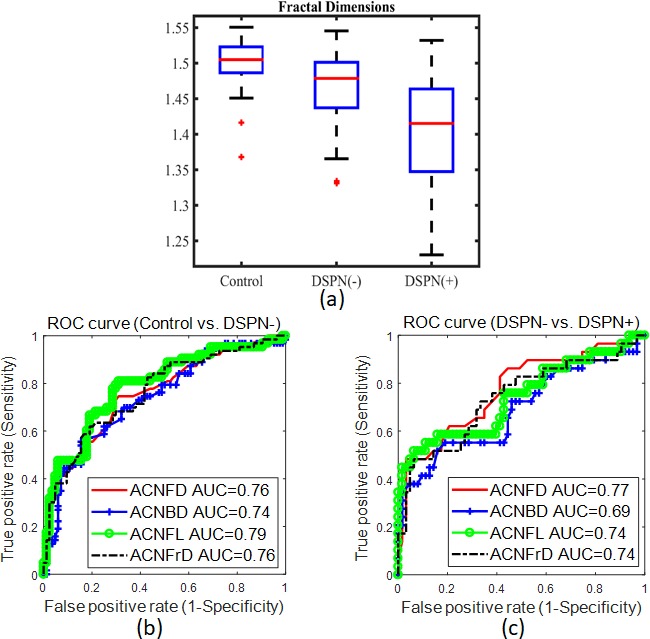
(a) Box plot of fractal dimension values for control, DSPN(−), and DSPN(+) groups. (b) ROC curves of ACNFD, ACNBD, ACNFL, and ACNFrD for discriminating control from DSPN(−). (c) ROC curves of ACNFD, ACNBD, ACNFL, and ACNFrD for discriminating DSPN(−) from DSPN(+).
ROC Analysis
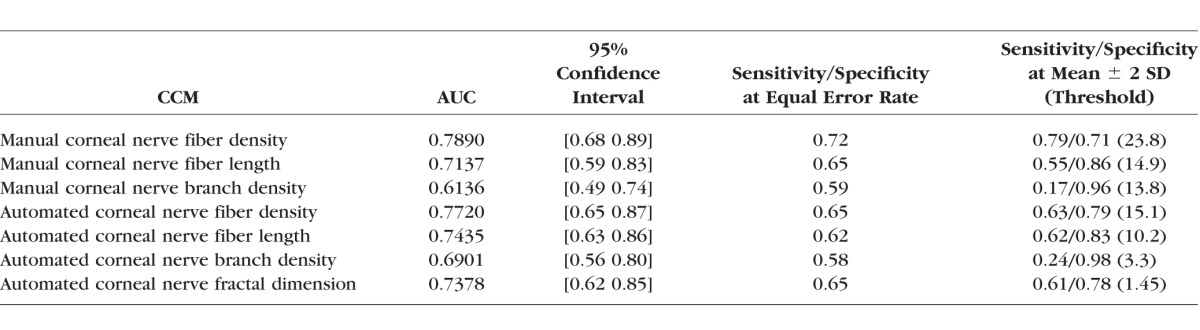
Diabetic patients were divided into two groups: no DSPN(−) (n = 63) and DSPN(+) (n = 29). Table 2 shows the AUC values, 95% confidence intervals, and sensitivity/specificity at the equal error rate point on the ROC curve for both manual and automated CCM features. The highest AUC values among the manual and automated CCM measures were obtained for CNFD, with AUC values of 0.79 and 0.77, respectively. The areas under the ROC curve for ACNFrD for discriminating control from DSPN(−) and DSPN(−) from DSPN(+) are 0.76 and 0.74, respectively (Figs. 2b, 2c). There was no significant difference between the ROC curves comparing ACNFrD to ACNFD (P = 0.30), ACNBD (P = 0.21), and ACNFL (P = 0.50) for discriminating control from DSPN(−) (Fig. 2c). There were no statistically significant differences between the ROC curves for ACNFrD compared to ACNFD (P = 0.50), ACNBD (P = 0.40), and ACNFL (P = 0.35) for discriminating DSPN(−) from DSPN(+).
Table 2.
AUC, 95% Confidence Interval Values, and Sensitivity/Specificity for Manual and Automated CCM for the Diagnosis of DSPN(+) From DPSN(−)
Discussion
Objective surrogate endpoints of diabetic neuropathy that accurately detect early disease and quantify disease progression and measure therapeutic response are required.2 Small fiber neuropathy is implicated in a number of clinically relevant outcomes including neuropathic pain,41 erectile dysfunction,42 altered gait,43 and foot ulceration.44 Although IENFD has been proposed as a valid measure of diabetic neuropathy,12 the invasive nature of skin biopsy limits its practical use as a diagnostic test.
CCM is a rapid, noninvasive ophthalmic imaging technique that can quantify small nerve fiber degeneration and regeneration in patients with diabetic neuropathy6,15,45–48 and that has been related to the severity of diabetic neuropathy.14,21,22,47 Automated subbasal corneal nerve image analysis allows rapid quantification of corneal nerve fiber degeneration,20,21,49 with comparable diagnostic efficiency to manual quantification.50 Previous reviews have highlighted the extensive diabetes-related complications in the cornea51–53 and have also shown that corneal nerve loss occurs in patients without diabetic retinopathy and significantly worsens in those with diabetic retinopathy.54–56 Moreover, we have also recently shown that a reduction in corneal nerve fiber length predicts worsening of diabetic retinopathy.57 CCM has also been deployed to assess nerve regeneration in clinical trials evaluating new therapies in sarcoid and diabetic neuropathy58,59 and after simultaneous pancreas and kidney transplantation.17
This is the first study to assess the diagnostic utility of corneal nerve fractal dimension. We show that ACNFrD is comparable to CNFD, CNBD, and CNFL in diagnosing patients with and without diabetic neuropathy. However, we believe that the additional utility of this measure may arise by characterizing the structural complexity of the corneal nerves, to provide an additional means of differentiating patients with neuropathies of different etiologies including amyloid neuropathy,23 CMT1A,24 chronic inflammatory demyelinating polyneuropathy,26,25 and HIV.27 It may also help to identify patterns of subbasal corneal nerve loss associated with central neurodegenerative conditions, including motor neuron disease,28 Parkinson's disease,29 multiple sclerosis,30 and stroke.60
A limitation of the present study is the relatively small number of patients with established neuropathy. However, we have introduced and evaluated the clinical utility of ACNFrD and shown that it is comparable to established CCM parameters in identifying patients with and without diabetic neuropathy. Further work is required to confirm the utility of ACNFrD in differentiating other peripheral and central neurodegenerative conditions.
Acknowledgments
The authors thank Mitra Tavakoli for undertaking CCM and Hassan Fadavi for performing neuropathy assessments in a proportion of subjects.
Supported by the Manchester Comprehensive Local Research Network, the National Institute for Health Research/Wellcome Trust Clinical Research Facility in Manchester, National Institutes of Health (R105991), and Juvenile Diabetes Research Foundation International (27-2008-362).
Disclosure: X. Chen, None; J. Graham, None; I.N. Petropoulos, None; G. Ponirakis, None; O. Asghar, None; U. Alam, None; A. Marshall, None; M. Ferdousi, None; S. Azmi, None; N. Efron, None; R.A. Malik, None
References
- 1. Abbott CA, Malik RA, van Ross ER, Kulkarni J, Boulton AJ. . Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the U.K. Diabetes Care. 2011; 34: 2220– 2224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Dyck PJ, Norell JE, Tritschler H,et al. . Challenges in design of multicenter trials: end points assessed longitudinally for change and monotonicity. Diabetes Care. 2007; 30: 2619– 2625. [DOI] [PubMed] [Google Scholar]
- 3. Malik RA. . Why are there no good treatments for diabetic neuropathy? Lancet Diabetes Endocrinol. 2014; 2: 607– 609. [DOI] [PubMed] [Google Scholar]
- 4. Boulton AJ, Kempler P, Ametov A, Ziegler D. . Whither pathogenetic treatments for diabetic polyneuropathy? Diabetes Metab Res Rev. 2013; 29: 327– 333. [DOI] [PubMed] [Google Scholar]
- 5. Dyck PJ, Herrmann DN, Staff NP. . Assessing decreased sensation and increased sensory phenomena in diabetic polyneuropathies. Diabetes. 2013; 62: 3677– 3686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Malik RA. . Which test for diagnosing early human diabetic neuropathy? Diabetes. 2014; 63: 2206– 2208. [DOI] [PubMed] [Google Scholar]
- 7. Breiner A, Lovblom LE, Perkins BA, Bril V. . Does the prevailing hypothesis that small-fiber dysfunction precedes large-fiber dysfunction apply to type 1 diabetic patients? Diabetes Care. 2014; 37: 1418– 1424. [DOI] [PubMed] [Google Scholar]
- 8. Dyck PJ, Argyros B, Russell JW,et al. . Multicenter trial of the proficiency of smart quantitative sensation tests. Muscle Nerve. 2014; 49: 645– 653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lauria G, Lombardi R. . Small fiber neuropathy: is skin biopsy the holy grail? Curr Diab Rep. 2012; 12: 384– 392. [DOI] [PubMed] [Google Scholar]
- 10. Hoeijmakers JG, Faber CG, Lauria G, Merkies IS, Waxman SG. . Small-fiber neuropathies--advances in diagnosis, pathophysiology and management. Nat Rev Neurol. 2012; 8: 369– 379. [DOI] [PubMed] [Google Scholar]
- 11. Polydefkis M, Hauer P, Sheth S, Sirdofsky M, Griffin JW, McArthur JC. . The time course of epidermal nerve fiber regeneration: studies in normal controls and in people with diabetes, with and without neuropathy. Brain. 2004; 127: 1606– 1615. [DOI] [PubMed] [Google Scholar]
- 12. Malik R, Veves A, Tesfaye S,et al. . Small fiber neuropathy: role in the diagnosis of diabetic sensorimotor polyneuropathy. Diabetes Metab Res Rev. 2011; 27: 678– 684. [DOI] [PubMed] [Google Scholar]
- 13. Malik RA, Kallinikos P, Abbott CA,et al. . Corneal confocal microscopy: a non-invasive surrogate of nerve fiber damage and repair in diabetic patients. Diabetologia. 2003; 46: 683– 688. [DOI] [PubMed] [Google Scholar]
- 14. Quattrini C, Tavakoli M, Jeziorska M,et al. . Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes. 2007; 56: 2148– 2154. [DOI] [PubMed] [Google Scholar]
- 15. Pritchard N, Edwards K, Dehghani C,et al. . Longitudinal assessment of neuropathy in type 1 diabetes using novel ophthalmic markers (LANDMark): study design and baseline characteristics. Diabetes Res Clin Pract. 2014; 104: 248– 256. [DOI] [PubMed] [Google Scholar]
- 16. Asghar O, Petropoulos IN, Alam U,et al. . Corneal confocal microscopy detects neuropathy in subjects with impaired glucose tolerance. Diabetes Care. 2014; 37: 2643– 2646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Tavakoli M, Mitu-Pretorian M, Petropoulos IN,et al. . Corneal confocal microscopy detects early nerve regeneration in diabetic neuropathy after simultaneous pancreas and kidney transplantation. Diabetes. 2013; 62: 254– 260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Chen X, Graham J, Dabbah M,et al. . Small nerve fiber quantification in the diagnosis of diabetic sensorimotor polyneuropathy: comparing corneal confocal microscopy with intraepidermal nerve fiber density. Diabetes Care. 2015; 38: 1138– 1144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Dabbah MA, Graham J, Petropoulos I, Tavakoli M, Malik RA. . Dual-model automatic detection of nerve-fibers in corneal confocal microscopy images. Med Image Comput Comput Assist Interv. 2010; 13: 300– 307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Dabbah MA, Graham J, Petropoulos IN, Tavakoli M, Malik RA. . Automatic analysis of diabetic peripheral neuropathy using multi-scale quantitative morphology of nerve fibers in corneal confocal microscopy imaging. Med Image Anal. 2011; 15: 738– 747. [DOI] [PubMed] [Google Scholar]
- 21. Petropoulos IN, Alam U, Fadavi H,et al. . Rapid automated diagnosis of diabetic peripheral neuropathy with in vivo corneal confocal microscopy. Invest Ophthalmol Vis Sci. 2014; 55: 2071– 2078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Alam U, Jeziorska M, Petropoulos I,et al. . Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fiber density in diabetic neuropathy. PLoS One. 2017; 12: e0180175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Rousseau A, Cauquil C, Dupas B,et al. . Potential role of in vivo confocal microscopy for imaging corneal nerves in transthyretin familial amyloid polyneuropathy. JAMA Ophthalmol. 2016; 134: 983– 989. [DOI] [PubMed] [Google Scholar]
- 24. Tavakoli M, Marshall A, Banka S,et al. . Corneal confocal microscopy detects small-fiber neuropathy in Charcot-Marie-Tooth disease type 1A patients. Muscle Nerve. 2012; 46: 698– 704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Stettner M, Hinrichs L, Guthoff R,et al. . Corneal confocal microscopy in chronic inflammatory demyelinating polyneuropathy. Ann Clin Transl Neurol. 2015; 3: 88– 100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Rajabally Y, Stettner M, Kieseier B, Hartung H, Malik R. CIDP. and other inflammatory neuropathies in diabetes - diagnosis and management. Nat Rev Neurol. 2017; 13: 599– 611. [DOI] [PubMed] [Google Scholar]
- 27. Kemp H, Petropoulos I, Rice A,et al. . Use of corneal confocal microscopy to evaluate small nerve fibers in patients with human immunodeficiency virus. JAMA Ophthalmol. 2017; 135: 795– 800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Ferrari G, Grisan E, Scarpa F,et al. . Corneal confocal microscopy reveals trigeminal small sensory fiber neuropathy in amyotrophic lateral sclerosis. Front Aging Neurosci. 2014; 16: 278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Kass-Iliyya L, Leung M, Marshall A,et al. . The perception of affective touch in Parkinson's disease and its relation to small fiber neuropathy. Eur J Neurosci. 2017; 45: 232– 237. [DOI] [PubMed] [Google Scholar]
- 30. Petropoulos I, Kamran S, Li Y,et al. . Corneal confocal microscopy: an imaging endpoint for axonal degeneration in multiple sclerosis. Invest Ophthalmol Vis Sci. 2017; 58: 3677– 3681. [DOI] [PubMed] [Google Scholar]
- 31. Bitirgen G, Akpinar Z, Malik R, Ozkagnici A. . Use of corneal confocal microscopy to detect corneal nerve loss and increased dendritic cells in patients with multiple sclerosis. JAMA Ophthalmol. 2017; 135: 777– 782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Falconer K. . Fractal Geometry: Mathematical Foundations and Applications. 3rd ed. New York: Wiley; 2013. [Google Scholar]
- 33. Tesfaye S, Boulton AJ, Dyck PJ,et al. . Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010; 33: 2285– 2293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. . A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia. 1993; 36: 150– 154. [DOI] [PubMed] [Google Scholar]
- 35. Meijer JW, Smit AJ, Sonderen EV, Groothoff JW, Eisma WH, Links TP. . Symptom scoring systems to diagnose distal polyneuropathy in diabetes: the Diabetic Neuropathy Symptom score. Diabet Med. 2002; 19: 962– 965. [DOI] [PubMed] [Google Scholar]
- 36. Petropoulos IN, Manzoor T, Morgan P,et al. . Repeatability of in vivo corneal confocal microscopy to quantify corneal nerve morphology. Cornea. 2013; 32: e83– e89. [DOI] [PubMed] [Google Scholar]
- 37. Chen X, Graham J, Dabbah M, Petropoulos I, Tavakoli M, Malik R. . An automatic tool for quantification of nerve fibers in corneal confocal microscopy images. IEEE Trans Biomed Eng. 2017; 64: 786– 794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Smith JT, Lange G, Marks W. . Fractal methods and results in cellular morphology—dimensions, lacunarity and multifractals. J Neurosci Methods. 1997; 69: 123– 136. [DOI] [PubMed] [Google Scholar]
- 39. University of Manchester. Early Neuropathy Assessment (ENA) software. Available at: http://research.bmh.manchester.ac.uk/ena/ACCMetricsuserinstructions/. Accessed February 1, 2018.
- 40. Hanley J, McNeil B. . The meaning and use of the area under a Receiver Operating Characteristic (ROC) curve. Radiology. 1982; 143: 29– 36. [DOI] [PubMed] [Google Scholar]
- 41. Marshall A, Lee-Kubli C, Azmi S,et al. . Spinal disinhibition in experimental and clinical painful diabetic neuropathy. Diabetes. 2017; 66: 1380– 1390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Azmi S, Ferdousi M, Alam U,et al. . Small-fiber neuropathy in men with type 1 diabetes and erectile dysfunction: a cross-sectional study. Diabetologia. 2017; 60: 1094– 1101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Almurdhi M, Brown S, Bowling F,et al. . Altered walking strategy and increased unsteadiness in participants with impaired glucose tolerance and type 2 diabetes relates to small-fiber neuropathy but not vitamin D deficiency. Diabet Med. 2017; 34: 839– 845. [DOI] [PubMed] [Google Scholar]
- 44. Pop-Busui R, Boulton A, Feldman E,et al. . Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017; 40: 136– 154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Tavakoli M, Petropoulos IN, Malik RA. . Corneal confocal microscopy to assess diabetic neuropathy: an eye on the foot. J Diabetes Sci Technol. 2013; 7: 1179– 1189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Ziegler D, Papanas N, Zhivov A,et al. . Early detection of nerve fiber loss by corneal confocal microscopy and skin biopsy in recently diagnosed type 2 diabetes. Diabetes. 2014. [DOI] [PubMed]
- 47. Sivaskandarajah GA, Halpern EM, Lovblom LE,et al. . Structure-function relationship between corneal nerves and conventional small-fiber tests in type 1 diabetes. Diabetes Care. 2013; 36: 2748– 2755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Halpern EM, Lovblom LE, Orlov S, Ahmed A, Bril V, Perkins BA. . The impact of common variation in the definition of diabetic sensorimotor polyneuropathy on the validity of corneal in vivo confocal microscopy in patients with type 1 diabetes: a brief report. J Diabetes Complications. 2013; 27: 240– 242. [DOI] [PubMed] [Google Scholar]
- 49. Dehghani C, Pritchard N, Edwards K, Russell AW, Malik RA, Efron N. . Fully automated, semiautomated, and manual morphometric analysis of corneal subbasal nerve plexus in individuals with and without diabetes. Cornea. 2014; 33: 696– 702. [DOI] [PubMed] [Google Scholar]
- 50. Scarr D, Lovblom L, Ostrovski I,et al. . Agreement between automated and manual quantification of corneal nerve fiber length: implications for diabetic neuropathy research. J Diabetes Complications. 2017; 31: 1066– 1073. [DOI] [PubMed] [Google Scholar]
- 51. Bikbova G, Oshitari T, Baba T, Yamamoto S. . Neuronal changes in the diabetic cornea: perspectives for neuroprotection. Biomed Res Int. 2016; 2016: 5140823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Ljubimov AV. . Diabetic complications in the cornea. Vision Res. 2017; 139: 138– 152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Shih KC, Lam KS, Tong L. . A systematic review on the impact of diabetes mellitus on the ocular surface. Nutr Diabetes. 2017; 7: e251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Bitirgen G, Ozkagnici A, Malik R, Kerimoglu H. . Corneal nerve fiber damage precedes diabetic retinopathy in patients with type 2 diabetes mellitus. Diabet Med. 2014; 31: 431– 438. [DOI] [PubMed] [Google Scholar]
- 55. Petropoulos I, Green P, Chan A,et al. . Corneal confocal microscopy detects neuropathy in patients with type 1 diabetes without retinopathy or microalbuminuria. PLoS One. 2015; 10: e0123517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Szalai E, Deák E, Módis LJ,et al. . Early corneal cellular and nerve fiber pathology in young patients with type 1 diabetes mellitus identified using corneal confocal microscopy. Invest Ophthalmol Vis Sci. 2016; 57: 853– 858. [DOI] [PubMed] [Google Scholar]
- 57. Srinivasan S, Dehghani C, Pritchard N,et al. . Ophthalmic and clinical factors that predict four-year development and worsening of diabetic retinopathy in type 1 diabetes. J Diabetes Complications. 2017; 32: 67– 74. [DOI] [PubMed] [Google Scholar]
- 58. Culver D, Dahan A, Bajorunas D,et al. . Cibinetide improves corneal nerve fiber abundance in patients with sarcoidosis-associated small nerve fiber loss and neuropathic pain. Invest Ophthalmol Vis Sci. 2017; 58: BIO52– BIO60. [DOI] [PubMed] [Google Scholar]
- 59. Lewis E, Perkins B, Lovblom L, Bazinet R, Wolever T, Bril V. . Effect of omega-3 supplementation on neuropathy in type 1 diabetes: a 12-month pilot trial. Neurology. 2017; 88: 2294– 2301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Khan A, Akhtar N, Kamran S,et al. . Corneal confocal microscopy detects corneal nerve damage in patients admitted with acute ischemic stroke. Stroke. 2017; 48: 3012– 3018. [DOI] [PubMed] [Google Scholar]